Article Text

Abstract
Objective To determine the best faecal calprotectin (FCP) cut-off level for differentiating between irritable bowel syndrome (IBS) and organic disease, particularly inflammatory bowel disease (IBD), in patients presenting with chronic diarrhoea.
Design Retrospective analysis of patients who had colonoscopy, histology and FCP completed within 2 months.
Setting District general hospital.
Patients Consecutive new patients with chronic diarrhoea lasting longer than 4 weeks.
Interventions Patients were seen by a single experienced gastroenterologist and listed for colonoscopy with histology. Laboratory investigations included a single faecal specimen for calprotectin assay (lower limit of detection: 8 µg/g), the results used for information only.
Main outcome measures Six FCP cut-off levels (range 8–150 µg/g) were compared against the ‘gold standard’ of histology: inflammation ‘present’ or ‘absent’.
Results Of 119 patients studied, 98 had normal colonoscopy and histology. The sensitivity of FCP to detect IBD at cut-off levels 8, 25 and 50 µg/g was 100% (with corresponding specificity 51%, 51%, 60%). In contrast, the lowest FCP cut-off, 8 µg/g, had 100% sensitivity to detect colonic inflammation, irrespective of cause (with negative predictive value (NPV) 100%). Importantly, 50/119 patients (42%) with FCP <8 µg/g had normal colonoscopy and histology.
Conclusions Our results suggest that using FCP to screen patients newly referred for chronic diarrhoea could exclude all without IBD and, at a lower cut-off, all without colonic inflammation, thus avoiding the need for colonoscopy. Such a major reduction has implications for resource allocation.
- CHRONIC DIARRHOEA
- STOOL MARKERS
- IBD
- IRRITABLE BOWEL SYNDROME
- HISTOPATHOLOGY
Statistics from Altmetric.com
Introduction
The majority of our patients referred with a view to colonoscopy for ‘probably irritable bowel syndrome (IBS) but to rule out inflammatory bowel disease (IBD)’ prove to have a normal examination. IBS is far more common but missing IBD may have serious consequences. Lacking a simple yet reliable clinical or laboratory means to distinguish between the two, we are forced to continue our current practice of ‘colonoscopy for all’, and to accept the high rate of negative examinations as the price necessary to ensure that IBD is not missed.
We routinely use the inflammatory marker, C-reactive protein (CRP), to track inflammation in our IBD patients, but in our experience it lacks sufficient sensitivity to help make the diagnosis. We therefore introduced faecal calprotectin (FCP) in our practice as growing literature in adult1 and paediatric gastroenterology suggests it is a more sensitive marker of gut inflammation.2–5
The protein, calprotectin is found predominantly in neutrophils.6 Gut inflammation is characterised by increased neutrophil infiltration, which in IBD can increase×≥10-fold7 ,8 these cells are eventually shed into the lumen and are passed in the faeces, in which calprotectin content can be measured. Thus, increased FCP levels reflect gut inflammation, perhaps more its severity than its extent.9
We aimed to assess the role of FCP in aiding differential diagnosis, maximising the numbers in whom IBD could be ruled out, making colonoscopy unnecessary, yet not miss anyone with the disease. For this we compared sensitivity and specificity at different FCP levels. Using the same approach, we then explored if FCP could also be used to rule out gut inflammation irrespective of cause.
Methods
All patients referred to our gastrointestinal (GI) clinic over a 2-year period (1 June 2009–31 May 2011) for investigation of diarrhoea of longer than 4 weeks duration were consecutively assessed by a single clinician (PB) using a standard protocol. Routine investigations included coeliac serology, thyroid function tests, iron studies (if anaemic), faecal elastase and FCP. If negative, then bile acid diarrhoea (BAD) was investigated for by the 75-SeHCAT retention test (retention value at day-7 of <10% is diagnostic).
Gastroscopy, principally to take duodenal biopsies, was carried out in those with positive coeliac serology for histological confirmation, and in others whose symptoms were suggestive of lactose intolerance: the tissue lactase level in the fresh biopsy specimens was determined using the semiquantitative slide-based Quick Lactase Test (BioHIT).
We continued our conventional practice of listing all patients for colonoscopy, the FCP results being gathered for information only. Only those with proven coeliac disease, or with pancreatic insufficiency (reflected by low faecal elastase levels, <200 µg/g), were not listed for the procedure. The examination was undertaken by experienced members of the gastroenterology team.
The analysis is based on the subset in whom colonoscopy, histology and FCP assay were completed within 2 months of the initial consultation. Most patients had serum CRP checked; we identified those where FCP and CRP were completed within a 2-week period.
The FCP distribution across four clinical groups was compared: D-IBS, ulcerative colitis, Crohn's disease and other organic diseases (comprising microscopic colitis, bacterial colitis, colonic polyps and colon cancer). The diagnosis D-IBS was applied to all patients with chronic diarrhoea yet otherwise in good health, without ‘alarm’ symptoms, and whose colonoscopy and histology proved normal. This large group includes two specific diagnostic subsets, those with bile acid malabsorption or lactase deficiency.
The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of FCP and CRP were assessed using histology as the ‘gold standard’. A ‘normal colonoscopy’ was defined as the absence of visible abnormality and inflammation on histology.
FCP was assayed with the Immunodiagnostik monoclonal antibody-based ELISA test. The assay detects very low levels of calprotectin but less reproducibly when below 8 µg/g. Hence, we selected 8 µg/g as our lower limit to calculate sensitivity and specificity.
Statistical analysis
FCP levels were compared between those with and without colonic inflammation. Patients in the ‘inflammation group’ included IBD (ulcerative colitis and Crohn's disease), microscopic colitis, inflammation due to infection or in association with polyps and colon cancer.
The manufacturer recommends a cut-off FCP of 50 µg/g to distinguish between inflammatory and non-inflammatory bowel conditions. We, however, explored six cut-off levels from 8 µg/g to 150 µg/g, and calculated sensitivity and specificity, and then examined the clinical significance of levels <8 µg/g.
Finally, we calculated sensitivity, specificity, PPV and NPV for FCP at different cut-off levels against histology, the ‘gold standard’. Two sets of dual forest plots of sensitivity and specificity and summary receiver operator characteristic (SROC) curves were constructed using the Cochrane software package, Review Manager.10 These were used to distinguish between two groups: IBD versus D-IBS and ‘organic’ disease versus D-IBS. The ‘organic’ disease group includes a wide spectrum: IBD, microscopic colitis, bacterial colitis, colonic polyps and cancer, that is, those in whom colonic inflammation was found.
Results
In the 2-year period June 2009–May 2011, 219 consecutive newly referred patients were seen, of whom 119 patients met the inclusion criteria and form the basis of this report. They comprised 55 men and 64 women of similar mean age (46.4 years and 45.9 years) and distribution (for the whole group: ≤40 years, 36%; 41–60 years: 46%; >60 years, 18%), the proportion of men and women within each age band being about equal.
Reasons for exclusion were lack of colonic biopsy (n=22) or FCP (n=73). Colonoscopy was avoided in five patients as initial screening confirmed coeliac disease in two and pancreatic insufficiency in three (faecal elastase <200 µg/g).
Results of colonoscopy and histology
The majority (98 of 119) had normal colonoscopy and histology. The others (n=21) had abnormal findings: IBD (n=12, six each with Crohn's disease and ulcerative colitis), tubulovillous adenoma (n=4), adenocarcinoma (n=1), microscopic colitis (n=2), bacterial colitis (n=2).
FCP results in the clinical groups
Figure 1 shows elevated FCP levels in all with Crohn's disease and ulcerative colitis, and in most with other organic diseases. The striking difference was in D-IBS, where 50 (of the 98) had levels <8 µg/g.
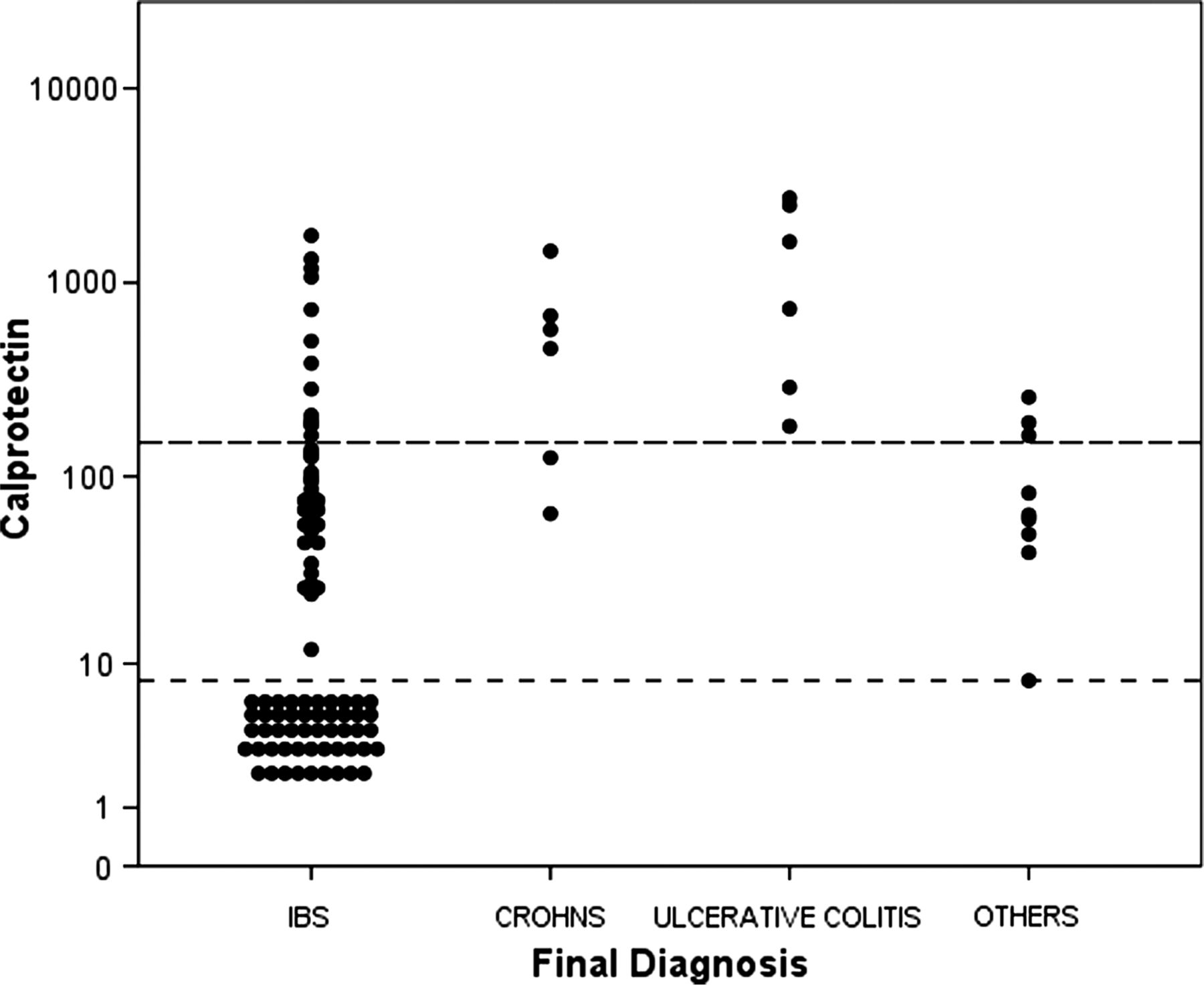
Individual patients’ FCP (μg/g) values (n=119). IBS n=98, Crohn's disease n=6, UC n=6. ‘Others’ n=9 (note that the 5th value from the top represents two patients). ‘Others’=other organic diseases (FCP value). Two microscopic colitis (8, 50). One bacterial colitis (190). One infective (257). Four adenoma (40, 60, 63, 163). One adenocarcinoma (82). FCP, faecal calprotectin; IBS, irritable bowel syndrome; UC, ulcerative colitis.
FCP results in relation to histology
Table 1 shows the details of FCP distribution in those with and without colonic inflammation. FCP was <8 µg/g in 50/98 in those without inflammation but, conversely, elevated in all 21 with it.
FCP distribution in the colonic histology groups
Patients with normal colonoscopy and histology: identifying a cause for the diarrhoea
A specific cause was found in 17 of the 98 patients in this category: BAD in 11 and lactase deficiency in six. FCP in BAD was <8 µg/g in eight, elevated modestly in two (52, 56) and markedly in one (1069). Among those with hypolactasia, FCP was <8 µg/g in three and raised in the others (53, 79, 99).
Inflammatory markers: diagnostic usefulness of CRP and FCP set against histology
CRP results were available in 114 of the 119 patients. Table 2 shows striking differences in sensitivity to detect inflammation, low for CRP and high for FCP.
Detecting inflammation: a comparison of CRP and FCP against histology, the reference ‘gold standard’
CRP when raised was associated with inflammation but normal levels did not exclude it. In contrast, FCP 8 µg/g had 100% sensitivity to detect inflammation. The correspondingly high NPV (100%) suggests this level may prove useful to exclude IBD and also any inflammation, irrespective of cause (which in 50 of the 119 patients with FCP <8 µg/g was indeed the case). Conversely, its poor specificity would result in many false positives among those categorised clinically as D-IBS.
Distinguishing IBD from D-IBS: analysis by SROC
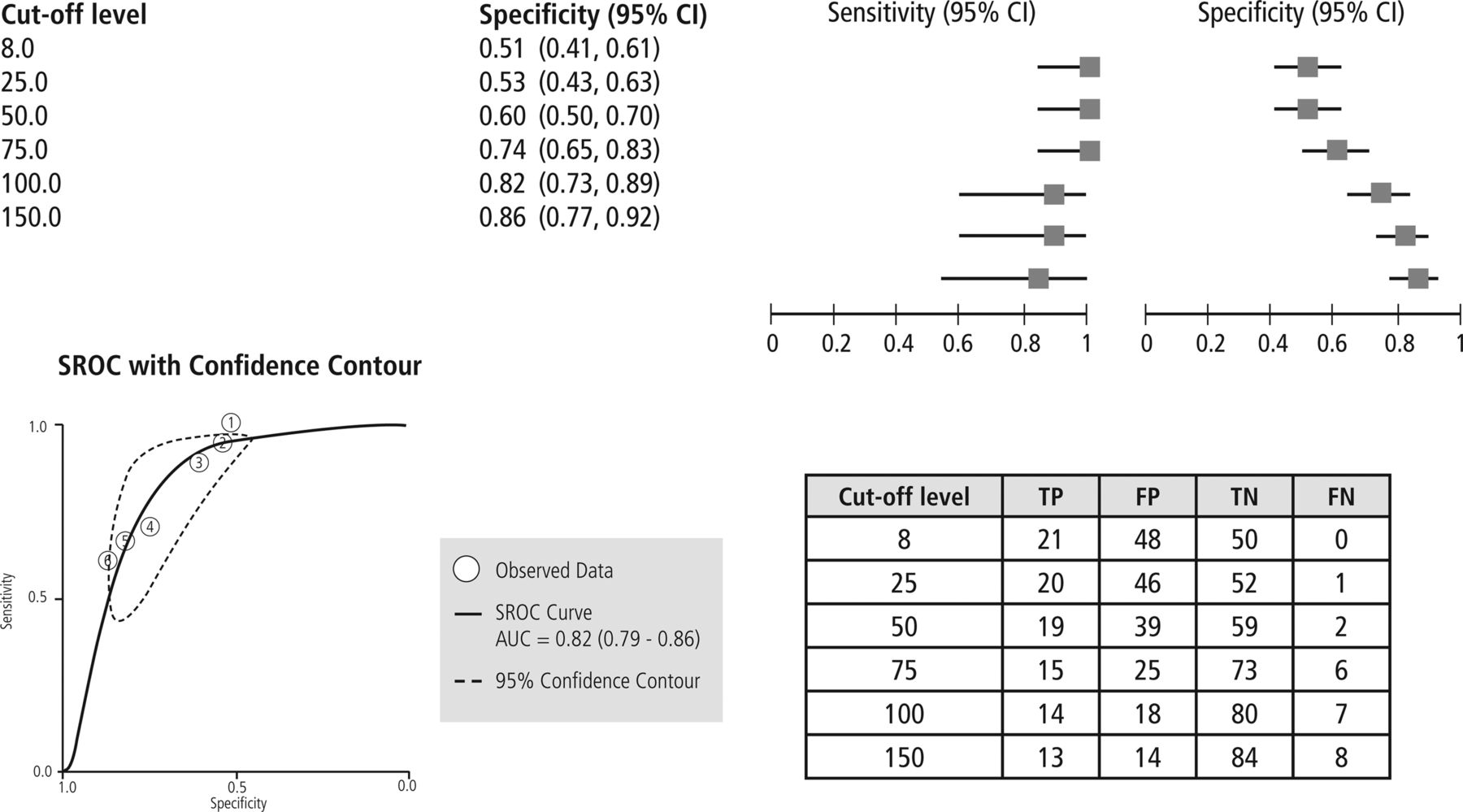
Figure 2 shows the changing relationship between sensitivity and specificity across the different FCP thresholds at distinguishing those with normal histology from others with confirmed IBD. FCP at levels of 50 μg/g was 100% sensitive for detecting IBD but specificity poor at 60%. At lower levels (25 and 8 μg/g), sensitivity was unchanged but specificity fell to 51%. Therefore, when the clinical objective is to distinguish between IBD and D-IBS, the optimal FCP cut-off would be 50 μg/g.
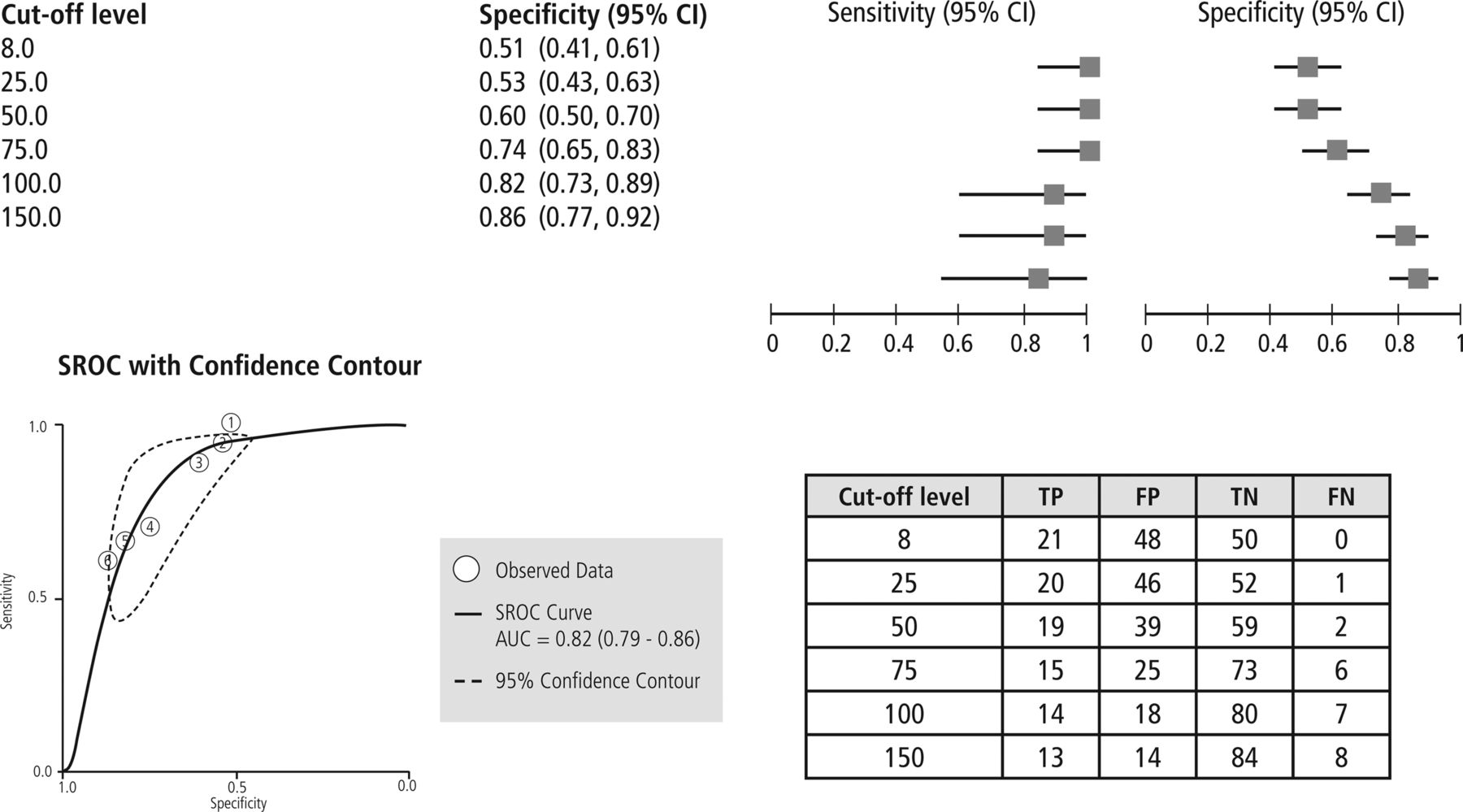
distinguishing IBD versus D-IBS. FCP: Six cut-off levels were used ranging from 8 to 150 μg/g. Top: Paired forest plot. Bottom right: Table of diagnostic accuracy at each FCP cut-off level. Bottom left: SROC curve. Diagnostic accuracy at each FCP cut-off level and 95% confidence contours. Each of the six circles represents an FCP cut-off value ranging from 8 (No. 1) to 150 μg/g (No. 6). Note: Circle No. 2 is a fusion of Nos. 1 and 2 as these overlap. TP, true positive; FP, false positive; FN, false negative; TN, true negative; FCP, faecal calprotectin; IBD, inflammatory bowel disease; IBS, irritable bowel syndrome; SROC, summary receiver operating characteristic.
Distinguishing organic disease from D-IBS: analysis by SROC
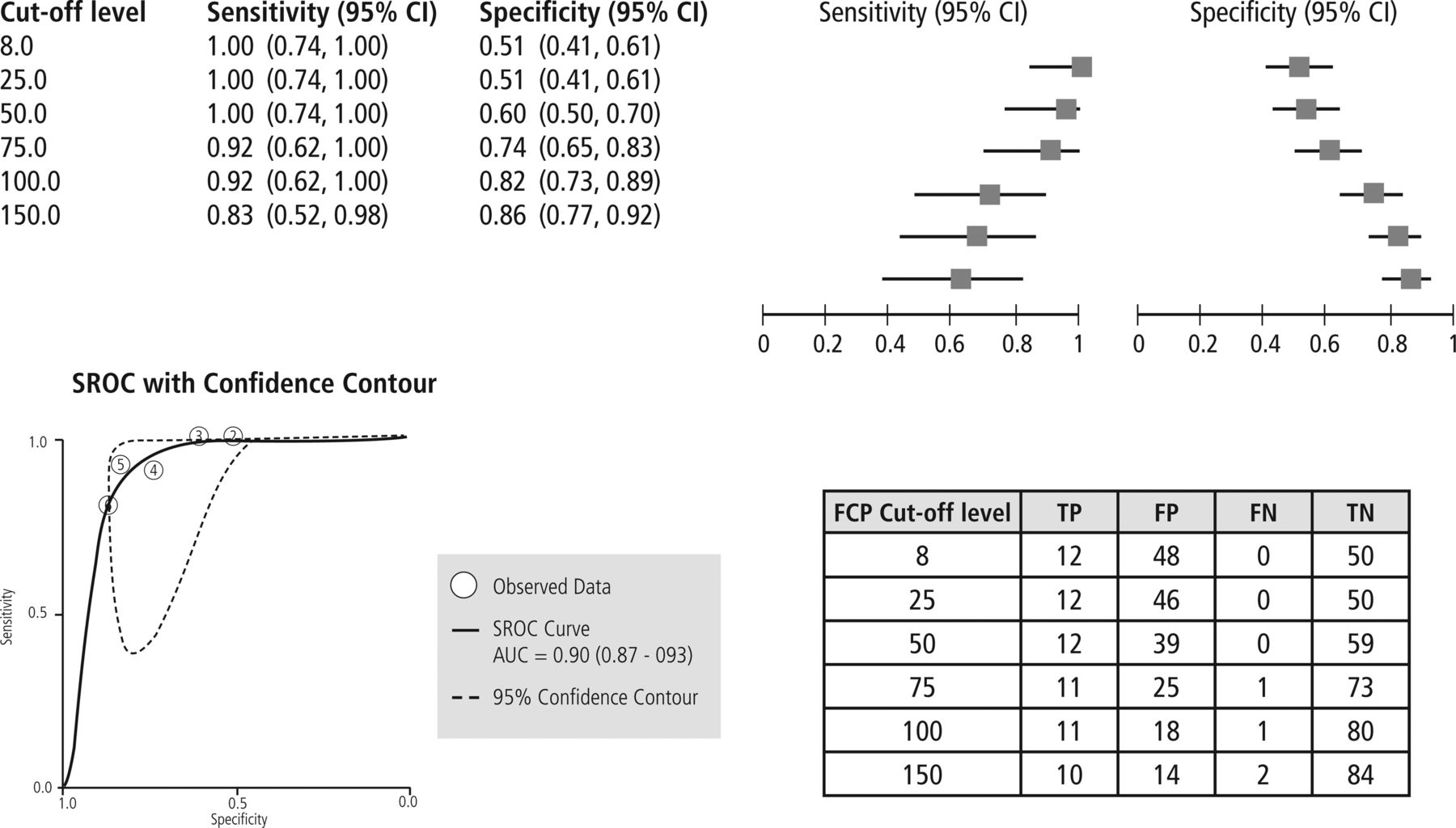
All those categorised as ‘organic’ disease had histological evidence of inflammation, whereas D-IBS patients did not. The lowest FCP cut-off, 8 µg/g, was highly sensitive (100%) to detect inflammation but had poor specificity (51%) (figure 3). However, this low cut-off had very high NPV (100%), indicating it was very good at ruling out organic pathology.

{kind=link}
{kind=link}
{kind=link}
Distinguishing organic disease versus D-IBS. FCP: Six cut-off levels were used ranging from 8 to 150 μg/g. Top: Paired forest plot. Bottom right: Tables shows diagnostic accuracy at each FCP cut-off level. Bottom left: SROC curve. Diagnostic accuracy at each FCP cut-off level and 95% confidence contours. Each of the six circles represents an FCP cut-off value ranging from 8 (No. 1) to 150 μg/g (No. 6). TP, true positive; FP, false positive; FN, false negative; TN, true negative; FCP, faecal calprotectin; IBS, irritable bowel syndrome; SROC, summary receiver operating characteristic.
Discussion
We initially used FCP in patients newly referred for investigation of diarrhoea to distinguish IBS from IBD. Our results suggest this can be achieved at FCP cut-off at 50 μg/g: all our IBD patients had higher values. However, there were only 12 IBD patients in our cohort, hence we are reluctant to develop policy based on so few. Nevertheless, our findings are consistent with the recent Health Technology Assessment report1 and other large studies.11 ,12
The advantage of our study is that it explored the usefulness of a range of FCP cut-offs, from which emerged the striking finding that 8 µg/g reliably detected colonic inflammation however caused, or excluded it: 42% (50/119) had lower values, all of whom had normal colonoscopy and histology. If these pilot results are confirmed by prospective studies, then avoiding colonoscopy in such a large proportion would spare patients the discomfort of the procedure, and benefit the hospital by reducing the number of colonoscopies (or making it available for other indications) while maintaining high levels of safety. Such a change would have major implications for resource allocation.
Conversely, elevated FCP signifies damage somewhere in the gastrointestinal tract but not its specific site. In clinical practice, it would guide us to investigate other areas if colonoscopy and histology proved to be normal.
Elevated FCP in other conditions
FCP was raised in IBD, as expected, but also in our admittedly small numbers with diverse conditions such as infective diarrhoea, microscopic colitis, adenomatous polyps and adenocarcinoma, findings which have also been noted by others.13 ,14
Increased FCP would be expected in infective diarrhoea when caused by organisms which trigger gut inflammation associated with neutrophil invasion, such as Shigella or Campylobacter, as opposed to with norovirus or adenovirus.15 ,16
Neutrophil invasion characterises IBD but lymphocytic infiltration is the hallmark of microscopic colitis in both its subtypes, ‘collagenous’ and ‘lymphocytic’. Calprotectin predominates in neutrophils and to a lesser extent in macrophages,6 ,9 so it is difficult to explain why FCP levels can be elevated in microscopic colitis. Nevertheless, the phenomenon has been documented,17–19 and is clinically relevant (see below).
Inflammation is more common within adenomatous polyps than in the adjacent mucosa, presumably neutrophil shedding leading to FCP elevation. The intensity of inflammation is directly related to polyp size20 and increased dysplasia,21 hence, identify those at higher risk of malignancy.21 In contrast, hyperplastic polyps have less inflammation.20
Some with BAD or with lactase deficiency had raised FCP, unexpected for these conditions, which fall within the spectrum of D-IBS, are not inflammatory; indeed colonic histology was normal. Crohn's ileitis resulting in BAD may remain undetected at colonoscopy unless the terminal ileum was examined or the disease was beyond reach of the instrument.22 ,23 We are, however, unable to explain why FCP elevation occurred in lactase deficiency, for the enzyme concentrations are highest only far away, in the mid-jejunum.24 Transient deficiency occurs in children and adults during rotavirus infection but soon returns to normal.25
Finally, although we have not observed an example of it in our cohort, FCP elevation from NSAID enteropathy26 ,27 is well recognised, and has also been observed on aspirin treatment.28
Chronic diarrhoea: FCP-based selection for colonoscopy
When faced with patients referred for chronic diarrhoea, gastroenterologists need to balance sensitivity and specificity: maximum sensitivity so as not to miss IBD or delay its diagnosis, but with maximum specificity to avoid carrying out colonoscopy in large numbers knowing it will prove negative in many. The current National Health Service (NHS) climate discourages follow-up, so for safety, clinicians tend to book colonoscopy for all at the initial visit.
FCP at cut-off 50 µg/g excludes IBD in anyone with lower values, while at 8 µg/g excludes colonic inflammation however caused. The lower value allows increased detection of microscopic colitis when FCP levels are raised only slightly. This is a condition of rising prevalence, particularly among the elderly29 ,30; as symptoms can be relieved with budesonide,31 it is necessary to recognise it which, in turn requires systematic biopsy for diagnostic histopathology. Thus, when colonoscopy appearances are normal in a ‘D-IBS’ patient, the endoscopist when aware of raised FCP would take more biopsies. However, such a low cut-off level has poor specificity, resulting in many undergoing colonoscopy and histology which would prove normal, that is, such patients are ‘false positives’.
Our observations suggest FCP cut-off at 50 μg/g excludes IBD making diagnostic colonoscopy unnecessary in 62 patients (52%), while 8 μg/g excludes colonic inflammation however caused, but with fewer avoiding colonoscopy, 52 patients (42%). This, in health economic terms, increases the ‘opportunity cost’, that is, fewer colonoscopy slots are released for use by other patients.
We therefore reach a situation of contrasting perspectives: the clinical focused on sensitivity in order not to miss pathology, the public health viewpoint focused on cost effectiveness and being prepared to miss occasional pathology when the opportunity cost of detecting it is too high, that is, other health benefits would have to be sacrificed.
Study limitations
Our conclusions are based on FCP results from a single faecal specimen sampled for assay at one point only, the investigation being done in a single centre and with a limited number of patients. The FCP assay is very reliable (within-assay variability 1.9%), but the distribution of calprotectin within faeces is uneven, evidenced by a ∼20% difference in results between ‘spot’ samples and after faecal homogenisation,6 and compounded by day-to-day variation of up to 54%.32
Recent studies, however, give a more optimistic picture. Thus, multiple subsamples from faecal specimens showed little variation in FCP levels, reported respectively as ‘no significant difference, p<0.01’33 and ‘coefficient of variation 4.2–7.6%’.34 Similarly, FCP in faeces collected consecutively on 2 days showed least variation when concentrations were <50 µg/g,34 and only low variability in faeces collected over 3 days, ‘intra-class coefficient 0.84’.35
Nevertheless, we would prefer to ask patients to provide two faecal samples, selecting the higher value for making clinical decisions, but recognise that acceptability may be a problem evidenced by our observation that one-third of patients failed to provide any sample despite careful explanation.
Minor study limitations
Inclusion required the key investigations (FCP and colonoscopy with biopsy) to have been completed within 2 months, sufficient time to allow postinfective inflammation to recede and be missed by the test done second.
The study was not ‘blinded’: the colonoscopies were done by several endoscopists and awareness of raised FCP by some might have influenced the number of biopsies taken. The histologists, however, were generally unaware of the FCP results.
Our study was in patients referred to secondary care with diarrhoea. The spectrum of patients seen in general practice is wider than they currently refer, with fewer patients having IBD. This would not alter the sensitivity for detecting it, but the PPV would fall, reflecting the smaller proportion with IBD.
Finally, the patients were seen by a single highly experienced gastroenterologist who adhered to a protocol, the majority reviewed in special Saturday clinics fully staffed. Such optimal conditions are difficult to replicate in busy weekday clinics staffed by doctors with variable experience.
Study strengths
Patients were asked for faecal samples only after the decision for colonoscopy had been made, that is, FCP results were collected for information only, not for decision making, thus avoiding bias. The reference ‘gold standard’ against which FCP was compared was histology, not colonoscopic appearances alone.
Detecting gut inflammation: FCP versus CRP
Sensitivity to detect histological inflammation was low with CRP but very high with FCP, the contrast also noted by others who demonstrated FCP was far superior to CRP and erythrocyte sedimentation rate in distinguishing Crohn's disease from IBS.32
FCP assay
There are several assay systems available in the UK, each with its own optimal range and lower limit of sensitivity. We use the Immunodiagnostik system because it can be automated, has a wide range and the lowest level of FCP detectable, making it best suited to exclude inflammation.36
Conclusion
Our results suggest FCP would be a valuable tool to screen patients newly referred with chronic diarrhoea. A cut-off at 50 µg/g would identify all cases with IBD as their levels are higher, while a lower cut-off of 8 µg/g predicts normal colonoscopy and histology in all those with lower values, accounting for 42% of our referrals. If confirmed by larger prospective studies, then FCP screening could identify those in whom colonoscopy need not be done. This benefits patients by avoiding invasive procedures, and the hospital by substantial reduction in colonoscopies or by releasing these resources for other indications, yet with considerable savings.
What is already known on this topic
-
Elevated faecal calprotectin (FCP) is a sensitive marker of gut inflammation but does not identify its cause or location.
-
Amongst patients newly referred for investigation of chronic diarrhoea, FCP <50µg/g virtually excludes inflammatory bowel disease (IBD).
What this study adds
-
In similar referrals, FCP <8µg/g predicts normal colonoscopy and histology, raising the question whether this invasive investigation could have been avoided. Such patients formed 42% of our referral population.
How might it impact on clinical practice in the foreseeable future
-
If confirmed by prospective studies, colonoscopy could be avoided in patients newly referred with chronic diarrhoea when screening FCP values are <8µg/g. Such a change in practice has major implications for service costs and patient convenience.
Acknowledgments
We thank Dr Pamela Royle and Dr Deepson Shyangdan of Warwick Medical School for producing the forest plots and SROC curves. At Rotherham Hospital we are grateful to Dr Michael Smith (Medical Physics) for preparing figure 1, John Slater (Graphic Design) for finalising figures 2 and 3 to comply with journal instructions, and to Beverley Mason (KDB's secretary) for administrative support throughout the development of the faecal calprotectin programme.
References
Footnotes
-
Contributors The patients were seen by PB. The faecal calprotectin assay and testing was developed by RE as part of his MSc project, and supervised by RE, MS, PB and KDB. Calculating sensitivity and specificity, positive and negative predictive values for each cut-off level was carried out by MS. All other relevant information was assembled by AB and PB. The dual forest plots and SROC curves were prepared by N Waugh and colleagues (whose contribution has been acknowledged). AB, MS, PB, NW and KDB developed the manuscript. KDB is the guarantor.
-
Competing interests None.
-
Ethics approval The faecal calprotectin test has been in use for many years. The current investigation is of patients referred for investigation of diarrhoea and for whom faecal calprotectin was an additional investigation. In effect, this is a clinical observational study, based on our usual approach to such patients, the data obtained by retrospective analysis.
-
Provenance and peer review Not commissioned; externally peer reviewed.