Article Text

Abstract
Objective To quantify the proportion of requests for colonoscopy that are performed as flexible sigmoidoscopy and documented reasons for this in ordinary UK hospital practice. To determine the effect these requests have on colonoscopy completion rate if they are included in the denominator of the calculated rate by individual endoscopist.
Design Retrospective study of 22 months flexible sigmoidoscopy practice at a major UK teaching hospital. All flexible sigmoidoscopies performed had their associated request form examined.
Setting UK NHS University Hospital.
Patients All patients receiving outpatient flexible sigmoidoscopy from January 2013 to October 2014 with no exclusions.
Intervention Conversion of colonoscopy to flexible sigmoidoscopy.
Main outcome measures Conversion of colonoscopy to flexible sigmoidoscopy, reason for conversion and adjusted colonoscopy completion rate.
Results 71 of the 3526 flexible sigmoidoscopies performed (2.0%), representing 71 of 5905 colonoscopy requests (1.2%). Conversion reason was noted only in 26 (37%) of converted cases. Adjustment of colonoscopy completion rate to include conversions pushed four of our unit's 22 endoscopists below the UK national 90% standard.
Conclusions Conversion to flexible sigmoidoscopy occurs in 1.2% of patients originally booked for colonoscopy. The reason for this conversion is often unqualified and may be inappropriate. Conversion can affect the colonoscopy completion rate, and therefore, should be included in endoscopists’ overall performance statistics.
- ENDOSCOPY
- CLINICAL DECISION MAKING
- MEDICAL STATISTICS
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Colonoscopy is the gold standard investigation for suspected lower gastrointestinal disease, allowing endoscopic examination of the entire colon.1 The quality of endoscopic investigations and therapy is regulated in the UK by the Joint Advisory Group on Gastrointestinal Endoscopy. It stipulates standards regarding multiple indices of quality in endoscopic investigation training and reporting. This includes the completion rate: that is the rate by which endoscopists achieve caecal intubation at colonoscopy. The current required standard is 90%.2
Colonoscopy carries small but significant risks of perforation (approximately 0.19%), major bleeding (approximately 0.24%) and risks associated with sedation.3 These risks vary in accordance with each patient's medical history, pharmacological history and the need for any therapeutic intervention.4
It has been suggested that colonoscopy is an over requested test with inappropriate requests estimated as high as 29%.5
Flexible sigmoidoscopy is another lower gastrointestinal endoscopic examination, proceeding only as far as the splenic flexure, and often requires less sedation to be completed successfully. It still carries a risk of perforation, sedation and bleeding. A large population-based study from the USA showed the risk of perforation to be roughly half that of colonoscopy.6
Given the high rate of inappropriate colonoscopy requests and the significant added risk that proceeding to the caecum entails, it could be argued that converting an inappropriate request for colonoscopy into a flexible sigmoidoscopy might be appropriate, especially in a high-risk patient. It is currently unknown how often colonoscopy requests are converted into flexible sigmoidoscopy examinations in the UK, nor the reasons for doing this. Clearly, flexible sigmoidoscopies cannot contribute to an endoscopist's caecal intubation rate so conversion will prevent these procedures from counting to the denominator of the colonoscopy completion rate. Therefore, it is possible that converting requests to flexible sigmoidoscopy will significantly increase the colonoscopy completion rate. This could be considered to be ‘gaming’ the system to produce a falsely flattering completion rate. The gaming of performance measurement systems is known to occur in the NHS and is one of the described unintended additional consequences of their introduction.7
The aims of this study were to investigate the frequency at which colonoscopy requests lead to flexible sigmoidoscopy being performed (the conversion rate) and the reasons for this. We then examined the effect of this practice on colonoscopy completion rates by individual endoscopist.
Method
The database of the Unisoft GI reporting tool (Unisoft Medical Systems, UK) was used to retrospectively identify all patients who underwent a flexible sigmoidoscopy between January 2013 and October 2014 at a large university teaching hospital. Flexible sigmoidoscopy procedures performed on an inpatient basis were excluded as the Trust encourages only flexible sigmoidoscopy to be performed in the acute setting.
Request forms and endoscopy reports were retrieved from hospital electronic databases to systematically review each sigmoidoscopy procedure in turn to determine whether the procedure had been requested as a colonoscopy. The endoscopy report was inspected for reasons given for converting the procedure to sigmoidoscopy. The reasons for conversion were tabulated by frequency. The overall conversion rate of colonoscopy requests to flexible sigmoidoscopy, and conversion rate by endoscopist were calculated.
In order to assess whether some endoscopists converted significantly more procedures than others, individual conversion rates were plotted against the number of colonoscopies performed over the same time period on a funnel plot. Funnel plot control limits were set at 95% and 99.9%.
Colonoscopy completion rates for individual endoscopists were calculated over the same time period—unadjusted and adjusted so that the denominator included sigmoidoscopy procedures that had been requested as colonoscopy. These data were visualised on a simple scatter plot.
It is possible that performance indicators other than colonoscopy completion rate may be associated with conversion of colonoscopy requests to flexible sigmoidoscopy. To examine this, conversion rate was plotted against performance indicators that were available from the Unisoft reporting software: polyp detection rate, use of sedation and patient discomfort.
All data computations and graphics were performed using R (R foundation for Statistical Computing, Austria), and the funnel plot used the ggplot2 package.8
Results
Over the 22-month study period, 4161 flexible sigmoidoscopy procedures were performed. Of these, 629 inpatient sigmoidoscopy and 6 colonoscopy procedures that had been erroneously coded as flexible sigmoidoscopy were excluded, leaving a study population of 3526. These procedures were performed by 22 individual endoscopists. Over the same time period, there were 5905 colonoscopy requests.
Seventy-one of the 3526 sigmoidoscopy procedures (2.0%) were originally requested as colonoscopy, and therefore, represented conversions. A total of 116 (3.3%) of the flexible sigmoidoscopies did not have a retrievable associated request after extensive electronic and manual searching. The 71 converted cases represented 1.2% of all colonoscopy requests.
A documented reason for conversion to sigmoidoscopy was found in only 26 (37%) of converted cases. The reasons for conversion are detailed in table 1. The most commonly cited reason for conversion was that the patient had not taken full bowel preparation. Given the surprising frequency in which no reason for conversion was cited, the indication for colonoscopy was reviewed in these 45 cases (see online supplementary table). In five cases, colonoscopy was requested for polypectomy or endoscopic mucosal resection (EMR) of a known lesion or for biopsies/tattooing of a known tumour. It is questionable as to whether these five cases mandated completion to the caecum, but the other 40 converted cases with no cited reason for conversion were for ordinary colonoscopy indications.
Documented reasons for conversion of 71 cases requested as colonoscopy to flexible sigmoidoscopy, in order of frequency
Conversion rate varied by individual with a range of 0%–3.2%. The mean conversion rate was 1.2% (SD 0.9%) and median conversion rate was 0.9% (IQR 0.5%–1.9%). A funnel plot of conversion rates against number of colonoscopies performed over the same time period by individual endoscopist showed that one endoscopist sat on the 99.9% limit (see figure 1). Three endoscopists were outside the 95% limit.
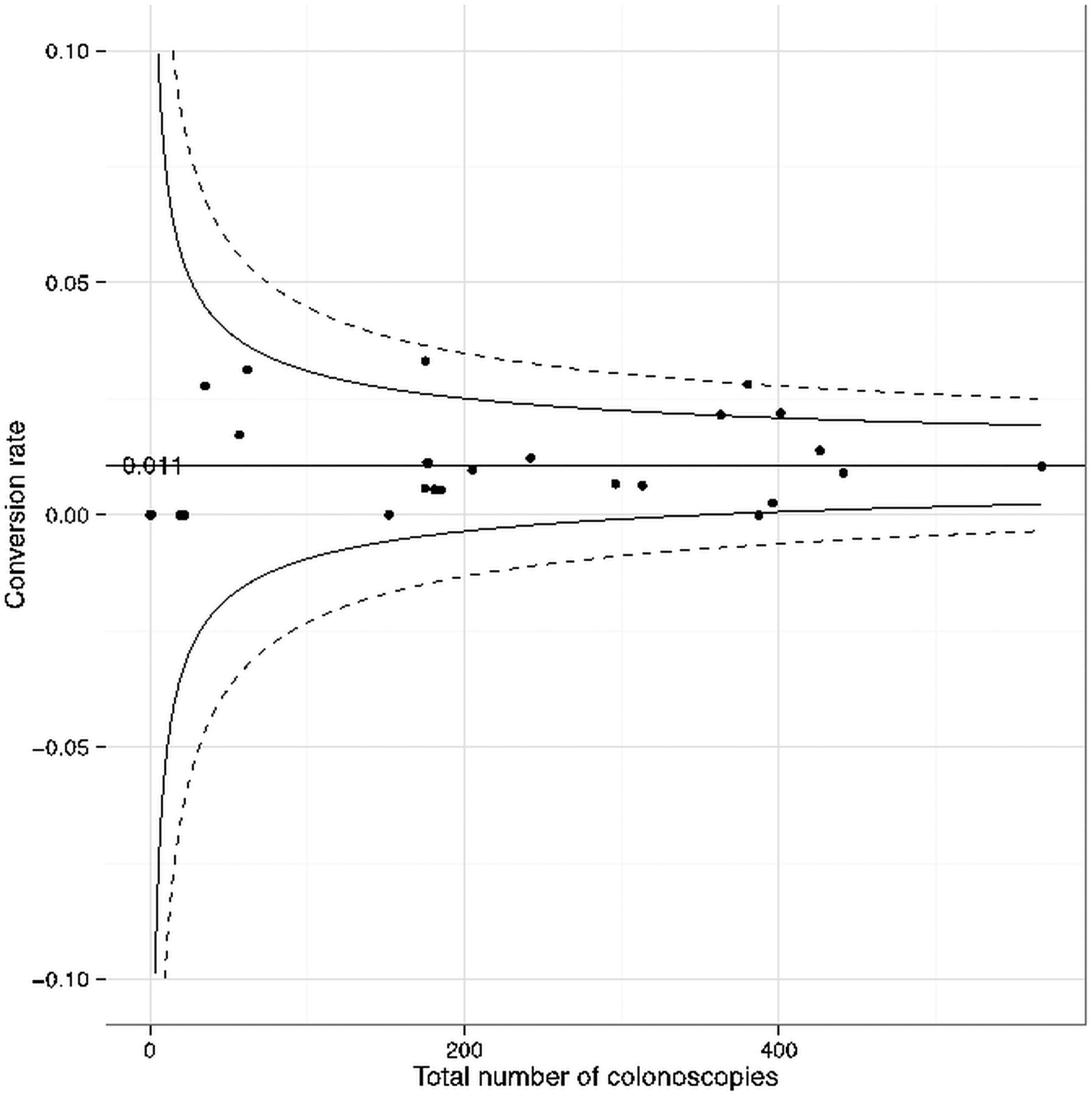
Funnel plot showing the conversion rate of colonoscopy requests to flexible sigmoidoscopy by total number of colonoscopies performed over the same time period by individual endoscopist. Curved black line and dotted line represent 95% and 99.9% control limits, respectively. Weighted geometric mean conversion rate=0.011.
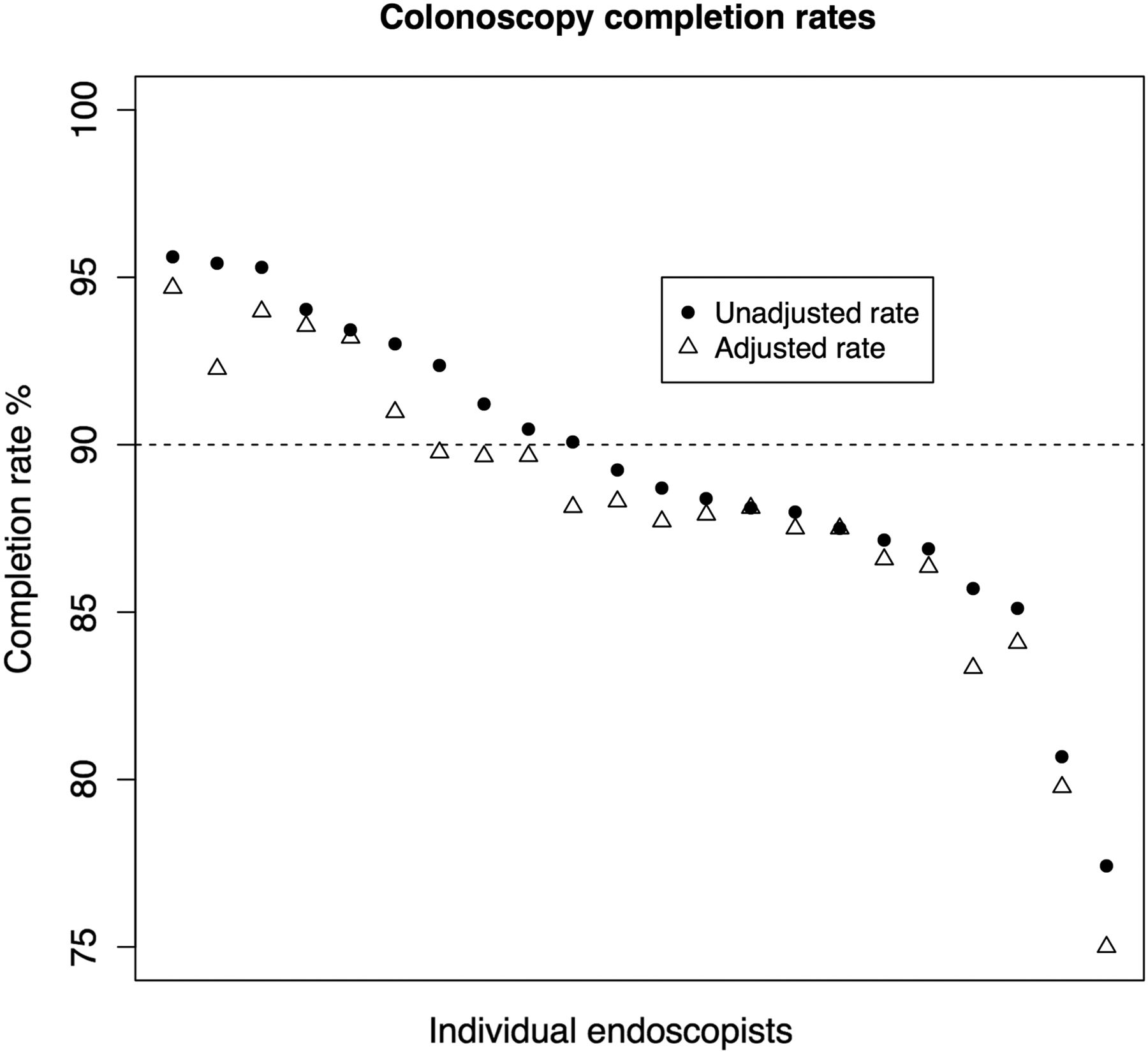
If the 71 converted cases had been completed as colonoscopy procedures, as requested, they would have counted to the total number of colonoscopy procedures performed by endoscopists, and therefore, the denominator of their colonoscopy completion rate. Converted cases were, therefore, allowed to contribute to the completion rate denominator resulting in an adjusted completion rate. Unadjusted and adjusted completion rates by endoscopist are shown in figure 2. Four endoscopists dropped below the 90% standard once their completion rate was adjusted for flexible sigmoidoscopy procedures requested as colonoscopy.
{kind=link}
{kind=link}
Colonoscopy completion rates by individual endoscopist: unadjusted and adjusted so that the denominator includes flexible sigmoidoscopy procedures requested as colonoscopy. Dotted line represents the 90% colonoscopy completion standard.
In terms of other performance indicators, neither polyp detection rate, use of sedation nor patient discomfort correlated significantly with conversion rate (see online supplementary figure).
Discussion
A small but significant number of flexible sigmoidoscopy procedures were requested as colonoscopy. It seems that most endoscopists convert at least some of their colonoscopy requests into flexible sigmoidoscopy. Importantly, the reasons for this were poorly recorded. This lack of transparency is unhelpful as there is no feedback to the requesting clinical health professionals allowing them insight into their requesting practices. Also, the endoscopists’ motives for conversion are hidden, opening them to accusations of gaming to improve their caecal intubation rate.
Of the 26 cases where a reason for conversion was cited, we suggest that 13 cases (50%) were legitimate reasons for conversion, namely: the patient had not taken the bowel preparation, colonoscopy was not indicated on clinical grounds and the patient chose not to undergo colonoscopy. Other cited reasons for conversion such as poor preparation, strictures, looping and patient discomfort may indeed limit the extent of a colonoscopy, but the procedure should still be recorded as an incomplete colonoscopy and count towards an endoscopist's incompletion rate.2 Sadly, due to limitations in our endoscopy reporting software, it is impossible to tell when in the process of performing endoscopy that the conversion occurred. Ultimately, the decision to convert a colonoscopy request to a flexible sigmoidoscopy ought to be made before commencing the procedure.
Conversion rates in our unit are low (≤3.2%) making it unlikely that dishonest gaming to boost an individual's completion rate is taking place to a large degree. Nevertheless, the completion rate for four endoscopists was pulled below the 90% standard when adjusted for converted cases. It is important to realise that not all of the converted cases should adjust the completion rate, but in the face of poorly documented reasons for conversion or knowledge that the decision to convert took place before starting the procedure, it is impossible to determine which cases should or should not be permitted to adjust the completion rate. The adjusted completion rate, therefore, represents the lowest possible completion rate for an individual endoscopist, taking all converted cases into account. It is noted from our data that two endoscopists had an unadjusted completion rate of <85%. These endoscopists were also performing a low volume of colonoscopies annually. Since this study, these two endoscopists have agreed by mutual consent to stop performing colonoscopy.
Individual endoscopist conversion rates vary and some individuals did not convert any cases (n=2). A funnel plot was used to define any endoscopists that were clear outliers, that is, converted significantly more cases than their peers. This is one statistical technique to identify outliers, having gained popularity from their use in meta-analyses to identify publication bias9 and have been used to compare the quality of colonoscopy among different endoscopy units.10 The precision of a measured rate is linearly related to the logarithm of the sample size so that control limits, constructed at the 95% and 99.9% level, funnel closer together with increasing sample size. A more detailed explanation of the use and construction of funnel plots can be found elsewhere.11 ,12
One endoscopist's conversion rate sat on the outer control limit. Rather than accuse such an individual of possible gaming, this statistical approach has the potential to simply identify such individuals for more detailed audit. For example, a procedure to tattoo or perform a polypectomy in the transverse colon following a recent total colonoscopy should not mandate repeated intubation to the caecum. Such a procedure in the transverse colon would be requested as a colonoscopy, but ought not mandate caecal intubation. Therefore, procedures such as this should not count towards the standard measure of caecal intubation in all comers. Perhaps there is place for a new classification of ‘planned limited colonoscopy’. An individual endoscopist might be exposed to more of such cases than his/her peers by being the local expert at polypectomy, for example, and thus make that endoscopist's completion rates below standard if those procedures are not distinguished from usual colonoscopy. The only alternative available to the endoscopist in such cases is to report the procedure as a flexible sigmoidoscopy to negate this effect. Clearly not all conversions are for such legitimate reasons, and it is important for governance and quality assessment that gaming is discouraged.
There is a dearth of published data on the frequency at which flexible sigmoidoscopy is performed despite a request for colonoscopy. To our knowledge, this is the first study to specifically address this question. We have shown that conversion to flexible sigmoidoscopy does indeed occur, although at a low rate of 2% in our endoscopy unit. We have shown that reasons for this conversion are poorly reported and in some cases, there may not be legitimate grounds to perform a flexible sigmoidoscopy as opposed to an incomplete colonoscopy. The latter has the potential to alter an individual's audited colonoscopy completion rate. Given the importance of the completion rate as a marker of quality endoscopy,2 we suggest that the conversion rate to flexible sigmoidoscopy and reasons for conversion should be continually audited along with overall completion rates. For this to occur, it is vital that the procedure requested and any reasons for conversion are recorded unambiguously by endoscopy staff prior to commencement of the endoscopic procedure. We would encourage other endoscopy units to measure their conversion rates and propose that funnel plots can be used to identify outlying endoscopists to examine processes leading to procedure conversion.
We suggest that a new classification of ‘planned limited colonoscopy’ be introduced (and the frequency of use of this classification audited). In electronic reporting systems this type of colonoscopy could have a mandatory field to explain the indication. Automated audit of conversions could also be introduced if electronic sigmoidoscopy reporting systems had mandatory fields for type of procedure requested and reason for conversion.
Since this study, endoscopists at our institution have been made aware of our findings and that colonoscopy conversion rates will be periodically audited. Endoscopists have, therefore, been advised to comment on any reasons for conversion in their report.
Key messages
What is already known on this subject?
There is no published data to quantify how frequently colonoscopy requests are converted to flexible sigmoidoscopy in clinical practice, thereby inflating colonoscopy completion rates.
What this study adds?
This study investigates the frequency of conversion of colonoscopy requests to flexible sigmoidoscopy in a large University teaching hospital, quantifies the effects of conversion on individuals' colonoscopy completion rates and examines reasons for conversion.
How it might impact on clinical practice in the foreseeable future?
Conversion of colonoscopy requests to flexible sigmoidoscopy is a legitimate metric to audit given its impact on colonoscopy completion rate. It is suggested that a planned limited colonoscopy should fall outside the definition of a converted request.
Acknowledgments
Many thanks to Kellie Ward (Endoscopy Clinical Audit Officer) and Selvameena Dhandapani (Business Process Manager, IT Services) at the University Hospital Birmingham for their help in retrieving endoscopy data and request forms.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online figure
- Data supplement 2 - Online table
Footnotes
Twitter Follow Chris Thompson at @chrisvthompson
Correction notice This article has been corrected since it published Online First. The conversion from colonoscopy requests figures have been corrected.
Contributors CT: data collection, literature review, study design, analysis, drafting of manuscript. SR: study design, critical revisions to manuscript. TI: study design, critical revisions to manuscript. RW: realisation of study concept, drafting of manuscript, final approval of manuscript. STW: realisation of study concept and design, data collection, statistical analysis, drafting of manuscript, final approval of manuscript, accountability for accuracy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement A full spreadsheet of the raw data can be obtained from the corresponding author (STW).