Article Text

Abstract
Introduction Mentorship has long been recognised as beneficial in the business world and has more recently been endorsed by medical and academic professional bodies. Recruitment of women into gastroenterology and leadership roles has traditionally been difficult. The Supporting Women in Gastroenterology network developed this pilot scheme for female gastroenterologists 5 years either side of the Completion Certificate of Specialist Training (CCST) to examine the role that mentorship could play in improving this discrepancy.
Method Female gastroenterology trainees and consultant gastroenterologists within 5 years either side of CCST were invited to participate as mentees. Consultant gastroenterologists of both genders were invited to become mentors. 35 pairs of mentor:mentees were matched and completed the scheme over 1 year. Training was provided.
Results The majority of the mentees found the sessions useful (82%) and enjoyable (77%), with the benefit of having time and space to discuss professional or personal challenges with a gastroenterologist who is not a colleague. In the longitudinal study of job satisfaction, work engagement, burnout, resilience, self-efficacy, self-compassion and work-life balance, burnout scale showed a small but non significant improvement over the year (probably an effect of small sample size). Personal accomplishment improved significantly. The main challenges were geography, available time to meet and pair matching. The majority of mentors surveyed found the scheme effective, satisfying, mutually beneficial (70%) and enjoyable (78%).
Conclusion Mentorship is shown to be beneficial despite the challenges and is likely to improve the recruitment and retention of women into gastroenterology and leadership roles, but is likely to benefit gastroenterologists of both genders.
- health service research
- quality of life
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Modern mentorship has a variety of definitions, and one widely quoted in the medical and academic world is from The Standing Conference on Postgraduate Medical and Dental Education (SCOPME), which described mentoring as:
The process whereby an experienced, highly regarded, empathic person (the mentor), guides another individual (the mentee) in the development and re-examination of their own ideas, learning, and personal and professional development.1
Mentorship has been commonly employed in the business world for many years and more recently has been adopted by the medical and academic communities. It is now widely endorsed within the National Health Service2 and by the General Medical Council,3 British Medical Association,4 Royal Colleges and Universities,5 with many of these organisations providing dedicated schemes to their members. Within the medical community, there is increasing evidence that although there is a relatively equal split of men and women entering medical school, fewer women attain senior clinical leadership and academic positions.6 One study quoted lack of role models and poor mentorship as key factors.7 Indeed, for those women who do take on senior roles, mentorship is often a crucial element to their career success.8 A study in 20149 found women were more likely to be dissatisfied with mentoring schemes and often face difficult in simply finding a suitable mentor.10
Supporting Women in Gastroenterology was established to examine the issue of gender discrepancy within gastroenterology, which traditionally has been less attractive to women.11 12 As part of this, the network set out to examine the benefit of mentorship to women.
Recruitment and design
The mentoring scheme was open to female gastroenterologists with up to 5 years either side of Certificate of Completion of Specialist Training (CCST) as mentees. Consultant Gastroenterologists of both genders were invited to become mentors on the scheme. Mentors were asked to provide a short profile of personal values, professional/personal achievements and external interests to enable mentees to choose a mentor who might suit their needs.
The scheme lasted 1 year, started in autumn 2015 and ended in autumn 2016. Pairs were encouraged to have a meeting 4–6 times during the year, with face-to-face meetings being preferable, but use of skype, telephone and email being alternatives acknowledging the restrictions of time and geography.
A mentee questionnaire was completed at the start and at the end of the year to provide longitudinal quantitative and qualitative data. Both surveys contained questions covering the areas shown in box 1. The initial survey included demographic data and information about job roles. A group of mentees were also invited to participate in a telephone interview once the scheme had finished. The interview sought opinions about the aims, benefits and challenges of participating in the scheme. A survey of mentors also took place to provide feedback on the scheme from their perspectives. Four main areas were covered—structure, benefits for mentors, challenges and women in gastroenterology. This was supported by a small group discussion at the end of the scheme which focused on experiences of the mentors and on future development of a society-wide mentoring scheme.
Survey areas and measurements
Job satisfaction using the Global Job, Career and Specialty Satisfaction scale (Williams et al 19). Maximum score is 5 and minimum is 1.
Work engagement using the Abbreviated Utrecht Work Engagement Scale (Schaufeli et al 20). Maximum score is 6 and minimum is 0.
Burnout using the Abbreviated Maslach Burnout Inventory (McManus et al,21 after Maslach and Jackson22). This consists of four subscales: Emotional Exhaustion and Depersonalisation indicate higher burnout, while Personal Accomplishment indicates lower burnout. The fourth measure is of satisfaction with a medical career. All four measures have a maximum score of 18 and minimum of 0.
Resilience using the Brief Resilience Scale (Smith et al 23). Maximum score is 5 and minimum is 1.
Self-efficacy using the General Self-Efficacy Scale (Schwarzer and Jerusalem24). Maximum score is 40 and minimum is 10.
Self-compassion using an abbreviated Neff scale25 after Bachkirova et al.26 Maximum score is 5 and minimum is 1.
Work-life balance was measured with Work Life Balance scale (Hill et al 27). Maximum score is 5 and minimum is 1.
All mentees and mentors were invited to attend a combined training session on mentoring, which covered the principles of modern developmental mentoring (as opposed to coaching, therapy, supervision or patronage). Mentor and mentee attributes are shown in table 1. The aim of the mentor was to help the mentee to reflect on the work they were doing both during and between the sessions; develop insight both about their situation and themselves; challenge self-imposed limitations and self-limiting beliefs; identify achievable goals; plan and implement actions which help to achieve goals and notice, reinforce and celebrate their successes.
Guidance on the structure of the sessions was given; this included establishing the ground rules of the relationship and how to approach problems if the relationship was not working for either party.
Mentor attributes and mentee attributes
Results
Mentee survey
Of the initial 40 mentor:mentee pairings, 35 were established and commenced the scheme. Dropout after pairings was due to various reasons such as moving jobs, pregnancy, time limitations. Twenty-nine mentee participants responded to the initial survey and 19 to both the initial and final surveys.
At initial survey, there were seven consultants, 15 registrars, four were in research and three in teaching role. Eighteen participants had one or more children, one was a carer for an elderly relative and 11 had no children. Twenty-three participants were white British, two were Asian British, three white (other), one Arab and one did not state.
At the end of the scheme, 22 participants completed the survey. Nineteen mentees were still matched with a mentor at the end of the scheme. Seventy per cent managed three or more sessions, and although two reported having had no mentoring sessions, it appears they had phone or skype conversations, and of a typical session duration. Ninety-five per cent of sessions lasted between 30 and 90 min.
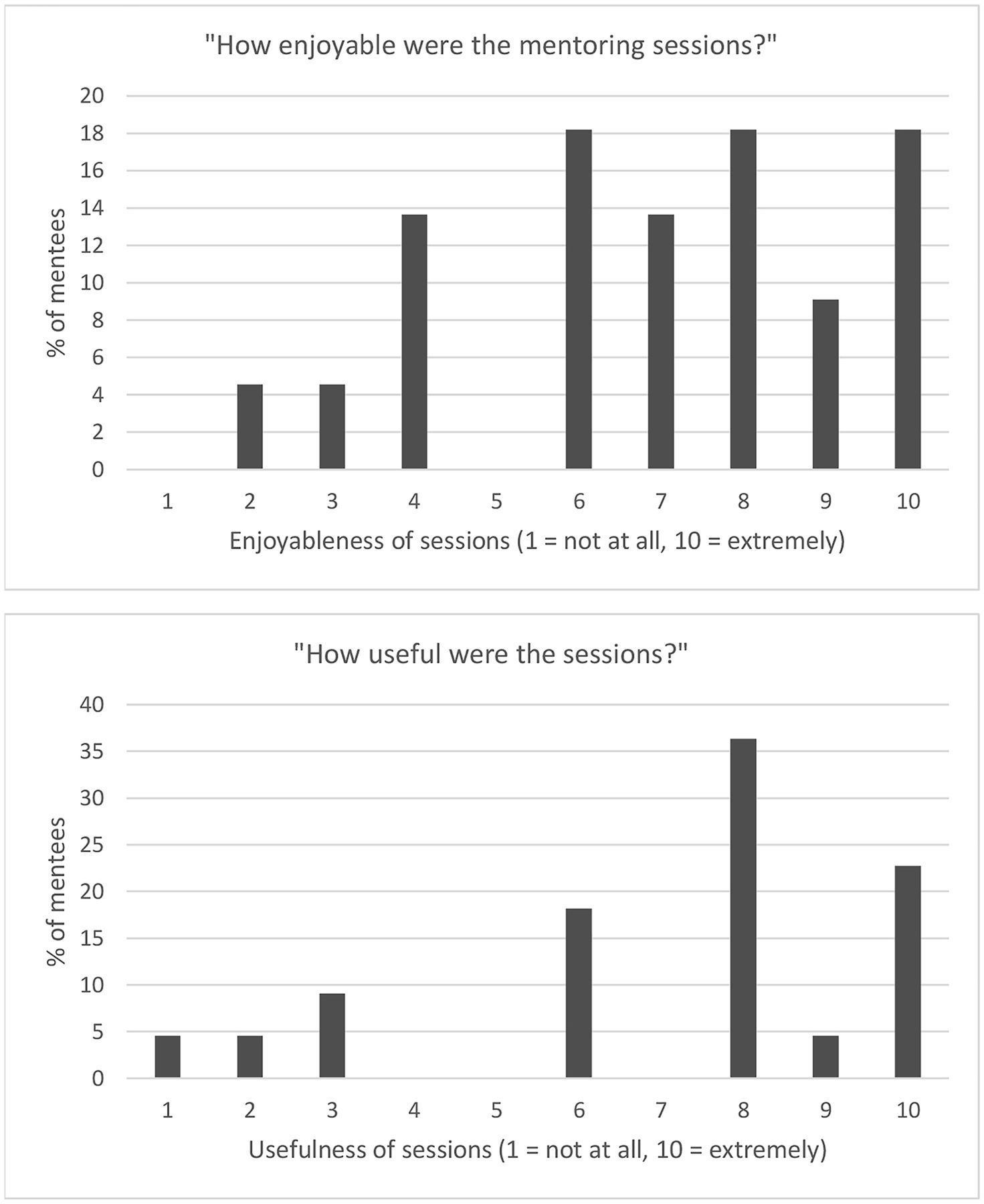
Generally, mentees were positive about their experiences (table 2). The majority reported looking forward to mentoring sessions, considered they had had a good relationship with their mentor, were well matched with their mentor and that they had achieved what they had hoped for at the outset of the scheme. Seventeen mentees (77%) gave the sessions an enjoyableness rating of six or more out of 10, with 10 being extremely enjoyable and 18 (82%) rating the usefulness as six or higher (figure 1).
Experiences of mentees (numbers of participants)

{kind=link}
Mentees’ ratings of enjoyableness and usefulness of mentoring sessions.
Longitudinal study
A total of 22 participants completed the final survey. Of those, 19 had participated in the baseline survey, so only their data was used for the longitudinal analysis. Analysis was carried out using paired t-tests for comparisons of scores from the two time points. Two-tailed tests were used for all variables to reflect the possibility of scores increasing or decreasing, with alpha set at 0.05. Effect sizes were measured using d and assessed using Cohen’s criteria of 0.2 being a small effect size, 0.5 a moderate effect and ≥0.8 a large effect.13
All items showed a change in mean score indicating improvement. Five items showed a small effect size. Of these, one—Personal Accomplishment—approached a medium effect size and showed a statistically significant improvement. This is likely to be due to small sample size. The results are summarised in table 3.
Summary of mean and analysis of changes from baseline to final survey
Mentee interviews
All mentees were invited by email to take part in telephone ‘exit’ interviews. Eleven responded, but three interviews could not be arranged within the necessary timescale. The remaining eight participants were asked about their experiences, what they had wanted out of the scheme, what they had found useful and what they might change if the scheme was taken forward.
Aims
Participants were primarily interested in support in making career decisions and managing their time. Personal life was also mentioned, but appeared to be less of a priority, other than where it became entwined with career in, for example, ensuring working hours were compatible with family obligations. Participant 2’s aims encapsulate the general needs expressed by participants:
To have a mentor who will give me support if I needed some kind of direction in my career and to give me advice if I was struggling in something and I needed some support … Or sometimes just to reassure that things… I’m doing the right things with my career, or not only career but sometimes in personal life
Most interviewees had a clear idea of what they hoped to gain from the scheme. However, there were comments among mentors and mentees that indicated difficulties finding a direction, which suggests it may be useful to outline the areas in which mentoring can be helpful and the principles underpinning the scheme, prior to mentees signing up.
Achieving space
Participants described the benefits of a mentoring relationship away from their usual commitments. This was first having a space away from the working environment,
I was away from work, I was in a different city, it allowed for time and separation…, which was quite important for me. Participant 8
Meeting a mentor outside one’s circle of colleagues was a catalyst for exploring new ideas, and having no direct working relationship was also important particularly if the mentee felt that they were struggling and could not discuss this with a colleague due to perceptions of competence and ability.
Finding and building a relationship with a mentor
Participants felt it was important for there to be a wide range of mentors at different levels and with different backgrounds, because of the variety of needs of mentees. There were some challenges with building rapport. Participants also found that meeting senior female gastroenterologists at the scheme training event was inspiring, and was also an opportunity to see both sides and to understand the mentors’ perspectives. Matching had generally worked well among the interviewees, and they recognised the specific benefits that their mentor’s personality or experience could contribute. It was also appreciated that there was the option to address a relationship that was not working well.
Challenges
The main difficulty for participants involved the practicalities of meeting up due to limited time available for meetings and geography (which increased the time and effort required for meetings). For some participants, specific demands within their work or family commitments delayed or limited engagement with the scheme. In other cases, participants made more time-consuming arrangements and did so because they felt the mentoring was highly beneficial. It was recognised that for there to be impartiality, there may need to be a compromise on location and vice versa. While some participants used skype and phone, it was felt that face-to-face meetings were important, particularly if certain issues were present, such as bullying or harassment.
Other difficulties raised by mentees included expectations not being met during the first session, imperfect matching of mentor and mentee or a tendency to fall back to forms of mentoring that the mentor and mentee had experience of in the past (generally a more patriarchal form). Some mentees were a few years into consultant post and felt that having a mentor would be more beneficial earlier in a career.
Benefits
Participants were positive about the outcomes they achieved:
I entered this with little expectation and have received guidance, experience and advice which has been instrumental. My mentor was extremely well matched and clearly experienced in doing this. The benefit of the scheme has been life changing.
It led to me making changes to my job plan and enabled me to review my career priorities. I was able to focus on what is important to me and I now have a more realistic and achievable personal development plan. It was really helpful to review my career plans with a senior, experienced but independent Consultant.
Overall, there was much praise for the scheme, appreciation of the opportunity to take part and the identification of specific positive outcomes among the participants.
Mentoring women in gastroenterology
Participants varied in the level of importance they placed on the scheme being focused on women. There was a preference for female mentors because of a belief that a successful woman is likely to have additional insight into how to make a career work for them. At application stage, there was a clear preference among mentees for female mentors.
One participant stated that while the scheme should not be restricted to women only, she had found it particularly beneficial to have a female mentor because of the lack of women gastroenterologists.
I haven’t worked with many female gastroenterologists, I’m struggling even to think of any, maybe one or two, so it’s interesting to find out another perspective if you haven’t regularly worked with women as a colleague or a senior. That’s new and interesting to have a mentor that’s female. Participant 5
Overall, there was a belief that the scheme should be extended to men, but at the same time, there should be recognition of the benefit of having female gastroenterologists as role models and of attention being paid to issues that particularly affect women.
Mentor responses
Eighteen female and nine male mentors completed the survey, which was enhanced by focus group feedback. Overall, mentors felt they had derived benefit from the scheme, including the opportunity to reflect on their own career, gaining a new perspective, a sense of satisfaction both in developing their own mentoring skills and developing their mentee. Seventy per cent felt that they had participated in an effective, high quality and satisfying mentoring relationship. Seventy per cent agreed that it was of mutual benefit and 78% enjoyed being a mentor.
Negative feedback from some mentors included the wish for more formal mentorship development or an opportunity to benchmark their performance. Some found it difficult to ensure that the sessions were mentee-led. There were mixed views on whether impartiality was thought to be enhanced by mentoring outside of their organisation or region. Twenty-two per cent felt no personal benefit from the scheme: only 44% felt that reciprocal learning had taken place.
Discussion
The long-term vision of the British Society of Gastroenterologists (BSG) is to encourage the active recruitment of the most talented medics to our specialty and to optimise their professional development and support through BSG membership. It is particularly important to attract more women into gastroenterology and to encourage and support them into leadership roles, to keep pace with the changing gender demographic in medicine. Mentorship is already widely accepted to be beneficial in many spheres. A review by Steven et al 14 found three main areas of benefit for participants in mentorship schemes: clinical practice, personal well-being and professional development. This was due to improved problem-solving skills and management of change. This supports previous work showing similar benefits to individuals, which also noted significant benefits to mentors and wider organisations.15
This pilot scheme for female gastroenterologists in the years either side of their first consultant post was shown to be successful for the majority of participants. Training in the principles of mentorship and guidance on structure of the sessions was helpful, with joint attendance by mentors and mentees bringing additional benefit. Matching of pairs was challenging, but largely successful, and in future it is worth drawing attention to the different aspects of mentoring to mentees making choices about their mentor. Current literature describes potential difficulties encountered with mentorship which appear to stem from the logistics and conduct of the schemes rather than the content itself. Examples of issues include: lack of understanding about roles and boundaries of the relationship,16 conflicts of interest,17 breach of confidentiality and mentor bias.18 Our results show that geographical locations of participants and time constraints were common difficulties, but not insurmountable, and the benefit of having a non-colleague mentor is significant. Perhaps, in future mentees could prioritise preferred qualities of mentor, location of mentor or separation from colleagues. The BSG Council has agreed to adopt, and is co-funding, a society-wide mentoring programme as a key membership benefit, which is likely to contribute to improvement in recruiting into gastroenterology and leadership roles. It is hoped that women will continue to benefit from the scheme which will be open to both genders.
Key findings
Participants who actively participated reported excellent outcomes, felt their aims had been achieved and had many positive comments to make about the scheme and its benefits.
All quantitative measures showed improvement over the year, although this was only statistically significant for one measure (Personal Accomplishment within the Maslach Burnout Scale).
The majority of participants felt that it would be appropriate to extend the scheme to men.
The key challenges were geography and time limitations.
Significance of this study
What is already known on this topic?
Recruitment of women into gastroenterology and leadership roles has traditionally been difficult. Mentorship has long been recognised as beneficial in the business world and has more recently been endorsed by medical and academic professional bodies.
What this study adds?
Mentorship is shown to be beneficial despite the challenges and is likely to improve the recruitment and retention of women in gastroenterology and leadership roles. The benefit is unlikely to be specific to women.
How might it impact on clinical practice in the foreseeable future?
Benefits for participants in mentorship schemes include positive impact clinical practice, personal well-being and professional development, due to improved problem-solving skills and management of change.
References
Footnotes
Contributors RJH was involved in the training, support, study design, data collection, analysis and report provided by Habe Consulting. CE was involved with study design. The report was edited and discussion was written by KS. VW provided the introduction. All other authors are part of the SWiG network and involved in the fruition of the mentorship programme and pilot study. They also contributed to the edition of the paper.
Funding The SWiG Network received small unrestricted support monies from Abbvie and Ferring.
Competing interests CE is on the Advisory Board for MSD, Ferring & Abbvie; research grant from Takeda 2017.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.