Article Text

Abstract
Aims: To assess whether case management of frequent attenders to the emergency department (ED) reduces subsequent attendances made by these patients.
Methods: Patients who attended the ED 10 times or more over a 6-month period were identified. Their cases were assessed and care plans put in place, if appropriate. Patient attendances over the subsequent 6 months were compared.
Results: 57 patients attended the ED 10 times or more over the 6-month period (1.4% of the departmental workload). The median number of ED attendances in this patient group was 12.0 (interquartile range (IQR) 10–14). In the subsequent 6 months following case management of these patients, median attendances in the same 57 patients dropped to 6.0 (IQR 2–13, p<0.001). The total number of attendances in this patient group dropped from 720 to 499, a reduction of 31%.
Conclusions: The findings of this study suggest that individual case management and implementation of care plans may help to reduce subsequent attendances in patients who frequently attend ED.
Statistics from Altmetric.com
Every emergency department (ED) has a population of patients who frequently attend the ED for healthcare. These frequent users have been defined as “those patients who attend on multiple occasions due to non-random events” and by the same author as “those who have attended more than four times in one year”.1 This patient population is often poorly managed within ED, where failure to recognise and address their needs can potentially lead to a cycle of repeated attendances.2 These patients are a significant workload for most ED and can be looked after poorly within this environment.3 Junior doctors may, through lack of experience, over and undertreat and investigate these patients, resulting in inappropriate management.
We often fail to recognise within the busy, time-pressured ED environment that these patients represent a vulnerable population with complex health and social needs.2 3 The reasons why these patients present to the ED are often multifactorial and social isolation is common in this group.4–6 Failure to address the needs of these patients can lead to worrying cycles of health-seeking behaviour and patients receiving fragmented and poorly coordinated care.2 Studies have shown that patients who attend the ED more than three times per year have a 5% higher mortality risk than those attending the ED only once per year.7
Case management of this patient population has been used in some centres in the USA and in Australia.4 8–14 Case management involves the process of identifying the individual patient’s needs and implementing or identifying ways of meeting these needs.4 Case management deals with the medical and social needs of the patient together.11 It is unclear whether we can extrapolate results from these studies to UK-based practice as a result of differences in healthcare provision. Many patients who frequently present to ED in the USA do so because they do not have health insurance and so do not have access to primary care physicians.9
The aim of this study was to identify the most frequent attenders to an urban ED and to introduce case management for these patients. A comparison was made of the numbers of ED attendances in these patients before and after case management was introduced to see if there were differences in attendance rates.
METHODS
This study was conducted at the ED of the Royal Infirmary of Edinburgh, which is a large urban ED in south-east Scotland serving a population of 621 836. Annual ED attendances are in the region of 99 000 patients per year. The study group consisted of an ED consultant, an ED specialist registrar (who was previously a general practitioner; GP) and a clinical nurse specialist in liaison psychiatry. Patients who frequently attended the ED over a 6-month period were retrospectively identified from the electronic patient management system (Trak) as part of a pilot study. Patients who had attended 10 times or more over the period were included in the study. The study members reviewed the case records of these patients and demographic and diagnostic details were extracted. Numbers of ED attendances in these patients were analysed. Care plans were put in place, if appropriate, which were accessible in real time by care providers. The case management team made a judgement as to whether each individual patient would benefit from a care plan at that particular point in time. At the end of the subsequent 6-month period the number of attendances of these 57 patients was again extracted from the electronic patient management system so a comparison could be made.
Consent from patients and ethical approval was not sought as case management and multidisciplinary review of difficult cases should be part of the routine management of such patients. Data were analysed using Excel and SPSS and a Wilcoxon signed ranks test was applied.
RESULTS
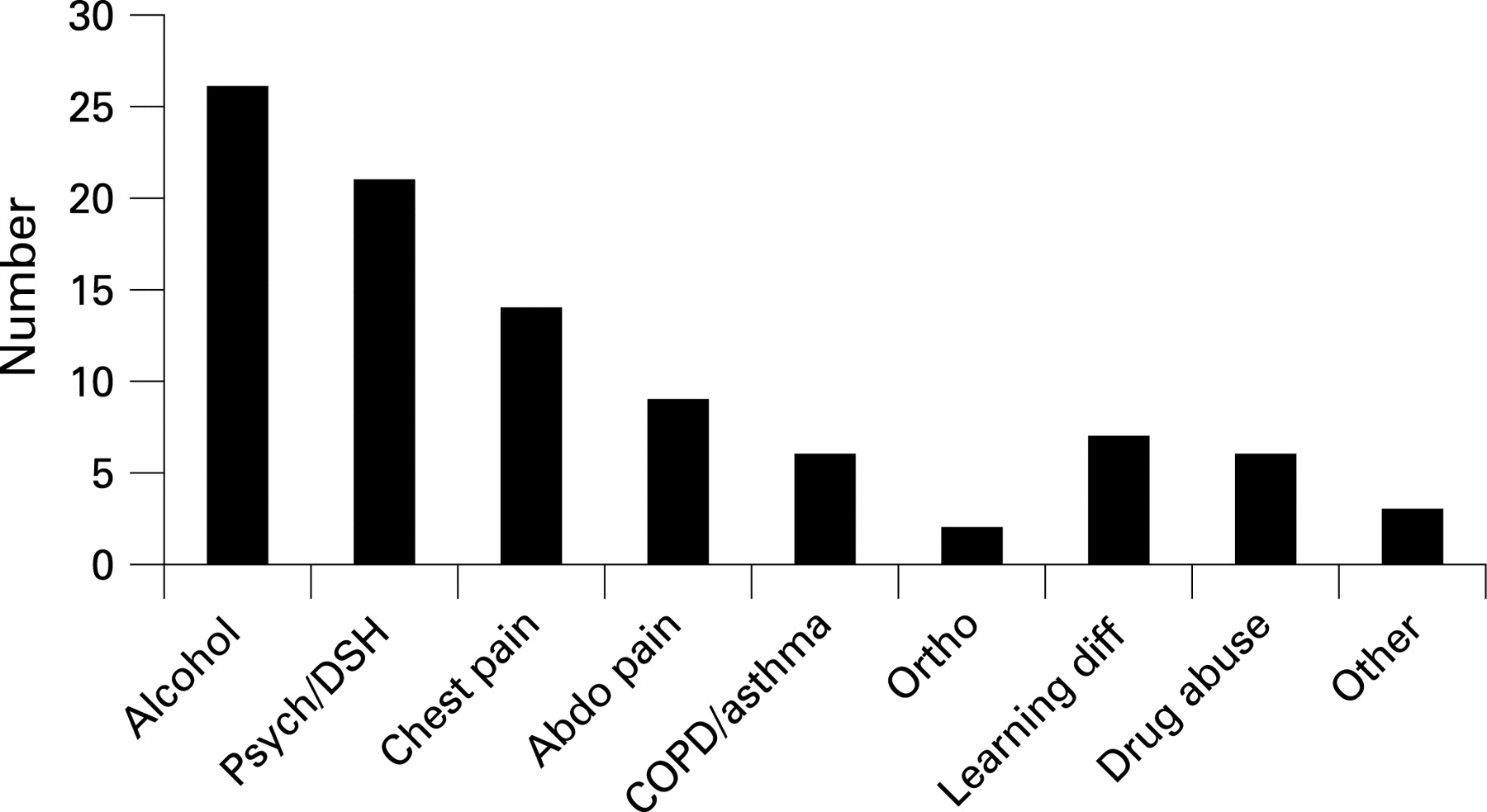
Over the 6-month period between October 2006 and March 2007, 57 patients attended the ED more than 10 times each. These 57 patients accounted for 720 ED visits, a median 12 ED attendances each (interquartile range (IQR) 10–14). Total patient attendances over this 6 months were 49 756, so these patients accounted for approximately 1.4% of the total departmental patient workload. In the 57 patients the male to female ratio was 1 : 1.8 and the mean age was 43.6 years. The documented problems or diagnoses in this group are shown in fig 1. The commonest of these included alcohol-related problems (46%), mental health problems (37%) and chronic complaints such as abdominal or chest pain (40%). Seven patients (12%) were homeless and only one patient (2%) was not registered with a GP.
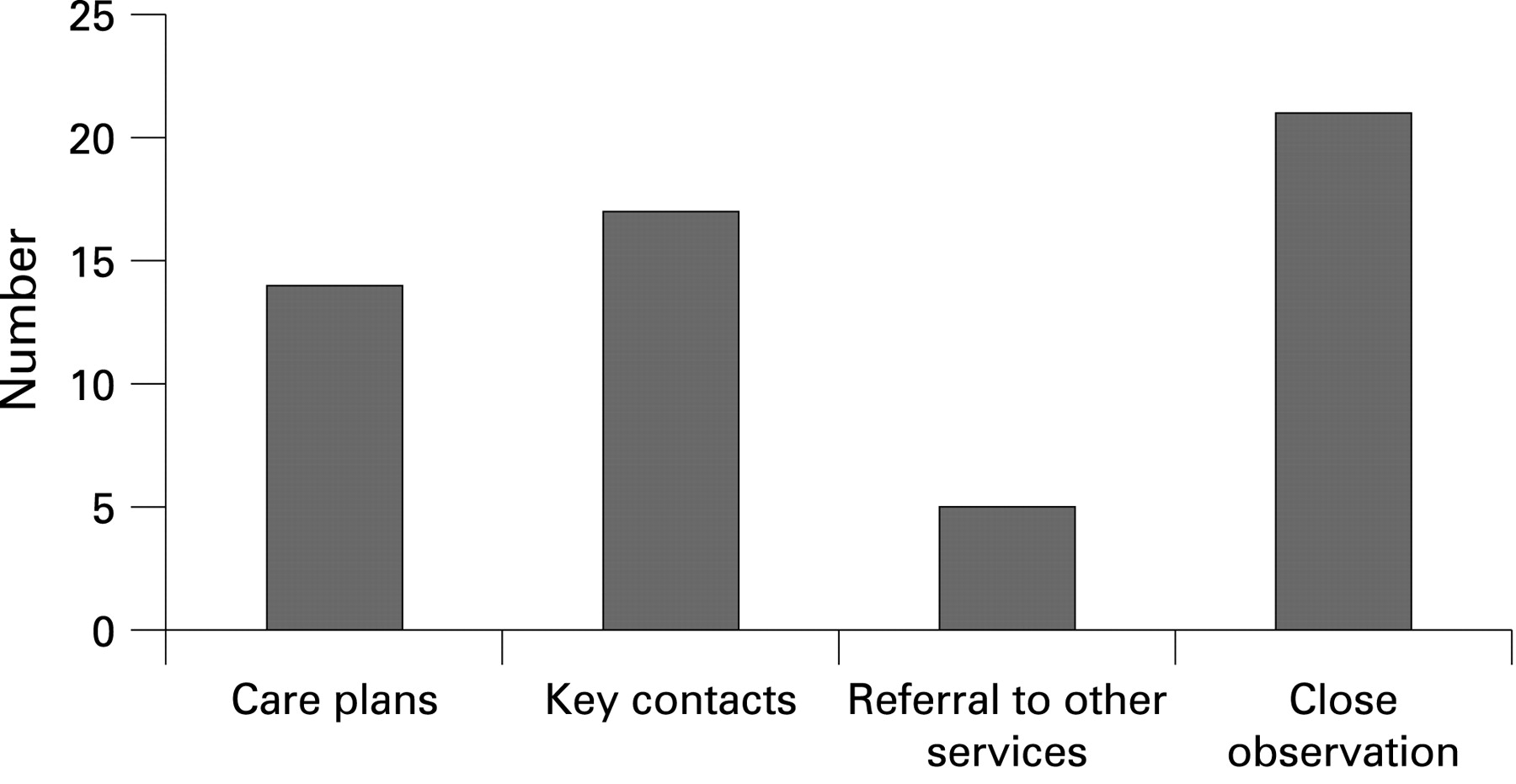
Case management of these patients consisted of a review of the individual patient’s case by the study group. Formal care plans, referrals and key contact details were put in place for 36 patients (63%) (fig 2). The remaining patients were assessed and the frequency and pattern of their ED usage was monitored. The majority of these patients showed a recent reduction in the number of attendances or were already fully engaged with services. These care plans were directly viewable by the care provider when they accessed the patient through a message placed on the electronic patient management system. An attempt was made in all of these patients to include key information here such as services that the patient was involved with, and included aspects such as key worker, community psychiatric team details and telephone numbers.

{kind=link}
{kind=link}
At the end of the subsequent 6 months, April 2007 to September 2007, following the implementation of these care plans the number of attendances in these 57 patients was again analysed. The total number of attendances fell from 720 to 499, a reduction of 31%. Median attendances fell from 12 (IQR 10–14) to six (IQR 2–13) (p<0.001). The number of attendances was reduced in 43 patients (75%). In terms of the group that received case management, a fall in the number of attendances was seen in 23 of 36 patients (64%). In the group that did not receive case management attendances fell in 18 of 21 patients (85%).
DISCUSSION
Most ED have systems in place to flag frequent ED users; many of these systems consist of special “regular” files kept at reception. A review of our case notes at reception showed that they consisted of many patients who had had a huge number of total attendances ever to the ED, in a historical sense, but did not reflect our current population of frequent attenders. Most ED frequent users are not “regular” attenders as such, but often present periodically with increased frequency, because of a medical or psychosocial crisis. For this reason it is essential that we try and identify and manage these patients in real time. Systems that can be used for this include electronic patient management systems, which flag up patients who have attended a certain number of times, for example, four times in a year. We also developed a “referral book”, which medical and nursing staff use to identify patients who they feel may merit case management. As important as identifying these patients is, it is equally important to develop a system that allows rapid access to key information. We were able to achieve this through devising alerts that allowed access to care plans and important points.
One of the major advantages of developing these initial care plans is that we became aware of the network of services that were available within the region and how to access them. We also realised that the ED probably needed to be part of the central focus in terms of addressing the problems that these patients had, as many were not well known to their primary care services and many were in fact using the ED as such a service. Previous work has shown that linking with primary care does not necessarily reduce ED attendances.11 Of our patients only one was not registered with a GP. We identified a network of interested professionals and set up a regular multidisciplinary forum to discuss the cases of frequent attenders. A broad range of enthusiastic professionals, including housing officers, social workers, the local homeless practice, psychiatric and alcohol services attended initial forums and became involved in the case management process.
Members of the multidisciplinary case management teams described in the literature include social workers and nurse case managers.4 9 13 They try and manage the diverse range of issues that are related to patients’ medical problems, for example, housing and alcohol misuse.9 Our case management team consisted of a consultant, a specialist registrar with primary care experience and a psychiatry nurse specialist. The team found the case management process very labour intensive (at least 2 h each per week) but also very satisfying. We believe that a multidisciplinary front door team consisting of a social worker, nurse specialist and alcohol counsellor could perform this role.
Previous work has concentrated on the epidemiology and demographics of frequent attenders to ED.3 Few studies have been performed looking at interventions in this patient population. The majority of the work that has been published is from the USA and Australia and similarly to our own study patient numbers were small. Okin et al9 in San Francisco introduced case management for 53 patients who attended the ED five times or more in one year and showed a reduction in mean ED visits from 15 to nine (p<0.01). They also showed that homelessness, drug and alcohol misuse reduced in this group who received the intervention. It is difficult to compare patients managed in the US healthcare system with those in the UK. Much of the case management in the USA focused on referral to a primary care physician or attaining Medicaid for patients. In our study all but one patient was registered with a GP, albeit that they may not be engaging with services there. This is often due to the chaotic lives and healthcare needs of these patients, which can often mean that they do not arrange or keep appointments.9
Lee and Davenport4 examined the impact of case management interventions in reducing the number of ED visits by frequent users in Florida. They tracked and identified patients who attended more than three times a month. In 50 patients who received case management there was no significant reduction in ED visits after the intervention. However, they did focus on the subset of frequent users who had unresolved pain, were drug seeking or who had no primary care physician, which may be a population in which case management is less effective.4 Pope and Fernandes11 in Canada recruited 24 patients voluntarily to a case management programme. In the 12 months after the intervention ED attendances dropped from a median of 26.5 to 6.5, although the study numbers were small and patients did consent to the process, which may have improved engagement.11 Spillane et al8 in Rochester conducted a trial in which patients who attended the ED 10 times or more in one year were randomly assigned either to receive case management or standard emergency care only. They found no significant differences between the case management group and the control group in terms of numbers of attendances over the subsequent year.8
In Melbourne an assessment, liaison and early referral team has been established to case manage patients with complex needs.10 They identified 150 patients who presented to the ED six or more times per year. Patients who received case management from other services, for example psychiatry, were excluded. Sixty patients received case management, yet total group attendances to the ED actually increased after the intervention (610 vs 777). However, primary care linkage and community care engagement increased in the group, leading the authors to suggest that this trend towards increased ED use may be a positive aspect in these patients. It may be that the results of the study are affected by the selected population (less than half of their frequent attenders) and it may be that certain groups of frequent attenders, such as people with mental health problems, may benefit most from case management. In our study 37% of patients had mental health problems.
Although our data show an encouraging trend towards reduced numbers of ED presentations over the 6 months following case management, it is difficult to determine cause and effect. The reduction may be due to the natural ebb and flow in the presentations of these patients. Small patient numbers, not involving patients in developing their own care plans and a retrospective–prospective design limit the study. Bias may have been introduced by failing to assign patients randomly to control and case management groups. However, the results do suggest that there may be a benefit in approaching the management of frequent attenders in a more holistic, patient-centred way. A follow-up study is required to assess whether improvements are sustainable and maintained over time.
In conclusion, this pilot study suggests that case management of patients who frequently attend the ED may be beneficial in reducing the number of subsequent attendances in these patients. ED play a central role in the medical and psychosocial care of these patients and this care should fall under the remit of a multidisciplinary front door team with input from mental health and social work professionals.
Acknowledgments
The authors would like to thank the Lothian Unscheduled Care Team for their support with this study.
REFERENCES
Footnotes
Competing interests: None.
Linked Articles
- Primary survey