Article Text

Abstract
Barrett's oesophagus (BO) is the only known precursor to oesophageal adenocarcinoma (OAC). Dysplasia and intramucosal cancer arising in BO can safely be treated with endoscopic eradication therapy (EET) due to the low risk of subsequent lymph node metastasis. Treatment at an early stage is paramount due to the ongoing poor prognosis and outcomes of patients with advanced OAC. The mainstay of treatment is endoscopic resection of visible lesions for accurate staging followed by ablation therapy to all remaining columnar-lined epithelium, most commonly with radiofrequency ablation. Successful eradication of dysplasia can be achieved in >95% of patients with this EET combined approach.
- BARRETT'S OESOPHAGUS
- OESOPHAGEAL CANCER
- ENDOSCOPIC PROCEDURES
- BARRETT'S CARCINOMA
Statistics from Altmetric.com
Background
The UK has one of the highest incidence of oesophageal adenocarcinoma (OAC) in the world.1 OAC has a poor prognosis, with <20% of patients surviving at 5 years.2 An important factor driving this poor survival is the late presentation of the disease.
The only known precursor to OAC is Barrett's oesophagus (BO). The overall risk of BO to progression to OAC is estimated at 0.12%–0.48% per year, while the risk for progression to OAC or high-grade dysplasia (HGD) is 0.26%–0.63% per year.3–7 Progression of low-grade dysplasia (LGD) to OAC has been reported as 5.1 per 1000 patient years compared with 1 per 1000 patient years without dysplasia.5 HGD and intramucosal cancer (IMC) has a reported risk of OAC of over 10% per year.8
Risk factors
Risk factors for progression to HGD or OAC include reflux,9 male sex,10 increasing age,7 obesity (particularly waist:hip ratio)11 and length of BO.12
The metaplasia, dysplasia, cancer pathway
Chronic exposure to acid or bile refluxate injures the epithelium resulting in inflammation and cell proliferation. In combination with genetic instability, this is thought to trigger the development of Barrett's metaplasia. Continued exposure and inflammation activates epithelial–mesenchymal transition to the development of LGD, HGD and finally invasive OAC.13
Staging of dysplasia/early cancer
Staging of early oesophageal cancers allows the stratification of patients according to subsequent lymph node metastatic risk and allows appropriate local modalities of treatment to be offered. Once a tumour involves regional nodes or distant metastases, local treatment with endoscopic intervention is no longer a curative option. It is therefore imperative in patients with Barrett's dysplasia or early OAC that treatment is offered when there is still curative intent. The depth of the cancer is correlated with the risk of lymph node metastases.14
IMC also known as a T1a cancer carries a 1.3% risk of lymph node metastasis,15 whereas the risk with submucosal T1b cancer is related to the depth of invasion;16 with SM1 carrying a 6% risk, SM2 a 23% risk and SM3 a 58% risk.17
Further risk factors for lymph node involvement include histological evidence of poorly differentiated tumour grade and lymphovascular invasion.17 Due to this risk of nodal disease, only LGD, HGD and tumours staged as T1a, or T1b with no poor prognostic markers are offered endoscopic treatment.18 Recent National Oesophago-Gastric Cancer Audit (NOCGA) data indicate the risk of surgical mortality following oesophagectomy is higher than the risk of lymph node metastases in patients with superficial cancer and HGD;19 hence, the British Society of Gastroenterology (BSG) Guidelines currently recommend endoscopic eradication therapy (EET) as first-line therapy for early disease.18
Dysplasia detection
Early detection of lesions in BO is essential to drive any subsequent endoscopic treatment options. Visualisation of subtle mucosal lesions can be enhanced with novel wide-field imaging technology that can be used on the entire oesophagus to highlight areas of interest including acetic acid chromoendoscopy and virtual chromoendoscopy (summarised in table 1). Both narrow band imaging (NBI) and i-Scan technologies can be combined with magnification endoscopy, which allow areas of interest to be viewed with up 136 times magnification.
Virtual chromoendoscopy technologies
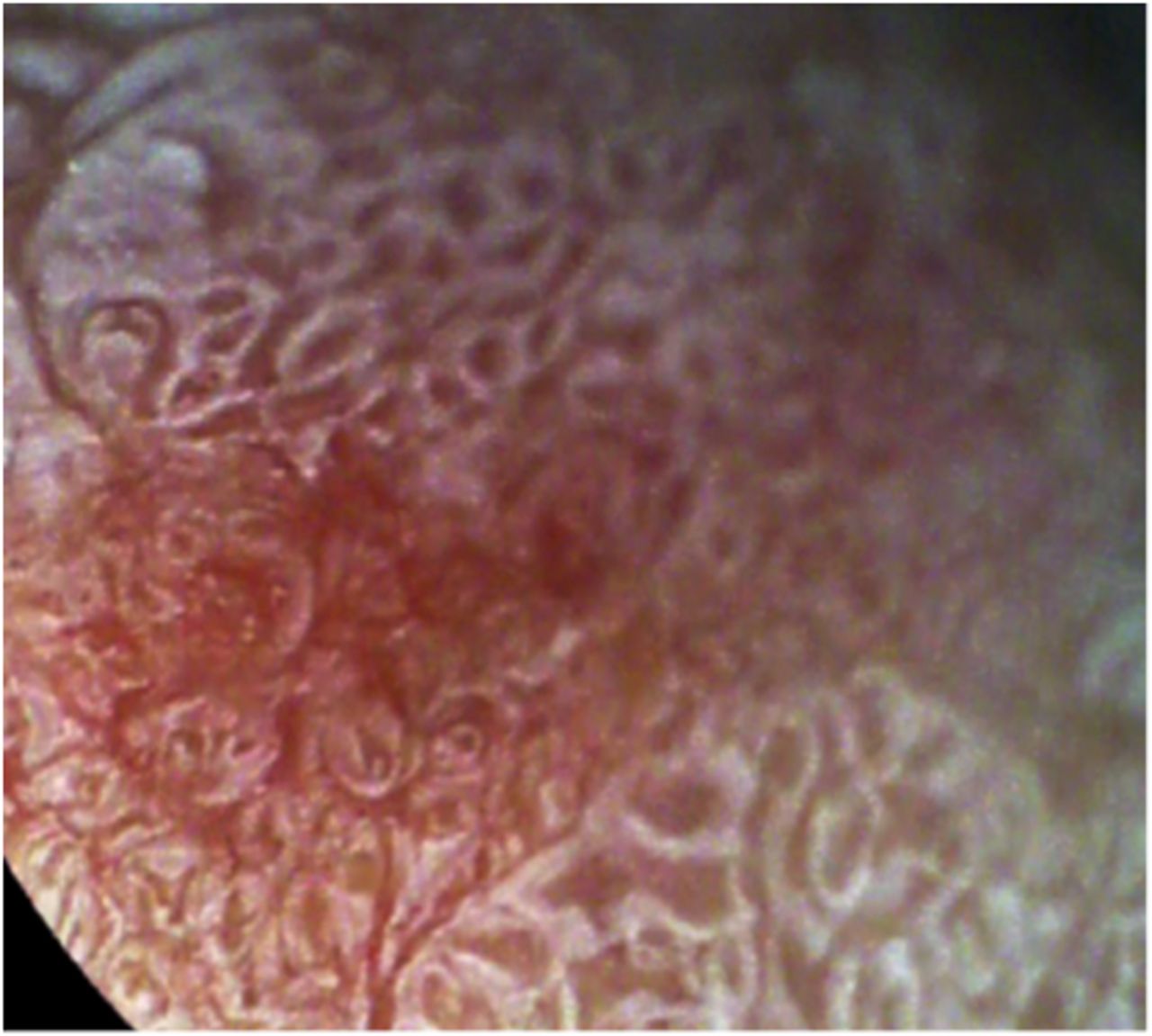
Acetic acid (2%–3% strength) causes the metaplastic (Barrett's) epithelium to whiten, highlighting the mucosal pattern. Dysplastic lesions are thought to lose this white appearance faster than non-dysplastic areas, permitting targeted assessment and sampling of these areas (figure 1). A recent meta-analysis of nine studies, calculated a pooled sensitivity of 92% and specificity of 96% for the diagnosis of high-grade dysplasia or IMC.20

i-Scan magnification endoscopy to demonstrate the loss of whitening after application of 2% acetic acid in dysplastic Barrett's oesophagus.
Real-time in vivo diagnosis of Barrett's dysplasia is possible with confocal laser endomicroscopy but requires a targeted approach and operator expertise for interpretation.21
Although all these technologies allow for greater detection of subtle lesions, they also require specialist expertise to recognise these abnormalities. Recent research has shown that a longer procedure time to allow a detailed inspection of the mucosa using high-quality white light imaging may yield just as accurate diagnosis.22
Treatment options
Historically, treatment for early gastrointestinal neoplasm required major surgery, with the associated morbidity and mortality of oesophagectomy. Early neoplasms confined to the superficial layers of the mucosa and submucosa can now be treated endoscopically with minimal risk of nodal and metastatic spread.17 Despite these advances and BSG guidelines, the 2015 NOCGA reported that of 930 patients with HGD, 26.2% underwent surveillance alone with no therapy, 67.5% received endoscopic treatment and 6.3% surgical resection.19
Endoscopic mucosal resection
Endoscopic mucosal resection (EMR) enables accurate histological assessment of the depth of invasion of early neoplastic lesions, thus being both a diagnostic and a therapeutic intervention. EMR can both upstage the diagnosis in 10% of patients and downgrade the diagnosis in 21%.23 EMR techniques include cap-assisted, ligation-assisted (the Duette multiband mucosectomy device, Cook, USA or the Captivator device, Boston Scientific, USA) and cap- and snare-assisted resection. As monotherapy, complete resolution of dysplasia (CR-D) rates are 87%–96%, but strictures occur in 12.5%–88% (higher rates with larger and circumferential resections).24 ,25
Endoscopic submucosal dissection
In contrast to EMR, where large lesions may be removed piecemeal, endoscopic submucosal dissection (ESD) allows large lesions to be removed en bloc, as well as resection of tumours arising from the muscularis propria. ESD requires extensive training, longer procedure time and is associated with an increased risk of bleeding and perforation.26 There is also an increased rate of stricture formation after ESD which can make subsequent ablation of the residual BO area challenging.27 Therefore, ESD is only considered for lesions larger than 15 mm, poorly lifting tumours and lesions at risk of submucosal invasion.28
Radiofrequency ablation
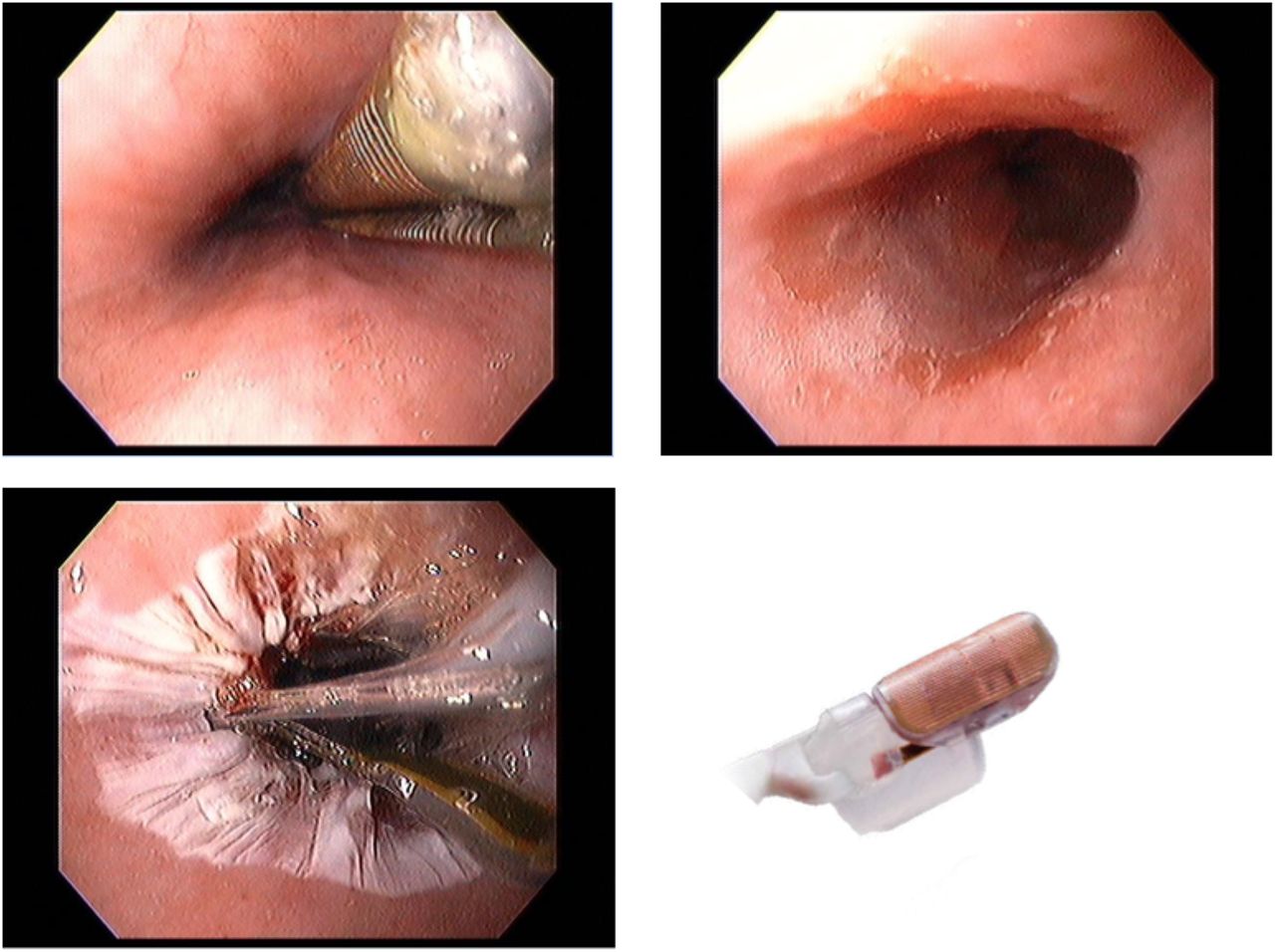
Radiofrequency ablation (RFA) (Medtronic) is a field ablation technique used to ablate the surface 500 µm of the gastrointestinal mucosa. It is primarily used in the treatment of Barrett's-related neoplasia using a balloon (to provide a 360° ablation field) or a focal device, mounted over the endoscope (figure 2). Several treatments over the course of months are required to effectively treat BO and any associated neoplasia. The treatment has a high success rates and good durability data now exist and has over the past 10 years become the mainstay of treatment of these patients with BO neoplasia.29
{kind=link}
{kind=link}
Radiofrequency ablation of Barrett's oesophagus. Circumferential Barrett's oesophagus prior to ablation (top left), placement of the 360 balloon catheter (top right) and following ablation (bottom left). Focal devices are also available (bottom right) (with permission from Medtronic).
The breakthrough randomised controlled trial in 2009 reported CR-D rates of 81% of patients with HGD with a 6% stricture rate.30 However, RFA treatment alone is insufficient for the treatment of Barrett's dysplasia where there are nodules or ulcers due to the risk of buried dysplasia. Therefore, all visible lesions are first removed with EMR and the residual BO, whether dysplastic or only metaplastic is treated with RFA.18 The UK RFA Registry reports that this combined EMR and RFA approach achieves CR-D rates of 86% and complete resolution of intestinal metaplasia (CR-IM) rates of 62%.31 Recently, a multicentre trial used this combined approach and allowed visible BO at the end of 12 months treatment to be retreated with either a further resection or an argon plasma coagulation (APC) treatment. This protocol achieved 92% CR-D and 87% CR-IM with only 4% of patients reporting recurrence at 36 months of follow-up.32 Treatment of LGD is now recommended following the SURF trial that reported patients who received RFA had lower rates of progression to HGD or OAC than those receiving surveillance only.33
Recurrence
With all endoscopic therapies for Barrett's neoplasia, recurrence of disease following initially successful treatment remains a risk. RFA has been shown to be a durable treatment option for Barrett's-associated neoplasia with a recent meta-analysis reported a pooled recurrence rate of 6.0% per patient year.34 Following eradication of HGD by endoscopic therapy or surgery, endoscopic follow-up is required35 and recent data combining the US and UK RFA registries, has suggested follow-up intervals can be stratified according to risk. Most patients with HGD and IMC should have endoscopic examinations of the treated oesophagus 3, 9, 18 and 30 months after treatment ends and should continue thereafter with yearly assessments.36
Specialised centres
Reflecting the centralisation of upper gastrointestinal surgical centres for cancer in the UK, the BSG also recommends the centralisation of endoscopic resection due to the low but significant risk of complications requiring surgical intervention. As most patients undergoing treatment for BO-associated dysplasia require dual therapy with EMR and RFA, the BSG advises that RFA also be performed only in centres where endoscopic resection can be performed. The BSG also recommends that a minimum of 30 supervised cases of EMR and RFA should be performed to acquire the necessary technical skills and management of complications.18
Argon plasma coagulation
APC uses argon gas to conduct electrical current to thermally ablate targeted tissue. APC is often used as an adjunct to alternative therapies, as it is cheap and easy to treat small areas of residual disease and has been demonstrated to significantly increase recurrence-free survival for the patients undergoing ablation after EMR compared with those having EMR alone.37 A feasibility study comparing APC with RFA recently reported preliminary findings that suggested that at 12 months there was no difference in CR-D rates.38 However, there are still no large volume data to support APC as first-line ablative therapy for patients with BO neoplasia and further studies are required in this field.
The future
The development of endoscopic tools to improve the diagnosis and management of patients with Barrett's dysplasia is on-going and evolving rapidly. Several technologies are currently in clinical trials to assess their efficacy.
Imaging
Autoflouresence (AF) is a virtual endoscopy technique using the variable quantities of fluorophores (substances that emit fluorescent light after exposure to short, blue light wavelengths). Alterations in the autofluorescence pattern of neoplastic tissue is translated into false colour images, usually depicting neoplasia in purple against a green background of healthy mucosa. AF has been integrated with high definition white light endoscopy and NBI as part of the ‘endoscopic trimodal imaging’ system.
Optical coherence tomography (OCT) uses reflected light in a manner similar to acoustic ultrasound to generate high-resolution three-dimensional images. This allows ‘visualisation’ of the mucosa to a depth of 1–2 mm. Currently performed with a probe through the working channel of an endoscope, the future may involve tethered capsule technology (where capsules attached to a string are swallowed and then retrieved) and rapid assessment of the tubular oesophagus. Recent studies have suggested a role for OCT for surveillance after ablation therapy with radio-frequency ablation.
Treatment
Cryoablation uses liquid nitrogen to form intracellular and extracellular ice that causes ischaemic necrosis on thawing and apoptosis of the treated cells. Previous limitations of cryotherapy included the large volume of gas produced during therapy; however, a new focal balloon device avoids this risk using a self-contained unit that does not introduce gas into the stomach (Cryoballoon Focal Ablation System, C2Therapeutics, USA).
A 2016 study reported on 96 patients, 91% of patients with LGD achieved CR-D and 61% CR-IM and 81% of those with HGD achieved CR-D and 65% CR-IM. No perforations or deaths were reported and there was a single stricture that did not require dilatation.39
Conclusion
The management of Barrett's-associated dysplasia has changed dramatically in the last 10 years. Our continued understanding of which lesions are amenable to EET means that we can confidently offer a long term curative treatment to the majority of patients with early disease and avoid disease progression and the need for surgery for these select patients. Meticulous lesion recognition with combined high-quality endoscopic imaging modalities followed by endoscopic resection and ablation with RFA remain the foundation of treatment for most patients. Advances in optical imaging for diagnostic and surveillance purposes coupled with new interventional technologies such as cryotherapy may further improve outcomes and allow us to treat a wider cohort of patients.
References
Footnotes
Contributors Both authors have contributed to the writing of this article.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.