Article Text

Abstract
Objective Developments in advanced polypectomy technique provide an alternative to surgery in the management of large and complex colorectal polyps. These endoscopic techniques require expertise and can potentially incur high complication rates. This survey evaluates current UK practice, attitudes and training in advanced polypectomy.
Design Anonymous online questionnaire.
Setting Colonoscopists within the UK were asked about their approach to large polyps (>2 cm).
Results Among the 268 respondents (64% of whom were BCSP accredited), 86% were confident in removing lesions >2 cm by endoscopic mucosal resection (EMR). Of these, 27% were classed as low volume operators (<10 lesions resected/annum) and 14% as high volume operators (>50/annum). By comparison, only 3% currently performed endoscopic submucosal dissection (ESD). Referring one or more benign polyps for surgery a year was common among responders of all levels (11–68%). Training deficiencies were common: only 21% of responders had received a period of training dedicated to advanced polypectomy; 58% of responders would welcome a national training scheme and a majority supported the implementation of advanced polypectomy accreditation with national guidelines. However, while 41% wanted nominated regional EMR experts, only 18% would welcome an integrated national referral network for large/complex polyps.
Conclusions EMR is practised widely while ESD service provision is very limited. Most experienced colonoscopists are confident to perform piecemeal EMR, even if their training is suboptimal and annual numbers low. Practices and attitudes were variable, even among self-defined level 4 operators. Improving training and implementation of accreditation were welcomed, but there was little appetite for mandated referral to subspecialist ‘experts' and national networks.
- ENDOSCOPIC POLYPECTOMY
- COLORECTAL ADENOMAS
- COLORECTAL CANCER SCREENING
- MEDICAL DECISION ANALYSIS
- HEALTH SERVICE RESEARCH
Statistics from Altmetric.com
- ENDOSCOPIC POLYPECTOMY
- COLORECTAL ADENOMAS
- COLORECTAL CANCER SCREENING
- MEDICAL DECISION ANALYSIS
- HEALTH SERVICE RESEARCH
Introduction
Polypectomy reduces the incidence of colorectal cancer.1–4 While the majority of polyps are small (<1 cm), between 0.8% and 5.2% are referred to as large (>2 cm) and removal of these lesions requires advanced endoscopic techniques to ensure complete and safe excision.3 ,5 Endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD) are two such techniques that can effectively remove large benign lesions and some selected early polyp cancers. In selected cases, these techniques should be offered as an alternative to surgery6 ,7 as they are safer, less invasive, more cost effective and can usually be performed as an outpatient procedure.7–10 However, both EMR and ESD techniques are associated with significant complications including bleeding and perforation (more prevalent with ESD). Incomplete resection of lesions is increasing recognised, especially if undertaken by inexperienced operators.11 ,12 Some evidence shows that outcomes improve after the first 50 procedures.13 If the initial resection is inadequately performed, formation of fibrosis at the site makes subsequent resection of residual or recurrent tissue more difficult.10 ,14 ,15
The introduction of the Bowel Cancer Screening Programme (BCSP) has resulted in an increase in the detection and removal of large polyps:16 in the BCSP in England, from September 2006 to September 2011, 1337 out of 65 535 (2.0%) polyps were ≥2 cm.17 ,18 In England it is estimated that every year the BCSP identifies 31 additional polyps ≥2 cm per million of the population screened.1 This burden is likely to increase with age extension of the screening programme to 75 years, the roll out of flexible sigmoidoscopy screening at 55 years and surveillance of patients already found to have large polyps.3 ,5 Within the BCSP there is marked variation between regions in the rate of surgery for benign polyps.8 This suggests that variability exists in relation to patient access to advanced polypectomy, polypectomy practice and attitudes towards these techniques.
In view of the increasing demand and to assess potential variability in advanced polypectomy service provision, we conducted a national survey. The survey was primarily targeted at the BCSP colonoscopists who are largely responsible for the resection of large and more complex colonic lesions. There is currently no formally recognised training programme in either EMR or ESD in the UK. Despite this, the survey aimed to assess the background level of training any colonoscopists may have received.
The aims were to 1) evaluate current practice and expertise in advanced polypectomy, 2) to determine the state of training in advanced polypectomy and identify training needs, 3) and to evaluate individual attitudes towards improving advanced polypectomy practice within the UK.
Methods
This survey was conducted between 30 August and 21 October 2012. An online web-based survey was constructed using Select Survey.NET software (Kansas, USA),19 which was hosted on a secure university server (University of Liverpool, UK).
Both the British Society of Gastroenterology (BSG) and the NHS BCSP in England approved the questionnaire. BCSP colonoscopists and BSG members were invited by email to complete the anonymous online questionnaire through a hyperlink which gave responders access to the web-based application. The questionnaire was sent on two separate occasions to increase the response rate: the first at the beginning of the study period and the second 2 weeks before closure. All responses were anonymous and the questionnaire was designed to take only 10–15 min to complete. Inclusion criteria required responders to be independent colonoscopists and currently practising in the UK.
Pilot study
Prior to national roll out, a pilot questionnaire was distributed to BCSP colonoscopists in the north-west of England between 7 and 21 May 2012 to complete and provide feedback. It enabled the investigators to test the software for data analysis and comprehension of the questionnaire. On the basis of feedback, the questionnaire was further refined.
Questionnaire structure
There were 36 questions in the questionnaire, divided into five sections:
-
Responder demographics
-
Current colonoscopy practice and experience
-
Polypectomy and EMR experience
-
Referral practices for difficult polyps
-
Responder's opinion on training in EMR/advanced polypectomy.
The questionnaire responses varied between quantified numerical values, value ranges, best option selection and yes/no answers.
Definitions
-
Advanced polypectomy: endoscopic removal of polyps of ≥2 cm.
-
EMR: piecemeal endoscopic resection of sessile or lateral-spreading lesions with a maximum diameter >2 cm.
-
Level 1: competent to remove small lesions <1 cm with hot and cold techniques.
-
Level 2: competent to remove lesions up to 3 cm with good access.
-
Level 3: able to tackle larger lesions (by EMR) or smaller lesions with difficult access.
-
Level 4: able to remove very large flat or polypoid lesions that might also be considered suitable for surgery.20
Data analysis
Only fully completed questionnaires by independent colonoscopists were analysed. Incomplete questionnaires, duplicate responses, submission from practitioners that did not perform colonoscopy and non-independent practitioners were excluded from the analysis. Statistical analysis was performed using SPSS V.20.0 software (SPSS, Chicago, Illinois, USA). Descriptive statistical tests were used to present the results.
Results
Three hundred and thirty-eight questionnaire submissions were received with 268 fully completed and valid responses. Of the 70 excluded responses; 52 submissions were incomplete, 2 were from non-UK based responders and 16 were not independent practitioners.
Respondent demographics
All regions in the UK were well represented in the sample (figure 1). The majority of responders were gastroenterologists (75%), 10% were surgeons and 9% nurse endoscopists. Over 55% were aged between 41 and 50 years (table 1).
Characteristics of responders to the survey

Number of responders in each deanery or country in the UK.
Median lifetime colonoscopy experience was 3000 (IQR 1300–5000) procedures, with a median of 10 colonoscopies a week; 40% of responders performed at least one session in a teaching hospital and 64% were BCSP accredited.
Training in advanced polypectomy
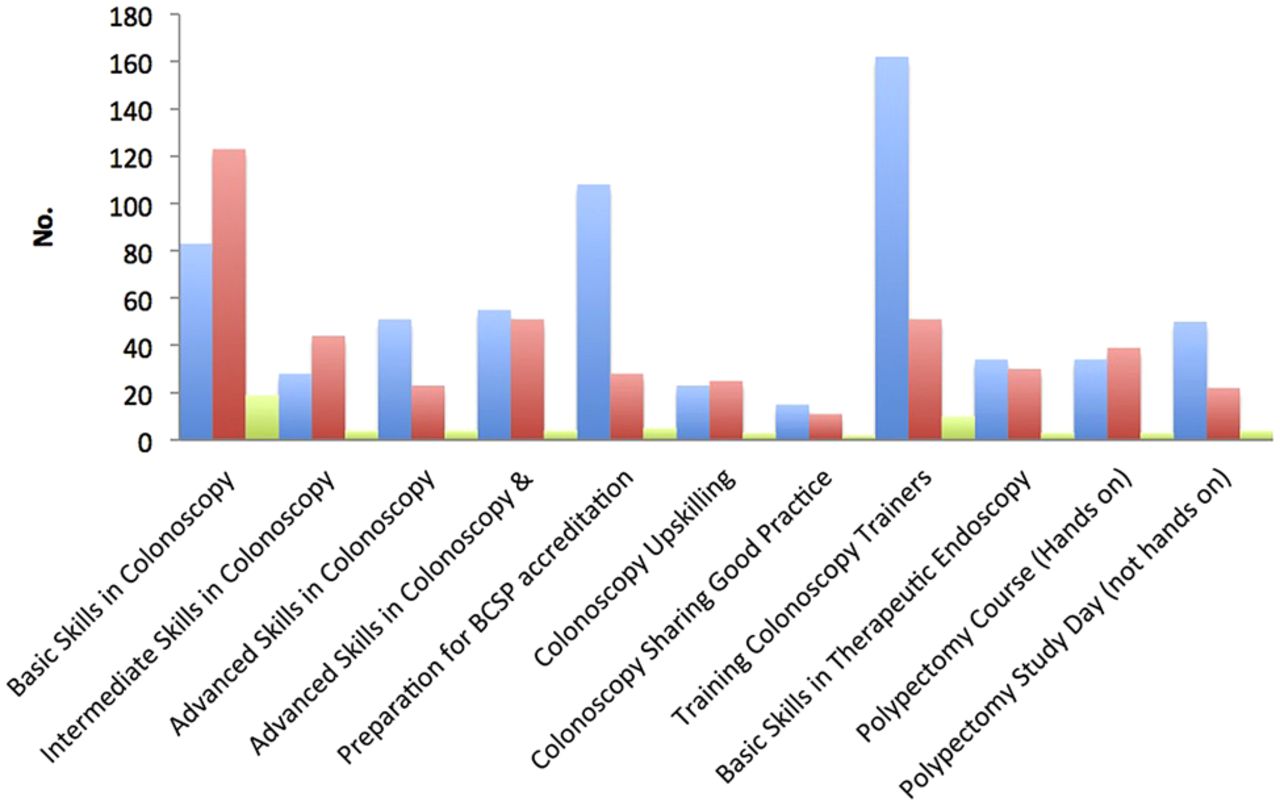
All responders had attended at least one endoscopy training course, either as a delegate or member of the teaching faculty. Over 50% of respondents were faculty for current JAG accredited endoscopy courses (figure 2). The commonest EMR training was direct teaching from an experienced colleague (21.7%), closely followed by those who had attended a workshop (19.6%). Overall, a quarter of respondents (56/268) had undertaken training in a unit that practised advanced polypectomy/EMR. Only 2.6% had undertaken an EMR fellowship for 6 months or longer. Fifty-eight percent of responders regarded themselves as predominantly self-taught while 16% were entirely self-taught (no formal EMR training on courses or by mentorship) (table 2).
Subjective ranking of the quality of training received
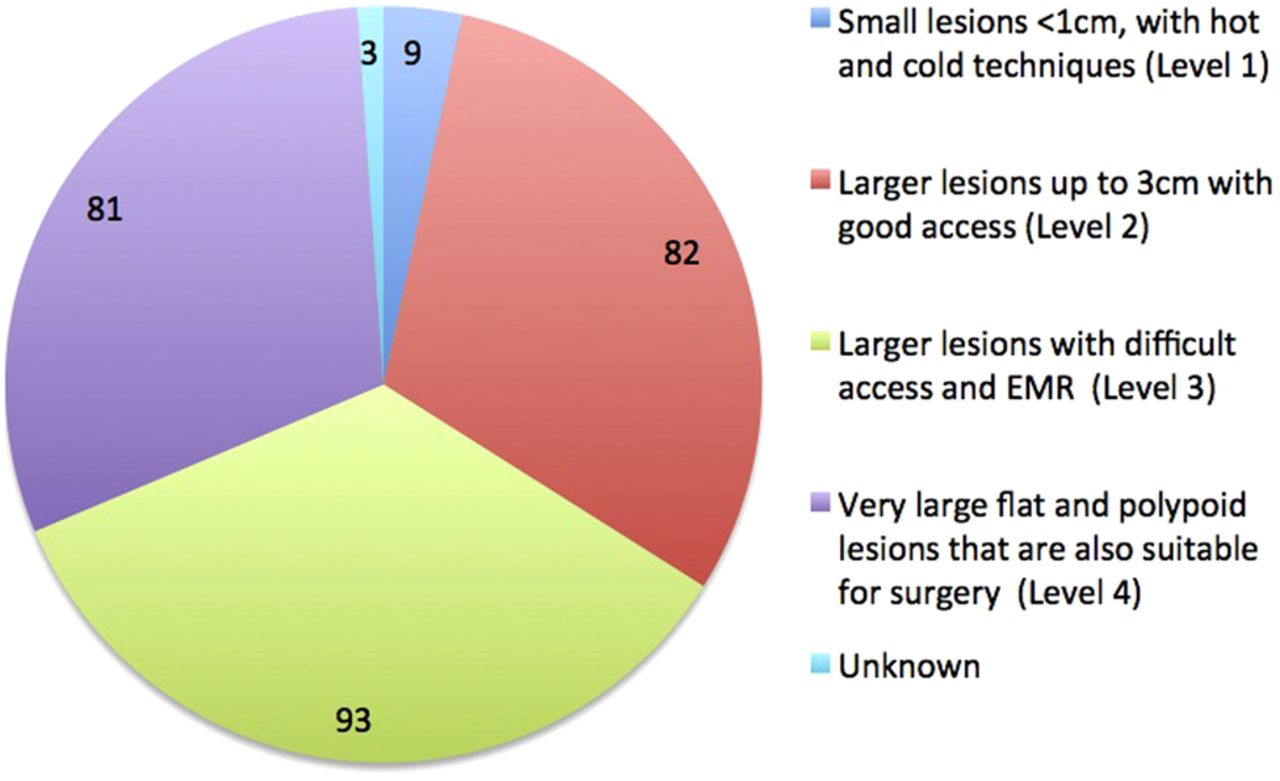
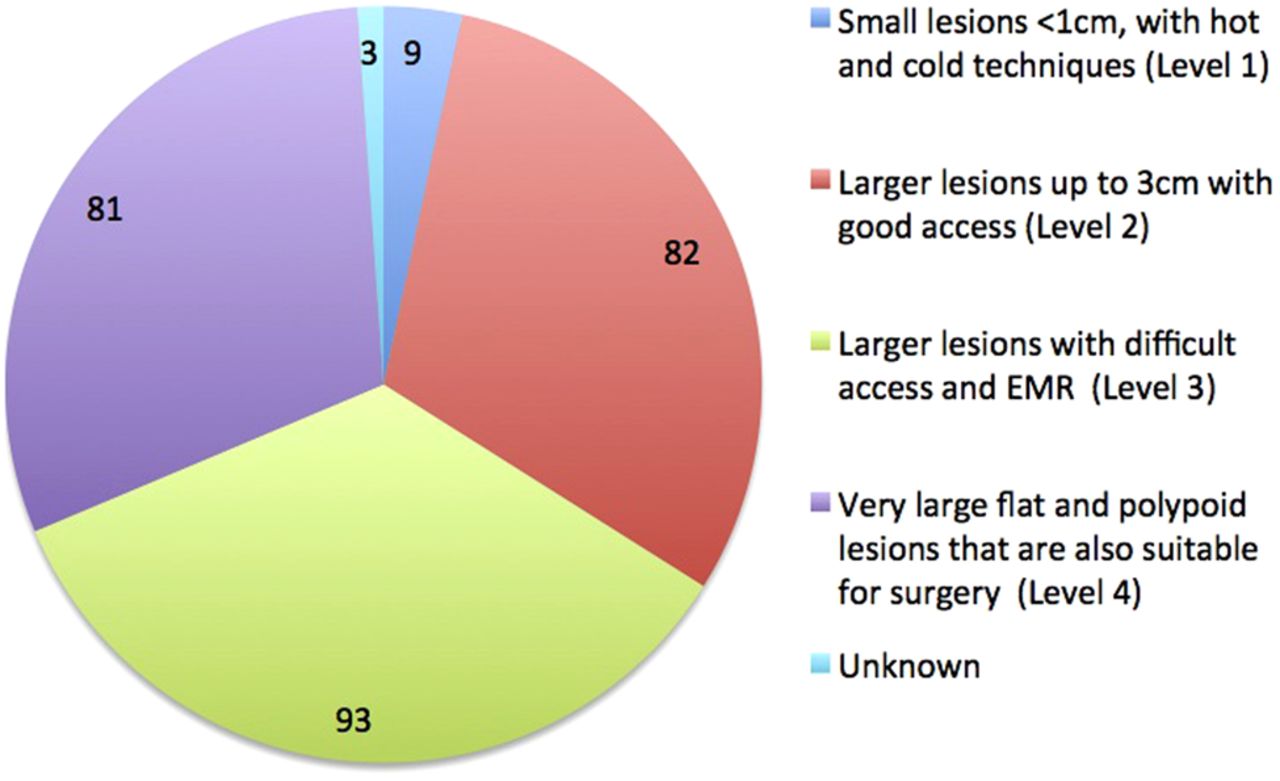
A clear majority (95.5%) of responders perform polypectomy on lesions up to 3 cm with good access; 30% described themselves as highly competent and able to remove very large flat and polypoid lesions that are also suitable for surgery.
Endoscopic submucosal dissection in the UK
ESD in the UK was very limited, with only seven (3%) of the responders performing full colorectal ESD, although 13 individuals (5%) use it as part of a hybrid technique. London and the South-East currently have the most ESD operators with three, followed by two each in Yorkshire and Humber and the North-West. All but one indicated that they would accept referrals from other units for ESD.
Current EMR practice and competency in the UK
Figure 3 describes the level of polyp complexity responders would tackle (level 1–4 competency scale).6 Only 3.4% self-classified as level 1, 30% level 2, 35% level 3 and 30% level 4. Eighty-six percent felt competent to remove sessile polyps >2 cm using EMR and 20.9% had removed polyps >6 cm in diameter. Half of the responders had performed EMR for more than 5 years. However, only 63% had performed more than 10 EMR procedures in the previous year, while 12% performed over 50 (table 1).

{kind=link}
{kind=link}
{kind=link}
Courses attended by responders either as a delegate, member of the teaching faulty or as an observer. All responders had been on at least one course as an observer or delegate.
Deficiencies and factors limiting practice in the UK
Responders were asked about their practice for managing polyps beyond their competence, but still potentially amenable to endoscopic removal: 32% declared they would routinely biopsy the polyp while 3.5% would snare a large piece for histology. Video recording was used by 20% in the assessment of large polyps.
A quarter of all the responders regarded themselves as operating close to the limit of what they deemed technically possible for EMR (level 4). Despite this, some colonoscopists would not remove a potentially resectable polyp due to a lack of confidence in assessing surface morphology (7%); uncertainty about the correct technique (2.5%); and lack of confidence managing immediate complications (2.5%). Further factors that limited advanced polypectomy practice included a lack of formal training in EMR (18.3%) and the opportunity to gain experience (17.9%) or a lack of guidelines in the management of large polyps (7.5%). All the individual reasons for limitations on practice are described in table 3 and then grouped under the major themes in table 4: governance issues (eg, responders that refer to an experienced colleague), training needs, lack of resources and finally responders without constraints (which are either fully competent or believe any case beyond their capability are better managed surgically). Overall, 31% of responders identified training needs and 21% identified a lack of resources as constraints on practice. The majority (59%) indicated they would welcome a national training scheme for complex polypectomy.
Factors limiting responders’ advanced polypectomy practice
Merger of similar statements from table 3 into common themes to explain why advanced polypectomy was currently limited
The commonest reasons for responders to constrain their EMR practice were doubts about achieving a complete resection (54%), a lack of time (35%) or concerns regarding complications (33%) (table 5).
Commonest reasons for responders to constrain their EMR practice
Advanced EMR practitioners in the UK
There was at least one level 4 operator in every deanery. Of the 81 self-rated level 4 operators, 17% had never removed a polyp >5 cm and 32% had performed fewer than 20 EMRs in the past year. Only 56% of level 4 operators agreed that they would attempt any polyp if EMR was technically feasible. Others felt constrained by their own technical ability or by time and resource limitations.
Referral practices
For polyps beyond a responder's perceived competence, most preferred referral to either an endoscopy colleague in their unit (34%) or outside (37%). However, 12% opted for immediate surgical assessment. Among all responders, 57% had referred at least one patient to surgery in the last year.
Over the last year, colonoscopists with least experience (levels 1 and 2) commonly referred at least one EMR case to another colleague (56% and 77%) but less often for surgical resection (11% and 52%). Conversely, the most experienced colonoscopists (level 4) referred less commonly to endoscopy colleagues (26%) and more often to surgery (68%) (table 6).
Referrals
Support for changes to the national delivery of advanced polypectomy
There was support for the implementation of national guidance (63%), formalised accreditation (59%) and a national training scheme (59%) on the technical aspects of advanced polypectomy/EMR. However, support for mandatory regional referral (19%) and an integrated national referral network for complex polypectomy (18%) was low. A significant minority supported a national database for EMR (35%) and ESD (31%). Most responders (77%) would be willing to supply data to a national audit if requested. In addition, most responders would be willing to submit data following serious complications (82%) and referral of benign polyps for surgery (79%). Overall, support for the submission of outcome data ranged between 77% and 82%.
Complications
Among those performing EMR, 23 (10%) admitted to a perforation in the previous year and 23% reported significant bleeding requiring a blood transfusion. Among the 23 responders with at least one perforation, 11 were level 4 colonoscopists and 15 were experienced practitioners having performed EMR for >5 years. Most responders who reported perforations were removing large lesions; nine had removed a lesion >6 cm and seven had removed lesions >4 cm. Surprisingly, of the 32 operators performing over 50 EMRs a year, only 12 (37.5%) reported a significant bleed in the preceding year.
Discussion
This is the first national study reviewing advanced polypectomy practice in the UK. There is a good distribution of self-rated expertise across the country but national coverage of ESD is very limited. This study demonstrates that practice is variable, with deficiencies in training and technique and unacceptable variation in referral to other endoscopists and for surgical resection.
The sample size of 268 practitioners provides a perspective of all UK practice and a broad range of experience. In 2011 the national colonoscopy audit identified 2681 colonoscopists in the in the UK, indicating the study captured at least 10% of consultant or nurse colonoscopists and specifically targeted the BCSP colonoscopists who provide the vast majority of the complex polypectomy service.15 Overall, 65% of responders were BCSP colonoscopists. The data highlight the fact that most of the workforce (75%) in this survey practising advanced polypectomy are gastroenterologists (surgeons 10% and nurse endoscopists 9%). The low response from surgeons could be explained by the relatively small proportion of surgically trained BCSP colonoscopists and the fact that the survey did not target specific surgical societies. The majority (54.9%) of individuals self-assessing as highly skilled colonoscopists are aged 41–50 years, suggesting there is unlikely to be a short fall of individuals with this expertise in the immediate future.
Most experienced colonoscopists appeared willing to attempt piecemeal EMR, even if their annual numbers are low. A surprising number of colonoscopists self-assessed themselves as level 4 experts, despite not providing data to support this level of practice. This suggests they may not fully understand the definition of level 4 polypectomy. It is clear the definition of level 4 polypectomy needs to be clearer and better understood. To acquire and maintain the expertise of level 4 polypectomy, a colonoscopist will almost certainly require a tertiary referral practice because the frequency of level 4 lesions in a single institution is unlikely to be sufficient. Inappropriate self-categorisation at level 4 is a major problem because it can adversely affect patients for three possible reasons: (1) the endoscopist may start a resection he cannot complete; (2) if resection is not attempted, the patient is less likely to be referred to a colonoscopist with the appropriate expertise; (3) as a result of this, the patient is more likely to be inappropriately referred for surgery.
With regard to the low number of ESD practitioners in the country, we need to remember that at present colorectal ESD is classed by the National Institute for Health and Care Excellence as an experimental procedure and to be undertaken with certain caveats. Definition of cases deemed appropriate and suitable for ESD in the UK remains to be determined. It is highly probable that there will be a significant difference in approach between Western and Eastern ESD practice. While there are a number of endoscopists practising the procedure, the technique is demanding, time consuming and the ideal training for the procedure is unknown. Finally, its role in relation to EMR is still not determined.21 Until some of these issues have been clarified, it is difficult to determine how many individuals would be required to provide a UK network for ESD referral. There is no doubt that ESD practice will be limited and possibly restricted by governance, similar to that seen in surgical service provision for gastrointestinal oncology patients.
This survey highlighted some issues regarding best practice, such as the disappointingly limited use of video documentation. Unhelpful actions such as routine polyp biopsy or, even worse, partial polypectomy were a relatively common practice feature. Improved training and referral pathways should enable better assessment of polyps and, subsequently, better decision-making. The low reporting of complications, even among high volume operators, may reflect high quality polypectomy but it also suggests a lack of robust processes for capturing and reviewing adverse events. In particular, significant bleeding seemed to be reported less than expected when compared with rates of 4–7% seen in large series.22 ,23
The survey revealed a deficiency in formal training, with less than half of the respondents having formal training in advanced polypectomy. More worryingly, there is evidence from this survey and other studies of deficiencies in practice (particularly referral to surgery for benign disease), which could be reduced by clear guidance and more formal training. Complete endoscopic removal of polyps >2 cm can be achieved in >95% cases, with low rates of complications and savings of up to £11 000 per patient.24 Therefore, the aim should be to minimise variation in practice, particularly to reduce surgical referrals of patients with benign endoscopically resectable lesions.
Within the UK BCSP, where standards should be among the highest, there is considerable variation in surgical referral rates (0–20% for benign polyps >2 cm within one BCSP region).8 One study found almost a quarter of 557 polyps ≥2 cm were referred directly for surgery.25 In this survey, reported constraints to performing advanced polypectomy included lack of training, a lack of resources and uncertainty about guidelines and referral pathways for further endoscopic assessment. All of these are amenable to clear guidance, training courses, a network of level 4 polypectomy expertise and more formalised referral pathways.
The referral of a complex polyp is established and successful within some units.13 Less is known about referral patterns around the country and between individual units. Our survey found that many colonoscopists appear willing to refer cases to a colleague for EMR, even if it involves transfer to another hospital. This indicates that informal networks of sub-specialists (experts) already exists, but the variation in referral to surgery suggests that this informal network is not working effectively within the overall service provision. Can a case be made for a more formal network of level 4 polypectomy referral? In this survey there was little appetite for mandated referral networks, and suggested national EMR databases also did not receive universal support. However, most responders said they would be willing to supply their own data for audit. We can only speculate as to the reasons for the lack of support, which may include concerns about losing consultant autonomy and the top-down implementation of more rules and guidelines for practice. However, other referral networks and multidisciplinary teams (MDTs) are generally very well regarded and supported. One study of over 2000 NHS healthcare professionals showed that over 90% agreed that MDT care improved clinical decision-making and allowed better coordinated care, which was more evidence-based and improved overall quality of treatment.26
To reduce variation in the management of complex polyps, we believe that all benign polyps considered for surgery should first be discussed at a regional MDT and that this should be a quality standard. To enable this to occur, there should be organised provision (similar to centralised stroke and cancer services) of regional MDTs/local networks. Such a formalised network would enable decisions to be made which are not constrained by the availability of expertise. There would be other positive benefits: regular contact with MDTs would foster better decision-making and lead to more uniform practice. While there appears to be resistance to such an approach, we believe colonoscopists would be quick to see its advantages if it was properly implemented and audited.
It is estimated there would need to be approximately 20 complex polypectomy units across the country, each serving a base population of 3 million. We propose that certain criteria (box 1) would need to be met before a centre could be designated as a referral centre and would anticipate that reimbursement would better reflect the resource needed to provide such a service.
Proposed quality indicators for complex polypectomy centers
-
Individual key performance indicators
-
Colonoscopy of tertiary referred lesions within 6 weeks of referral.
-
Video documentation of the lesion (photo documentation as minimum)
-
Video documentation post-resection (photo documentation as minimum)
-
Complete excision with no recurrence at 12 months from the index procedure
-
Record of complications at 30 days
-
Follow-up consultation (telephone consultation as a minimum)
-
-
Demonstration of ability to provided endoscopy list time for the additional workload with dedicated lists (guide: each complex lesion may take half a list or more)
-
Staff to include at least two endoscopists that can cover each other and endoscopy nurses with training in complex polypectomy
-
Equipment (including the necessary snares and haemostasis devices)
-
Surgeons (for discussion at the MDT and in case of operative treatment of perforations or bleeding)
-
Robust referral system including administrative staff support and the IT tools for a virtual MDT.
In conclusion, this study has helped to define the current state of advanced polypectomy practice in the UK. It has identified perceived limitations and constraints in referral practice and highlighted uncertainties in therapeutic competence and a lack of clear national guidelines. The study also indicates that there are sufficient experienced colonoscopists to provide a national referral network, which would reduce surgical intervention for benign disease. The introduction of such a top-down solution was not popular among the surveyed cohort. However, we believe a ‘hub and spoke’ approach that encourages referral of complex polyps to local MDTs will benefit patients by reducing constraints on decision-making and, through this, reduce the variability in patient care, and particularly inappropriate surgery for benign polyps.
SIGNIFICANCE OF THIS STUDY
-
What is already known on this subject?
-
The removal of large or complex colorectal polyps can be challenging, but if benign, they can almost always be safely resected endoscopically. Inadequate resection technique can lead to adenoma recurrence and complications.
-
What are the new findings?
-
This study demonstrates that practice in removal of complex colonic polyps is variable, with deficiencies in training and technique, and unacceptable variation in referral to other endoscopists, or for surgical resection. Many colonoscopists are performing complex polypectomy despite having low annual numbers of such cases.
-
How might it impact on clinical practice in the foreseeable future?
-
The deficiencies in training and evidence of suboptimal practice support the case for regional referral networks. Such networks, together with a requirement for all cases considered for surgery to be discussed in an MDT, would ensure that treatment decisions are not constrained by inadequate referral pathways and/or the necessary endoscopic expertise. Regional specialty centres would mean dedicated, advanced therapeutic colonoscopists had a sufficient case load of complex cases to develop and maintain expertise, and to train the next generation of advanced colonoscopists.
References
Footnotes
-
Contributors All authors contributed equally to the study conception and design. JG, POT and SS designed and ran the pilot study while JA and RV contributed to refinements in the final version. JG collected and analysed the data. All authors contributed to writing and drafting of the manuscript and all gave final approval for the version to be submitted.
-
Funding JG received an unconditional award from Cook Medical.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.