Article Text

Statistics from Altmetric.com
Introduction
The concept of burn-out, defined as a complex construct of emotional exhaustion, depersonalisation and a decline in personal achievement, was first introduced by Herbert Freudenberg nearly five decades ago.1 Burn-out affecting all levels of healthcare professions is increasingly reported in the literature.2–4 Up to one-half of gastroenterologists report burn-out, with increased rates among trainees, early career physicians and interventional endoscopists.5 A recent UK survey on practising gastroenterologists reported significant rates of emotional ill health and work-related stress which impacted work performance.6
The factors contributing to burn-out among gastroenterologists include excessive clinical work load with increasing demands related to the complexity of patient care, work productivity, electronic health records (EHR), documentation to measure endoscopy standards as well as the lack of autonomy, administrative support, workplace relationships, work and home conflicts.5 6 Furthermore, the drivers of clinician burn-out may also lead to ‘moral injury’ when the knowledge of the care needs of the patient often at odds with the ability to provide it due to constraints are beyond the clinicians’ control.7
Burn-out may have grave consequences to the health of physicians and is associated with depression, increased risk of substance abuse and a twofold increase in the risk of suicide.4 6 In a UK survey,6 one-fifth of the respondents required occupational health or medical interventions including use of antidepressants or anxiolytics. Burn-out is linked to suboptimal patient care practices potentially impacting on safety, reduced access to care, and reduced patient satisfaction. Furthermore, the healthcare system as a whole may be adversely affected due to the cost associated with physician turnover and reduced productivity.
Since the first case of COVID-19 was reported in Wuhan, China in December 2019, there has been an exponential increase in publications related to both COVID-19 and burn-out. The viral pandemic not only amplified the burn-out pandemic among gastroenterologists but it has uncovered additional layers to this global problem.
The impact of COVID-19
The COVID-19 pandemic has led to unprecedented challenges for healthcare systems globally. In addition to the physical exhaustion, psychological challenges are reported in healthcare workers with high rates of anxiety, depression and insomnia.8 In addition to this systemic problem encountered by all High Expectations and Risk Occupation (HEROs),8 gastroenterologists face a unique set of challenges.
Gastroenterologists are being faced with the challenges of the repeated waves of the pandemic impacting their routine practice. Changing guidelines in relation to aerosol generating endoscopic procedures which form a significant proportion of practice has been difficult to adapt. There is fear that personal protective equipment (PPE) supplies in order to protect ourselves, our patients and our loved ones that we go home to at night may run out. Gastroenterologists have faced further difficulties related to changes in practice patterns such as cancellation of routine clinics and endoscopy lists and in some hospitals, physicians are even being asked to redeploy to other areas including as internal medicine physicians. There have been financial reasons for stress such as physicians facing pay cuts worldwide which has impacted gastroenterologists as well.
The fallout from the pandemic has extended to trainees in Gastroenterology as well. A recent international survey by Pawlak et al has found that there has been a significant impact on endoscopic training globally including significant reports of burn-out among trainees.9 Many factors are implicated in burn-out among trainees during the pandemic, including reducing training opportunities, worry about job security, lack of social interaction and increased working hours.10
The power of human contact in medicine is also suffering as a result of COVID-19 restrictions. Our interactions with colleagues are more limited and most often via virtual meetings as we sit behind our desks at home. Virtual visits and even in-person clinic visits (with masks on) have changed our interactions and affect the rapport between physicians and patients. There is no longer the opportunity to interpret a patient’s understanding or grasp of what was said by non-verbal cues such as facial expressions hidden behind the masks. A new diagnosis of cancer that would normally prompt a gesture like a hug or hand on the shoulder is now no longer considered normal in this era of social distancing and layers of PPE. Family members are no longer allowed to accompany loved ones in the preoperative area prior to endoscopy and are forced to wait in cars. We struggle to connect with our patients who are not tech savvy or who cannot afford to communicate with us electronically and there is increasing recognition that virtual consultations are here to stay post pandemic due to resource and environmental considerations. Our inboxes are flooded with messages from patients who want to be seen but are fearful of the possibility of acquiring COVID-19 if they come to our clinics and hospitals.
At some point, we must ask ourselves when enough is enough. When is it acceptable to say no, to work less, accept vulnerability and ask for help.
Future steps and considerations
Prevention and management of burn-out requires interventions at an organisational level and the individual level in parallel. Organisations should be particularly aware of the emotional needs of all healthcare professionals including gastroenterologists under the HEROs framework.8 Competent leadership, open communication, transparency, interventions to reduce the EHR burden and employee assistance programmes that include wellness and stress management are paramount to tackling this pandemic of burn-out.
At the individual level, it is critical to have both self-awareness to recognise burn-out and self-compassion at this time. We can learn from our individual triggers for burn-out and try to avoid these when possible. However, many stressors are structural or systemic in healthcare, and often out of our control. More importantly, we must learn to modulate our response to these stressors and create better ways to interact, increase efficiency, while feeling supported.
Herein, we offer five potential strategies for gastroenterologists in hopes to help in minimising burn-out (figure 1):

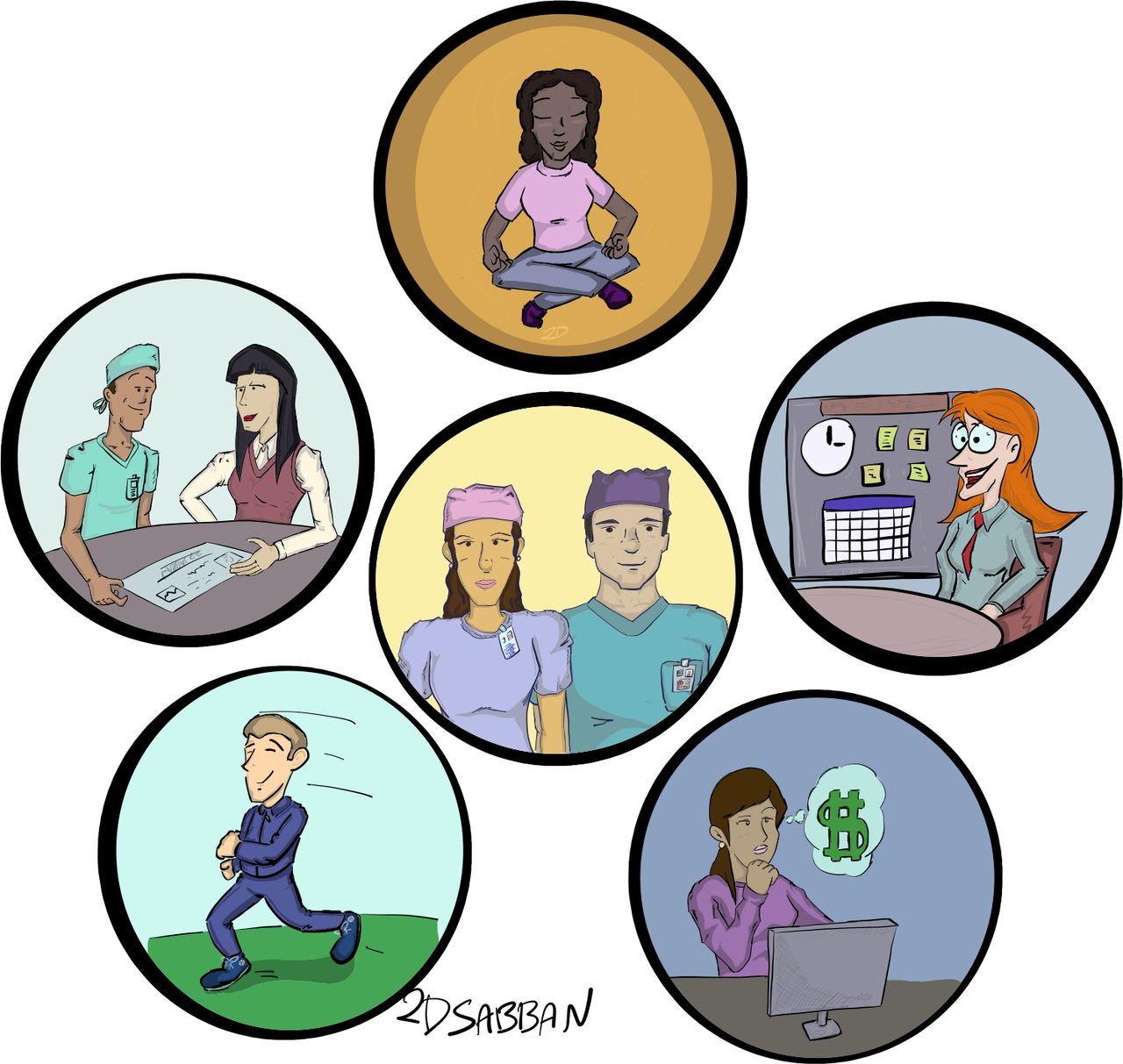{kind=link}
Image illustrated by Abdulhameed Al-Sabban.
Avoid isolation
Isolation appears to be a major contributor to physician burn-out, and conversely, social support and connectedness is associated with significant mental and physical well-being.11
Gastroenterologists should create as well as avail, of opportunities to connect with peers and colleagues at the organisational level, and through professional societies. In fact, engagement in professional societies and social groups has been shown to help overcome physician burn-out.12
Although opportunities to travel, socialise and attend meetings in-person are limited due to the pandemic, many medical societies currently are offering professional and educational support for virtual connections. In addition, social media, in particular Twitter, provides a connection with other gastroenterology colleagues from around the world in a variety of forums.13 Connecting with family or others in the local community can be helpful as well.
Be fiscally and environmentally sustainable
Gastroenterologists like all healthcare professionals should use sustainability principles in their practice. This may range from adopting ‘green’ principles in areas such as endoscopy14 by opening up opportunities in innovative care models fit for the next decade. We should find ourselves as innovators developing creative ways to repurpose, reframe and reallocate scarce resources. Given the financial uncertainty many private practice and employed physicians are facing due to the decreased volume, this may be counterbalanced by fiscally conservative sustainable healthcare delivery to decrease financial pressures. If facing job insecurity, other career options to explore include locums tenens, research, consulting or pharmaceutical industry positions.
Refine time management and documentation skills
Gastroenterologists should prioritise responsibilities, use templates where possible and delegate tasks that can be safely completed by a non-physician to other team members.15 Document the necessary information without being superfluous and complete the note at the time of the visit or immediately after. Review expectations with patients and administrators about electronic mail messaging as it cannot replace an office or telemedicine visit.
Consider professional coaching and counselling
Gastroenterologists should actively seek care for anxiety and depression that may be associated with burn-out. Professional assistance for stress management via cognitive–behavioural therapy or mindfulness-based stress reduction) can help with burn-out.16 In a recent randomised study of physicians, six coaching sessions over a 5-month period reduced emotional exhaustion, decreased burn-out and improved quality of life and resilience scores compared with controls.17 Coaching can help to set goals, provide accountability, and identify values and strength in character.
Incorporate daily self-care practices
Self-care is tending to and actively nurturing to one’s well-being. Physical, mental and emotional self-care is key to avoid and mitigate burn-out. This includes getting adequate nutrition, sleep, exercise and avoiding unhealthy coping mechanisms. Incorporating practices for stress reduction depending on personal interests such as mindfulness, spending time within nature and breathing exercises may be beneficial. A number of applications such as Headspace or CALM have been recommended to be useful for healthcare professionals to build moral resilience by focusing on self-care.18 Physical exercise is also a well-established factor to improve mood and alleviate stress and may help mitigate and prevent burn-out among gastroenterologists.19
Summary
The demands on the gastroenterologist extend beyond his or her hours at work. Although a vaccine for COVID-19 is here now, there will never be a vaccine for burn-out. We need to tackle burn-out as a profession—recognising it, addressing it, and resolving it.
Ethics statements
Footnotes
Twitter @AparnaRepakaMD
Correction notice This article has been corrected since it published Online First. The first affiliation has been amended.
Contributors ND: conception of manuscript. All authors: edited and contributed to the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- UpFront