Article Text

Abstract
Aims: Exposure to diagnostic radiation may be associated with increased risk of malignancy. The aims of this study were to (1) examine patterns of use of imaging in Crohn’s disease; (2) quantify the cumulative effective dose (CED) of diagnostic radiation received by patients; and (3) identify patients at greatest risk of exposure to high levels of diagnostic radiation.
Methods: 409 patients with Crohn’s disease were identified at a tertiary centre. CED was calculated retrospectively from imaging performed between July 1992 and June 2007. High exposure was defined as CED>75 mSv, an exposure level which has been reported to increase cancer mortality by 7.3%. Complete data were available for 399 patients. 45 were excluded (20 attended outside the study period, 25 were primarily managed at other centres).
Results: Use of computed tomography increased significantly and accounted for 77.2% of diagnostic radiation. Mean CED was 36.1 mSv and exceeded 75 mSv in 15.5% of patients. Factors associated with high cumulative exposure were: age <17 years at diagnosis (hazard ratio 2.1, confidence interval (CI) 1.1 to 4.1), upper gastrointestinal tract disease (odds ratio (OR) 2.4, CI 1.2 to 4.9), penetrating disease (OR 2.0, CI 1.0 to 3.9) and requirement for intravenous steroids (OR 3.7, CI 2.0 to 6.6); infliximab (OR 2.3, CI 1.2 to 4.4); or multiple (>1) surgeries (OR 2.7, CI 1.4 to 5.4).
Conclusions: Identifiable subsets of patients with Crohn’s disease are at risk of exposure to significant amounts of diagnostic radiation. Given the background risk of neoplasia and exposure to potentially synergistic agents such as purine analogues and other immune modulators, specialist centres should develop low-radiation imaging protocols.
Statistics from Altmetric.com
Protracted exposure to low-level ionising radiation, including diagnostic radiation, is widely believed to be associated with an increased incidence of malignancy.1–3 Diagnostic imaging is frequently essential for patients with Crohn’s disease at initial diagnosis, for monitoring response to therapy, and for peri-operative evaluation.4 Patients with Crohn’s disease require more imaging studies than patients with other forms of inflammatory bowel disease and may undergo repeated imaging studies over years of illness.5 While the association between diagnostic radiation exposure and the induction of cancers remains controversial, cumulative exposure to significant levels of ionising radiation may be of particular concern in patients with Crohn’s disease, who often present in adolescence and carry an increased life-time risk of developing small bowel lymphoma and other intestinal malignancies.6 ,7
Therefore, the aims of this study were to (1) examine patterns of use of diagnostic imaging in patients with Crohn’s disease at a tertiary referral centre; (2) quantify the associated cumulative effective dose (CED) of diagnostic radiation received by these patients; and (3) identify factors associated with exposure to high levels of diagnostic radiation. The results show increasing use of computed tomography (CT) in patients with Crohn’s disease over the 15 year study period, demonstrate that the majority of patients received a CED of less than 50 mSv, and identify subsets of patients who are at risk of high cumulative exposure.
METHOD
Study population
Individuals with Crohn’s disease were identified from the dedicated patient database of a tertiary referral centre for the treatment of inflammatory bowel disease. Demographic and clinical data were obtained by chart review. A total of 409 patients with a diagnosis of Crohn’s disease were identified. Complete data were available in 399 cases. Patients who did not attend during the study period of 1 July 1992 to 30 June 2007 were excluded (n = 20). Patients who were primarily managed at other specialist centres were also excluded (n = 25), as they were likely to undergo a significant proportion of the required imaging studies at their primary treatment centre. A total of 354 patients were included (167 men, 187 women, mean age at enrolment 32.2 years, age range 8.6–78.3 years). Mean follow-up was 6.7 years (range 0.1–14.5 years). Table 1 shows baseline characteristics at referral (gender, smoking history, family history, age at referral and age at diagnosis), and the course of disease during follow-up (Montreal classification of Crohn’s disease,8 medications required and surgical history) for the entire cohort. At study conclusion, 271 patients (76.6%) remained under active follow-up, 33 patients (9.3%) had been discharged, 38 patients (10.7%) had defaulted from further follow-up and 12 patients (3.4%) were deceased.
Diagnostic imaging
Details of all imaging studies performed on patients in the cohort during the 15 year study period were obtained from the department of radiology’s computerised imaging records (Keogh Radiology Information System version 2.7, KS Medical, Dublin, Ireland). The accuracy of the capture of all imaging studies for the population was ensured by the centralised nature of local radiology services and the use of one imaging centre for all patients, regardless of health insurance status. CED was calculated retrospectively based on all imaging studies dated from 6 months prior to first clinical contact with the gastroenterology service, to 6 months after most recent clinical contact, using the reference effective doses for diagnostic imaging studies published by the United Kingdom National Radiation Protection Board.9 (Examples are shown in table 2.)
In all cases, the indication for gastrointestinal imaging was one of the following: to establish the initial diagnosis of Crohn’s disease; to determine the extent of stricturing disease; or to detect extramural complications. Abdominal CT examinations were performed with oral and intravenous contrast enhancement, using either a single-slice CT (Siemens Somatom, Siemens Medical Solutions, Erlangen, Germany) or a four-detector CT (Toshiba Aquilon, Toshiba Medical Systems, Zoetermeer, The Netherlands).
To ensure an accurate estimate of total diagnostic radiation exposure, all imaging studies performed for non-gastrointestinal indications were also included (eg, neuro-imaging, skeletal films, angiography). High cumulative exposure to diagnostic radiation was defined as CED exceeding 75 mSv (effective dose equivalent to 3750 standard chest x rays). Cumulative exposure to low-level ionising radiation of this magnitude has previously been estimated to increase mortality due to all cancers by 7.3%.10
Data analysis
Data compilation and statistical analyses were performed using Microsoft Access 2007 (Microsoft Corporation, Washington, USA), GraphPad Prism version 5.01 (GraphPad Software Incorporated, San Diego, USA) and Stata version 10.0 (StataCorp, College Station, Texas, USA). Analyses of the difference between groups of non-parametric data were performed using the Mann–Whitney U test or the Kruskall–Wallace test, as appropriate. The associations between baseline characteristics at referral and diagnostic radiation exposure were calculated by Cox proportional hazards analysis (expressed as hazard ratios (HRs)). The associations between course of disease during follow-up and diagnostic exposure were analysed by logistic regression (expressed as odds ratios (ORs)). Analyses were adjusted for duration of follow-up.
RESULTS
Increasing use of diagnostic imaging
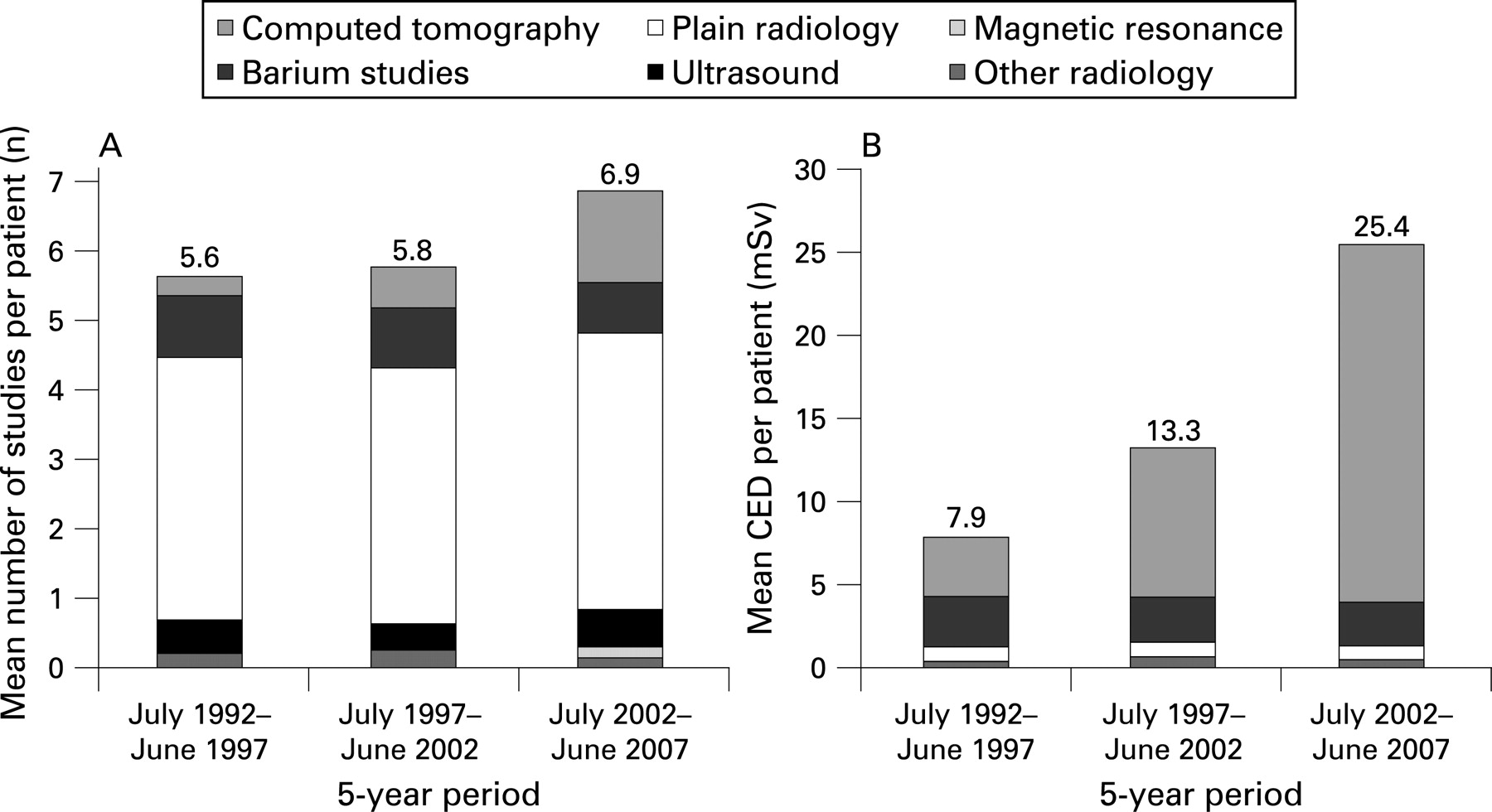
During the study period there were increases in both the number of studies performed per patient and the amount of diagnostic radiation received by patients (fig 1).

During the first 5 years of the 15 year study, the mean number of imaging studies performed per patient attending was 5.6 (95% CI 4.4 to 6.8 studies/patient) and the mean CED received by patients who underwent imaging was 7.9 mSv (95% CI 5.3 to 9.8 mSv/patient). Computed tomography (CT) accounted for 5.2% of imaging studies performed and 46.3% of radiation exposure during this first 5 years.
In the final 5 years of the study period, the mean number of studies performed per patient had increased to 6.9 (95% CI 5.8 to 8.0 studies/patient) and the mean CED of diagnostic radiation for patients who underwent imaging was 25.1 mSv (95% CI 21.1 to 29.1 mSv/patient). Of the imaging studies performed during this period, 19.7% were CT scans, accounting for 84.7% of diagnostic radiation.
Over the entire study period, CT imaging accounted for 16.2% of imaging studies performed and 77.2% of all diagnostic radiation. The increased frequency of CT imaging coincided with a decreased utilisation of barium studies. During the first, second and third 5 year intervals of the study period, barium studies accounted for 15.7%, 14.6% and 10.2% of studies performed, respectively. Magnetic resonance imaging accounted for less than 1% of imaging studies in the period July 1992 to June 2002 and accounted for 2.1% of studies in the subsequent final 5 years of the study period. The numbers of plain radiographs, ultrasound studies and other imaging studies (eg, nuclear medicine, angiography, endoscopic retrograde cholangiopancreatography) remained relatively constant, accounting for 70.5% of all studies recorded and 8.1% of all diagnostic radiation.
Cumulative effective dose received by patients
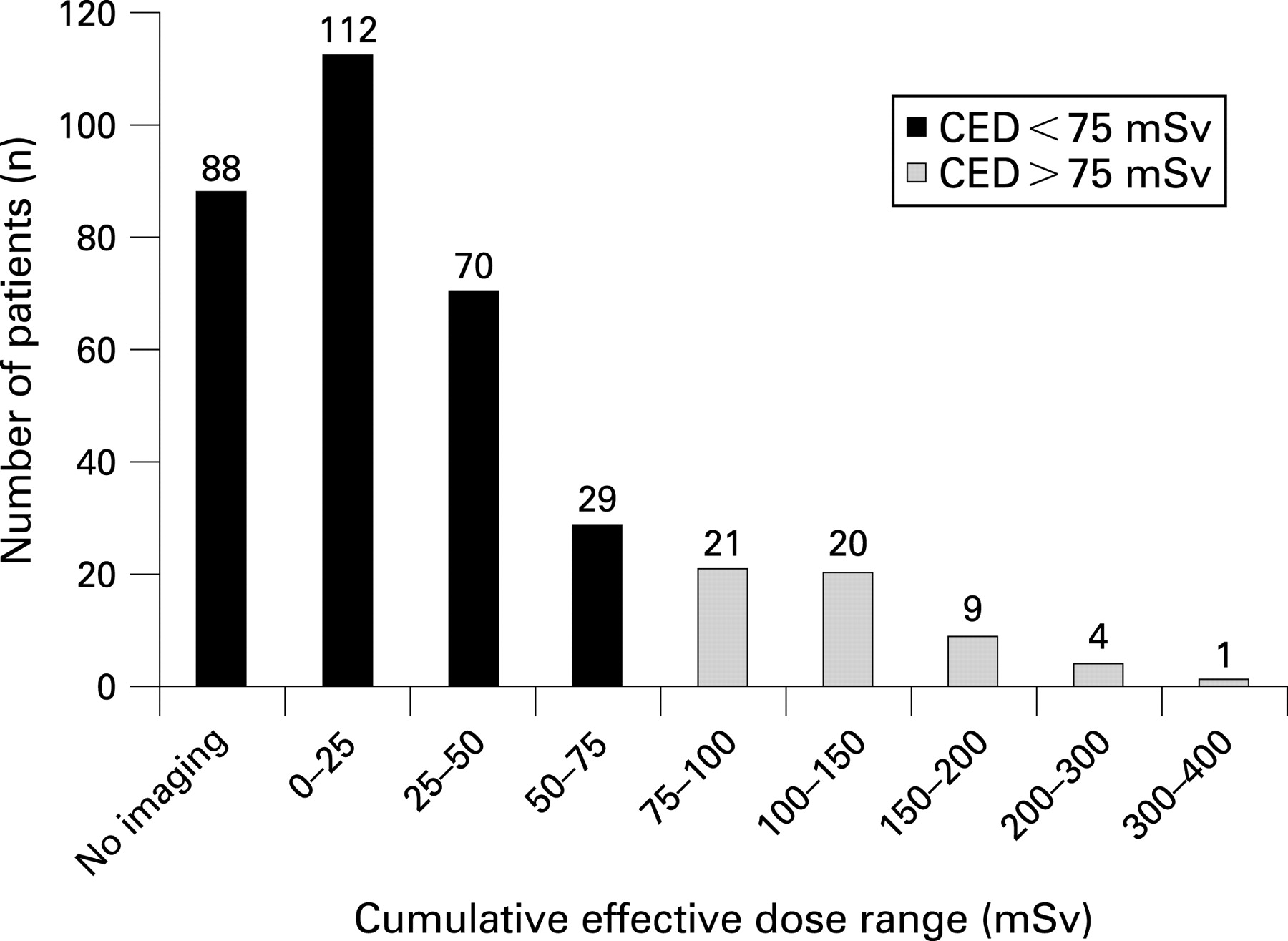
A total 4392 imaging studies were performed, exposing the population to an estimated 12 780 mSv of ionising radiation. The mean CED per patient was 36.1 mSv (95% CI 30.8 to 41.4 mSv, fig 2). Patients received a mean 8.1 mSv of diagnostic radiation per year of follow-up (95% CI 6.5 to 9.7 mSv/year). The mean number of studies performed per patient was 12.4 (95% CI 10.5 to 14.3 studies). Two hundred and sixty-six patients (75.1% of cohort) underwent at least one diagnostic imaging study (fig 3).

Patients at risk of high exposure (CED >75 mSv)
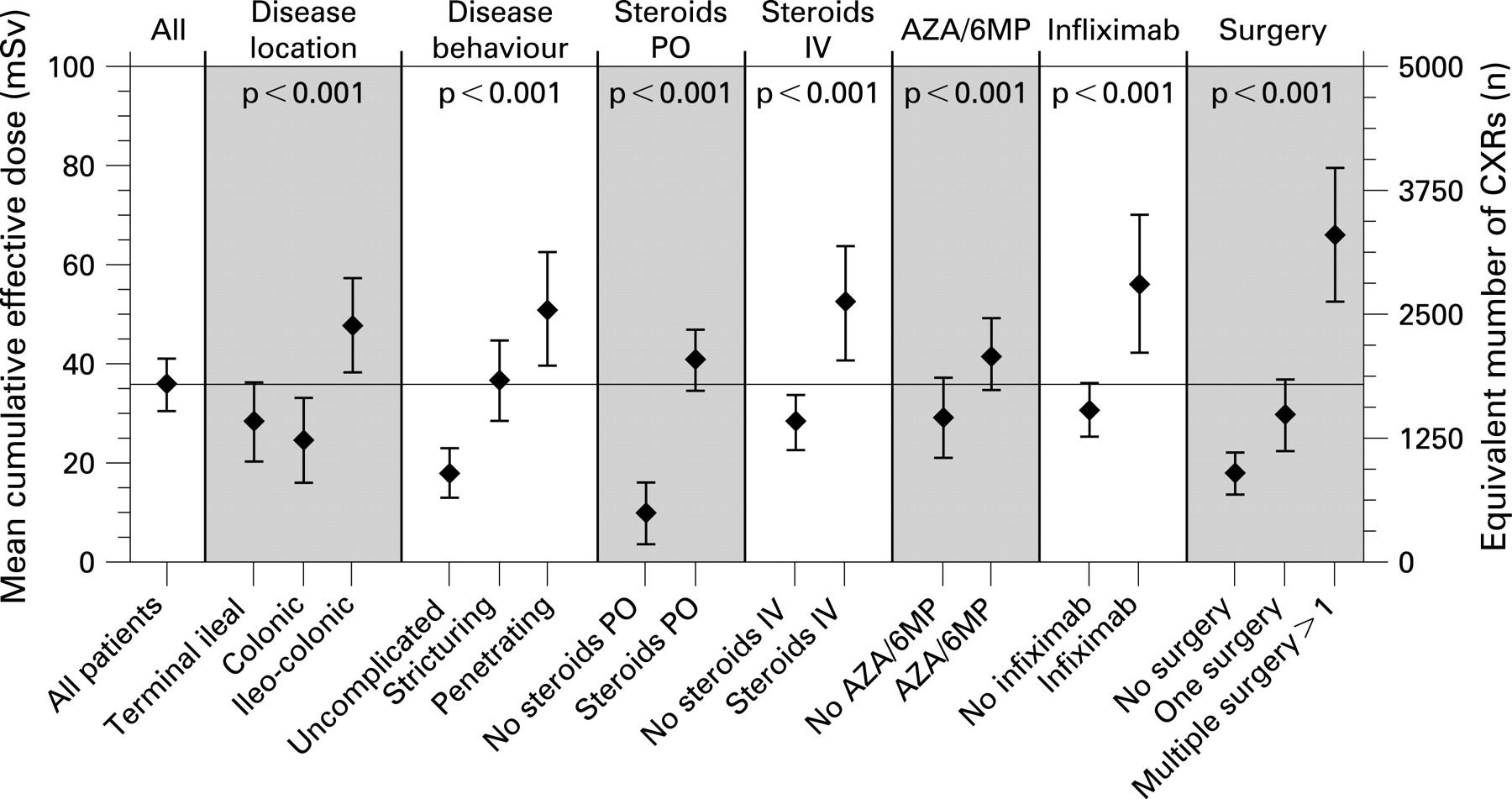
Total CED exceeded 75 mSv in 55 of the 354 patients (15.5%, fig 3). The mean time from enrolment to high exposure was 6.2 years (95% CI 5.3 to 7.2 years). The mean age of patients upon reaching high CED was 39.1 years (range 16.9 to 84 years). Table 1 shows the associations between patient factors and high cumulative exposure, adjusted for duration of follow-up.
Among the baseline characteristics examined, only age at diagnosis influenced cumulative exposure. Patients aged less than 17 years who were diagnosed with Crohn’s disease were more likely to receive a high CED (HR 2.1, 95% CI 1.1 to 4.1, p = 0.02).
Disease distribution and disease behaviour both had significant associations with exposure (table 1 and fig 2). Patients with ileo-colonic disease received a higher mean CED than those with ileal or colonic disease alone (mean CED 49 vs 27 mSv, respectively, p<0.0001). Patients with upper gastrointestinal tract involvement were more likely to receive high CED (OR 2.4, 95% CI 1.2 to 4.9, p = 0.02). Exposure was significantly lower among patients with non-stricturing, non-penetrating disease behaviour, than among those with strictures or disease penetration (mean CED 18.3 vs 44.5 mSv, respectively, p<0.0001).
Patients were more likely to receive a CED in excess of 75 mSv if they required at least one course of oral steroids (OR 3.8, 95% CI 1.1 to 12.7, p<0.01), intravenous steroids (OR 3.7, 95% CI 2.0 to 6.6, p<0.0001) or infliximab (OR 2.3, 95% CI 1.2 to 4.4, p = 0.01). The association between high exposure and requirement for intravenous steroids or infliximab is shown in fig 4A. Patients who required immunosuppressive medications (6-mercaptopurine, azathioprine or methotrexate) received higher mean CED than patients who did not require immunosuppression (mean CED 42.2 vs 29.5 mSv, p<0.0001).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Patients who underwent their first surgical procedure for Crohn’s disease during the study period (n = 176) were more likely to receive a high CED (OR 3.6, 95% CI 1.7 to 7.5, p<0.001) and, in most cases (30 out of 37), reached the 75 mSv threshold subsequent to the first surgery (mean time from first surgery to high CED 3.2 years, range −4 to 11.3 years). Patients who required more than one Crohn’s-related surgery were more likely to receive high CED (fig 4B) and had the highest mean exposure of all groups (mean CED 66.6 mSv, 95% CI 52.9 to 80.3 mSv, fig 2).
Smokers did not receive a significantly higher mean CED than non-smokers (mean CED 38.4 mSv and 34.1 mSv, respectively). Linear regression demonstrated that although exposure generally increased with length of follow-up and with disease duration, these factors accounted for a small proportion of the overall variability in CED (r2 = 0.08 and 0.02, respectively).
Seven patients developed malignancies during the study period, resulting in two deaths (two cutaneous basal cell carcinomas, two cutaneous squamous cell carcinomas, one Dukes’ B colonic carcinoma, one fatal case of B cell lymphoma of small bowel, and one fatal case of metastatic melanoma). Mean CED at diagnosis of malignancy was 29.9 mSv (range 0–99.3 mSv) and exceeded 75 mSv in only one case (a cutaneous squamous cell carcinoma affecting a 74-year-old male patient).
DISCUSSION
This study has shown a notable increase in the use of CT imaging to evaluate patients with Crohn’s disease over the last 15 years. There has been a parallel increase in diagnostic radiation exposure. These findings are consistent with the rapidly increasing availability and utilisation of CT in clinical medicine worldwide.11 ,12 Although significant diagnostic radiation exposure among patients with Crohn’s disease has been reported previously,5 this study is the first to identify the subgroups of patients who are at greater risk of high cumulative exposure.
Over a mean follow-up period of 6.7 years, the majority of patients with Crohn’s disease attending a specialist centre received a CED of less than 50 mSv of diagnostic radiation. However, more than 15% of patients received cumulative doses in excess of 75 mSv. In keeping with the age profile of the entire cohort, patients in the high exposure group were young, with an average age of less than 40 years. The data indicate that eventual lifetime exposure may be higher, particularly in patients with complicated disease and those who require corticosteroids, infliximab or surgery. It is of note that patients undergoing their first surgical procedure for Crohn’s disease during the study period were more likely to receive a high CED after surgery. This suggests that imaging was performed to monitor post-operative progress or complications, a suggestion which is supported by the relatively high mean exposure among patients who required multiple surgical procedures.
Although the computerised records of imaging procedures were complete, it was not possible to retrospectively measure the actual effective dose incurred by the cohort over the 15 year study period. For this reason, CED was calculated using the detailed reference effective doses published by the UK National Radiation Protection Board.9 Given the complexity of imaging the diseased bowel, abdominal imaging studies in Crohn’s disease may involve higher exposures than the quoted effective doses. While retrospective calculations may therefore underestimate the actual CED somewhat, the central message of the results would most likely have been similar if conducted prospectively. Furthermore, the retrospective approach avoided any confounding influence on investigator behaviour that may occur with a prospective study in this setting.
The potentially carcinogenic impact of ionising radiation may be particularly relevant to patients with Crohn’s disease, who are at increased risk of developing gastrointestinal carcinoma and tumours of the liver or biliary tract,6 and carry a significant excess risk of developing small bowel lymphoma.7 There is general consensus that although the absolute risk of lymphoma in patients with Crohn’s disease is low, the relative risk increases with disease severity and with need for immunosuppression.13 ,14 It is therefore notable that in this study exposure to diagnostic radiation was higher among patients with clinical markers of increased disease severity (younger age of onset, more extensive disease, more aggressive disease behaviour and need for multiple surgeries) and patients who required 6-mercaptopurine, azathioprine or infliximab.
During the follow-up period, malignancies occurred in seven patients, five of whom developed skin cancers and two of whom were diagnosed with gastrointestinal malignancy. In all but one case, CED was less than 75 mSv when the cancer was diagnosed. Due to the low overall incidence of cancers in patients with Crohn’s disease, examination of a causal link with diagnostic radiation exposure at the levels we have reported would require an extremely large cohort with follow-up extended to several decades.
It has been estimated that diagnostic imaging results in 5500 deaths due to radiation-induced cancers in the United States each year.15 ,16 The US National Research Council estimates that for every 1000 patients undergoing a 10 mSv CT examination of the abdomen, one patient will develop a radiation-induced neoplasm in their lifetime.1 A balanced review of the issues and evidence regarding links between diagnostic radiation and the induction of cancer has recently been published.2
Although the association between diagnostic x ray exposure and cancer remains the subject of debate,2 ,3 several epidemiological studies have shown direct evidence of increased cancer-related mortality following protracted exposure to low levels of ionising radiation, including diagnostic radiation.10 ,17–19 Occupational exposure to a cumulative dose of 75 mSv of ionising radiation has been associated with a 7.3% increase in mortality due to all cancers.10 In the context of such epidemiological evidence, the CED of diagnostic radiation we report in certain patients with Crohn’s disease may represent potentially harmful exposure.
Computed tomography imaging offers many advantages in the assessment of complicated Crohn’s disease: widespread availability; high sensitivity and specificity for detection of luminal and extra-luminal disease;20 rapid acquisition of images with high spatial and temporal resolution; and a shorter overall acquisition time compared to conventional enterography and magnetic resonance imaging (MRI).21 However, it should be borne in mind that the effective dose of radiation from most CT studies is relatively high compared to other modalities.9 ,22 Strategies to reduce the effective dose of radiation incurred by patients undergoing CT imaging can be employed without sacrificing image quality12 ,23 and should be considered for all patients, particularly those who are likely to require multiple examinations.
In many clinical scenarios, imaging modalities which impart no radiation dose have proven efficacy in inflammatory bowel disease.20 ,21 ,24–27 The use of ultrasound imaging to assess Crohn’s disease is well established, particularly as part of the initial screening of symptomatic patients and follow-up imaging of patients with a known diagnosis of small-bowel Crohn’s disease.26 ,27 Ultrasonography is non-invasive, inexpensive, widely available and well tolerated by patients. However, diagnostic performance is operator-dependent, sensitivity for the detection of fistulae is low and there is poor correlation between ultrasound findings and disease activity.24
The study period extended from July 1992 to June 2007. Clinically useful MRI evaluation of the bowel has only been available since the late 1990s.24 MRI has several advantages over CT for the patient with Crohn’s disease:21 ,24 ,28 submucosal enhancement can differentiate active inflammation from wall-thickening alone; and improved soft tissue contrast gives better visualisation of fistulae and peri-anal disease. MRI is radiation-free, which allows for safe real-time magnetic resonance fluoroscopy if required. However, in addition to limited availability and higher costs compared to other modalities, the use of MRI is often restricted by increased acquisition time and patient discomfort.25 In many centres, specialties outside of gastroenterology are prioritised for MRI access (eg, orthopaedics, neurology and rheumatology).21 For these reasons, MRI accounted for less than 2% of imaging examinations recorded in this study. With increasing awareness of radiation exposure due to CT imaging, and improving availability of MRI facilities, it is likely that magnetic resonance enterography will emerge as an important diagnostic tool in the routine assessment of patients with Crohn’s disease.
Identifiable subsets of patients with Crohn’s disease are at risk of cumulative exposure to significant levels of diagnostic radiation, primarily due to computed tomography examinations. Patients with early onset of illness, penetrating disease and those who require corticosteroids, infliximab or multiple surgeries are at greater risk of high exposure. Given that Crohn’s disease is a life-long illness which often presents in adolescence, the background risk of neoplasia in these patients, and concomitant exposure to potentially synergistic agents such as purine analogues and other immune modulators, specialist centres should develop low-radiation imaging protocols.
REFERENCES
Footnotes
Funding: The authors are supported in part by Science Foundation Ireland, by the Health Research Board of Ireland and by the European Union.
Competing interests: None.
Ethics approval: Study approval was granted from the combined university and hospitals research ethics committee on 5 March 2006.