Article Text

Abstract
Understanding and addressing patient attitudes to their care facilitates their engagement and attendance, improves the quality of their experience and the appropriate utilisation of resources. Gastrointestinal endoscopy is a commonly performed medical procedure that can be associated with patient anxiety and apprehension. Measuring patient attitudes to endoscopy can be undertaken through a number of approaches with contrasting benefits and limitations. Methodological validation is necessary for accurate interpretation of results and avoiding bias. Retrospective post-procedure questionnaires measuring satisfaction are easily undertaken but have limited value, particularly in directing service improvements. Patient experience questionnaires indicate areas of poor care but may reflect the clinician's not the patient's perspective. Directly assessing patient priorities and expectations identifies what is important to patients in their healthcare experience (patient-reported value) that can also provide a basis for other forms of evaluation. Published studies of patient attitudes to their endoscopy procedure indicate the importance of ensuring that endoscopists and their staff control patient discomfort, have adequate technical skill and effectively communicate with their patient relating to the procedure and results. Environmental factors, including noise, privacy and the single-sex environment, are considered to have less value. There are contrasting views on patient attitudes to waiting times for the procedure. Implementing patient-centred care in endoscopy requires an understanding of what patients want from their healthcare experience. The results from available studies suggest implications for current practice that relate to the training and practice of the endoscopist and their staff.
- ENDOSCOPY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
“If quality is to be at the heart of everything we do, it must be understood from the perspective of patients.” Darzi next stage review1
Why is understanding patients’ attitudes important for healthcare
Understanding patients’ attitudes towards their care is essential to improving the quality of their clinical experience.1 It promotes dialogue between services users, providers and purchasers,2 provides patients with ‘voice’3 ,4 that empowers them in making healthcare choices, can direct service reconfiguration5 ,6 and incentivises quality improvements.
There is an established association between meeting patient expectations of their clinical management and higher levels of satisfaction.7–10 High patient expectations prior to intervention and a perception that they have been met are both associated with increased likelihood of treatment compliance9 ,11 ,12 and improved clinical response,10 ,13 ,14 and, conversely, failing to meet patients’ expectations is associated with reduced satisfaction with their healthcare.15 Moreover, for care to be patient centred, clinicians should seek and respect patients’ views on how they wish to be managed, see them as partners in shared clinical decision making—the basis of “no decision about me without me”16—and as the basis of the informed consent process. Finally, understanding and recognising patients’ attitudes to their care is essential to avoid procedures or other interventions that patients do not wish to undergo, that can lead to unnecessary management and cost and potentially detrimental effects on patients’ relationship with their healthcare providers.17
How do we define and measure patient attitudes to their care?
Patients’ attitudes to their care can be defined from a number of perspectives (box 1). Satisfaction studies are simple, quantitative questionnaire-based evaluations of the patient journey or its component steps. This information may indicate the need for further assessment, but does not indicate where improvements should be made. Moreover, expressing satisfaction is a multifaceted and individual-dependent response with questionable validity.18 Published studies of patient satisfaction are commonly associated with poor methodology and are therefore of limited value.19
Defining patient attitudes to healthcare
Preferences: ideas on what should occur during clinical management;20 reflects patient choice or priorities (of individuals or a population).5 ,6
Expectations: beliefs on what should occur (normative) or what will actually happen, irrespective of what is desired (predicted).6
Evaluations: opinion of a healthcare experience, for example, satisfaction rating.20
Reports: objective reflection of a healthcare experience, for example, what actually happened.20
By comparison, patient experience studies (reports) can comprehensively assess a range of aspects of patient care at an organisational or wider level and can identify areas of poor practice or where potential improvements could be made.21 The results of large-scale studies such as national patient postal surveys,22 however, may be misleading as they are based on the assumption that participating patients are representative of the wider population and that lessons are generalisable across different environments and specialties, which in both cases may result in bias.
Patient-reported experience measures (PREMs) are generic, self-reported evaluations used to assess an individual patient's response to any aspect of a single healthcare event within a single organisation or specialty. These can provide specific information on the patient experience,23 contrasting with patient-reported outcome measures that address clinical response to an intervention.24 However, in both large-scale patient studies and PREMs, measures of experience may be based around evaluating aspects of care that clinicians consider to be important (or propose that patients consider important) and that may inaccurately reflect the attitudes of patients themselves.
Studies evaluating the healthcare experience may be more relevant where they are based on patient-reported preferences and expectations that identify the aspects of their care that they consider to be important in their clinical management25 ,26 or ‘patient-reported value’. The results of such studies can be used at a group or individual level to determine whether patient priorities in their care were met, where services can be improved and indicate how services should be redesigned. Addressing patients’ preferences and expectations positively influences their opinions of the healthcare they receive, their engagement with doctors and clinical management and is a measure through which the performance of the clinical service can be assessed.27
A number of generic frameworks have been developed that aim to assist clinicians in managing patients around their attitudes to their care. These include The Point of Care programme based on the Institution of Medicine's definition of patient-centred care28 and the Picker Institute's eight quality dimensions reflecting the care domains most important to patients (eg, highest ‘value’ from a patient perspective)29 (box 2).
Picker Institute quality dimensions reflecting the care domains most important to patients29
Fast access to reliable health advice
Effective treatment delivered by trusted professionals
Participation in decisions and respect for preferences
Clear, comprehensible information and support for self-care
Attention to physical and environmental needs
Emotional support, empathy and respect
Involvement of and support for family and carers
Continuity of care and smooth transition
Why is understanding the patient experience in endoscopy important for endoscopists?
Endoscopy describes a set of invasive medical procedures indicated for diagnostic investigation, therapy, surveillance and screening of a wide range of disorders of the gastrointestinal (GI) tract, including benign, premalignant and malignant conditions. These are commonly performed in the UK, with over half a million gastroscopies alone per year,30 equating to approximately 1% of the population31 and that is likely to increase with the introduction of the UK's national flexible sigmoidoscopy colorectal cancer screening programme.32
Developing an understanding of the patient-reported experience and value in the endoscopy process is important for both patients and clinicians. It is essential to facilitating patient engagement with their care, addressing their preprocedural anxiety and tolerance of the procedure33 and improving the overall quality of the healthcare experience. Failure to recognise such factors may adversely influence patients’ subsequent re-engagement with clinical management34 that includes willingness to attend or reattend for endoscopy.35 This may therefore determine the effectiveness of bowel cancer screening or surveillance programmes.36 The experience of individual patients may also influence the attitudes of other future or potential patients in engaging with endoscopy, through informal discussions with friends, family or acquaintances, formal networks or social media, particularly where this reflects reporting of negative experiences, as procedures to ‘be feared’.37
Furthermore, endoscopy is a resource-associated intervention and associated with significant costs. Failing to address patient expectations may lead to two sources of potential waste. First, unattended appointments that may reflect patients’ concerns over the procedure, and second in those who undergo procedures but would prefer not to (although this has different implications for benign and potentially malignant disease).17
The Global Rating Scale (GRS) was developed by the Joint Advisory Group on Gastrointestinal Endoscopy (JAG) to evaluate and accredit units which perform endoscopic procedures.38 JAG has emphasised the importance of the patient ‘experience’ within the organisation of the patient pathway and developed the GRS based around a ‘patient-centred’ service for endoscopy (box 3). One of the four domains of the GRS relates to the patient experience and includes an assessment of patient comfort, privacy and dignity, post-procedure care and opportunity for feedback. The mandatory inclusion of patient-reported evaluations of their experience in a specialty-based regulatory and accreditation framework was groundbreaking when introduced and the GRS has now become an internationally respected and recognised system.
Patient-centred standards from the Global Rating Scale (GRS) (clinical quality)38
Appropriateness
Information/consent
Safety
Comfort
Quality
Timely results
Quality of patient experience
Equality
Timeliness
Choice
Privacy and dignity
Aftercare
Ability to provide feedback
Methodology in studies of patient attitudes in endoscopy
Many methods for assessing patient experience of endoscopy have been used and reviewed elsewhere.39 These commonly demonstrate poor validation processes and use clinician-derived domains and data interpretation, even though patient assessment of ‘value’ within the procedure may differ considerably.39 For example, Yacavone compared patient and clinician ranking of aspects of the endoscopic procedure in terms of importance for obtaining patient satisfaction (1=most important, 15=least important). This noted that endoscopists overemphasised the importance of the ‘wait for endoscopy appointment’ (9.8 vs 11.5) and ‘waiting time before procedure’ (7.2 vs 10.5). By comparison, patients attributed relatively higher importance to physician and nurse knowledge of medical history (6.8 vs 9.7), physician discussion with primary physician (8.8 vs 12.8) and physician discussion after the procedure (7.1 vs 10.4).40 One measure of patient experience that has been subject to a validation process, a Canadian and UK-based study41 was based on clinician not patient-derived domains. Furthermore, the chosen domains of the GRS were selected from focus group studies of clinical staff not patients with only a single small Scottish focus-based study proposing (content) validation.42 This lack of validation in published quality and accreditation frameworks suggests that results should therefore be interpreted with care (as discussed above).
A further cohort-related factor that may introduce bias into results and should therefore be considered reflects demographic characteristics of recruited patients2 (sampling bias). For example, elderly patients commonly demonstrate higher levels of satisfaction (particularly if familiar with healthcare prior to the National Health Service), a finding that is also associated with female gender. Female and younger patients also have increased preprocedure concerns (16% vs 8%); however, ‘concern over the diagnosis’ demonstrates a converse relationship,43 also influenced by educational status.44 In addition, acquiescence bias may result from involvement of members of staff or untrained interviewers in the evaluation process, leading to false-positive feedback (for this reason, it may be an advantage for independent trained staff or lay assistants to collect feedback).18 This may also explain the more negative patient reports of their experience from postal surveys compared with those questioned face to face or over the telephone,45 for example, patients not reporting negative experience to a staff member who is perceived to be involved in that patient's future care. Finally, two other potential sources of bias include, first, the use of sedation that has an amnesic effect influencing patients’ memory and therefore satisfaction with their procedure.46 Second, the timing of the evaluation that leads to a more positive reported experience if undertaken sooner after the procedure.45
Assessing patient satisfaction in endoscopy
A number of quality assessment studies of endoscopic management have been undertaken47 with assessment of patient experience commonly as a secondary outcome but demonstrating a relationship to the quality of clinical care.48 Others that have focused on the patient experience in endoscopy have included that by Ko et al49 who surveyed 261 Canadian patients using a modified score based on the Group Health Association of America 9-item system (mGHAA-9—a questionnaire on satisfaction) with a number of question with Likert-style responses. A total of 87% (226/261) of patients were satisfied overall and only 1% (3/261) considered their experience dissatisfying. Positive factors related to satisfaction included the personal manner of the doctors and nurses and endoscopists’ perceived technical skill. The physical environment and time with the doctors discussing the diagnosis were also important. The authors noted that “the patient's perception of the endoscopist's technical skill was highly confounded by the endoscopist's personal manner”. Seip et al50 assessed patient satisfaction among patients undergoing upper GI endoscopy, suggesting high levels of satisfaction overall with dissatisfaction related to abdominal discomfort, with no significant effect of sedation on scores. Drossman et al43 reviewed patient concerns prior to endoscopy noting the importance of diagnoses, particularly malignancy, and discomfort during the procedure. Finally, Del Rio et al51 noted the association between dissatisfaction with waiting times and inadequate explanation of the procedure to the patient. A study of day surgery more generally demonstrated a relationship between dissatisfaction and prolonged times between admission, operation and discharge and postoperative pain.52
Determining patient priorities, expectations and reported value in endoscopy
Patient priorities, expectations and patient- reported value in endoscopy have been described in a number of studies. Yacavone et al40 also used a mGHAA-9 survey and an extensive validation process to measure patient satisfaction with endoscopy among 437 patients undergoing various procedures. A 15-point ranking scale allowed patients to list the aspects of the endoscopy experience from most to least important in leading to a satisfactory experience. The study identified factors considered by patients to be important in obtaining a satisfactory experience as technical skill and personal manner of the endoscopist, control of discomfort and personal manner of support staff/nurses. By comparison, low levels of importance in obtaining a satisfactory experience were associated with waiting time for the endoscopy appointment, waiting time preprocedure and explanations and noise level in the examination room.
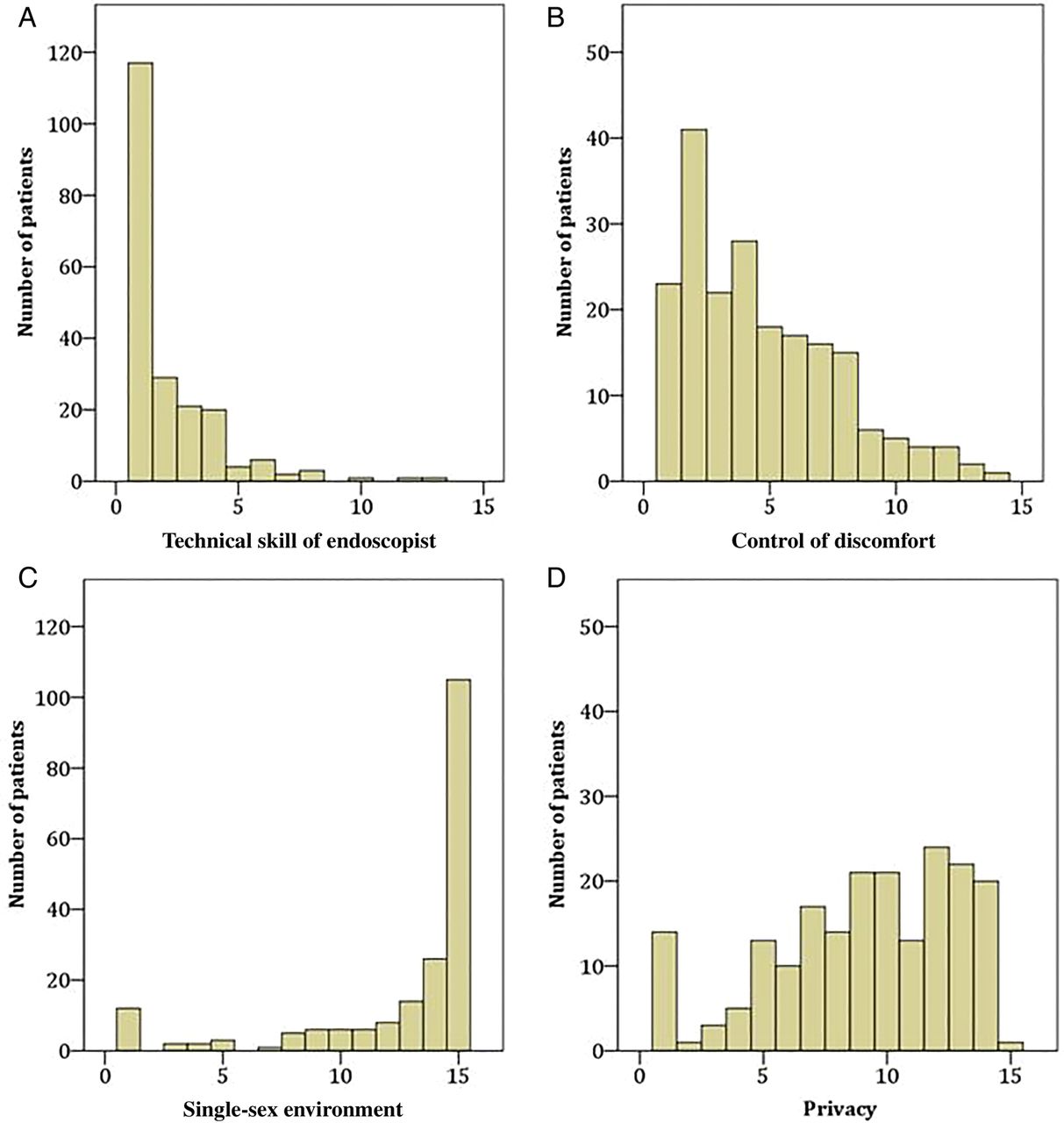
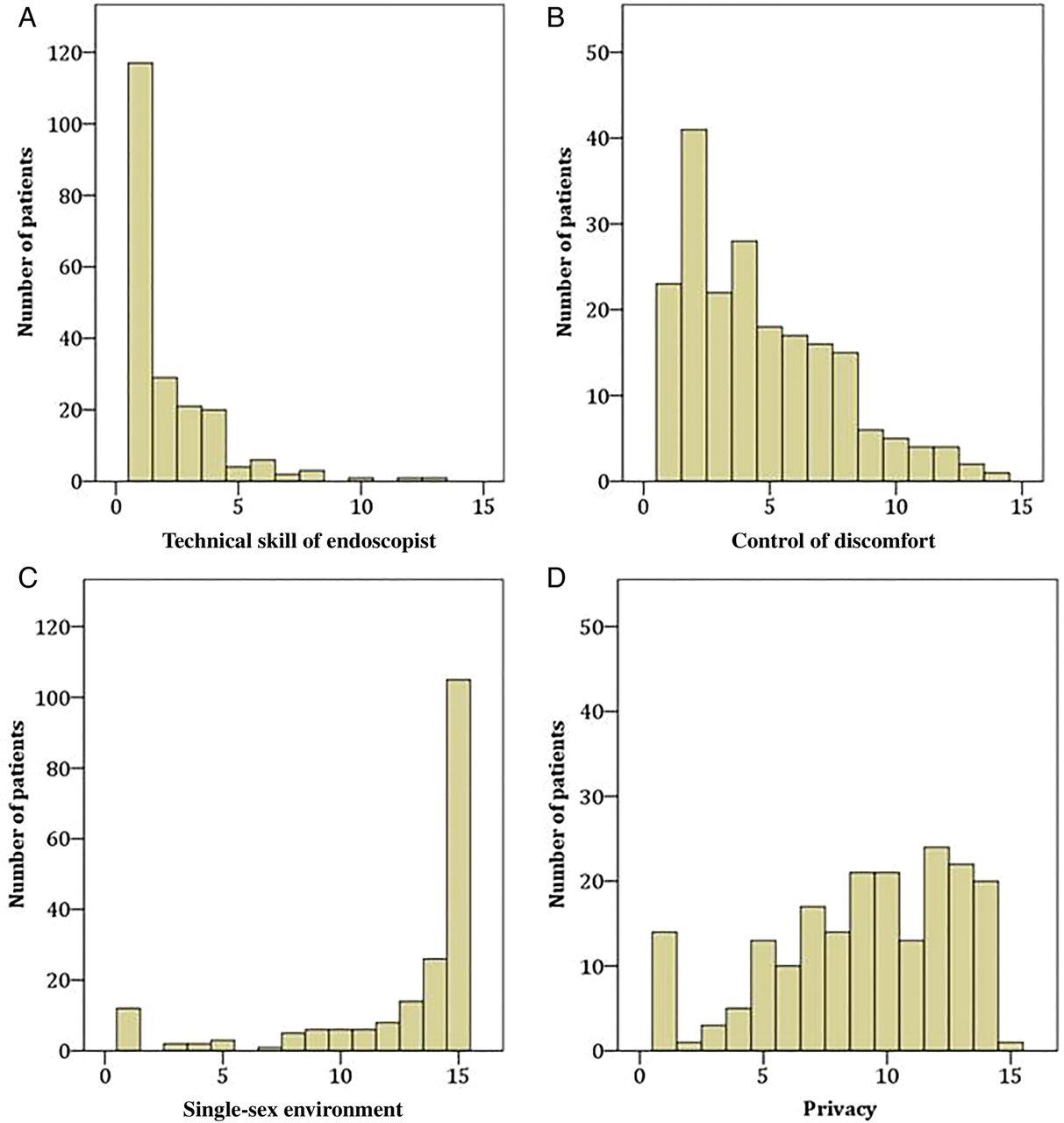
A similar ‘ranked prioritisation’ methodology was used by Hydes et al53 in a preprocedure survey of patient attitudes to unsedated upper GI endoscopy with similar findings (table 1). Comparisons of patient subgroups post-procedure or with previous endoscopy history demonstrated no difference in outcomes. A follow-up study by McEntire et al54 used the same methodology to assess patient attitudes to colonoscopy again with similar findings, identifying technical skills and personal manner of the endoscopists and the control of discomfort as most important with the lowest levels of value accorded to single-sex environments, noise and privacy (figure 1).
Patient responses (n=202) to a ranking questionnaire of individual aspects of care considered important for obtaining satisfaction with the upper gastrointestinal endoscopy experience*53
{kind=link}
Preprocedure patient ranking of aspects of their care important for obtaining satisfaction with their colonoscopy experience (1=high, 15=low for importance) (adapted from McEntire et al).54
Implications for practice
Modern clinical practice has increasingly focused on patients’ attitudes to their healthcare. The direction of endoscopy services by clinicians in the UK has been at the forefront of this approach, now involving formal accreditation of centres through the use of a quality assurance framework based around the patient experience. The focus of further development should be on developing patient-centred care but clearly from the patient's perspective. This requires an understanding of what patients want or value from their endoscopy experience.
Evaluating patients’ expectations and preferences of their care indicates their priorities, for example, what is of ‘value’26 in their journey from their perspective. Studies of patient-reported value repeatedly identify the importance of the practitioner–patient interaction and specifically, the endoscopists’ technical skill (including the ability to control discomfort) and communication skills. These are ranked as of greater importance to patients than environmental factors such as single-sex environments, noise and even privacy.
This may have considerable implications for current approaches to evaluating the quality of endoscopy practice in the UK and including the bowel cancer screening and endoscopic surveillance programmes. First, it demonstrates a need to clearly define methods of validation of any measurement system for assessing the patient experience. Second, patient feedback should be derived from identifying what patients’ want from their endoscopic procedure and whether these issues were met, and not as retrospective assessments to determine if what was received was satisfactory. Third, alternative routes of obtaining such information that are user friendly and with less potential for bias may need to be considered such as social media or on-line patient evaluation sites (eg, http://www.iwantgreatcare.org) but the validation, independence and representation of such methods would need to be carefully evaluated for the data to be meaningful.
Finally, the practical obstacles relating to obtaining valid and accurate data on the patient experience will need to be considered. This may be resource related, such as staff time or cost, or process related such as ensuring patient confidentiality and an appropriate environment that may present difficulties within a busy endoscopy unit.
Furthermore, the available data raise questions over whether current practice focuses on the factors identified by patients as most important to their endoscopy experience, that provide the greatest value. These include the endoscopist's technical ability and their communication skills and the control of discomfort during the procedure. For example, although technical aspects of training have been greatly improved and made more consistent through the UK JAG and the JAG Endoscopy Training Scheme, communication skills are not explicitly taught or assessed in the context of teamwork and non-technical skills training other than being acknowledged in current training programmes. This may be an area of development through dedicated courses.55 Improved communication and technical skills may also be important in reducing patient discomfort during endoscopic procedures; however, the available data also suggest that there should be a reassessment of the current trends towards lower sedation or unsedated procedures46 ,56 possibly reflecting concerns of clinical risks, particularly in the elderly.57 It may be argued that sedation reduces discomfort and anxiety and improves tolerance in endoscopy58 ,59 and that patients should be aware of the risks of higher levels of sedation and analgesia but should have the opportunity to contribute towards the decision on levels of use prior to their procedure (but within recognised acceptable maximum levels) and where the acceptable balance between risk and benefit lies. This may mean that higher levels of sedation are indicated than currently being suggested.
However, in order to improve the patient experience as above, there may also be a need to improve the circumstances within which the endoscopist operates. This may include adequate training of endoscopists and other staff, appropriate and modern equipment and introduction of new technology (eg, carbon dioxide insufflation during colonoscopy) and sufficient availability of supporting staff. It may also involve ensuring an effective working environment by avoiding rushed procedures due to overbooked lists and insisting on rest breaks for staff. Moreover, these factors should not be adversely influenced by addressing environmental issues such as privacy, noise or a single-sex environment that are considered a lower priority by patients.
In conclusion, understanding patient attitudes to their care should now be considered a fundamental component of their management in endoscopy as in medicine more generally. Patient experience measures must be derived from patient narratives and significant work is needed to develop these. The subsequent provision of data may lead to a necessary re-evaluation of the priorities of clinical practice for endoscopists and as a basis for implementation or further development of quality assurance frameworks.
References
Footnotes
Correction notice This article has been corrected since it published Online First. The corresponding author's affiliations have been corrected and contact details amended. The Open Access licence has also been added.
Contributors All contributors have also authored part of this article.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.