
Abstract
Background
Current data indicate that infliximab—given immediately after surgery—may be very effective in preventing postsurgical recurrence of Crohn’s disease. However, it is unknown whether a similar benefit would result from early diagnosis and treatment, rather than prevention of endoscopic recurrence.
Aims
The primary outcome of this study was to clarify whether infliximab, given after diagnosis of postoperative endoscopic recurrence of Crohn’s diseases (Rutgeerts score ≥ 2) can induce endoscopic remission (score <2) at 54 weeks. The secondary outcomes were improvement in the endoscopic score and clinical recurrence at 54 weeks.
Methods
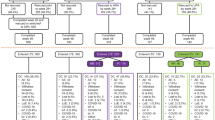
In this prospective open label multicenter pilot study 43 patients with ileocolonic Crohn’s disease subjected to curative surgery underwent colonoscopy 6 months after surgery. Patients with endoscopic recurrence (Rutgeerts score ≥2) were treated with either mesalamine 800 mg tid or infliximab 5 mg/kg bw on a maintenance basis. Colonoscopy was performed after 54 weeks of therapy.
Results
A total of 24/43 patients were diagnosed with endoscopic recurrence at 6 months. Thirteen were treated with infliximab and 11 with mesalamine. None of the 11 mesalamine-treated patients had endoscopic remission at 54 weeks. Two had clinical recurrence at 8 and 9 months. Fifty-four percent of patients treated with infliximab had endoscopic remission at 54 weeks (P = 0.01) while 69% had an improvement in the endoscopic score. None had clinical recurrence.
Conclusions
Treatment of postsurgical endoscopic lesions by infliximab appears superior to mesalamine. However, a sizeable proportion of patients did not fully benefit from this strategy.



Similar content being viewed by others


References
Sorrentino D, Terrosu G, Avellini C, et al. Prevention of postoperative recurrence of Crohn’s disease by infliximab. Eur J Gastroenterol Hepatol. 2006;18:457–459.
Sorrentino D, Terrosu G, Avellini A, et al. Infliximab and low dose methotrexate for prevention of postsurgical recurrence of ileocolonic Crohn’s disease. Arch Intern Med. 2007;167:1804–1810.
Regueiro M, Schraut W, Baidoo L, et al. Infliximab prevents Crohn’s disease recurrence after ileal resection. Gastroenterology. 2009;136:441–450.
Sorrentino D, Paviotti A, Terrosu G, et al. Low-dose maintenance therapy with infliximab prevents postsurgical recurrence of Crohn’s disease. Clin Gastroenterol Hepatol. 2010;8:591–599.
Biancone L, Cretella M, Tosti C, et al. Local injection of infliximab in the postoperative recurrence of Crohn’s disease. Gastrointest Endosc. 2006;63:486–492.
Yamamoto T, Umegae S, Matsumoto K, et al. Impact of infliximab therapy after early endoscopic recurrence following ileocolonic resection of Crohn’s disease: a prospective pilot study. Inflamm Bowel Dis. 2009;15:1460–1466.
Sorrentino D, Paviotti A. Infliximab for postsurgical endoscopic recurrence of Crohn’s disease: no trumpets yet. Inflamm Bowel Dis. 2009;15:1458–1459.
Bratcher JM, Korelitz BI. Toxicity of infliximab in the course of treatment of Crohn’s disease. Expert Opin Drug Saf. 2006;5:9–16.
Lewis JD, Schoenfeld P, Lichtenstein GR. An evidence-based approach to studies of the natural history of gastrointestinal diseases: recurrence of symptomatic Crohn’s disease after surgery. Clin Gastroenterol Hepatol. 2003;1:229–236.
Jewell DP, Satsangi J, Lobo A, et al. Infliximab use in Crohn’s disease: impact on health care resources in the UK. Eur J Gastroenterol Hepatol. 2005;17:1047–1052.
Rutgeerts P, Geboes K, Vantrappen G, et al. Predictability of the postoperative course of Crohn’s disease. Gastroenterology. 1990;99:956–963.
Camma C, Giunta M, Rosselli M, Cottone M. Mesalamine in the maintenance treatment of Crohn’s disease: a metaanalysis adjusted for confounding variables. Gastroenterology. 1997;113:1465–1473.
Vermeire S, Van Assche G, Rutgeerts P. Laboratory markers in IBD: useful, magic, or unnecessary toys? Gut. 2006;55:426–431.
Hanauer SB, Korelitz BI, Rutgeerts P, et al. Postoperative maintenance of Crohn’s disease remission with 6-mercaptopurine, mesalamine, or placebo: a 2-year trial. Gastroenterology. 2004;127:723–729.
Sandborn WJ, Feagan BG, Hanauer SB, et al. A review of activity indices and efficacy endpoints for clinical trials of medical therapy in adults with Crohn’s disease. Gastroenterology. 2002;122:512–530.
Sorrentino D, Paviotti A. Postoperative recurrence of Crohn’s disease: the beginning of the end? Gastroenterology. 2009;137:1181–1182.
Regueiro M, Kip KE, Schraut W, et al. Crohn’s disease activity index does not correlate with endoscopic recurrence one year after ileocolonic resection. Inflamm Bowel Dis. 2011;17:118–126.
Van Assche G, Dignass A, Reinisch W, et al. The second European evidence-based consensus on the diagnosis and management of Crohn’s disease: special situations. Journal of Crohn’s and Colitis. 2010;4:63–101.
Fleiss JL, Tytun A, Ury HK. A simple approximation for calculating sample sizes for comparing independent proportions. Biometrics. 1980;36:343–346.
Pinheiro JC, Bates DM. Mixed-effects models in S and S-PLUS. New York: Springer; 2000.
Holm SA. Simple sequentially rejective multiple test procedure. Scand J Stat. 1979;6:65–70.
Peyrin-Biroulet L, Loftus EV Jr, Colombel JF, Sandborn WJ. The natural history of adult Crohn’s disease in population-based cohorts. Am J Gastroenterol. 2010;105:289–297.
De Cruz P, Kamm MA, Prideaux L, Allen PB, Desmond PV. Postoperative recurrent luminal Crohn’s Disease: a systematic review. Inflamm Bowel Dis 2011. (Epub ahead of print). doi:10.1002/ibd.21825.
Sorrentino D, Paviotti A, Fiorino G. Anti-TNF’s for postoperative recurrence in Crohn’s disease: the if’s and how’s. Curr Drug Targets. 2010;11:219–226.
Bernstein CN. Anti-tumor necrosis factor therapy in Crohn’s disease: more information and more questions about the long term. Clin Gastroenterol Hepatol. 2010;8:556–558.
Peyrin-Biroulet L, Bigard MA, Malesci A, et al. Step-up and top-down approaches to the treatment of Crohn’s disease: early may already be too late. Gastroenterology. 2008;135:1420–1422.
Sachar DB. Recurrence rates in Crohn’s disease: predicting the future and predicting the past. Gut. 2006;55:1069–1070.
Parsi MA. Does smoking decrease the response to infliximab in patients with Crohn’s disease? Inflamm Bowel Dis. 2008;14:S18–S19.
Gisbert JP, Panés J. Loss of response and requirement of infliximab dose intensification in Crohn’s disease: a review. Am J Gastroenterol. 2009;104:760–767.
Danese S. Mechanisms of action of infliximab in inflammatory bowel disease: an anti-inflammatory multitasker. Dig Liver Dis. 2008;40:S225–S228.
Barnes MJ, Powrie F. Regulatory T cells reinforce intestinal homeostasis. Immunity. 2009;31:401–411.
Miossec P, Korn T, Kuchroo VK. Interleukin-17 and type 17 helper T cells. N Engl J Med. 2009;361:888–898.
Lamb CA, Mohiuddin MK, Gicquel J, et al. Faecal calprotectin or lactoferrin can identify postoperative recurrence in Crohn’s disease. Br J Surg. 2009;96:663–674.
Renna S, Cammà C, Modesto I, et al. Meta-analysis of the placebo rates of clinical relapse and severe endoscopic recurrence in postoperative Crohn’s disease. Gastroenterology. 2008;135:1500–1509.
D’Haens GR, Vermeire S, Van Assche G, et al. Therapy of metronidazole with azathioprine to prevent postoperative recurrence of Crohn’s disease: a controlled randomized trial. Gastroenterology. 2008;135:1123–1129.
Ardizzone S, Maconi G, Sampietro GM, et al. Azathioprine and mesalamine for prevention of relapse after conservative surgery for Crohn’s disease. Gastroenterology. 2004;127:730–740.
Herfarth H, Tjaden C, Lukas M, et al. Adverse events in clinical trials with azathioprine and mesalamine for prevention of postoperative recurrence of Crohn’s disease. Gut. 2006;55:1525–1526.
Peyrin-Biroulet L, Deltenre P, Ardizzone S, et al. Azathioprine and 6-mercaptopurine for the prevention of postoperative recurrence in Crohn’s disease: a meta-analysis. Am J Gastroenterol. 2009;104:2089–2096.
Reinisch W, Angelberger S, Petritsch W, et al. Azathioprine versus mesalazine for prevention of postoperative clinical recurrence in patients with Crohn’s disease with endoscopic recurrence: efficacy and safety results of a randomised, double-blind, double-dummy, multicentre trial. Gut. 2010;59:752–759.
Ford AC, Khan KJ, Talley NJ, Moayyedi P. 5-Aminosalicylates prevent relapse of Crohn’s disease after surgically induced remission: systematic review and meta-analysis. Am J Gastroenterol. 2011;106:413–420.
Conflict of interest
D. Sorrentino: advisory board, consultant and research grants from Schering-Plough-Merck, Centocor, Abbott, Roche, Giuliani and UCB Pharma. G. Zoli: advisory board and consultant for Schering-Plough-Merck. W. Fries: advisory board and research grants from Schering-Plough-Merck; advisory board for Abbott. S. Danese: advisory board, consultant and research grants from Schering-Plough-Merck, Centocor, Abbott, UCB Pharma, Ferring and Takeda. The other authors have no potential conflicts of interest to disclose. This study was not sponsored by the pharmaceutical industry.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sorrentino, D., Terrosu, G., Paviotti, A. et al. Early Diagnosis and Treatment of Postoperative Endoscopic Recurrence of Crohn’s Disease: Partial Benefit by Infliximab—A Pilot Study. Dig Dis Sci 57, 1341–1348 (2012). https://doi.org/10.1007/s10620-011-2025-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-011-2025-z