Article Text

Abstract
Objective: To quantify fatigue in non-alcoholic fatty liver disease (NAFLD), to determine whether perceived fatigue reflects impairment of physical function and to explore potential causes.
Patients and methods: A cohort study was carried out on 156 consecutive patients with histologically proven NAFLD studied in two cohorts. Phase 1 determined the perceived fatigue experienced by NAFLD patients (assessed using the Fatigue Impact Scale (FIS)) in comparison with normal and liver disease controls, and the relationship to physical function (actigraphy). In phase 2, biological associations of fatigue in NAFLD were explored.
Results: Fatigue was markedly higher in NAFLD patients than in controls (mean (SD) FIS 51 (38) vs 8 (12), p<0.001). NAFLD patients showed significantly lower physical activity over 6 days (7089 (2909) mean steps/day vs 8676 (2894), p = 0.02). A significant inverse correlation was seen between FIS and physical activity (r2 = 0.1, p = 0.02). Fatigue experienced by NAFLD patients was similar to that in primary biliary cirrhosis (n = 36) (FIS 64 (9) vs 61 (2), p = NS). No association was seen between FIS and biochemical and histological markers of liver disease severity or insulin resistance (homeostasis model assessment (HOMA)) (r2<0.005). Significant association was seen between fatigue severity and daytime somnolence (Epworth Sleepiness Scale) (r2 = 0.2, p<0.001).
Conclusion: Fatigue is a significant problem in NAFLD, is similar in degree to that in primary biliary cirrhosis patients and is associated with impairment in physical function. Fatigue in NAFLD appears to be unrelated to either severity of underlying liver disease or insulin resistance, but is associated with significant daytime somnolence.
Statistics from Altmetric.com
The term non-alcoholic fatty liver disease (NAFLD) describes a spectrum of liver histology characterised by excess fat within the liver that affects individuals who drink little or no alcohol. It ranges from simple fatty liver (steatosis), through fat with necroinflammation and/or fibrosis—so-called non-alcoholic steatohepatitis (NASH), to advanced fibrosis, cirrhosis and hepatocellular cancer (HCC).1 NAFLD is strongly associated with visceral obesity, insulin resistance, hypertension and dyslipidaemia, and is considered to be the liver manifestation of the metabolic syndrome.2 With the increasing incidence of obesity and diabetes in Western countries, NAFLD has become a growing problem, and is now recognised as the most common liver disease in these countries and the most common cause of incidental abnormal liver blood tests.3 Based on data from several recent well-conducted North American and European studies using ultrasound or MRI to diagnose hepatic steatosis, the prevalence of NAFLD in the West lies somewhere between 20 and 30%.4–6
Descriptions of patient experiences in the clinic and qualitative research would point to fatigue as a problem in those with NAFLD. There is, however, limited quantitative evidence of to what degree this perception is true.7–11 These studies were, however, limited by the approach taken for assessment of fatigue (patients were asked whether they were fatigued or not, with no attempt to quantify fatigue severity). Here we quantify, for the first time, the true impact of fatigue, its associations and relationships in a large well-characterised cohort of patients with histologically proven NAFLD.
METHODS
Subjects
The study was performed in two phases. In order to determine the degree to which fatigue is a problem in NALFD, in phase 1 we quantified fatigue and determined the prevalence of perceived fatigue and its relationship to actual activity levels in a consecutive cohort of NAFLD patients who were compared with age-, sex- and body mass index (BMI)-matched normal and liver controls. Normal controls were obtained from our large cohort of volunteers who have agreed to participate in clinical studies of fatigue pathogenesis; appropriate individuals were identified from this cohort who were age and BMI matched to the NAFLD population. Normals controls were taking no potentially vasoactive medication or had significant comorbidity. In phase 2, in order to examine fatigue associations in NAFLD, we explored potential causes and consequences by using data from the Newcastle NAFLD database. This is a large continuously updated cohort of consecutive patients attending the Tertiary Liver Clinic who had had NAFLD diagnosed histologically. For the purposes of this study, only those subjects who had had liver biopsy within the past 12 months were included. The diagnosis of NAFLD was based on the following criteria: (1) elevated aminotransferases (aspartate aminotransferase (AST) and/or alanine aminotransferase (ALT)); (2) liver biopsy showing steatosis in at least 10% of hepatocytes; and (3) appropriate exclusion of liver disease of other aetiology including alcohol- or drug-induced liver disease, autoimmune or viral hepatitis, cholestatic or metabolic/genetic liver disease. These other liver diseases were excluded using specific clinical, biochemical, radiographic and/or histological criteria. All patients had a negative history of ethanol abuse as indicated by a weekly ethanol consumption of <140 g in women and <210 g in men. History of alcohol consumption was specifically investigated by interviewing the patients, and in almost all cases a close relative. In addition, blood alcohol levels were measured randomly to exclude further patients who abused alcohol.
Assessment tools
All subjects completed a series of assessment tools designed to quantify the impact of various categories of symptoms. All assessment questionnaires have been validated for self-completion and have been previously used in patients with liver disease.12 Fatigue was measured using the Fatigue Impact Scale (FIS); this is a well-validated instrument that has been extensively used in studies including a wide range of chronic diseases (including validation for use in patients with liver disease), with higher scores reflecting increasing fatigue (possible range 0–160).13–17 Depressive symptoms were examined using the Beck Inventory version 2, where a score of >20 is considered indicative of moderate or severe depression, and <20 as mild or no depression,18 Quality of life (QoL) was examined with the liver-specific instrument the Chronic Liver Disease Questionnaire (CLDQ). The CLDQ includes 29 items in the following domains: abdominal symptoms, fatigue, systemic symptoms, activity, emotional function and worry (range 29–203 from worst to best QoL).19 The Epworth Sleepiness Scale (ESS, possible score range 0–24) was used to assess daytime hypersomnolence, a score of ⩾10 being indicative of significant daytime hypersomnolence.20
Phase 1: the prevalence of fatigue in NAFLD and its relationship to physical activity
In order to explore whether similar impairment occurs in NAFLD, subjects with histologically proven NAFLD were invited to participate in studies to determine activity, how it related to fatigue and the prevalence of fatigue compared with age-, sex- and BMI-matched controls. Two age-, sex- and BMI-matched control groups were recruited who underwent the identical protocol to that of the NAFLD subjects. The first control group were normal volunteers recruited via notices in the Hospital, and the second was a liver disease comparator group of patients with primary biliary cirrhosis (PBC; the liver disease where the symptom of fatigue has been best described and studied).21–27 Subjects were excluded if they had a Beck score consistent with depression. All subjects attended for six complete days of physical activity monitoring as described below. All subjects gave fully informed consent. In all subjects, details of height, weight, BMI, evidence of comorbidity, such as diabetes, and medication use were recorded. Physical activity monitoring was performed by accelerometry over a constant 6 day period (Tuesday 14:00 to Monday 12:00) using the Actigraph system (Actigraph; MTI Health Services, Pensacola, Florida, USA; http://www.theactigraph.com/). The monitors were belt-worn at the waist and initialised for the pedometer mode. These devices has been extensively validated against physical activity diaries and other methods of activity monitoring28–30 Data were downloaded after 6 days and analysed using the manufacturer’s Windows-based software (Actisoft). Normative values for activity levels (based on the number of steps) have previously been established in the UK (http://www.nationalobesityforum.org.uk/APPG%201%20April%2004.pdf). Subjects taking under 5000 steps per day are classified as “sedentary”, those taking between 5000 and 7499 steps/day as “low active”, between 7500 and 9999 steps/day as “somewhat active” and <10 000 steps/day as “active”.
Phase 2: associations of fatigue in NAFLD
In all subjects included in the Newcastle NAFLD database, liver function tests (LFTs) and insulin resistance were determined from blood sampled on the same day as liver biopsy was performed. LFTs included albumin, platelets, liver enzymes, immunoglobulins and bilirubin. Insulin resistance was measured using the HOMA (homeostasis model assessment) index (calculated as fasting (glucose × insulin)/22.5).31
Liver biopsy was performed for clinical purposes in all patients and immediately fixed in formalin. Paraffin-embedded sections of 5 μm thick were stained with H&E, Masson’s trichrome and periodic acid–Schiff (PAS) after diastase digestion. Each biopsy was evaluated by an experienced pathologist for the severity of steatosis (<33% of hepatocytes containing fat, grade 1; 33–66%, grade 2; >66% grade 3), the presence of hepatocyte injury (ballooning; scored from 0 to 2, lobular inflammation scored from 0 to 3) and the stage of fibrosis (pericellular/perivenular or periportal fibrosis, stage 1; pericellular/perivenular and periportal fibrosis, stage 2; bridging fibrosis, stage 3; cirrhosis, stage 4) using the National Instititue of Health Clinical research Network scoring system. Necroinflammatory score was calculated as the sum of ballooning plus lobular inflammation scores.32
Statistical analysis
Data were analysed using Graphpad Statistical Software. All variables were parametric and therefore comparisons between groups were by one-way analysis of variance (ANOVA) and by Student t test. Correlations between individual parameters were assessed by Spearman rank test. Corrections were made for multiple testing (Bonferroni correction) and therefore a difference was considered statistically significant when p<0.005. Multivariate analysis was performed using SPSS (SPSS- Corps, Chicago, Illinois, USA).
RESULTS
Phase 1: the relationship between perceived fatigue and physical activity in NAFLD
Impact of fatigue in NAFLD and matched controls.
In order to determine fatigue severity and its relationship to physical activity, 36 subjects with histologically proven NAFLD were invited to participate in studies to determine activity, how it related to fatigue and the prevalence of fatigue compared with matched controls. Activity monitoring was also performed in 36 age-, sex- and BMI-matched control subjects. Details of this group are shown in table 1. Fatigue severity (measured by the FIS) was significantly higher in the NAFLD group compared with controls (mean (SD) 51 (38) vs 8 (12); p<0.001) (fig 1).

The relationship between fatigue status and activity in NAFLD.
Compared with the matched controls, the NAFLD patients took significantly fewer steps per day and more controls achieved the recommended >7500 steps per day level of activity (table 1, fig 2). In the NAFLD population there was a significant inverse correlation between fatigue severity and mean number of steps per day (p = 0.02) (fig 3). When depression screener scores were considered as a covariate in a multivariate model, this relationship remained significant (p = 0.04),


There were significantly more diabetics in the NAFLD group, which could potentially confound the results. However, when the diabetics were compared with the non-diabetic NAFLD patients there were no significant differences in BMI, fatigue scores or activity levels (data not shown).
Fatigue status and activity in NAFLD compared with PBC.
PBC is the liver disease that is classically associated with fatigue.17–23 PBC predominantly affects women and therefore in order to compare the prevalence of fatigue and activity levels in NAFLD with those in PBC patients, the data from the 18 female NAFLD patients were compared with those of 18 matched female normal controls and of a cohort of 36 age- and BMI-matched females with PBC (matched 2 to 1). FIS scores were not significantly different between female NAFLD and PBC subjects, nor were the levels of activity or the number of steps taken (table 2).
Phase 2: fatigue and its associations in NAFLD
To investigate the degree of fatigue and its associations in patients with NAFLD, the Newcastle NAFLD database was interrogated and all patients diagnosed histologically within the previous 12 months were included (n = 120). The values from the CLDQ domains confirm that patients with NAFLD are highly symptomatic to a degree comparable with that seen in severe stages of chronic liver disease25 (table 3). There were strong negative correlations between the FIS scores and all domains of the CLDQ, underlining the fact that fatigue is a major determinant in all features of health-related QoL in NAFLD.
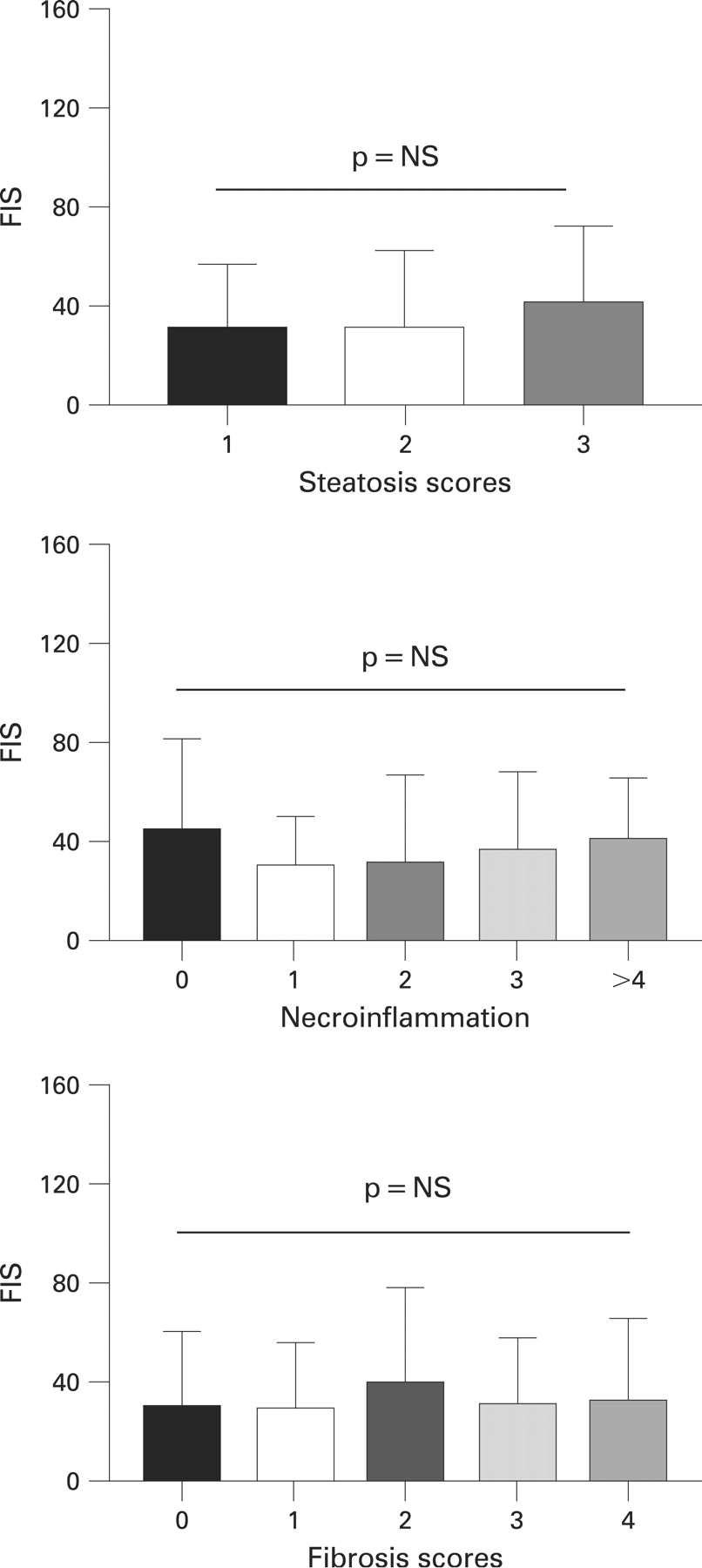
To seek evidence of potential mechanisms of fatigue in NAFLD, we looked for correlations between fatigue status and clinical, biochemical and histological variables in the cohort of 120 NAFLD patients. The demographic and biochemical details of the patient cohort are shown in table 4. There were no significant correlations between FIS and LFTs, immunoglobulins or HOMA values. Similarly, there were no statistical differences in FIS scores according to the severity of steatosis, fibrosis or the presence of hepatocyte injury (fig 4). FIS was found to correlate with the Beck depression score (p<0.001, r2 = 0.5). In order to consider the potential confounding effect of depression, we went on to consider the associations when those with moderate or severe depression were excluded (n = 33). There were no significant correlations found between fatigue and any biochemical or histological parameter of liver disease severity in those with no or mild depression (n = 87) (all p>0.1, r2<0.01).
A strong correlation was seen between FIS and ESS (p<0.001; r2 = 0.2; fig 5) which remained significant after correction for multiple testing and after inclusion in a multivariate model with depression screener scores included as a covariate (p<0.001), suggesting that increasing fatigue is associated with excessive daytime somnolence. There was no correlation between ESS and any biochemical or histological parameter of liver disease severity, HOMA, BMI, age or sex. In order to explore this more fully and determine whether elevated ESS or FIS or both were influenced by liver disease severity, the whole group were separated into those with excessive daytime somnolence (ESS>10) with and without significant fatigue (mean (SD) FIS values from the normal control population from phase 1 (ie, FIS ⩾29)) and potential differences between groups explored (table 5). No significant differences were found between the NAFLD subgroups.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
Metabolic syndrome and its hepatic manifestation, NAFLD, are considered a global epidemic. This study has shown in a large well-characterised cohort with NAFLD that the symptom of fatigue is a significant problem in this patient group. The association between NAFLD and increased BMI has led to the assumption that symptoms such as fatigue are related to excess weight (“tired fat people”); however, we have shown that when compared with an age-, sex- and BMI-matched normal control population, NAFLD patients have higher fatigue levels and reduced physical activity despite comparable BMI, and this appears to be unrelated to depression. This study has gone someway to refute the misconception that symptoms such as fatigue are related entirely to excess weight, and may now allow directed studies into the pathogenesis of fatigue in NAFLD.
It is possible that the results of our study are influenced by the healthy control group that we have studied. Despite the fact that they were not specifically selected, this control group appears to have low levels of fatigue compared with control groups in other recent studies.16 17 In order to confirm whether fatigue is a problem in NAFLD, we also compared our results with those of another fatigue-associated liver disease, PBC. The severity of fatigue experienced by those with NAFLD appears to be comparable with that experienced by patients with the autoimmune liver disease PBC22–27 and, as in PBC, is associated with a reduction in physical activity23 and excessive daytime somnolence.33 We have confirmed that in NAFLD, as in PBC, fatigue severity is unrelated to the severity of the underlying liver disease, measured by conventional parameters of liver disease severity such as liver biochemistry and albumin, and also liver histology.22–27 In addition, our study has also shown that fatigue in NAFLD is unrelated to insulin resistance. These findings have implications for the clinical management of patients with NAFLD as they would suggest that improving the liver abnormality, or treating the underlying insulin resistance, may not impact significantly upon QoL in general and fatigue severity in particular.
The finding of a relationship between excessive daytime somnolence and fatigue in NAFLD raises the question of the role of obstructive sleep apnoea (OSA) in the pathogenesis of fatigue in NAFLD. It is certainly possible that the increased prevalence of OSA reported in patients with NAFLD34–36 accounts for a proportion of the fatigue seen in NAFLD. We would suggest that although OSA may be a cause of excessive daytime sleepiness and fatigue in some patients with NAFLD, this is not the whole answer, which is clear when the number of NALFD patients with ESS<10 who are fatigued is considered (n = 34). This is further reinforced by our findings that the gold standard subjective measure of excessive daytime sleepiness, the ESS, did not correlate with insulin resistance or liver disease severity, parameters that have in previous studies been found to be correlated with the severity of OSA.36 We would suggest that as in PBC,33 excessive daytime somnolence and related fatigue occurs in NAFLD, and that in a proportion of patients this is related to the presence of OSA. Our findings suggest, however, that this proportion is small and that the remainder experience these symptoms not due to OSA but to another process (or processes) arising as a direct consequence of NAFLD per se or associated with NAFLD.
In order to determine whether fatigue severity was related to liver disease severity, we chose to include only patients in whom the diagnosis of NAFLD had been confirmed by liver biopsy. It is our clinical practise to perform liver biopsy in this patient group, but it could be argued that NAFLD patients referred to a tertiary referral hospital who have a biopsy might have more severe liver disease. The finding of no association between liver histological parameters and fatigue severity would suggest that despite this potential confounder, the results from this study would be applicable to NAFLD patients seen in routine hepatology practise.
There were strong negative correlations between fatigue and all domains of the CLDQ and depression. It is possible that fatigue is in part a psychological response to the diagnosis of a chronic liver disease; it is difficult, however, to determine the direction of this relationship and it is equally possible that impact upon QoL and associated depression are a consequence of fatigue, as has been found in other chronic liver diseases.22–27 The strong correlations seen in this study between individual domains of the CLDQ are also interesting considering recent observations in PBC of the high prevalence of autonomic dysfunction in association with fatigue severity.26 27 The finding of gastrointestinal symptoms in association with fatigue points to a common underlying pathogenesis in NAFLD which recent studies in PBC suggest could be provided by autonomic dysfunction.37
The relationship between increasing fatigue and impaired physical activity in NAFLD raises interesting aetiological questions. The assumption in PBC has been that perceived fatigue leads to reduced physical activity, but there is equally the possibility that reduced exercise leads to NAFLD and associated fatigue—that is, is the symptom of fatigue cause or consequence of reduced physical activity? Further studies aimed at exercise interventions in NAFLD patients may address the direction of the relationship.
There are a number of further potential mechanisms whereby those with NAFLD might experience fatigue. First, it may be that it is the presence of metabolic syndrome itself (rather than its liver manifestation NAFLD) that is the pathogenic process that leads to the symptom of fatigue. Considering that both NAFLD and the metabolic syndrome appear to go hand in hand,38 39 it is unlikely that discriminating between these two is likely. Alternatively, fatigue in NAFLD may arise secondary to having a chronic disorder, since fatigue is frequently seen in chronic non-hepatological disorders. As an example of a direct result of NAFLD, we would suggest that fatigue may arise due to factors produced by the fatty liver acting extrahepatically (eg, in brain or muscle) to cause the symptom of fatigue, irrespective of the presence of hepatic inflammation or fibrosis. Inflammatory cytokines, reactive oxygen species (ROS) and free fatty acids (all recently shown to be systemically elevated in NAFLD)40–43 would be candidates worthy of further study in this regard. On the other hand, the fatty liver may fail to clear potential fatigue-inducing factors which would lead to their accumulation in the systemic circulation, with gut-derived endotoxin a clear candidate in this context. Kupffer cell phagocytic function is reduced in animal models of NAFLD,44 and it has recently been shown that circulating endotoxin lipopolysaccharide (LPS) levels are increased in patients with NAFLD45 and that LPS can induce the secretion of proinflammatory and potentially fatigue-inducing cytokines such as interleukin 6 and tumour necrosis factor α46 47 by adipocytes that express Toll-like receptors.48 Alternatively the association between fatigue and NAFLD may be indirect, with both related to some extrahepatic factor such as adipose tissue inflammation.49 Clearly studies that first confirm our findings in other populations and move towards understanding the pathogenesis of fatigue in NAFLD are urgently needed to identify treatment targets for the most prominent symptom in this increasing number of patients. At present, OSA, adipose tissue inflammation, circulating cytokines, lipids, ROS and endotoxin all appear to be candidates worthy of further study.
REFERENCES
Footnotes
-
Competing interests: None.
-
Ethics approval: The study was reviewed and approved by the Sunderland LREC.
-
Patient consent: All subjects gave fully informed consent.
Linked Articles
- Digest