Article Text

Abstract
Introduction The early use of risk stratification scores is recommended for patients presenting with acute non-variceal upper gastrointestinal (GI) bleeds (ANVGIB). AIMS65 is a novel, recently derived scoring system, which has been proposed as an alternative to the more established Glasgow–Blatchford score (GBS).
Objective To validate the AIMS65 scoring system in a predominantly Caucasian population from Scotland and compare it with the GBS.
Design Retrospective study of patients presenting to a district general hospital in Scotland with a suspected diagnosis of ANVGIB who underwent inpatient upper GI endoscopy between March 2008 and March 2013.
Outcomes The primary outcome measure was 30-day mortality. Secondary outcome measures were requirement for endoscopic intervention, endoscopy refractory bleeding, blood transfusion, rebleeding and admission to high dependency unit (HDU) and intensive care unit (ICU). The area under the receiver operating characteristic (AUROC) curve was calculated for each score.
Results 328 patients were included. Of these 65.9% (n=216) were men and 34.1% (n=112) women. The mean age was 65.2 years and 30-day mortality 5.2%. AIMS65 was superior to the GBS in predicting mortality, with an AUROC of 0.87 versus 0.70 (p<0.05). The GBS was superior for blood transfusion (AUROC 0.84 vs 0.62, p<0.05) and admission to HDU (AUROC 0.73 vs 0.62, p<0.05). There were no significant differences between the scores with respect to requirement for endoscopic intervention, endoscopy refractory bleeding, rebleeding and admission to ICU.
Conclusions AIMS65 accurately predicted mortality in a Scottish population of patients with ANVGIB. Large prospective studies are now required to establish the exact role of AIMS65 in triaging patients with ANVGIB.
- GASTROINTESTINAL BLEEDING
- GASTROINTESINAL ENDOSCOPY
Statistics from Altmetric.com
Introduction
The early use of risk stratification scores is recommended by the International Consensus Upper Gastrointestinal (GI) Bleeding Group for patients presenting with acute non-variceal upper GI bleeds (ANVGIB).1 Such predictive models permit identification of patients who are suitable for early hospital discharge or even outpatient care. The most widely used is the Glasgow–Blatchford Score (GBS), which is based on the blood urea nitrogen, haemoglobin, systolic blood pressure (SBP), heart rate (HR) and the presence of melaena, syncope, hepatic disease and cardiac failure. The score ranges from 0 to 23 and the risk of requiring clinical intervention and death has been shown to increase with increasing score.2 More recently, a simpler scoring system known as AIMS65 was devised, which is based on serum albumin (<30 g/dL), international normalised ratio (INR) (>1.5), altered mental status (Glasgow Coma Scale (GCS) <14), SBP (<90) and age (>65).3 One point is scored for the presence of each variable and the derivation cohort showed it to accurately predict mortality, length of stay and cost in patients with ANVGIB, while the validation cohort showed it to be superior to the GBS in predicting mortality;3 ,4 however, its ability to predict the need for clinical intervention has yet to be established, as has its validity in non-US populations.
Therefore, the aim of this study was to examine the ability of the AIMS65 score in predicting mortality and the need for clinical intervention in comparison with the GBS and to validate it in a predominantly Caucasian population from Northern Europe.
Methods
Study design and setting
This was a retrospective study of patients who presented with a suspected primary diagnosis of ANVGIB and underwent upper GI endoscopy (UGIE) at Raigmore Hospital, Inverness, Scotland, between March 2008 and March 2013. Raigmore Hospital is the only acute district general hospital of the Highlands serving a population of 350 000 people and has a bed capacity of 452. It covers a large rural area (33 000 km2) and provides both high dependency and intensive care. Within the region, there are two district general hospitals, a rural island hospital and several community hospitals from which referrals are taken. The endoscopy unit is run by three consultant gastroenterologists, one nurse endoscopist and three consultant surgeons and operates Monday–Friday 9:00–17:30. During working hours, emergency inpatient endoscopies are performed on a ‘stop the list’ basis at the discretion of the consultant gastroenterologist. Outside of these hours, it operates on an emergency basis only. All out-of-hours endoscopies are performed by the on-call surgical team.
Participants
All potential subjects were identified by the department of medical records from discharge summaries only using the following International Classification of Diseases (ICD) 10 codes: K22.6, K25.0, K25.2, K25.4, K25.6, K26.0, K26.2, K26.4, K26.6, K27.0, K27.2, K27.4, K27.6, K28.0, K28.2, K28.4, K28.6, K29.0 K92.0, K92.1 and K92.2 (see online supplementary data for explanatory table of diagnoses used for identifying patients). Medical notes were then retrieved, reviewed and patients were included in the study if they were admitted via the emergency department or acute medicine with a suspected primary diagnosis of ANVGIB and underwent UGIE as an inpatient. ANVGIB was defined as suspected bleeding from the upper GI tract as manifest by haematemesis (including coffee-ground vomiting) and/or melaena. Reasons for exclusion included no UGIE performed as an inpatient, variceal bleed, ANVGIB as an inpatient and age <18 years.
Data collection
Following review of the medical notes, the following information was collected from all eligible cases: age, date of admission and discharge, mortality, requirement for high dependency unit (HDU) and/or intensive care unit (ICU) admission, comorbidities (ischaemic heart disease, cardiac failure, liver disease, chronic renal disease, malignancy), medications at time of admission, endoscopic diagnosis, time taken for UGIE to be performed, repeat bleed (defined as further haematemesis, passage of fresh melaena, continuing or recurrent hypotension and/or tachycardia ± fall in haemoglobin after the first endoscopy), admission HR, BP and respiratory rate, the presence of syncope and/or melaena in the history, assessment of mental status/GCS, admission haemoglobin, urea, clotting profile, requirement for blood transfusion, pretransfusion haemoglobin and the number of units transfused.
The collected data were recorded on a predesigned Excel spreadsheet and used to calculate the GBS score and AIMS65 score for each patient. The methods for calculating the GBS and AIMS65 score are shown in table 1 and have been previously well described.2 ,3 ,6 ,7
Breakdown of the AIMS65 and Glasgow–Blatchford scoring systems
Outcomes
The primary outcome measure was 30-day mortality. Secondary outcome measures were requirement for endoscopic intervention, requirement for intervention for endoscopy refractory bleeding, blood transfusion, rebleeding and admission to HDU and ICU.
Data analysis
All demographic data are expressed as the mean (with SD) and median where appropriate. The accuracy of the various scoring systems in identifying the need for intervention and outcomes was assessed by the receiver operating characteristic (ROC) curve and area under the ROC (AUROC). The distribution of the GBS and AIMS65 score according to mortality was plotted to provide definitive cut-off scores. All analyses were carried out using SPSS V.19.
Results
Patient characteristics
There were 924 patients with an ICD-10 code indicating a possible diagnosis of ANVGIB. Of these we identified 328 patients who met the inclusion criteria. Reasons for exclusion included ANVGIB as an inpatient, variceal bleed, lower GI bleed, paediatric patient, UGIE not performed as an inpatient but planned as an outpatient procedure, variceal bleed, gynaecological bleed and miscoded. A full breakdown of patient characteristics can be seen in table 2.
Patient characteristics
The endoscopic findings were of 44.8% (n=147) peptic ulcer disease, 9.8% (n=32) oesophagitis, 8.2% (n=27) gastritis/erosions, 2.1% (n=7) duodenitis/erosions, 4% (n=13) Malloy–Weiss tear, 2.1% (n=7) malignancy, 9.8% (n=32) other and 19.2% (n=63) had no abnormality found. 74.5% (n=244) patients who underwent UGIE required no endoscopic intervention, 21.6% (n=72) required endoscopic therapy in order to achieve haemostasis, 1.5% (n=5) failed to achieve endoscopic haemostasis and proceeded to surgery, 0.3% (n=1) failed to achieve endoscopic haemostasis and proceeded to radiological intervention and 1.8% (n=6) proceeded straight to surgery.
Performance of the GBS and AIMS65 score
30-day mortality
The overall 30-day mortality was 5.2%. For AIMS65 scores, mortality increased with increasing score, with scores of 0, 1, 2, 3, 4, and 5 for mortality rates of 0.8%, 1%, 6.8%, 30.4%, 100% and 100%, respectively. The AUROC for AIMS65 score predicting mortality was 0.87 and was superior to the GBS (AUROC 0.87 vs 0.70, p<0.05) (figure 1).
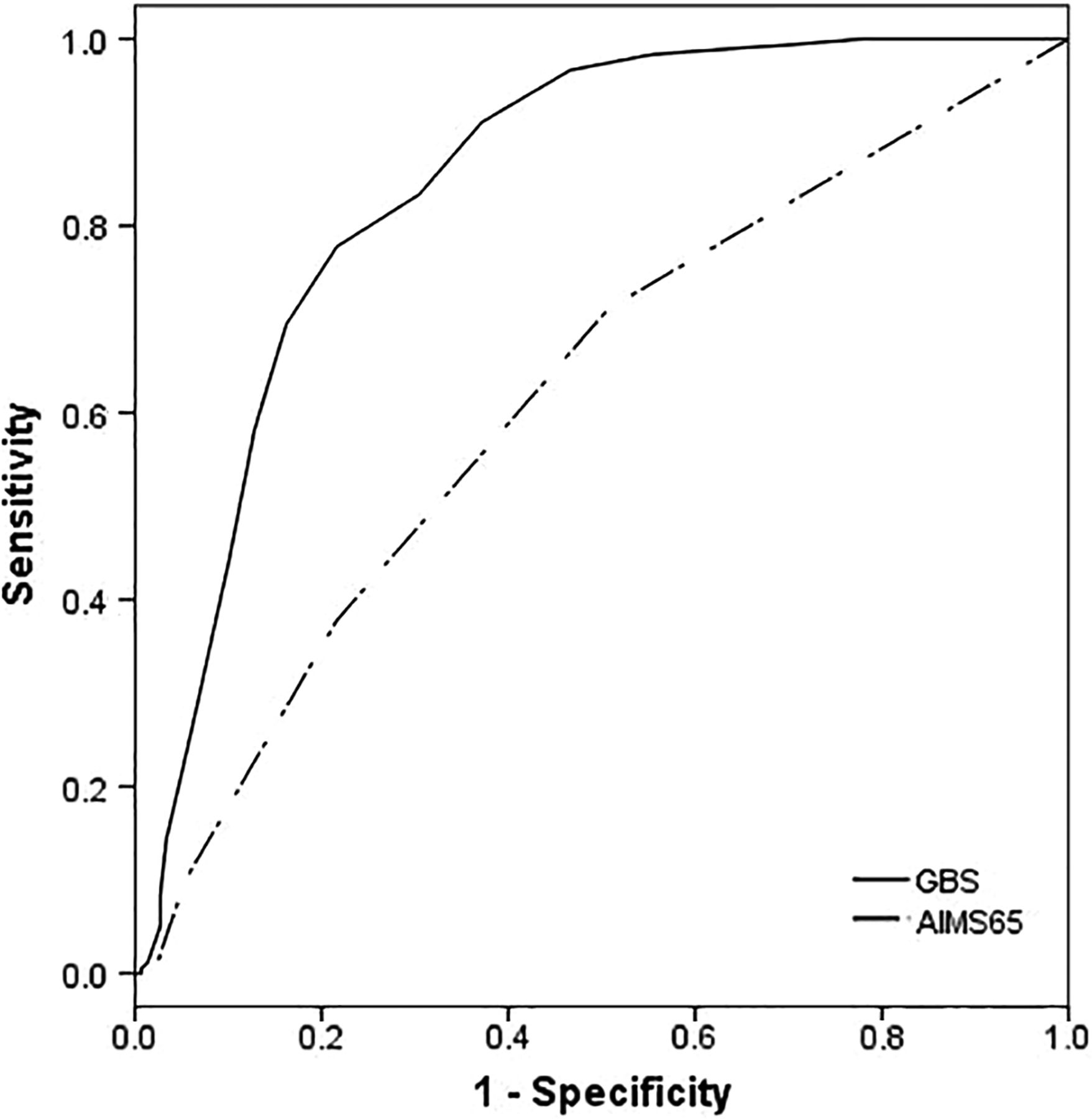
Receiver operating characteristic (ROC) curves for the AIMS65 score and Glasgow–Blatchford score (GBS) as predictors of 30-day mortality. AIMS65 score was superior to the GBS for predicting 30-day mortality from acute non-variceal upper gastrointestinal bleeding.
The cut-off point that maximised the sum of the sensitivity and the specificity was 1 for the AIMS65 score (sensitivity 0.94, specificity 0.60) and 3 for the GBS (sensitivity 1.0, specificity 0.82). Mortality for patients with AIMS65 scores of ≤1 (low risk) was 0.88% and for scores ≥2 (high risk) 15%. Mortality for patients with GBSs of ≤3 (low risk) was 0% and for scores ≥4 6.3%.
Endoscopic intervention
In total, 21.6% (n=72) of patients required an endoscopic intervention in order to achieve haemostasis. 72.2% (n=52) received injection of epinephrine, 20.8% (n=15) received injection of epinephrine and endoclip and 6.9% (n=5) received argon beam therapy. When comparing the AUROC of the AIMS65 score and GBS for endoscopic intervention, we found no significant differences, with AUROC of 0.55 and 0.60, respectively (for ROC curve, see online supplementary data).
Endoscopy refractory bleeding
In total, 3.7% (n=12) of patients required surgical (n=11) or radiological intervention (n=1) for endoscopy refractory bleeding. Mortality in those undergoing further intervention for endoscopy refractory bleeding was 16.7% (n=2). When comparing the AUROC of the AIMS65 score and GBS for those requiring intervention for endoscopy refractory bleeding, we found no significant differences, with AUROC of 0.75 and 0.76, respectively (for ROC curve, see online supplementary data).
Blood transfusion
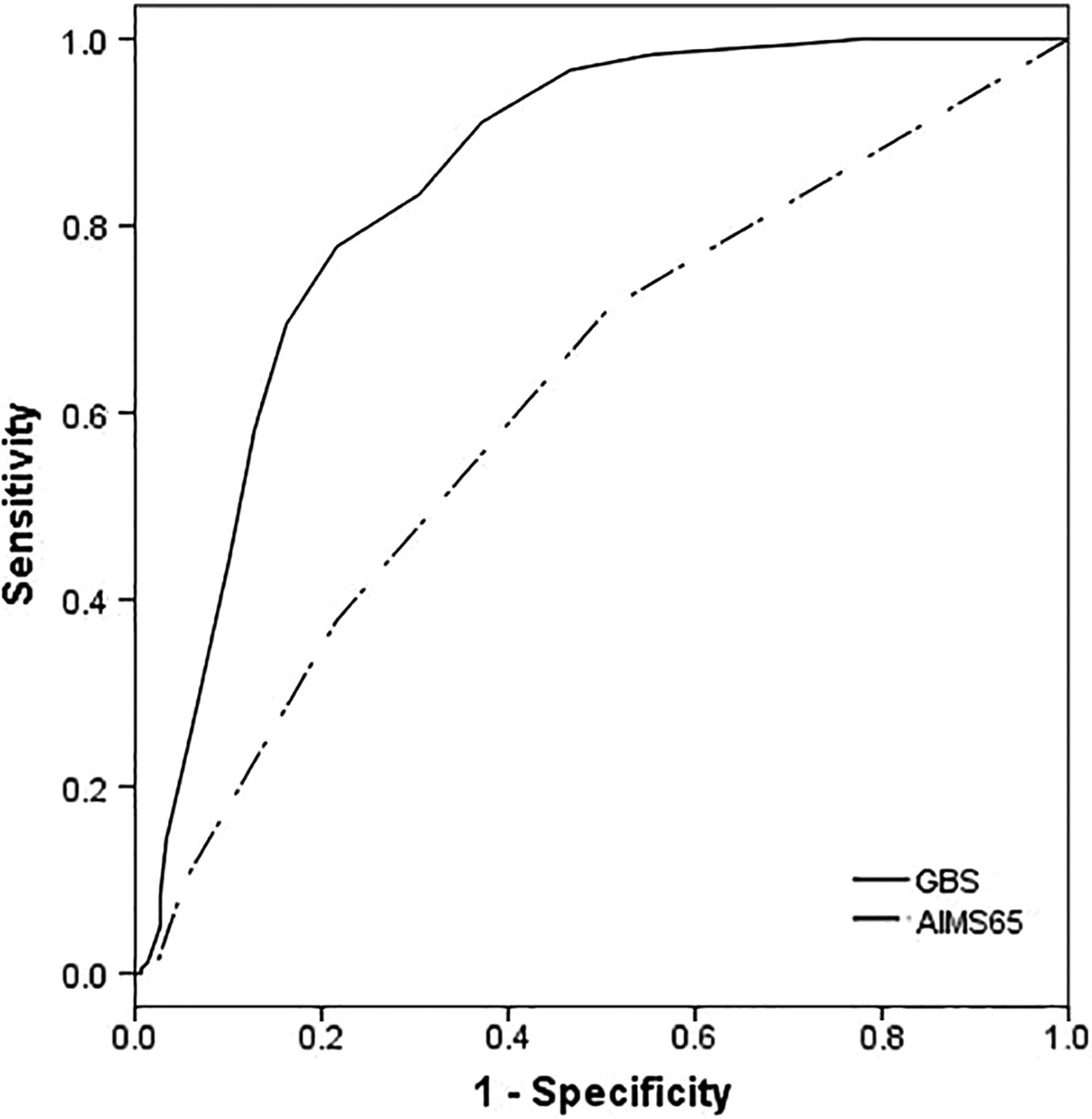
In total, 57.6% (n=189) of patients received a blood transfusion. Both the mean and the median pretransfusion haemoglobin was 7.6 g/dL (SD 1.7). The mean and median number of red blood cell (RBC) units transfused was 3.3 (SD 2.6) and 2.0, respectively. When comparing the AUROC of the AIMS65 score and GBS for need for blood transfusion, we found the GBS to be superior to the AIMS65 score, with AUROC of 0.84 and 0.62, respectively (p<0.05) (figure 2).

Receiver operating characteristic (ROC) curves for the AIMS65 score and Glasgow–Blatchford score (GBS) as predictors of requirement for blood transfusion. The GBS was superior to the AIMS65 score for predicting need for blood transfusion.
Admission to high dependency and ICUs
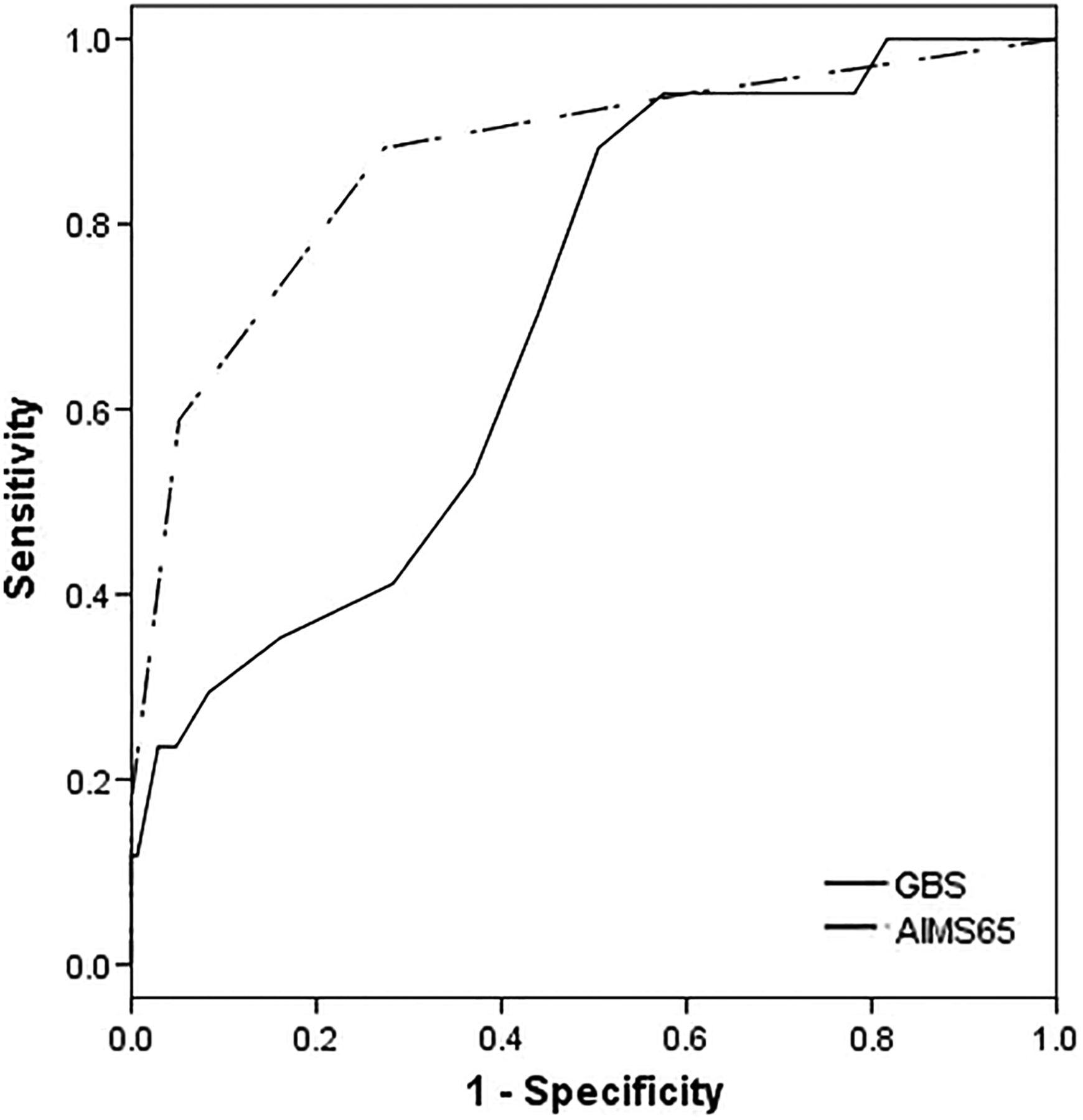
25.6% (n=84) of patients were admitted to the HDU. When comparing the AUROC of the AIMS65 score and GBS for HDU admission, we found the GBS to be significantly superior to the AIMS65 score (AUROC of 0.73 vs 0.62, p<0.05) (figure 3).

{kind=link}
{kind=link}
{kind=link}
Receiver operating characteristic (ROC) curves for the AIMS65 score and Glasgow–Blatchford score (GBS) as predictors of requirement for high dependency unit (HDU). The GBS was superior to the AIMS65 score for predicting HDU admission.
Four per cent (n=13) of patients were admitted to level 3 or ICU settings. When comparing the AUROC of the AIMS65 score and GBS for ICU admission, we found no significant difference, with an AUROC of 0.72 for both scores (for ROC curve, see online supplementary data).
Rebleeding
Clinical evidence of rebleeding occurred in 20.8% (n=15) of patients who required endoscopic intervention in order to control haemorrhage. When comparing the AUROC of the AIMS65 score and GBS for risk of rebleeding, we found no significant difference between the two scores (AUROC of 0.67 vs 0.65) (for ROC curve, see online supplementary data).
Discussion
We investigated the AIMS65 score as a predictor of 30-day mortality, need for clinical intervention and risk of rebleeding in comparison with the GBS in patients presenting with ANVGIB. We found the AIMS65 score to be superior to the GBS in terms of predicting 30-day mortality, whereas the GBS was superior in predicting the need for RBC transfusion and admission to HDU. We found no significant differences between the two scores with respect to requirement for endoscopic intervention, endoscopy refractory bleeding, admission to ICU and risk of rebleeding. This is the first validation in a predominantly Caucasian population from Northern Europe, and our results compare favourably with both derivation and validation cohorts, as well as an Australian population, published as a conference abstract.3–5
Studies looking at AIMS65 in four independent populations have delivered conflicting results. In a retrospective South Korean study, 149 patients who presented to the emergency department with peptic ulcer bleeding were analysed.8 They found the AIMS65 score to be a poor predictor of clinical outcome. However, they failed to compare the AIMS65 score with a previously validated scoring system such as the GBS. A similar retrospective study in Japan looked at 192 patients who presented with GI bleeding and found high AIMS65 scores to be a good predictor of prognosis in comparison with the GBS.9 Like the aforementioned South Korean study, this was a relatively small study that furthermore included patients presenting with lower GI bleeding, a condition for which neither the GBS nor AIMS65 score is validated. A retrospective Australian study analysed 424 patients presenting with both ANVGIB and variceal bleeding.5 They found AIMS65 to be superior to the GBS in predicting inpatient mortality, while the GBS was superior in terms of predicting need for RBC transfusion. However, they also found AIMS65 to be superior to the GBS in predicting need for ICU admission. Finally, a prospective Turkish study looked at 211 patients who underwent UGIE and found AIMS65 and the GBS to be comparable in predicting 30-day mortality, rebleeding and requirement for endoscopic intervention.10
The finding that the AIMS65 score is a better predictor of mortality than the GBS is not all that surprising given that AIMS65 was developed with the aim of predicting mortality, while the GBS was developed with the intention of predicting need for clinical intervention. Despite this, the exact role of AIMS65 in triaging patients in the emergency department remains to be established. Although a good predictor of mortality, it is of little use in helping practitioners decide if patients can be managed safely on an outpatient basis. In our study, patients with AIMS65 scores of 1 or below (69.5% (n=228) of the study population), which we defined as low risk, suffered mortality, required endoscopic intervention and blood transfusion. On the other hand, patients with a GBS ≤3 suffered no mortality, did not require endoscopic intervention and received no RBC transfusion, potentially allowing 17.4% (n=57) of patients to be managed safely on an outpatient basis. This observation is in keeping with the previously mentioned prospective Turkish study, which also found low-risk AIMS65 scores to require blood transfusion, endoscopic intervention and suffer rebleeding.10 A GBS ≤3 has recently been shown to be an appropriate cut-off in hospitalised patients who develop acute upper GI bleeding.11 Given that most of the costs associated with ANVGIB are associated with hospital admission, scoring systems which safely lead to a better and more appropriate use of resources are more likely to be preferred.1 ,12 However, given that larger prospective studies have found that patients with a GBS of 2–3 are at risk of adverse outcome such observations require further study with properly defined patient pathways before one could consider extending the clinical utility of the GBS.7
AIMS65 strong association with mortality is worthy of further consideration. While increasing age is an obvious risk factor for death, as is presentation with shock, the other components of the AIMS65 score have not been included in other risk assessment scores for upper GI bleeding. Decreasing serum albumin concentrations and INR >1.5 have both been shown to be independent predictors of mortality and may act as a proxy of comorbid cardiovascular and hepatic disease.13 Impaired level of consciousness is also a strong predictor of mortality and is included in other risk assessment tools for other conditions.14 This is interesting as only six of our patients had their deaths directly attributed to their GI bleed. Where the information was available, the rest were felt to be as a direct result of ischaemic heart disease and cardiac failure, with GI bleed as a contributory factor, which is in keeping with large prospective studies which have reported 80% of deaths in peptic ulcer bleeding are as a result of non-ulcer bleeding causes.15 Whether those patients with high-risk AIMS65 scores would benefit from early intervention is beyond the scope of our work but is a possible area for future prospective studies.
This study has several limitations. It is retrospective in nature and derived from one small centre. It is unlikely that our cohort represents a near consecutive sample of patients and that a significant number of low-risk patients have been missed. Hospital guidance on the discharge of low-risk patients changed during the study period with a preendoscopy Rockall score of zero used as per the Scottish Intercollegiate Guidelines Network (SIGN) guidelines prior to these being superseded by the 2012 National Institute for Health and Care Excellence (NICE) guidelines, which recommended using a GBS of zero.16 ,17 There is also the use of clinician judgement in those patients with low-risk scores, with its common practice to employ a 24 h period of observation before seeking GI consultation (in patient UGIE vs outpatient UGIE). Unfortunately, we didn't keep records of those patients who ultimately didn't undergo UGIE as an inpatient, nor do we have records of those patients with a GBS of zero who were discharged directly from the emergency department. Furthermore, some low-risk patients who were just coded ICD K21/K29 without supplementary use of K92 would have been missed by our search strategy, resulting in an underestimation of those with erosive disease. We acknowledge that these features lead to potential problems with selection bias which may affect the internal validity of our study and as such, our results should be interpreted with this in mind. A small number of patients didn't have clotting profiles performed on admission and, where this occurred, was taken from a coagulation profile performed later in the admission. An assessment of mental status and/or GCS wasn't always documented by the admitting doctor and, where this occurred, was taken from the patient's nursing admission document. Our cohort is relatively small, which meant that the frequency of some events occurred at a level that one might question the validity of our findings. This is particularly true with respect to ICU admission and the low frequency with which this occurred is likely to reflect cultural differences in defining critical illness. Given that we considered this an exploratory study, we have not corrected for multiple comparisons and cannot exclude the possibility that the significant findings have arisen by chance. Although AIMS65 was originally developed from a database which included both variceal and non-variceal upper GI bleeds, we have looked at non-variceal bleeds only, meaning our findings can only be applied to this patient group.
However, the characteristics of our cohort are comparable with the results of the UK Comparative Audit of Upper GI Bleeding, increasing the generalisability of our findings to the UK and other healthcare systems comparable with the NHS.18 Being conducted in a district general hospital without ready access to on-demand endoscopy, particularly out-of-hours, reflects the situation for the vast majority of hospitals in the UK and again increases the generalisability of our findings. Although relatively small in size, our cohort is the largest validation of the AIMS65 score until now and is comparable in size with other validation studies. Unlike the original derivation and validation studies, we looked at 30-day mortality as opposed to inpatient mortality. As the only acute hospital for a large rural area of 33 000 km2, many of our patients are subsequently stepped down to smaller community hospitals once they have undergone their initial acute management. Thus, looking at inpatient mortality only would have biased our findings and potentially resulted in a spuriously low mortality figure.
In conclusion, we independently validated for the first time the AIMS65 score in a predominantly Caucasian population from Northern Europe. Although superior to the GBS in terms of predicting mortality, the exact role of the AIMS65 scoring system in triaging patients presenting with ANVGIB remains to be established. Future prospective studies should look to answer this question and define the role of the AIMS65 scoring system in the setting of acute upper GI bleeding, particularly with respect to identifying those patients who may benefit from early intervention on the basis of their predicted mortality.
Key messages
What is known on this topic
AIMS65 is a novel, recently derived scoring system for acute upper GI bleeding, which has been shown to accurately predict mortality, cost and length of stay in US populations.
What this study adds
AIMS65 accurately predicted mortality in a Scottish population and was superior to the Glasgow-Blatchford score (GBS).
The GBS was superior in predicting requirement for blood transfusion and admission to HDU.
Non-inferiority to the GBS was demonstrated with respect to requirement for endoscopic intervention, endoscopy refractory bleeding, rebleeding and admission to ICU.
How might it impact on clinical practice in the foreseeable future
AIMS65 predictive capacity warrants testing in prospective studies to establish the exact role of this scoring system in the triaging of patients with acute upper GI bleeding.
Its ease of use may help clinicians to follow consensus recommendations to use risk assessment scores for targeted management.
Acknowledgments
We wish to thank the medical records department of Raigmore Hospital, particularly Sabine Kelly, for identifying and sourcing all the medical records required for this project. Part of this work was presented at the 2014 United European Gastroenterology Week Annual Conference.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors AJP and CV had the original idea. AJP designed the study, collected data, conducted the analysis and wrote the paper. FM helped design the study, collected data and was involved in editing the paper. SM, GC, JB, CM, MR and RC collected data. DDLH provided expert opinion and was involved in writing and editing the paper. CV provided expert opinion, was involved in writing and editing the paper and led the group. All authors reviewed the paper prior to its final submission.
Competing interests None declared.
Ethics approval NHS Highland Clinical Governance team as a retrospective audit.
Provenance and peer review Not commissioned; externally peer reviewed.