Article Text

Abstract
Introduction Joint Advisory Group (JAG) certification in endoscopy is awarded when trainees attain minimum competency standards for independent practice. A national evidence-based review was undertaken to update standards for training and certification in flexible sigmoidoscopy (FS).
Methods A modified Delphi process was conducted between 2019 and 2020 with multisociety representation from experts and trainees. Following literature review and Grading of Recommendations, Assessment, Development and Evaluations appraisal, recommendation statements on FS training and certification were formulated and subjected to anonymous voting to obtain consensus. Accepted statements were peer-reviewed by national stakeholders for incorporation into the JAG FS certification pathway.
Results In total, 41 recommendation statements were generated under the domains of: definition of competence (13), acquisition of competence (17), assessment of competence (7) and postcertification support (4). The consensus process led to revised criteria for colonoscopy certification, comprising: (A) achieving key performance indicators defined within British Society of Gastroenterology standards (ie, rectal retroversion >90%, polyp retrieval rate >90%, patient comfort <10% with moderate-severe discomfort); (B) minimum procedure count ≥175; (C) performing 15+ procedures over the preceding 3 months; (D) attendance of the JAG Basic Skills in Lower gastrointestinal Endoscopy course; (E) satisfying requirements for formative direct observation of procedural skill (DOPS) and direct observation of polypectomy skill (SMSA level 1); (F) evidence of reflective practice as documented on the JAG Endoscopy Training System reflection tool and (G) successful performance in summative DOPS.
Conclusion The UK standards for training and certification in FS have been updated to support training, uphold standards in FS and polypectomy, and provide support to the newly independent practitioner.
- ENDOSCOPY
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Flexible sigmoidoscopy (FS) is the third most frequently undertaken endoscopic procedure in the UK, with over 500 000 procedures each year. FS is the first line diagnostic investigation for the assessing for anorectal and distal colonic pathology, and is used in some countries for colorectal cancer screening.1 It is recognised that practice variation exists within endoscopy which can impact on patient outcomes.2 3 Accordingly, national standards and quality assurance (QA) frameworks have been implemented in the UK by the Joint Advisory Group in Gastrointestinal Endoscopy (JAG) and British Society of Gastroenterology (BSG) over the last two decades to maximise the effectiveness and safety of endoscopy, reduce practice variation and to optimise the patient experience.4 5
Pivotal to high-quality endoscopy is training and certification. In the UK, the process is overseen by JAG.6–8 Certification is a standardised process which formally credentials a trainee for independent and unsupervised endoscopy nationwide. The JAG FS certification process was originally formulated in 2011 based on pragmatism and consensus. In the era of technological advances, increasing expectations for high-quality endoscopy, and the changing shape of UK training,9 there is a clear need to ensure that these certification pathways remain valid, up to date and evidence based. Following consultation with UK Specialist Advisory Committees, a committee was assembled by JAG and stakeholders, including BSG and Association of Coloproctology of Great Britain & Ireland (ACPGBI), to develop evidence and consensus-based recommendations relevant to training and certification in FS, with emphasis on polypectomy competencies. The aim was to develop a set of recommendations which would form the framework of FS certification within the UK and cover the following domains: (1) definition of competence, (2) acquisition of competence, (3) assessment of competence for FS and polypectomy and (4) postcertification support.
Methods
Guideline development
A modified Delphi process on training and certification on lower gastrointestinal (GI) endoscopy was commissioned by the JAG QA of Training Working Group, with inclusion of JAG, BSG, ACPGBI, training leads and trainee members, and representation from England, Wales, Scotland and Northern Ireland. Through a series of teleconferences, participants were allocated to seven working groups based on the scope of the guideline. The process for FS was held alongside that for colonoscopy certification. Domains of ‘defining competence’, ‘acquisition of competence’ and ‘assessment of competence’ working groups were assigned for diagnostic lower GI endoscopy and polypectomy. Each working group framed questions relevant to training and certification. Where relevant, a Population, Intervention, Comparator, Outcome format was applied. Literature searches were then systematically conducted on major databases including EMBASE, Medline, PubMed and the Cochrane Database of Systematic Reviews. Results were collated and summarised into recommendation statements; these were appraised using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) framework.10 The level of evidence and strength of recommendation were provided for each statement. Although it is standard practice to align recommendations with the level of evidence, statements could receive discordant recommendations (eg, strong recommendation for low quality evidence) if, on balance, the perceived benefit outweighed the paucity of available evidence.
Consensus process
An anonymised, electronic voting process was undertaken during a 2-day face-to-face meeting to measure consensus with recommendation statements. Five Likert scale responses were provided for each statement (strongly disagree, disagree, neither agree nor disagree, agree and strongly agree), with votes for Agree and Strongly Agree indicating agreement with a statement. For each statement, agreement from at least 80% of the group was specified a priori as the threshold for acceptance. For statements that were not accepted, up to three rounds of revisions and revoting were permitted before they were rejected. On collation of the accepted statements, the document was sent to stakeholder groups for review. Accepted recommendation statements (including duplicate statements from the colonoscopy pathway relevant to FS training) were included in the final FS certification pathway document.
Recommendation statements
In total, 45 recommendation statements were generated under the domains of: definition of competence (N=16), acquisition of competence (N=20), assessment of competence (N=8) and postcertification support (N=4). These are summarised in table 1.
Summary of the consensus statements for training and certification in FS
Trainee-relevant key performance indicators (KPIs) in flexible sigmoidoscopy (extrapolated from the UK quality standards document by Rees et al)4
Defining competence
1.1: Competence in flexible sigmoidoscopy is defined as the ability to perform flexible sigmoidoscopy, including all relevant periprocedural and postprocedural aspects and demonstrating relevant endoscopic non-technical Skills (ENTS) consistent with current UK endoscopy best practice standards and guidelines.
Evidence: Low; Recommendation: Strong; Agreement: 100%
Competence in an endoscopic procedure may be defined as the ability to independently carry this out in a safe and effective manner, and across a spectrum of case difficulties and case contexts. For FS, this should cover the necessary periprocedural and postprocedural aspects according to national standards, set by the JAG,11 the BSG and the ACPGBI (table 2).4
FS and colonoscopy share a number of pre, peri and post procedural QA aspects relevant to both trainees and independent practitioners. At present, separate QA standards have not been produced for FS by the relevant national bodies and therefore the group agreed standards relevant to FS training could be drawn from national colonoscopy quality standards.4 A similar approach, in terms of assessment of unit and endoscopist performance, was taken by JAG with extrapolation of relevant colonoscopy key performance indicators (KPIs).11 Guidance for tattoo placement and biopsies for chronic diarrhoea should also be followed.4
Endoscopic non-technical skills (ENTS) are complementary to technical skills and are important for a safe and effective procedure.12 They involve cognitive, interpersonal and social skills and cover communication and teamwork, situational awareness, leadership, judgement and decision making.13 ENTS are essential component of practice with potential positive effects on team performance and clinical outcomes.14 ENTS training, when delivered to an experienced endoscopy team, demonstrates significant improvements in knowledge and attitudes towards patient safety.12 In a recent randomised controlled trial (RCT), novice trainees exposed to ENTS training were rated to be more competent during their first hands-on colonoscopy procedures.15 All JAG direct observation of procedural skills (DOPS) and direct observation of polypectomy skills (DOPyS) assessment forms were updated in July 2016 to emphasise and objectively measure ENTS competencies.16
1.2: Competence in flexible sigmoidoscopy requires the ability to recognise normal findings, describe and document abnormal findings and take appropriate action.
Evidence: Very low; Recommendation: Strong; Agreement: 100%
A competent endoscopist should be able to recognise abnormal findings and manage them accordingly. Any pathology and treatments should be adequately described using recognised classification systems and documented. The size, number and location of lesions found, particularly if not removed, must be recorded and ideally supported with photodocumentation. The location should include the approximate segment and, where applicable, the distance from the anal verge.
1.3: Competence in flexible sigmoidoscopy includes the ability to identify and manage immediate and late complications of the procedure demonstrating effective clinical, endoscopic and non-technical skills (ENTS) to coordinate subsequent action
Evidence: Very low; Recommendation: Strong; Agreement: 100%
Although rare, the complications of FS may be serious, life altering or fatal. Complications may range from minor (eg, discomfort, vasovagal reactions), moderate (eg, cardiac abnormalities, effects of over sedation) or severe (eg, haemorrhage or colonic perforation).17 18 Perforation rates range between 21.9 per 100 000 cases (screening population) and 0.9 per 1000 (unselected cases),17 19 20 and are higher with therapy. Complications should be measured over the 30 days postprocedure and may be classified as intraprocedural, postprocedural (<14 days post) or late (>14 days).21 Endoscopists should be able to recognise complications promptly, apply effective clinical, endoscopic therapy and ENTS to initiate and coordinate appropriate management. In addition, competent endoscopists should demonstrate immediate leadership of the endoscopy team in managing the complication, appropriate communication with other teams if needed and duty of candour in discussions with patients and their next of kin.
1.4: Competent endoscopists should be able to recognise the adequacy of the endoscopic procedure performed and recommend subsequent action.
Evidence: Very low; Recommendation: Strong; Agreement: 96%
FS procedures are often performed in the UK with enema preparation and without sedation. The goal of FS is to examine as much of the distal colon as is required to answer the clinical question posed, as much as the the bowel preparation permits to be examined adequately (ideally to the splenic flexure) or to the limits of patient tolerance.22 Endoscopists should recognise the limitations of the procedure and exercise judgement and decision-making to recommend or arrange subsequent investigations to investigate the patient’s symptoms (ie, with repeat or alternative tests). This includes appropriate referral for colonoscopy based on FS findings.22
1.5: When sedation is used in FS, doses are within those defined by the current BSG colonoscopy guidance.
Evidence: Low; Recommendation: Strong; Agreement: 87%
Thresholds for safe sedation have been defined in the BSG colonoscopy guidelines.4 For patients aged <70, the median total dose in procedures where sedation is given should be ≤50 mg pethidine (≤100 μg fentanyl) and ≤5 mg midazolam (or equivalent drugs). For patients aged ≥70, the median total dose should be ≤25 mg pethidine (≤50 μg fentanyl) and ≤2 mg midazolam (or equivalent drugs). These are transferable to FS practice and should be adhered to in procedures where sedation is required.
1.6: Comfort scores in FS should be within those defined by the current BSG colonoscopy guidance.
Evidence: Low; Recommendation: Strong; Agreement: 96%
The BSG position statement on patient experience of GI endoscopy states that discomfort, pain and embarrassment during the procedure should be controlled and kept to a minimum.23 The BSG colonoscopy guidelines recommend that rates of moderate-severe discomfort should be <10%. We recommend that this KPI should apply to FS and measured using the 5-point modified Gloucester comfort scale,24 with nurse-reported scores of 4 and 5 indicating significant discomfort.
1.7: Competence in polypectomy should be based on achieving all competencies defined in the DOPyS form rather than a set minimum number of procedures.
Evidence: Low; Recommendation: Strong; Agreement: 96%
The DOPyS assessment form outlines all the individual competencies needed for the safe and effective resection of commonly encountered polyps. This covers technical and non-technical skills, and are different for sessile and pedunculated polyps. Competency in polypectomy does not correlate with other lower GI endoscopy KPIs and therefore assessment of competency should be driven by performance in DOPyS assessments as validated comprehensive polypectomy assessment tools.
1.8: Endoscopists should be able to competently document polyps using the Paris classification.
Evidence: Low; Recommendation: Strong; Agreement: 100%
In vivo assessment of colorectal polyp morphology enables decision making with regard to the appropriateness and mode of endoscopic therapy.25 The Paris classification provides standardised nomenclature for polyp morphology, classifying lesions to protruding (sessile, pedunculated, subpedunculated), flat (flat elevated or depressed) or depressed, although mixed morphology may be also present.26 The Paris classification can be predictive of submucosal invasion,27 with rates of submucosal invasion, with rates ranging from 1.4% for the most commonly observed lesions (Paris IIa granular), 7.5% (Paris 1s) to 31% for Paris IIc or IIa+IIc lesions.28 Paris classification therefore aids decision making with polypectomy and should be routinely used for the documentation of polyp morphology and be included in the endoscopy report.
1.9: Endoscopists should competently use at least one validated optical diagnosis system to classify and document polyps.
Evidence: Moderate; Recommendation: Strong; Agreement: 100%
Advancement of imaging techniques, new classification systems, and the use of artificial intelligence have lead to an increased viability for optical diagnosis of colonic lesions.25 To date, many classification systems have emerged (eg, Sano, Narrow-band imaging International (NBI) Colorectal Endoscopic Classification (NICE), JNET, SIMPLE, Kudo, Workgroup on serrAted polypS and Polyposis (WASP), BLI Adenoma Serrated International Classification (BASIC)) with some more widely used than others. Competency in validated optical diagnosis systems is critical in assessing the realtime malignant potential of polyps and therefore their immediate and further management.
Kudo et al first described five different ‘pit patterns’, according to mucosal surface seen by magnifying endoscopy, as a helpful tool to predict histology.29 Specific analysis of lesions with a Kudo type V pit pattern found a vastly higher incidence of malignancy than with other pit pattern types (56% vs 4.4% (pit pattern III) vs 5% (pit pattern IV) vs 0% (pit patterns I+II), n=479, p<0.001.29 The Sano classification was described in 2006 using NBI and was based on vascular patterns.30 In an attempt to simplify the process and make use of a more universal system, the NICE classification was created in 2009, based on lesion colour, vessel and surface pattern, and has been widely implemented.31
Although using the validated NICE classification for real time prediction of polyp histology for small lesions (<10 mm) was not superior to high definition white light endoscopy in a German RCT,32 data appraising the ‘resect and discard’ strategy showed that the use of NICE classification might prevent leaving in situ high grade adenomas or small invasive colorectal cancers.33 Further work has shown NICE to be a valid tool for predicting deep submucosal invasive carcinomas (SIMC) with overall sensitivity and negative predictive value of 92%.34 The modified Sano classification, additionally, has been found to outperform NICE for differentiating neoplastic polyps and predicting resectability in a previous RCT.35
In order to address differences in surface patterns in elevated and superficial lesions, the JNET classification was developed and validated as a tool for hyperplastic polyps, sessile serrated lesions (SSL), adenomas and SIMC but was less applicable for shallow submucosal cancers.36 37 To further differentiate lesions into hyperplastic, SSL or adenomatous, the WASP classification was developed which led to a sustained increased in accurate diagnosis especially for SSLs.38
The BASIC classification is based on blue light imaging and takes into account polyp morphology, crypt and vessel characteristics. It has high interobserver concordance and has been validated for diminutive colorectal polyps,39 with lesion recognition accuracy improving with training.40
1.10: Endoscopists competent in flexible sigmoidoscopy should be able to define the difficulty level of polypectomy using the SMSA scoring system.
Evidence: Low; Recommendation: Strong; Agreement: 96%
The SMSA scoring system comprises four factors which determine the complexity of a polypectomy; (S) Size, (M) Morphology, (S) Site and (A) Access.41 Application of SMSA divides complexity of polypectomy into four levels: level 1 (4–5), level 2 (6–8), level 3 (9–12) and level 4 (>12). Defining the difficulty level of polypectomy aids therapeutic decision making, correlates with adverse events and can avoid unnecessary repeat procedures.42 43 For larger polyps, the SMSA level can also determine the appropriate endoscopist and time slot allocation for a future polypectomy.
1.11: Endoscopists in flexible sigmoidoscopy should be competent to perform safe and effective polypectomy of SMSA level 1 polyps as a minimum.
Evidence: Low; Recommendation: Strong; Agreement: 100%
Within the UK Bowel Scope guidelines, the presence of adenomas ≥10 mm is an indication for colonoscopy to exclude proximal lesions.44 45 It is reasonable to expect endoscopists in FS to resect lesions <10 mm. As SMSA has replaced size criteria alone for evaluating difficulty of polypectomy (ie, level 1: <10 mm polyp; level 2: 10–20 mm polyp), competency in FS should include competency in SMSA level 1 polyps as a minimum. Where possible, resections should be complete and performed en bloc to facilitate histological assessment.
1.12: Endoscopists must be able to competently demonstrate safe and appropriate use of diathermy relevant to polypectomy.
Evidence: Low; Recommendation: Strong; Agreement: 100%
Cold snare polypectomy (CSP) is feasible for sessile polyps <10 mm and may result in lower rates of delayed bleeding.46 47 For SMSA level 1 polyps, diathermy is used for pedunculated polyps and in cases where CSP is not possible. Modern diathermy machines have automated energy delivery systems that simplify diathermy into two operator dependent variables: (A) pedal (yellow for blended cut with coagulation; blue for coagulation, (B) settings (current and effect size—which is often automated based on location and type of polypectomy). However, significant variation still exists in the use of diathermy for polypectomy among endoscopists.48 49 Pure coagulation current is favoured by some due to its efficient haemostatic properties but delayed bleeding can occur and prolonged use might cause deep thermal injury. Blended current alters the current and blend delivered according to tissue resistance and was thought safer due to the rationale that it provides adequate cutting with effective haemostasis although immediate bleeding may be observed.50 A recent RCT comparing the two diathermy modalities found no difference in risk of serious adverse events, complete resection rate or polyp recurrence.51
Trainees should have a basic understanding of the electrosurgical unit and diathermy settings needed for safe polypectomy. A recent UK survey identified practice variations and knowledge gaps in diathermy use which may not only affect safety in polypectomy but also the quality of training delivered to subsequent generations of endoscopy trainees.48 Understanding of diathermy should be supported through the JAG Basic Skills Courses and teaching should also be delivered during polypectomy hands on simulation, enabling assessment and development of trainees’ skills in a protected and safe environment.52
1.13: Endoscopists should be able to competently manage post-polypectomy perforation and bleeding using endoscopic clips and at least one other method of haemostasis while demonstrating relevant ENTS.
Evidence: Low; Recommendation: Strong; Agreement: 100%
Bleeding and perforation are the most common and serious complications of polypectomy. Endoscopists should be able to mitigate, recognise and manage such complications.53 Complication rates can be reduced through correct resection technique, optimisation of risk (eg, adequate submucosal injection for endoscopic mucosal resection or application of postresection mechanical clips) and the safe use of diathermy where indicated.54 Importantly, polypectomy must not be attempted for lesions outside the competence level of the endoscopist. Once resected, careful examination of the mucosal defect is important to check for deep mural injury, bleeding or residual polyp.
For postpolypectomy bleeding, haemostasis can be achieved in most cases with the use of through the scope (TTS) clips.55 Other common therapies include direct thermal therapy with coagulation forceps or snare tip coagulation and coagulation therapy with argon plasma coagulation. There are no direct comparative trials between clips and thermal methods and they should be applied as required in an individual case-by-case basis, although caution should be taken to avoid prolonged thermal therapy in the resection site for risk of delayed perforation.56 Over the scope clips,57 haemostatic powders58 and self-assembling matrix forming gels59 may also be considered, with interventional radiology or surgical intervention being options should endoscopic management fail.
For intraprocedural perforation, endoscopic closure is a safe and effective alternative to surgery and is thus the treatment of choice for select cases. In a systematic review of 24 cohort studies, successful closure was achieved in 90% of intraprocedural perforations using endoscopic methods.60
Although some skills might be acquired later with further experience and exposure, independent endoscopists should be competent with TTS clip placement and at least one other form of haemostasis. In addition to technical skills, demonstration of ENTS is also crucial to coordinate subsequent patient management.
Acquiring competence
2.1: Lower GI endoscopy training should take place in a unit that maintains its training environment to JAG standards.
Evidence: Very low; Recommendation: Weak; Agreement: 100%
The JAG accreditation standards for endoscopy services have set quality standards to ensure that all training centres deliver safe and effective training.61 Here, each trainee should have a nominated trainer who performs to BSG standards, has received appropriate training as an endoscopy trainer (Train the Colonoscopy Trainer course) and is assessed regularly by trainees and peers (trainee feedback and through Direct Observation of Training Skills). Training should be supplemented by access to recommended JAG courses, mandatory training (ie, mandatory basic skills courses), assessment and certification tools (JETS access) and appropriate supervision pre and post certification. Finally, each certified endoscopy unit should maintain a suitable environment and have policies in place to support training opportunities in line with a trainee’s personal development plan.
2.2: FS trainers should meet individual key performance indicators as defined by JAG and/or BSG.
Evidence: Low; Recommendation: Strong; Agreement: 100%
Trainers in FS should maintain their own competencies and safety standards in FS as defined by JAG or colonoscopy as defined by the BSG.4 All trainers should have attended a JAG approved Train the Endoscopy Trainer for example, Train the Colonoscopy Trainer course before they are assigned to a trainee. Adherence to these requirements should be assessed regularly with departmental policies in place to assist the individuals when necessary.
2.3: The training programme should include opportunities to gain experience and competencies in ENTS.
Evidence: Low; Recommendation: Strong; Agreement: 100%
The acquisition of higher ENTS competencies can lag behind the development of the technical skills of scope control and may be addressed through focused and structured ENTS training. In the RCT by Grover et al, structured simulation-based curriculum covering ENTS improved colonoscopy and integrative (ENTS) performance in novice trainees compared with self-directed simulator based training.62 An assessor-blinded RCT by the same group found that novice trainees exposed to a comprehensive non-technical skills curriculum (covering didactic teaching and case base scenario, virtual reality (VR) simulation, scenario training and specific non-technical skills feedback) demonstrated superior overall performance and ENTS ratings in their hands-on cases compared with the control group.63 Additionally, didactic teaching and multiprofessional in situ simulation training can be used to improve ENTS.12 64 65
2.4: Trainees in flexible sigmoidoscopy should attend a JAG approved Basic Skills in Flexible Sigmoidoscopy or Colonoscopy course during training.
Evidence: Low; Recommendation: Strong; Agreement:100%
2.5: Lower GI endoscopy trainees should apply for a JAG approved basic skills course at the start of LGI endoscopy training and attend this within their first 70 procedures.
Evidence: Low; Recommendation: Strong; Agreement: 91%
The Basic Skills in Colonoscopy course was implemented by JAG in response to poor performance demonstrated in the 2004 UK wide colonoscopy audit.6 66 Further, JAG Basic Skills in FS courses have also been developed. JAG approved training courses aim to standardise the delivery of endoscopy theory and hands-on techniques to all trainees. This ensures that all trainees receive essential skills training and enables them to continue skills development in their local units until certification. Hands-on endoscopy courses can lead to positive and sustained improvement on key areas of skills acquisition.67 An interrupted time series analysis found that attendance of the Basic Skills in Colonoscopy course results in a step-change improvement in performance in all trainees,68 but maximal benefit was found in trainees at earlier stages training (lifetime procedure count <70). We, therefore, advise that the course should be undertaken early in the individual’s training journey and preferably within their first 70 lower GI endoscopy procedures.
2.6: Virtual reality simulation training for endoscopic technical skills is encouraged in conjunction with conventional endoscopy training to enhance development of early endoscopic technical skills. Trainee simulator-based training should be directly supported by appropriately skilled trainers/supervisors.
Evidence: Moderate; Recommendation: Strong; Agreement: 91%
The use of VR simulators for endoscopy training has been well studied.69–73 Studies related to the impact of virtual FS specifically are less frequent and more dated than studies in other endoscopy modalities.74–76 Noting this, the three published studies vary in findings but are included in a large Cochrane database systematic review.72
In theory, VR simulators permit skills development in a protected environment without discomfort or harm to patients. Overall, simulators show good validity, can distinguish between competency levels, and can improve endoscopic procedure completion and mucosal visualisation compared with those who receive no training.77 The limited data from studies using VR simulators within FS improves patient comfort, shortens insertion time and improves measures of hand-eye skill measures.74–76 Within individual RCTs, VR simulation training improves colonoscopy completion rates in the first 10 patient-based procedures,78 and increase competency during the first 100 cases.79 While VR simulators are effective as a precursor to patient-based training, there is insufficient evidence for VR to replace early hands-on training or to count towards a trainee’s lifetime procedure count.
Regarding polypectomy, the optimal simulator approach has not yet been established. Interim results of a randomised trainee cohort study have failed to show a significant increase in DOPyS performance in the group that received specific augmented reality training in addition to conventional simulator based training.80 At present, it is unclear what proportion of polypectomy training should consist of cognitive didactics, use of simulation/ex vivo models, observation of experts or supervised hands-on polypectomy. There is a lack of robust data on the efficacy and effectiveness of training interventions which increase trainees’ competencies and this has led to practice variation in different institutions and countries.81 In a study of eight gastroenterology trainees who underwent a lecture based training which included basic principles of polyp characterisation, polypectomy technique, outcome and management of complications, the training did not result in improvement in overall competencies assessed by DOPyS.82 Different training methods such as educational videos are increasingly used and have demonstrated effect on the learning curve of polypectomy skills.83 Studies supporting the use of simulators for polypectomy are limited. The Welsh Institute for Minimal Access Therapy colonoscopy suitcase is an ex vivo porcine simulator for polypectomy that has shown content validity for training in polypectomy skills. The simulator was validated for snare polypectomy and correlated with the real-life level of expertise of the user.84
Training with GI simulators can increase early clinical performance but the optimal manner to deliver training is still under review. Feedback appears to be essential to derive benefit from simulation training.62 85 86 As such, simulation based training should be directly supported with coaching and feedback from appropriately skilled trainers to maximise efficacy.87 88
2.7: Training in polypectomy should start early during flexible sigmoidoscopy training and continue in parallel with this.
Evidence: Very low; Recommendation: Weak; Agreement: 100%
Trainees in FS should be competent in the resection of SMSA level 1 polyps. The group consensus was to encourage training in polypectomy early during FS training, using acquisition of scope handling competencies, particularly fine control of the scope tip, as cues to commence practical skills training in polypectomy. Trainees should acquire knowledge, assessment and management skills in lesion recognition as their training in FS commences and progresses. Practical training in polypectomy should not be deferred until competency in diagnostic procedures is achieved.
2.8: Polypectomy training should include skills acquisition in cold snare, hot snare and basic lift assisted polypectomy to a minimum of SMSA level 1.
Evidence: Low; Recommendation: Strong; Agreement: 100%
As SMSA level 1 competency is the minimum requirement for competency in FS, trainees should be familiar with all the different techniques that might be utilised in endoscopy to safely and effectively remove such polyps. Cold biopsy polypectomy (CBP) is a technique used for diminutive polyps (≤5 mm) but has been associated with high rates of incomplete resection (approximately 39%).89 The use of jumbo biopsy forceps appears superior to standard forceps for small sessile polyps although the efficacy remains questionable (78.8% vs 50.7%).90 Overall, CBP appears inferior to CSP, although resection rates may be similar in polyps <4 mm.91 92
CSP is favoured for small sessile lesions due to its safety profile. The CRESCENT study and a recent meta-analysis comparing CSP with hot snare polypectomy (HSP) for polyps <10 mm reported similar complete resection rates of 92%–98%, but lower delayed bleeding rates and shorter procedure times for the CSP groups.47 93 94 En bloc resection for lesions >10 mm is less feasible with CSP,95 96 although the lower residual polyp rates seen with SSLs compared with adenomas (1.1% vs 11%) indicate a selective role for piecemeal CSP.97 98
HSP is the main technique used for pedunculated polyps but also for larger lesions (>10 mm), especially adenomas, as part of a lift assisted polypectomy (endoscopic mucosal resection). It is associated with higher risk of perforation but also delayed bleeding depending on the current/setting used and type of polyp removed. Trainees should be aware of the strengths and weaknesses of each polypectomy method and apply these appropriately.
2.9: Trainees should receive training in the Paris polyp classification system and validated optical diagnosis systems. When available supportive web-based training tools should be utilised and any relevant modules completed prior to the basic skills course.
Evidence: Moderate; Recommendation: Strong; Agreement: 96%
Trainees should receive a structured training approach to gain competency in the use of the Paris polyp classification and at least one validated optical diagnosis system to classify and document polyps (statements 1.9 and 1.10). These could include NICE,32–34 99 Japan NBI Expert Team (JNET),36 99 Blue light imaging adenomas serrated international classification (BASIC)39 100 and the Workgroup serrAted polypS and Polyposis (WASP) classification38 to improve diagnostic accuracy of hyperplastic, adenomatous and malignant histology and to predict serrated histology. Other proposed classifications such as i-Scan Classification for Endoscopic Diagnosis (ICE) and Simplified Identification Method for Polyp Labelling during Endoscopy (SIMPLE) utilising the i-scan optical enhancement platform exist, but they have not been fully validated in clinical practice.101 Ideally, training in optical diagnosis should consider encompassing multiple endoscopic platforms. Analysis of post colonoscopy colorectal cancers (PCCRC) highlight that 89% of these can be avoided with 8% of cases being attributed to detected polyps in the area of subsequent cancer not being removed.102 This suggests inadequate lesion assessment (and subsequent decision not to proceed with resection) at the index procedure has an important role in development of these cancers.
Training modules can be didactic or web based and should include all commonly encountered lesions including hyperplastic polyps, adenomatous polyps, SSLs and cancer to allow effective implementation in clinical practice. Recently, Smith et al found no difference in diagnostic accuracy for the prediction of diminutive/small polyps between trainees assigned to didactic training and computer based training.103 The optimum mode of optical diagnosis training is therefore unclear.
Optical diagnosis training should be incorporated into the Basic Skills in Colonoscopy course with a combination of precourse self-study material and in-course discussions to enhance understanding. Systematic, feedback based training programmes have helped endoscopists with different levels of experience to develop high accuracy and good intraobserver agreement using the NICE classification,104 while in-class teaching and self-directed learning using a standardised educational tool for NICE criteria had similar results in accuracy of comparing adenomatous vs hyperplastic colonic polyps in a recent RCT.105
2.10: Appropriate discussion and reflection related to polyp classification and management should occur throughout training.
Evidence: Very low; Recommendation: Strong; Agreement: 100%
Polypectomy is a complex task that requires significant training time to acquire the relevant decision making and practical skills. Lesion recognition and description with appropriate application of Paris classification and optical diagnosis platforms is an important first step and requires continuous practice, case variation and adequate exposure. Management planning and decision making with regards to the optimal therapeutic approach for a lesion using the SMSA score along with all other non-technical skills around polypectomy are critical for a safe and effective resection technique. These discussions could precede hands-on technical skills experience and will aid future development. Regular feedback, use of DOPyS and reflective tools can facilitate these discussions.
2.11: Attendance at a hands on (tissue/tissue-like) model endoscopy course with exposure to differing polyp resection techniques, submucosal injection techniques, haemostatic therapy, polyp retrieval techniques and tattooing is encouraged.
Evidence: Very low; Recommendation: Strong; Agreement: 96%
Endoscopic training in therapeutics should start when the trainee has developed some early essential skills (basic tip control) and continue throughout their training. Procedures can harbour life threatening complications or be part of a high-risk clinical scenario, and prove challenging even in experienced hands.
One way to increase confidence of the trainee and to make the task safer is to deconstruct and learn the different steps of a new technique in a more controlled, less stressful environment of a hands on model course. The existing JAG accredited model courses; Hands-on Polypectomy Skills Course and the pilot Upper Gastrointestinal Haemostasis course run on this principle.
Supportive evidence for improvement in task competency is lacking although one RCT reported significant improvements in the performance of polypectomy, control of upper GI bleeding and oesophageal dilatation following a hands-on course.106 Additionally, a recent evaluation study of the 1-day BSG-JAG developed pilot haemostasis course in two centres showed that trainee confidence increased in both in their understanding and delivery of main therapeutic techniques in the management of upper GI bleeding.107
2.12: All parameters described in DOPS/DOPyS should be included during skills training.
Evidence: Very low; Recommendation: Strong; Agreement: 100%
The FS DOPS and DOPyS are formative assessment tools for diagnostic FS and polypectomy respectively which itemise specific competencies in sequential order.108 109 Each competency item is grouped within a domain, for example, preprocedure, procedural, management of findings, postprocedure and ENTS.108 All items covered within DOPS and DOPyS are necessary for competence (Statement 1:10) and should be covered during FS and polypectomy training.
2.13: A trainee should undertake a minimum of 175 flexible sigmoidoscopy procedures during their training to be eligible for summative assessment.
Evidence: Low; Recommendation: Strong; Agreement: 100%
In contrast to colonoscopy, the learning curve to competency in FS has been poorly studied. In order to ensure that all endoscopists achieve the breadth of FS exposure to different case complexities and pathology encountered, a minimum procedure number is necessary in line with other JAG certification modalities. This minimum number has varied within the literature. In North America, a minimum procedure count of 15–25 supervised procedures was initially recommended in the 1980s. This was increased by the ASGE to a minimum of 25 procedures before competency with 60 cm endoscopes was assessed. A 1999 study by Wallace et al on FS screening patients found no difference in intubation depth >40 cm and polyp detection rates between physician and non-physician endoscopists after 100 supervised procedures.110
The UK study by Siau et al based on FS DOPS assessments (N=468 trainees) found that 150–174 procedures were required to attain competency in >90% of DOPS competencies, although competencies such as ‘postprocedural skills’ required 175–199 procedures.108 The study did not factor in competency acquisition rates for SMSA 1 polypectomy. In another JETS e-portfolio analysis, FS certification was awarded to 194 trainees after performing a median of 262 supervised procedures (IQR 210–334).8
The group consensus was to mandate a minimum procedure count to 175 procedures (to include up to a maximum of 75 colonoscopy procedures) before competence may be assessed. In reality, it is expected that more procedures may be required to meet the competency demands laid out in this certification framework.
2.14: A trainee should have a minimum number of dedicated training lists as defined by the JAG training standards.
Evidence: Very Low; Recommendation: Strong; Agreement: 100%
Current JAG training standards state that each trainee should have a minimum of 20 dedicated training lists a year in addition to access to ad hoc training opportunities.61 With impending changes to structure of medical training, on-call rotations, dual accreditation commitments and the minimum procedure count of >175 procedures for certification, ensuring adequate training opportunity is important for trainees to achieve their certification during training. Increased availability and attendance of endoscopy training opportunities will be required to achieve this goal during specialty training where appropriate.
2.15: It is recommended that a trainee should receive a minimum of one DOPS per training list.
Evidence: Low; Recommendation: Weak; Agreement: 96%
DOPS assessments were developed to standardise skills assessment in a structured approach, to facilitate feedback provision and to support the certification process. They provide formal objective evidence of skills acquisition for both technical and non-technical skills.111 112 Accurate regular assessment of a trainees’ performance when learning a new skill can help them reach their full potential,113 while delivering constructive feedback after a procedure can stimulate reflection and enhance learning.114 For training programmes, DOPS help to identify areas for improvement and when performed at regular intervals can be used to chart competency development. Indeed, the lifetime colonoscopy DOPS count is an independent predictor of procedural competency.108 The updates to DOPS forms in 2016, which incorporated ENTS and a change in scoring format from a performance-based scale to a supervision-based scale improved the validity of these assessments.16
The updated requirements for certification include a minimum of 15 mandatory formative DOPS (approximately 1 per 10 procedures). For pragmatism, we advise a minimum of one DOPS per training list to guide feedback and future learning objectives.
2.16: It is recommended that a minimum of one DOPyS should be completed for every training list where a polypectomy has been attempted by a trainee.
Evidence: Low; Recommendation: Weak; Agreement: 96%
Similar to DOPS (statement 2.18), DOPyS should be performed regularly to chart competency development in polypectomy.109 Although DOPyS assessments should ideally be completed after every polypectomy performed to enhance performance, this may not always be feasible due to time restraints. Where applicable, we advise at least one DOPyS per training list where a polypectomy has been attempted.
2.17: Trainees must complete a reflection tool on JETS every 50 procedures. This forms a framework for meetings with their endoscopy supervisor every 6 months or less.
Evidence: Low; Recommendation: Strong; Agreement: 100%
Reflective practice is encouraged in the General Medical Council standards for good practice and forms an important aspect of the portfolio within the HEE Clinical Endoscopist accelerated programme for endoscopy training. It empowers practitioners to develop self-awareness and insights on their strengths and weaknesses, optimises the learning process, consolidates practice and identifies opportunities for improvement.115 Trainees are encouraged to reflect on their clinical practice, endoscopic skills, interesting cases, ENTS, complications, etc using the JETS ‘‘‘Reflection Tool’ at least once every 50 procedures. In line with GMC recommendations, this is one of the new requirements for endoscopy certification which should be reviewed by the endoscopy trainer during appraisal meetings.
Assessment of competence
3.1: DOPS should be used as the competency assessment tool in lower gastrointestinal endoscopy.
Evidence: Low; Recommendation: Strong; Agreement: 100%
The FS DOPS assesses 24 individual competencies under 5 broad domains (7 preprocedure; 8 procedure; management of findings; 2 postprocedure; 4 ENTS).108 It shares the same structure as the colonoscopy DOPS and includes a supervision-based scoring scale and an ENTS section.116 117
Although other competency assessment tools have been developed internationally for colonoscopy,77 112 118 119 these lack validation for FS. Previously, an assessment tool with six generic and four specific technical skills presented by Sarkar et al showed moderate reliability (Cronbach alpha: 0.79–0.81), with scores correlating with experience.120 Another competency assessment tool by Thomas-Gibson et al applied video assessment of FS extubations in FS screening practitioners to evaluate skills based on overall competence and five individual domains: time spent viewing mucosa, re-examination of poorly viewed areas, suctioning of fluid pools, luminal distension, and lower rectal examination. This assessment tool demonstrated good reliability and was able to distinguish between endoscopists with different adenoma detection rates.121 The Resident Practice Audit in Gastroenterology (RPAGE) instrument assesses professionalism, interpretation of data, patient safety, knowledge, independence and technical skills, in addition to an overall score, and is being evaluated in Canada.122
As endoscopy trainees and trainers in the UK are familiar with DOPS, we recommend the continued use of DOPS as the default formative and summative assessment tool during FS training.
3.2: Each formative DOPS should be performed on a single preselected case.
Evidence: Low; Recommendation: Strong; Agreement: 91%
Endoscopy skills should be demonstrated across a breadth of different scenarios and with different case difficulties to ensure competency across a range of case contexts.112 DOPS assessments can be initiated by either the trainee or trainer but should be prospectively selected to minimise selection bias.
3.3: The last five DOPS prior to summative assessment must be rated competent without supervision in >90% of all items, with none requiring maximal or significant supervision.
Evidence: Low; Recommendation: Strong; Agreement: 96%
DOPS performance can be used to gauge readiness for summative assessment. Competent performance in FS DOPS should be demonstrated in more experienced trainees who have met or are approaching eligibility requirements for summative assessment. Trainees should be competent in >90% of items assessed in DOPS,108 with up to 10% of items scoring ‘minimal supervision’ and no items rated as requiring ‘maximum supervision’ or ‘significant supervision’’.
3.4: DOPyS should be used as the polypectomy competency assessment tool for both technical and non-technical skills.
Evidence: Low; Recommendation: Strong; Agreement: 100%
DOPyS is a validated polypectomy assessment tool for colonoscopy and FS,109 which has been endorsed by the US Multi-Society Task Force (USMSTF) on colorectal cancer.123 The use of DOPyS improves trainees documented exposure to therapeutic endoscopy, provides formal evidence of polypectomy skills acquisition and serves as an effective tool for assessing and certifying polypectomy in the UK.111 DOPyS was also used by Patel et al in the validation of Cold Snare Polypectomy Assessment Tool (CSPAT), which was developed specifically for CSP.124
3.5: For competence at SMSA level 1 polypectomy, a minimum of 2 SMSA level 1 DOPyS should be competently performed using the following methods: cold snare polypectomy, diathermy-assisted resection of stalked polyps and diathermy-assisted EMR. The last four DOPyS (level 1) should score ‘competent for independent practice’ in all items.
Evidence: Very low; Recommendation: Strong; Agreement: 100%
Statement 2.9 highlighted the importance of applying the correct method for polypectomy according to the size and type of the polyp to reduce risk and improve outcomes, including mitigating PCCRC.125 These techniques might be required to remove an SMSA level 1 polyp and thus trainees need to demonstrate competence in each modality. A systematic review on the learning curve for polypectomy based on ‘independent en bloc resection’ and delayed post polypectomy bleeding rate suggests that 250–400 polypectomies are required.126 The I-DOPyS study suggested a median of 15 polypectomies to achieve competence in CSP.127
We recommend a minimum of 2 assessments for SMSA level 1 polyps at the standard of ‘competent for independent practice’ for each modality (CSP, diathermy assisted resection of stalked polyps and diathermy assisted EMR). In total, this constitutes a minimum of 6 competent DOPyS for SMSA Level 1 polyps with the four most recent SMSA level 1 DOPyS scoring ‘competent for independent practice’ in all items.
3.6: Eligibility for summative assessment in FS may be triggered once the following are met:
Minimum FS procedure count of 175 (including colonoscopy numbers).
Meeting minimum KPIs over the preceding 3 months, that is, rectal retroflexion ≥90%, polyp retrieval rate ≥90%, moderate-to-severe discomfort ≤10%.
Physically unassisted procedures ≥90%.
≥15 procedures over the last 3-month period.
Attendance of JAG Basic Skills in Lower GI endoscopy course.
Meeting formative DOPS and DOPyS requirements.
Minimum of 15 formative DOPS.
Last 5 DOPS rated competent without supervision for 90%+ of all items.
Evidence of competency in SMSA level 1 polypectomy.
Engagement with the JETS reflection tool (minimum of 3 reflection entries).
In addition to DOPS, JAG certification adopts the use of minimum procedural numbers and KPIs from self-reporting methods to inform readiness for summative assessment. The KPIs for competent practice are aligned with trainee-relevant metrics featured within the UK colonoscopy quality standards (Statement 1.1). In line with previous JAG certification criteria,128 KPIs will continue to be measured over the last 3 months with a minimum of 15 procedures to enable sufficient practice volume to gauge performance. The eligibility criteria for summative assessment reflects the requirements described within this document.
3.7: For successful completion of the summative DOPS assessment, the trainee should be rated as ‘ready for independent practice' in all items within 4 DOPS by a minimum of 2 different assessors who are not the trainee’s usual trainer.
Evidence: Low; Recommendation: Strong; Agreement: 100%
To ensure objectivity of summative assessment, JAG had traditionally mandated DOPS to be scored by assessors who are not the trainee’s usual trainer (defined as the dedicated named trainer allocated to the trainee during their attachment who supervises most training lists), involving a total of four summative DOPS performed within a 1-month window. This could involve different permutations, that is, as a 2+2 process simultaneously (2 assessors over 2 cases), as a 2+2 process sequentially (2 assessors over 4 cases), as a 2+1 + 1 process (3 assessors over 4 cases), as a 1+1 + 1 + 1 process (4 assessors over 4 cases) or as a 3+1 process sequentially (2 assessors over 3 cases).
Although there are data suggestive of the role for distant supervision, that is, through magnetic endoscopic imager configurations,129 video recordings,67 130 or live video transmissions on tablet devices,131 these are currently insufficient to be recommended as alternatives to directly observed assessments within the same room due to their limitations with ENTS assessments.
Post-certification support
4.1: Newly certified endoscopists should have access to a named individual and meet on a regular basis to discuss cases and to review progress.
Evidence: Very Low; Recommendation: Strong; Agreement: 96%
The transition between supervised training and newly independent practice can be a challenging period and may be the first opportunity to undertake practice without an in-room trainer. Most newly certified practitioners will require a defined period of supervision (eg, 1 year) and ongoing endoscopy exposure to achieve the outcomes of an experienced practitioner.132 Assigning a named individual to meet regularly with a newly certified endoscopist to review progress and to discuss any clinical and non-clinical challenges faced during this period offers support and allows a relationship of trust and rapport to develop. Instances where such support may be beneficial may include: review of photodocumentation (and indeterminate lesions), postprocedural management plans, therapeutic decision making. Such meetings should be conducted on a regular basis, to safeguard patient management and to facilitate skills development for the newly independent practitioner. The supervisor should possess valid credentials (appropriately experienced with competent KPIs) and have attended a Train-the-Trainer’s course.
The recent implementation of the UK National Endoscopy Database enables procedural data to be uploaded to a centralised server to benchmark an endoscopist’s KPIs against national quality standards.133 In accordance with JAG QA standards,61 performance data of all independent endoscopists should be reviewed at regular intervals to enable practitioners to discuss queries, concerns, raise issues with caseload or time management, and to receive support and upskilling where necessary. This should also include plans for support if underperformance is self-reported or observed during the newly independent period, in line with JAG guidance.134
As part of professional development, training requirements of newly certified endoscopists should be identified, discussed and recorded on an individualised personal development plan. For FS, this could include mentored lists (statement 4.4) to improve specific technical or non-technical skills or upskilling to colonoscopy.
4.2: Endoscopy departments should have systems in place to ensure appropriate list size and caseload selection for newly certified endoscopists.
Evidence: Very Low; Recommendation: Strong; Agreement: 96%
The path from competent to high-quality practice involves an ongoing learning curve postcertification. Newly certified endoscopists need to be able to demonstrate all the appropriate technical and non-technical skills without a trainer in the room which can increase their mental workload and might lead to longer times to complete a test safely. Data from Siau et al showed that after colonoscopy certification, 18% of trainees had a dip in performance (CIR <90%) in their first 50 procedures, which improved after 100 additional independent procedures.132 Endoscopy departments should allow for adjustments on the lists of the newly independent endoscopists with reduced caseload if applicable, for example, for the first 6 months, to encourage familiarisation with independent practice and as confidence develops. It is advisable for progress to be reviewed by the named individual assigned to the newly certified endoscopist (statement 4.1) and if applicable, to review caseload after the transition period.
4.3: Certified endoscopists should perform at least 100 procedures a year to maintain competence.
Evidence: Very Low; Recommendation: Weak; Agreement: 100%
Performing a minimum annual volume of endoscopy procedures helps to maintain competence and is associated with improved patient outcomes.135–137 Previously, an international taskforce on FS screening called for a minimum number of procedures per year to maintain competency, although this number was not specified. The BSG recommends a minimum of 100 colonoscopies per year with an aspirational standard of 150 procedures per year to be undertaken by the endoscopist or directly supervising a trainee in the room.4 We, therefore, recommend a minimum of 100 lower GI procedures per year (to include FS and colonoscopy procedures) to maintain competence in FS.
4.4: Certified endoscopists should have access to mentored lists.
Evidence: Low; Recommendation: Strong; Agreement: 91%
Within the Bowel Cancer Screening Programme framework on mentorship and QA, a mentor is defined as ‘a trusted counsellor or guide’. It is important for new certified endoscopists to feel supported by their department and be given access to mentored lists for a defined period, for example, first 6 months, after certification. A mentored list may involve a colleague with expertise either observing the newly independent endoscopist or vice versa. This can be useful to facilitate ongoing training, reflective practice and upskilling during this transition period, for supporting underperformance, or for imparting Train-the-Trainer skills to those who wish to eventually train others. Such an approach can also improve career satisfaction and mitigate burnout.138
Discussion
This document provides a robust evidence-based framework for training, assessment and certification in FS in addition to measures during the early postcertification period to support the transition from trainees into independent practitioners (summarised in figure 1). Where evidence has been sparse, statements integral to training and certification have been sourced from expert consensus.
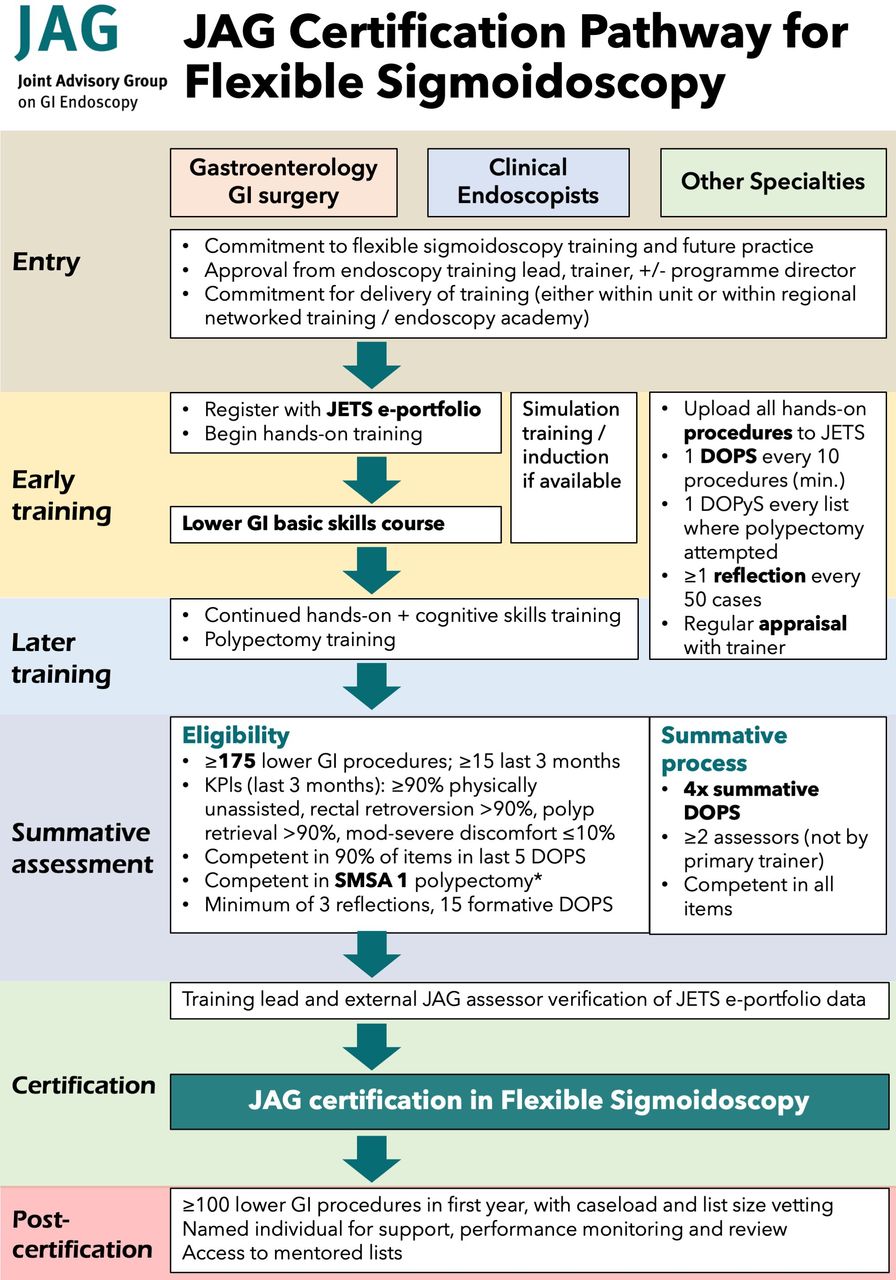
{kind=link}
Summary of the JAG certification pathway in flexible sigmoidoscopy.* ≥90% rectal retroflexion; 90% polyp retrieval, ≤ 10% mod/severe pain); **Minimum of 2 DOPyS demonstrating competency in each of cold snare polypectomy, diathermy-assisted resection of stalked polyps and diathermy-assisted endoscopic mucosal resection for SMSA Level 1 polyps.
Competency endpoints will continue to be measured through a combination of KPIs (via NED/JETS e-portfolio), DOPS assessments, and with a minimum procedural number of 175 procedures as a competency safeguard. A minimum competency standard of SMSA level 1 polypectomy has now been defined. Where relevant, KPIs have been aligned with those derived from the UK quality standards in colonoscopy and JAG standards which form the competency benchmark.
The eligibility criteria for summative assessments have now been updated in line with latest evidence and with an emphasis towards competence in polypectomy. These include the following: (1) competence in SMSA level 1 polypectomy has replaced the previous requirement of polypectomy of lesions larger than 10 mm and (2) additional emphasis on DOPyS for SMSA level 1 polyps. With the increasing evidence on the value of feedback through formative assessments, DOPS and DOPyS are now recommended for each dedicated training list. Active reflection is encouraged and included within the certification criteria. The JAG certification pathway is summarised in figure 1.
We acknowledge that additional training and support may be required for trainers with the introduction of this curriculum. Some of the standards, for example, characterising lesions by SMSA classification, use of at least one validated optical diagnosis system, undertaking DOPS and DOPyS assessments may be a challenge for existing trainers. While these are already covered in JAG Train-the-Trainers courses, trainers should familiarise themselves with this document and identify trainer development needs that may be bridged through self or peer-assisted learning.
The recommendations for training and competency acquisition have been laid out to include evidence-based interventions which have been shown to benefit competency development, much of which is surmised from the colonoscopy literature. This is particularly relevant with the incoming Shape of Training reforms and with disruptions to training due to the COVID-19 pandemic where training in lower GI endoscopy has been particularly affected.139 Specialty training programmes in the UK should ensure adequate endoscopy training provision, including the availability of fellowships, or if required, the continued access to training during the post-CCT period. It is hoped that this updated certification pathway will ensure that patients can expect to receive high-quality care from the newly independent endoscopist.
Ethics statements
Patient consent for publication
References
Footnotes
Twitter @drkeithsiau, @susi_green, @pelicanhere, @SiwanTG
Contributors Conception: KS, AM. DELPHI design: KS, AM. Literature searches: All authors. Electronic voting: All authors. Manuscript draft: All authors. Critical review and approval of final version: All authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests ER has received research funding from Medtronic.
Provenance and peer review Not commissioned; externally peer reviewed.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Linked Articles
- Commentary