Article Text

Abstract
Objective To determine rates of faecal biomarker results capable of suggesting potentially treatable causes of irritable bowel syndrome (IBS) symptomatology in a population of patients with symptoms of IBS who meet Rome III criteria for that condition.
Design Descriptive, retrospective study in which faecal biomarker results (dichotomised into ‘normal’ and ‘abnormal’ values) were related to data from patient-completed questionnaire data identifying demographics, Rome III criteria for IBS and IBS phenotype (IBS-D, IBS-C, IBS-M and IBS-U).
Setting Commercial reference laboratory.
Patients Individuals whose physicians ordered faecal biomarker testing for evaluation of chronic abdominal symptoms consistent with IBS.
Interventions None.
Main outcome measures Rates of occurrence of abnormal results on any of seven faecal biomarkers suggesting a treatable cause for IBS symptoms.
Results Abdominal symptoms meeting Rome III criteria for IBS were present in 3553 records (the population), which were subjected to further analysis. Abnormal biomarker results (the outcomes) occurred in 94% of cases; 73% and 65% of records indicated growth of a bacterial potential pathogen and low growth of beneficial organisms, respectively. Abnormal results for all other faecal biomarkers occurred with frequencies from 5% to 13%. Frequency of abnormal results for elastase, calprotectin, eosinophil protein X, and beneficial organisms rose significantly with age, and differed significantly across IBS phenotypes.
Conclusions A large proportion of patients manifesting symptoms meeting Rome III IBS diagnostic criteria have faecal biomarker results indicating potential underlying, treatable causes of their symptoms. Faecal biomarker testing is an appropriate means of identifying potentially treatable causes of IBS symptoms.
- IRRITABLE BOWEL SYNDROME
- PRIMARY CARE
- CLINICAL DECISION MAKING
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Abdominal symptoms consistent with irritable bowel syndrome (IBS) are highly prevalent and impose substantial burdens on sufferers and the healthcare system in general. A positive diagnosis can be made using Rome Foundation criteria for IBS, but such clinical criteria do not offer guidance on management of any individual patient's condition, leading to continued use of invasive and costly diagnostic imaging techniques that produce meaningful results in only a small fraction of cases.1 ,2
Current evidence indicates that symptoms associated with IBS, including those contributing to a positive diagnosis by Rome III and other clinical criteria, frequently arise from a number of independent, and often treatable, conditions.3 The actual frequency of the presence of such underlying causes of IBS symptoms, however, remains unknown.
In the present study, therefore, we attempted to characterise the frequency and distribution of results for seven faecal biomarkers capable of suggesting underlying conditions that could be responsible for producing symptoms in accordance with those diagnostic criteria, in a group of subjects with chronic abdominal pain meeting current Rome III IBS criteria.
Methods
This study was a retrospective, observational evaluation of faecal biomarker results in a population of subjects with abdominal pain, verified by a validated, self-administered questionnaire to have IBS by Rome III criteria.
Setting
The study was conducted by Genova Diagnostics (GDX, Asheville, North Carolina, USA), a commercial CLIA-certified reference laboratory. GDX routinely includes a validated, self-report Rome III IBS questionnaire in all collection kits used for faecal biomarker testing.
During the study period, from April 2013 to March 2014, all records for which patient questionnaires were completed were eligible for inclusion. Questionnaires were prelabelled with bar codes that associated them with faecal specimens for results reporting. For this study, all data were stripped of patient identifying information prior to analysis, and no protected health information was recorded for study purposes. Thus, the data set for analysis included results of faecal biomarker testing, age, gender and results of the Rome III survey only. Results of the Rome III survey were used to identify subjects who met Rome III criteria for IBS, and to categorise them by IBS phenotype.
Patient population
GDX serves a predominantly US-based ambulatory patient population; faecal biomarker testing is typically ordered by primary care physicians when patients present with gastrointestinal (GI) symptoms without obvious cause. Thus, records included in this study represent a ‘real world’ population selected by primary care providers who use faecal biomarker testing provided by GDX in response to their concerns about potential sources of GI symptomatology.
For this study, only patients whose age was indicated as ≥18 years, who had faecal testing for any of the biomarkers of interest, and whose Rome III questionnaire provided a positive diagnosis of IBS were included. Not every Rome III-confirmed subject had every biomarker ordered on test requisitions. There was no study-mandated intervention; the ordering of faecal biomarker tests was at the discretion of the referring physician.
Faecal biomarkers
Based on previous work, we selected seven target biomarkers each of which produced abnormal results in more than 2% of subjects with abdominal symptoms consistent with IBS (table 1).4 The clinical validity and diagnostic performance of these target biomarkers have been summarised in other published studies.5–12
Targeted faecal biomarkers in patients with Rome III-confirmed IBS
Supplementary table
Supplementary table
Statistical analyses
Faecal biomarker results were dichotomised into ‘normal’ and ‘abnormal’ categories based on the cut-offs shown in table 1. Frequency distributions for abnormal results were prepared for each biomarker and for other study variables, including age, gender and Rome III IBS subcategory. Differences in distribution of abnormal biomarker results between age, gender, and IBS subcategories were analysed by Chi-square for significance.
Results
A total of 24 258 faecal specimens were received during the study period. Of those, 7503 included completed demographic surveys; calculation of a true survey response rate was not possible because it could not be confirmed that all specimen collection kits in use during the study period included survey forms. The flow diagram in figure 1 illustrates further selection of records based on age and record completion data.
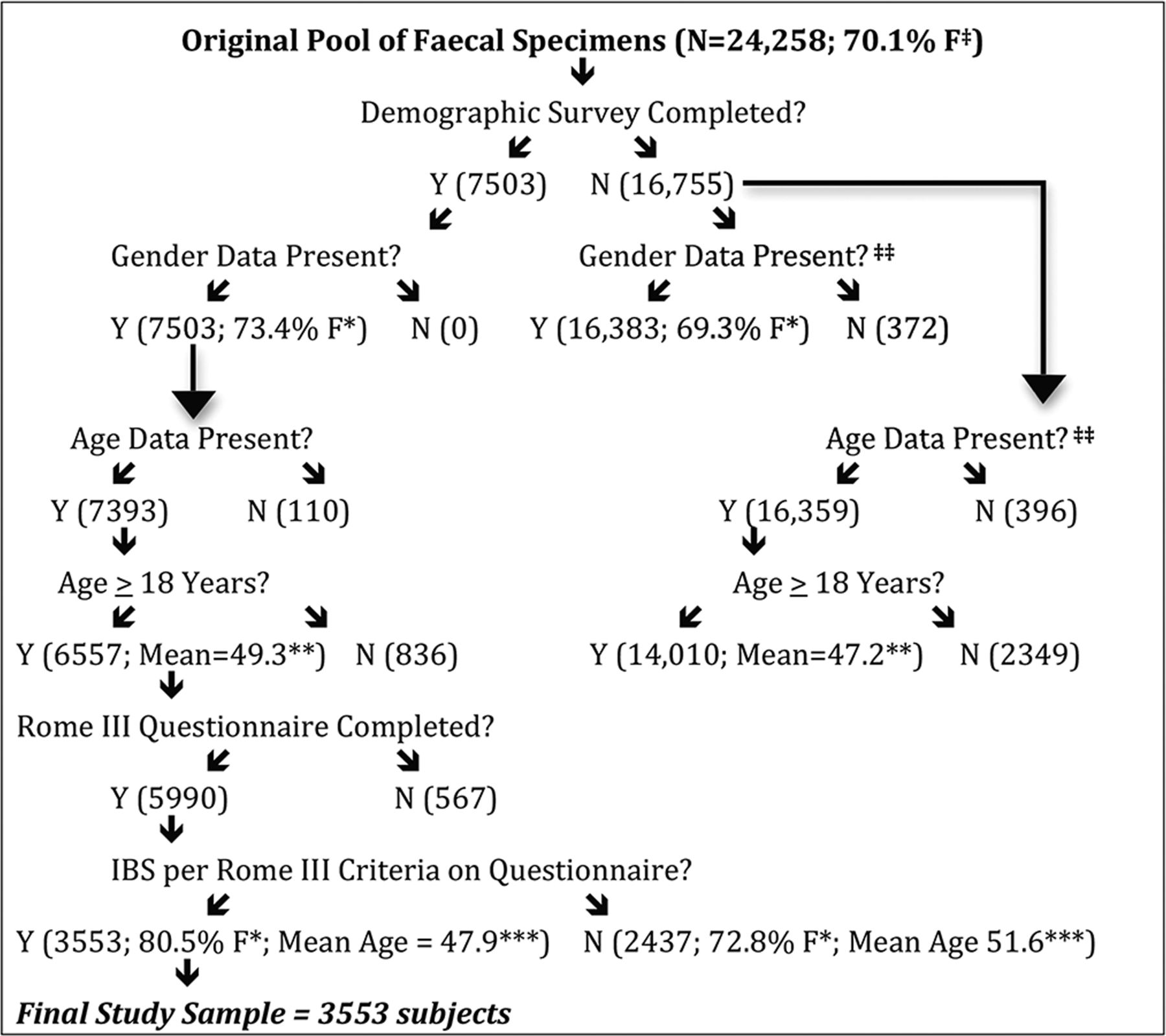
Flow diagram of sample selection and reduction of subject numbers by application of exclusion criteria. ‡Data from Medical Record; ‡‡Records missing gender and age data were not identical. *Δ Gender: p<0.001; **Δ Age: p<0.001; ***Δ Age: p<0.05.
After exclusion of records missing age and Rome III data, and selection of those indicating IBS by Rome III criteria, 3553 records were included for further analysis.
Gender, age and Rome III subcategory distributions
The study population of 3553 subjects consisted of 2860 (80.5%) women and 693 (19.5%) men. There were 1892 (53.3%) 18–49-year-old subjects, with 1348 (37.9%) aged 50–69 years, and 313 (8.8%) aged 70 years or greater.
Figure 2 shows the distribution of Rome III subcategories of IBS in the total population of Rome III-confirmed subjects.
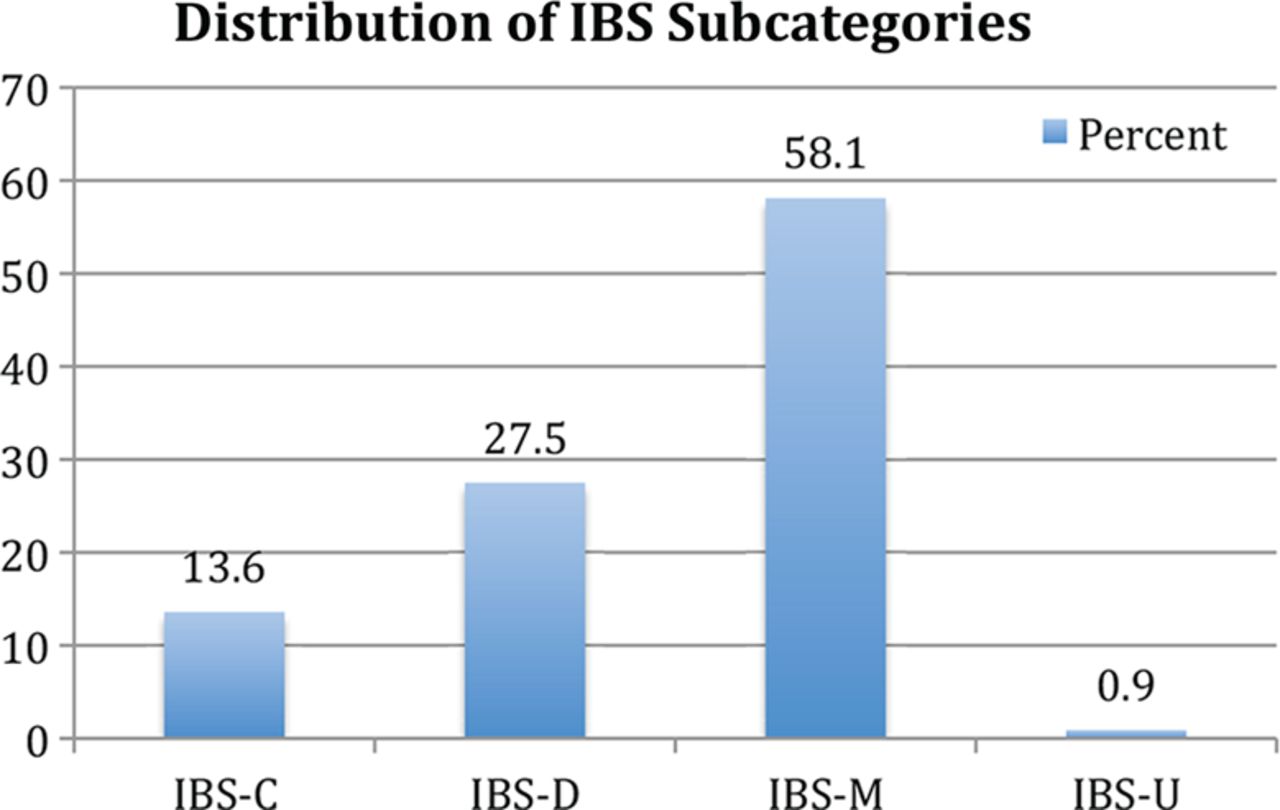
Distribution of ROME-III irritable bowel syndrome (IBS) subcategories in the study sample of 3553 individuals.
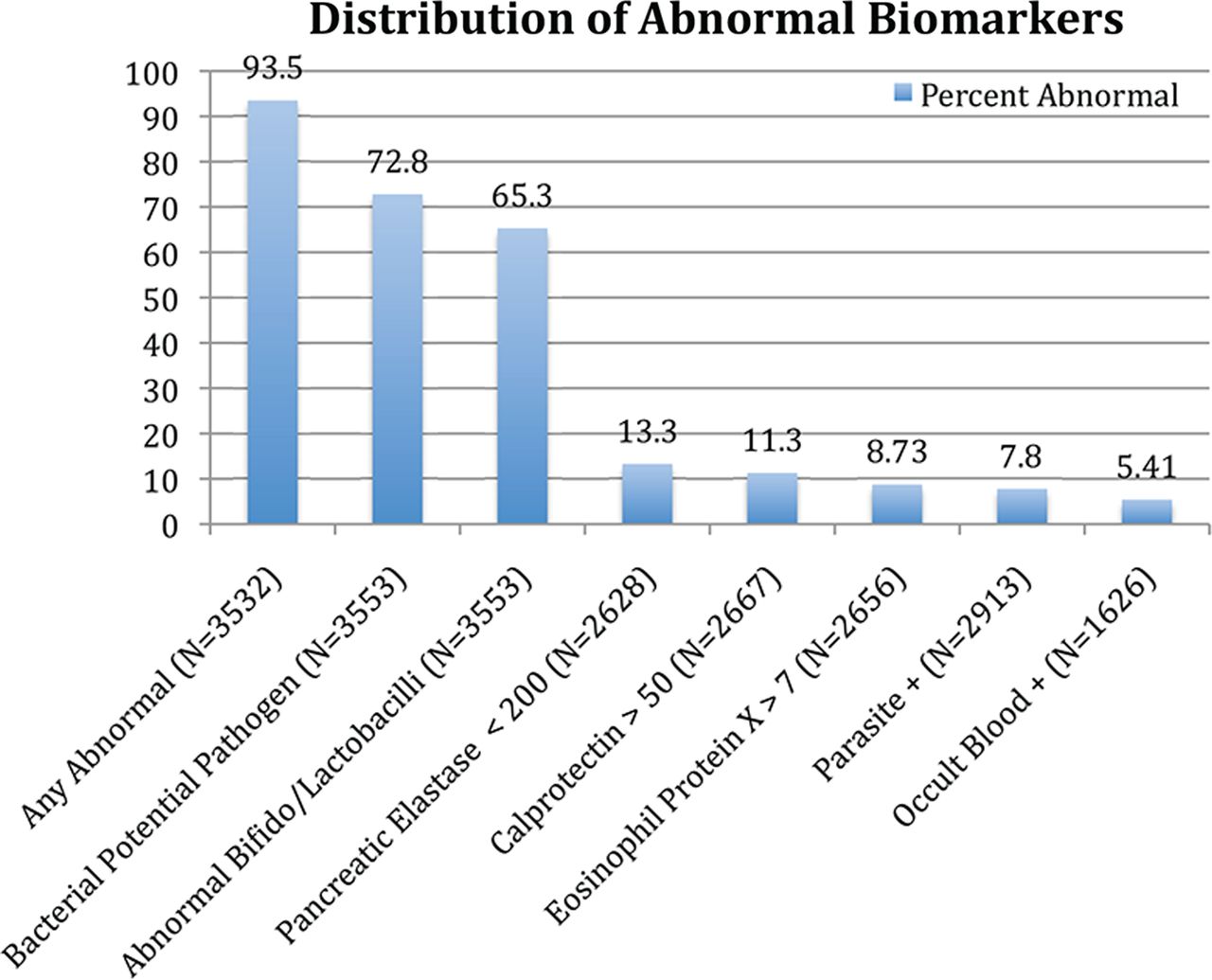
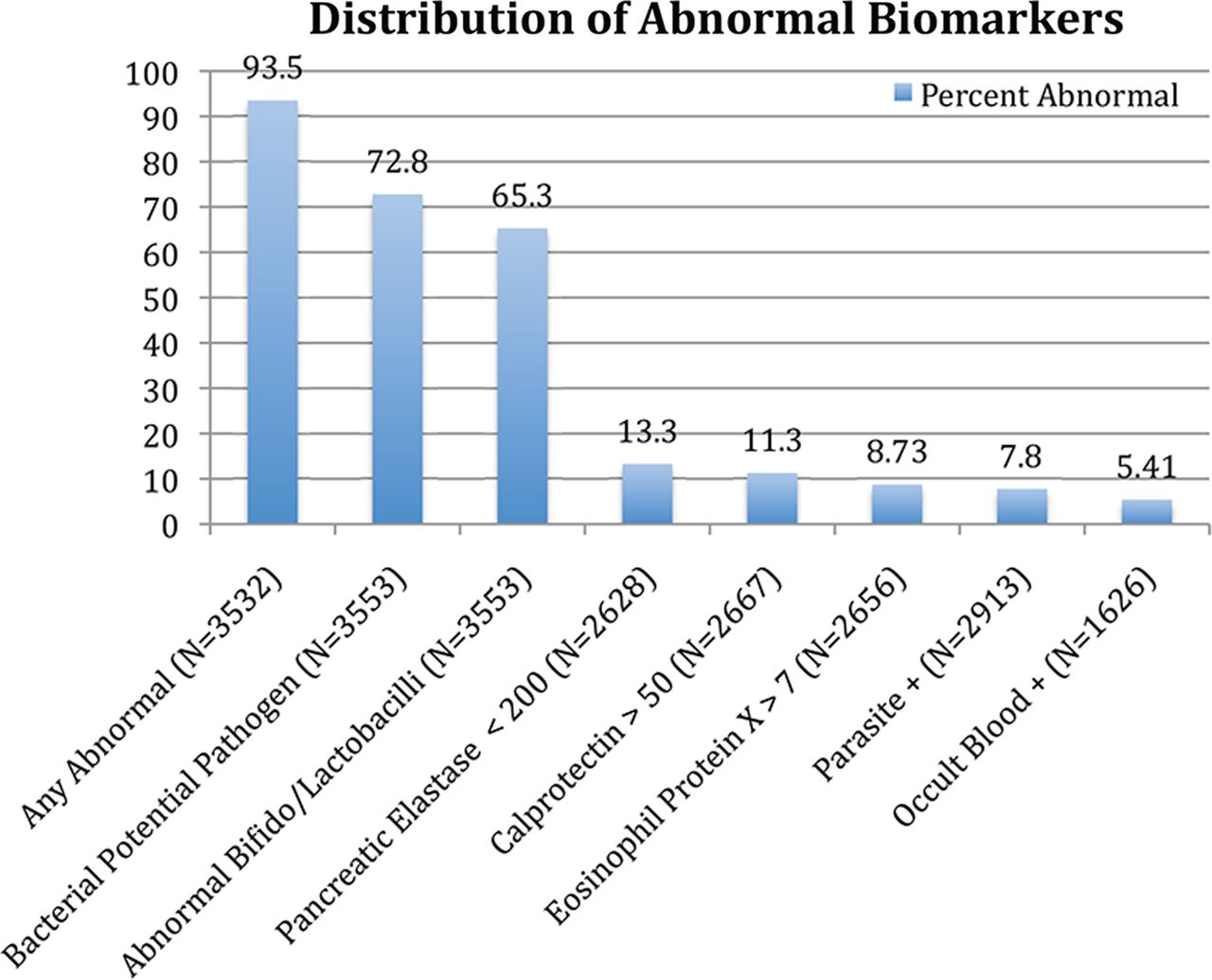
General distribution of abnormal biomarker results
Figure 3 shows the frequency of abnormal biomarker results in the entire Rome III-confirmed study population; not all subjects were tested for all biomarkers, therefore, the total number of subjects tested for each biomarker appears in parentheses.
{kind=link}
{kind=link}
{kind=link}
Distribution of abnormal biomarker results in study sample (N=3553). Note that any individual may have had zero, one or more than one abnormal result, and that not every individual had every biomarker tested.
Tests for the biomarkers pancreatic elastase-1 (PE-1), faecal calprotectin (FC) and eosinophil protein X (EPX) produce continuous results, with ‘abnormal’ being defined as values above or below clinically relevant cut-offs as shown in table 2.
Distribution of results for continuous biomarkers
We examined possible relationships between several individual biomarkers. For example, elevated levels of EPX and FC or the presence of faecal occult blood (FOB) may each indicate mucosal inflammation and parasitosis may cause inflammation. In our cohort only 48.9% (112/229) of subjects with elevated EPX levels also had an elevated FC value. In IBS subjects with a documented parasite, 7.3% (14/193), 4.3% (9/210) and 3.1% (3/97) had an abnormal FC, EPX or FOB, respectively.
Distribution of abnormal biomarker results by gender
There was a significant gender effect on several of the biomarkers studied. There were significantly more male than female subjects with abnormal PE-1 results (17.2% vs 12.4%, p<0.001). A small but significant female predominance was seen in abnormally low levels of growth of Bifidobacteria/Lactobacillus, with abnormal results in 67.3% of women versus 57.1% in men (p<0.001). All other abnormalities were evenly gender distributed.
Distribution of abnormal biomarker results by age
The frequency of abnormal results for several individual biomarkers rose significantly with increasing age categories, as shown in table 3. Subjects in the middle age group (50–69 years) had significantly greater frequency of abnormal commensal organisms (low growth of Bifidobacteria/Lactobacillus), compared with the youngest and oldest groups.
Proportion (%) of subjects with abnormal results by age
No significant age effects were seen on the rates of abnormal results for occult blood, parasites or bacterial potential pathogens.
Distribution of abnormal biomarkers by Rome III IBS subcategory
Table 4 shows significant differences in the occurrence of abnormal faecal biomarker results by Rome III IBS subcategory (the category IBS-U included only 32 records (0.9%), and was dropped from subsequent analyses).
Proportion (%) of subjects with abnormal results by IBS subcategory
No significant effects of IBS subcategory were seen in rates of abnormal results for FOB, parasites or PE-1. There were no significant differences by Rome III subcategory for having abnormal results for the outcome ‘any abnormal’ (IBS-C, 24.4%, IBS-D, 28.8%, IBS-M 25.0%).
Discussion
The present study represents, to our knowledge, the largest population of patients with Rome III-confirmed IBS in which a complete characterisation of demographics and IBS subtypes has been attempted, and the only one to date in which an array of faecal biomarker results has been described. As noted, there was no control group; this study was not intended to evaluate the discriminatory power of any of the biomarkers as diagnostic of IBS; in fact, subjects in whom abnormal biomarkers were detected would be candidates for an alternate diagnosis based on those results, and a broader workup, potentially including endoscopy in certain cases, would be appropriate.
The principal findings in this study are that the rate of abnormal results on the faecal biomarkers evaluated is quite high, at 94% overall; we identified significant differences in faecal biomarker patterns occurring by age category, and by IBS phenotype. This study confirms and strengthens our previous findings in a study of patients with presumed IBS based on ICD-9 codes alone,4 demonstrating quite similar distributions of abnormal biomarker results in a population confirmed to have IBS by Rome III criteria. The current study also includes analyses of biomarker results by Rome III subcategories, and presents a more detailed distribution of results of biomarker tests returning continuous results.
Implications of abnormal biomarkers in an IBS population
Changes in our understanding of IBS have led to the recognition that the syndrome is unlikely to have a single, identifiable cause, but also that it ought no longer to be considered a diagnosis of exclusion. Rather, the notion that IBS is an ‘umbrella’ diagnosis of a phenotype defined by symptoms that are common to a number of discrete disease processes has gained currency.3 ,15
In the present study, we have taken initial steps to characterise a group of biomarkers capable of suggesting alternative, treatable conditions or underlying causes producing the IBS phenotype as defined by Rome III criteria. The intention is to improve outcomes of patients classified as meeting IBS criteria by identifying and treating reversible disorders. Ultimately, it is to be hoped that faecal biomarker testing will have the effect of shrinking the number of patients in whom the diagnosis of IBS, without further specification, is the end point of the diagnostic evaluation.
Our analysis suggests that parallel assessment of multiple biomarkers may have significant clinical utility in differentiating specific underlying aetiologies of IBS presentations. For example, FC and EPX (assessing neutrophilic inflammation and eosinophilic inflammation, respectively) appear to be independent biomarkers. This finding is consistent with other published studies demonstrating that EPX may be a marker of treatment response in collagenous colitis, which is thought to have more eosinophilic involvement than inflammatory bowel disease (IBD).16 ,17
Consistent with our previous work in a non-Rome III-confirmed IBS population,4 we identified a high overall rate of abnormal findings on selected faecal biomarkers. The two microbiota-related biomarkers, bacterial potential pathogens and abnormal growth of the beneficial commensals Bifidobacteria and Lactobacillus, accounted for a large proportion of abnormal results. These are non-standard biomarkers, and accurate values for their rates in healthy populations are not known, so it is possible that these findings have relatively little significance.
On the other hand, there is increasing evidence from other studies that community-level dysbiosis is a highly prevalent, important and potentially contributory factor to IBS, particularly in the diarrhoea-predominant subtype.15 ,18
Others have shown, using 16S rRNA gene sequencing by PCR, that significant phylotype-level alterations exist in the intestinal microbiota of patients with IBS in comparison with control subjects, that such differences persist between certain IBS subtypes, and that patients with IBS carry microbiota of significantly less biodiversity than do healthy control subjects.19–24
These studies appear to suggest that our culture-based result may indeed be a rough indicator of shifted microbial patterns in IBS, and make a case for further study using our faecal biomarkers in combination with advanced microbiome genomic sequencing.
Implications of abnormal biomarkers by IBS subtype
We found substantial differences between IBS subgroups in terms of biomarker results. Patients in the IBS-D subcategory had significantly higher rates of abnormal calprotectin, EPX and bacterial potential pathogens, compared with the IBS-C and IBS-M groups. Compared with IBS-M, patients in the IBS-D and IBS-C groups had significantly higher and lower rates of abnormal calprotectin and EPX, respectively. These findings appear to suggest biological differences between these subgroups, and to represent greater inflammatory responses in patients with IBS-D than in patients with IBS-C.
Subjects in the IBS-D group also had a higher rate of bacterial potential pathogens (see online supplementary table 1) compared with patients with IBS-M, though the numerical difference was small. Given that these were culture-based results, and that the definition of ‘potential pathogen’ is to some extent arbitrary, further study of the composition of the entire GI microbiome might shed clearer light on the role of various bacterial taxa in the etiopathogenesis of IBS.
Our findings in these regards appear consistent with previous work by others suggesting that patients with IBS-D have higher rates of both low-grade inflammation and dysbiosis.
Future studies should focus on the clinical utility of faecal biomarkers in management of patients whose symptoms meet Rome III criteria for IBS. It has already been shown using retrospective medical claims analysis that a structured faecal biomarker panel can reduce healthcare costs and unnecessary utilisation of services in evaluating patients with abdominal symptoms consistent with having IBS.25 It is to be anticipated that such a structured panel, composed of carefully selected biomarkers, will be shown prospectively to improve patient outcomes by directing management strategies towards the underlying, treatable causes of IBS symptoms, and at the same time to reduce utilisation of invasive and costly diagnostic procedures.
Application of faecal biomarkers in clinical decision-making for patients with IBS
It is important to recognise that the clinical utility, in terms of negative and positive predictive values (NPV, PPV, respectively) of any diagnostic test is dependent on the prevalence of the condition of interest in the population under discussion. Values for NPV and PPV in the literature are frequently misleading, because they are typically derived from prevalence figures in populations with high concentrations of the condition of interest, whereas in unselected clinical populations, the prevalence, and, hence, the predictive values, may be considerably different.26
Using published prevalence figures in patients with IBS seen in primary care settings for endocrine pancreatic insufficiency (6.1%27) and neutrophilic inflammation (eg, IBD (1%28)), and the published performance characteristics of the PE-1 and FC assays used in this current study,5 ,8 ,9 it is readily shown that the NPVs of both biomarkers are greater than 99%, while the PPV of FC is relatively low, confirming its known use as a screening test to rule out inflammatory processes.9
On the other hand, PE-1 has, using these same assumptions, a PPV of 46.3%. This suggests that the PE-1 assay could serve to identify a subset of patients with IBS in whom a trial of pancreatic enzyme therapy is worthwhile, treating only about one patient who does not have exocrine pancreatic insufficiency (EPI) for each one correctly managed.
Additional potential biomarkers in assessment of patients with IBS
As IBS is increasingly recognised as a syndrome with multiple, possibly interacting, underlying causes, we anticipate the emergence of additional biomarkers that may be of substantial clinical utility in management.
For example, bile acid malabsorption (BAM) has been shown to be present in 25% or more of patients meeting clinical criteria for IBS, especially those with the IBS-D phenotype.29 ,30 The established standard for making the diagnosis of BAM is the 23-seleno-25-homotaurocholic acid test (SeHCAT), which is time-consuming and, while approved in most European countries, is as yet unavailable in the USA.31 Other studies, such as the 14C glycocholate test, involve radiation exposure, and may have difficulty in differentiation BAM from small intestinal bacterial overgrowth (SIBO), while measurement of serum 7 α-hydroxy-4-cholesten-3-one (C4) lacks sufficient clinical validation.31
Direct measurement of bile acids in faecal matter may provide a simpler means of detecting BAM in patients with IBS, and elevated levels of faecal bile acids have indeed been identified in both patients with IBS-D and functional diarrhoea.31 ,32 Total faecal bile acid levels appear to have clinical validity, showing significant association with SeHCAT retention at day 3, and a good correlation (r=0.606) with serum C4 levels.31 A further potential advantage of direct faecal bile acid measurement is that low, rather than high levels of bile acids have been associated with IBS-C and functional constipation.31 ,33 ,34
Increased intestinal permeability (IP) has also recently been associated with syndrome-defining symptoms of IBS, and has been detected in mucosa of patients with IBS.35 Zonulin is a peptide signalling molecule that disrupts tight junctional proteins between intestinal mucosal cells, leading to increased intestinal permeability (IIP).36 Serological testing for zonulin has been demonstrated to correlate well with gold-standard lactulose/mannitol testing in patients with increased IP from several causes (R2=0.7935).37 A recent study, published to date in abstract form only, has demonstrated elevated blood zonulin levels in subjects with IBS-D.38
Intestinal dysbiosis, as noted above, is a common finding in patients with IBS.39 ,40 Improving accessibility of real-time, multiplex PCR sequencing may yet prove a useful biomarker of dysbiosis, which has been shown to respond well symptomatically to therapy with certain specific probiotic preparations such as B. infantis 35624.41–43
Finally, symptoms of IBS induced by SIBO appear to respond well to treatment with the non-absorbed antibiotic rifaximin, increasing the need for a reliable and convenient biomarker of this condition. Several such biomarkers have recently been identified by Pimentel et al,44–46 who suggest that antibodies against cytolethal distending toxin B and vinculin have potential utility in distinguishing IBS-D from IBD; the immunological targets of these antibodies are known to be produced by bacteria that cause acute gastroenteritis and have been identified in animal models of postinfectious IBS.
As the role of various treatable conditions in patients meeting symptom criteria for IBS grows, it seems likely that these and other biomarkers will be of increasing interest in evaluating such patients and formulating targeted treatment plans.
Limitations
This was a retrospective study, comprised of data from subjects whose physicians ordered faecal biomarker testing as part of their clinical evaluation for abdominal symptoms. Thus, it is susceptible to selection biases, and is not presented as a true cross-sectional study representative of the general population of patients with IBS. This study does, however, represent the largest population of patients with Rome III-confirmed IBS described in detail, including data on faecal biomarker patterns. We therefore believe that, despite these limitations, it significantly extends our knowledge of the nature and characteristics of IBS.
Additionally, with a large number of patients being studied with a range of biomarkers, there is a danger of type I error. However, the biological plausibility of the types of biomarker profiles seen with specific ‘IBS’ phenotypes suggests that this is less likely.
Conclusions
This study showed a high rate of abnormal results on faecal biomarker testing, further confirming previous findings and supporting the concept of IBS as an ‘umbrella’ diagnosis with a suite of symptoms produced in common by a number of different and potentially treatable underlying causes. Future prospective studies may further delineate subpopulations with potentially treatable causes of symptoms consistent with IBS, ultimately shrinking the pool of patients in whom ‘IBS’ represents a diagnostic stopping point, instead refining diagnostic procedures and guiding therapy.
Acknowledgments
Teresa McBride assisted in the conduct of the analysis. Lupine Creative Consulting assisted with the preparation of the manuscript. Audrey Kopp provided administrative assistance in preparation and submission of the manuscript.
References
Footnotes
Contributors All listed authors contributed to the conceptualisation, design, execution, analysis and writing of this manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.