Article Text

Abstract
Background Inflammatory bowel disease (IBD) predominantly affects young adults at critical socioeconomic periods of their lives. There are no studies examining the process of transfer of care for adult patients with IBD changing healthcare providers. Our aims were to assess the quality of referral information provided when patients with an established IBD diagnosis transfer care between heathcare providers and to assess the impact of referral quality on patient outcome.
Methods Retrospective data pertaining to IBD transfer of care referrals were collected from 16 hospitals across London over a 2-month period. Data were collected on patient demographics, source and content of referral and cross-referenced with an established transfer of care checklist. Patient outcome within the 6 months following transfer was also documented.
Results 154 cases were identified, over half of which transferred due to patient relocation. Details included in transfer letters were in many cases incomplete. In over 70% of cases, the letter came from primary care, including when a tertiary opinion was sought. Although referrals from primary care contained fewer patient data points, there was no association with poor patient outcomes at 6 months.
Conclusion This is the first study examining the quality of transfer of care in adult patients with IBD. We highlighted a significant and underreported issue and found that the majority of referrals were led by primary care. Though the inclusion in the referral of fewer data points was not associated with poor outcomes, we highlighted an area where gastroenterologists might take more responsibility to provide smooth and robust transfer of care.
- inflammatory bowel disease
- audit
- epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known on this topic
Patients with inflammatory bowel disease (IBD) undergoing paediatric to adult transition benefit from the application of quality standards to minimise disruption to their continuity of care.
What this study adds
We demonstrate the previously unknown scale of IBD patient transfer in the greater London region and show that this process is largely led by general practitioners rather than gastroenterologists.
How might it impact on clinical practice in the foreseeable future
We believe this study will inform the development of new standards of care for patients with established IBD who wish to transfer their care between providers.
Introduction
The prevalence of inflammatory bowel disease (IBD) is increasing, affecting 1 in 125 people in the UK,1 the majority of patients cared for in a hospital setting. Incidence peaks in the third and fourth decades of life, affecting people at critical social and economic periods of their lives. This population is particularly mobile and likely to move to locations more frequently than older persons2; hence, there is the potential for frequent changes in healthcare providers, which may impact on care.
A multidisciplinary approach is currently the gold standard in providing holistic care with most patients requiring regular outpatient follow-up and long-term medication to prevent disease flares and associated complications.3 Continuity of care is vital in managing IBD, and we can learn from studies of the process of transition from paediatric to adult care. Although this is also a relatively under-researched area, there are comprehensive guidelines and pathways for the transitioning of care between paediatric and adult IBD services.4 Crucially, difficulties in transition for this cohort have been shown to negatively impact engagement with health services and adherence to therapy.5
There is a paucity of evidence regarding adult patients with IBD who need to transfer their care to a new secondary or tertiary care provider, both in terms of how effectively this is done and whether it affects outcome. There is a risk of miscommunication when patients move between care providers, and currently, there is no metric capturing this process.6 We do not know how common transfer of care in adult patients with IBD is, nor how it may impact on their experience and disease course.
This is the first study, to our knowledge, to look into this under-researched area of IBD care. We expect our findings to inform future guidelines as well as the expected standards of IBD care, with the aim of benefiting patients and their carers.
Aims
Our primary aim was to assess the quality of referral for adult patients transferring care between providers, according to the number of key data points included in the referral. This was assessed against the Cornerstones Health ‘IBD Checklist for Care Continuity’ (see online supplementary appendix).
Supplemental material
Our secondary aims were to identify the frequency of transfer of care among the London population and to report disease-related outcomes in patients transferring their care, determining whether the quality of the referral was related to poor outcome.
Methods
The pan-London Gastroenterology London Investigative Network for Trainees network is a collaborative group of trainees based at hospitals across London. Participation in the trainee network is on a voluntary basis, and individuals self-selected to collect data from individual hospital sites according to an agreed proforma. Retrospective data were obtained for outpatient IBD transfer of care referrals between 1 January and 28 February 2018.
We identified all referrals for new adult patients attending outpatient clinics who were transferring their care from an existing gastroenterology team elsewhere. All new patients with IBD attending outpatients were included in the study, and all patients had an established diagnosis of IBD.
Since no prescriptive standards currently exist in the UK or continental Europe on optimal clinical documentation in regard to transfer of care in IBD, we elected to use as a guide the IBD Checklist for Care Continuity provided by Cornerstones Health, a US-based not-for-profit organisation aiming to advance IBD care worldwide. To our knowledge, this is the only widely available document with guidance on continuity of care for patients with IBD, though it has not previously been used as a research tool.6 This is a freely available checklist based on the consensus of international IBD experts and was used as a guide for the data collection.
Original notes, electronic data and clinic letters were interrogated. Local departmental approval was gained each for each participating site.
Variables collected
Adults over the age of 18 years were included if they had an existing diagnosis of IBD and were transferring to a secondary or tertiary healthcare provider. Hospital records were assessed for measures of good quality care transition as derived from Cornerstones Health IBD Checklist for Care Continuity.6
The following information was recorded on a standardised proforma: patient demographics, source of transfer letter and reason for transfer, information relating to the IBD diagnosis (type of IBD, Montreal classification, medication history, surgical history, coexisting conditions, latest endoscopy and imaging) and patient outcome within 6 months of a consultation following the referral. This study aimed to identify missing data; therefore, data points not recorded in the transfer of care dataset were treated as not recorded. Where there were missing data in the outcome data, that is, no data on steroid use, those data were reported as missing and were excluded from the analysis. A poor outcome was defined as experiencing at least one of the following: a clinically diagnosed disease flare, steroid prescription, Accident and Emergency (A&E) attendance or hospitalisation.
Analysis
Discrete variables were analysed by Fisher’s exact test. Continuous variables were analysed by Kruskall-Wallis test with correction for multiple comparisons using the Benjamini, Krieger and Yekutieli correction (false discovery rate (FDR) 0.05). Statistics was performed using GraphPad Prism V.7 (TreeStar).
Results
Population
In total, 16 centres were included in the study. A total of 154 referrals of patients with known IBD diagnoses were identified in the 2-month study period. Fourteen referrals were excluded from analysis either as a result of incomplete referral data (n=6) or as they concerned transition from paediatric to adult care (n=8). A total of 140 referrals to transfer care received in 14 centres were therefore included in the analysis. Diagnoses were ulcerative colitis in 53.5% (n=75), Crohn's disease in 45.7% (n=64) and IBD unclassified in 0.7% (n=1).
Reason for transfer of care
The majority of transfers of adult care were for those moving geographical area (n=74, 52.9%), followed by those seeking a transfer into the NHS from the private sector (n=23, 16.4%), those seeking second opinions (n=21, 15%), those being referred for a tertiary opinion (n=14, 10%) or those lost to follow-up (n=3, 2.1%) (figure 1A). In five cases (3.6%), the reason for referral was unclear in the referral letter.
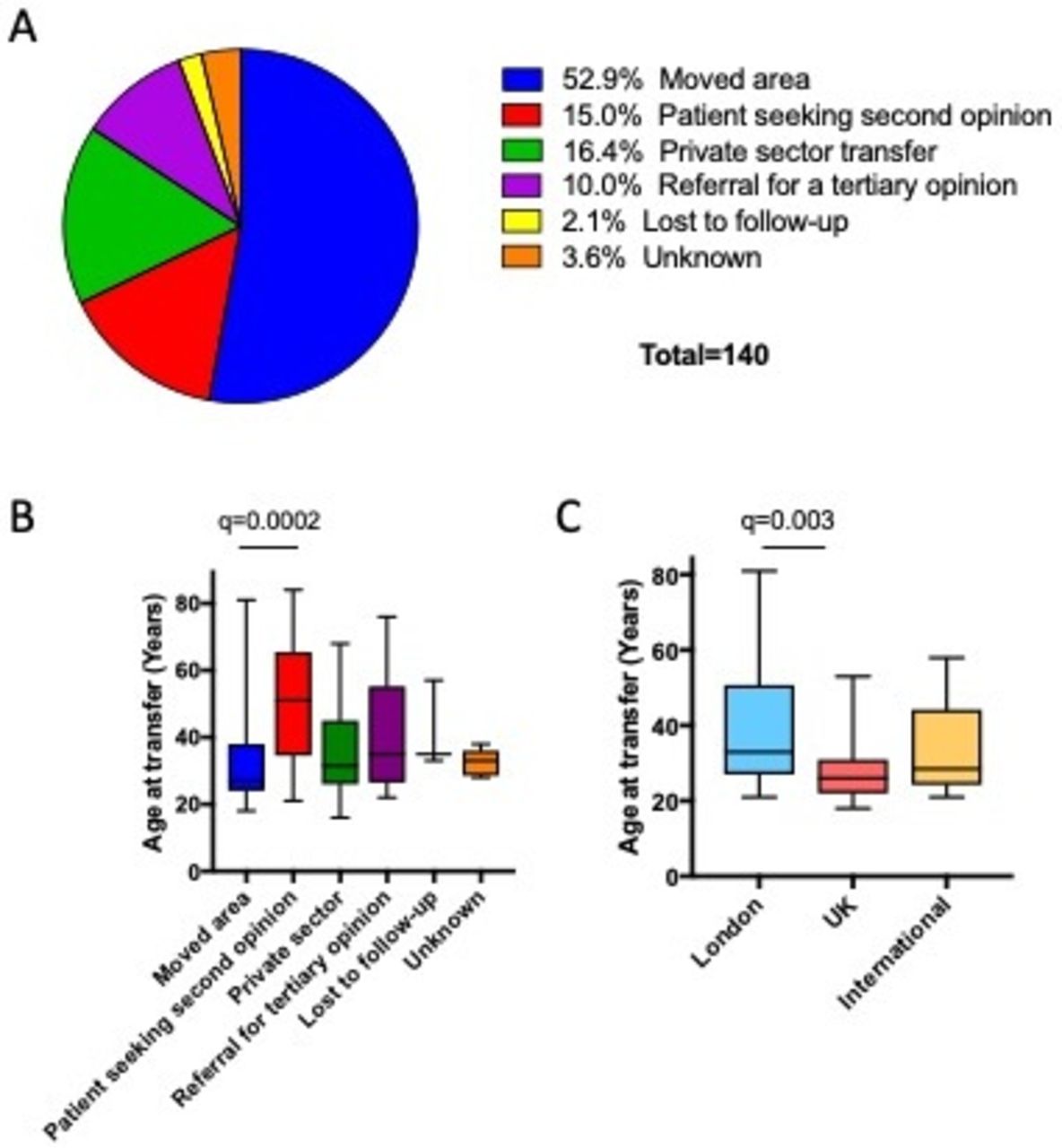
(A) Pie chart showing the reason given for transfer across all patients in the cohort. (B) Box plot showing the ages of patients grouped by their reason for transfer. (C) Box plot showing the ages of patients grouped by their geographical origin of transfer (London denotes transfer within London; UK denotes transfer from another location within the UK; International denotes transfer from outside the UK). Statistics was obtained using Kruskall-Wallis test with correction for multiple comparisons (FDR 0.05). Only statistically significant differences are displayed on the graphs.
The median age of referred patients was 32 years (IQR 26–46). The median age of patients seeking a second opinion was 51 years (IQR 34.5–65.5), which was significantly greater than those transferring their care due to a geographical relocation (27 years; IQR 24–38, q<0.001) (figure 1B). There were no statistically significant differences in age at referral between groups of patients transferring their care for other reasons.
The geographical origin of referrals was examined where data were available (n=91). Patients transferring care within London were significantly older at 33 years (IQR 27.0–50.75, n=48) compared with those transferring their care into London from other parts of the UK (26 years; IQR 22–31, n=23, q=0.003) (figure 1C). There was no significant difference between those referred within or into London from the UK and those immigrating from outside (28.5 years; IQR 24.25–44.5, n=20).
Source of referral information
To assess which group of practitioners is responsible for transfer of data, the primary referral source was assessed in each case. In the majority of cases, information regarding transfer of care came from primary care (n=100, 71.4%), with a minority coming from secondary care (n=29, 20.7%), and the rest, exclusively in the setting of those transferring from the private sector, came from private practice (n=11, 7.9%) (figure 2A).

(A) Pie chart showing the sources of the referral letter. (B) Pie charts showing sources of the referral letter grouped by the reason for transfer (i–iv as indicated).
The majority of referrals for those moving area were performed by primary care as opposed to secondary care (62 of 74 cases, 83.8%). This was also reflected in those being referred for a second opinion, in which primary care clinicians performed the majority of referrals (16 of 21 cases, 76.2%). Over half of transfers from private practice were also performed by primary care (12 of 23 cases, 52.2%) (figure 2Biii), and half of all referrals for a tertiary opinion were made by primary care (7 of 14 cases, 50%) (figure 2Biv). Any patients who were lost to follow-up were re-referred by primary care (n=3). There were five referrals for which the reason for transfer was not evident in the referral letter.
Information included in referral
The Cornerstone transfer of care bundle aims to improve the quality of transfer through the inclusion of specific details of care of patients with IBD.5 The inclusion of key pieces of data was assessed according to referral source, as demonstrated in figure 3A. Several criteria were documented more frequently by secondary care referrers compared with primary care referrers. These included the date of diagnosis (96.6% vs 64%, p=0.0003), medical history (89.7% vs 27%, p<0.0001), surgical history (65.5% vs 23%, p<0.0001), the most recent endoscopy report (51.7% vs 21%, p=0.002) and the most recent imaging findings (48.3% vs 11%,p<0.0001). However other data points, including data sufficient to apply the Montreal classification (28% vs 13%, not significant (n.s.)), current medication (90% vs 87%, n.s.) and comorbidities (52% vs 39%, n.s.) were equally likely to be included regardless of the referral source.
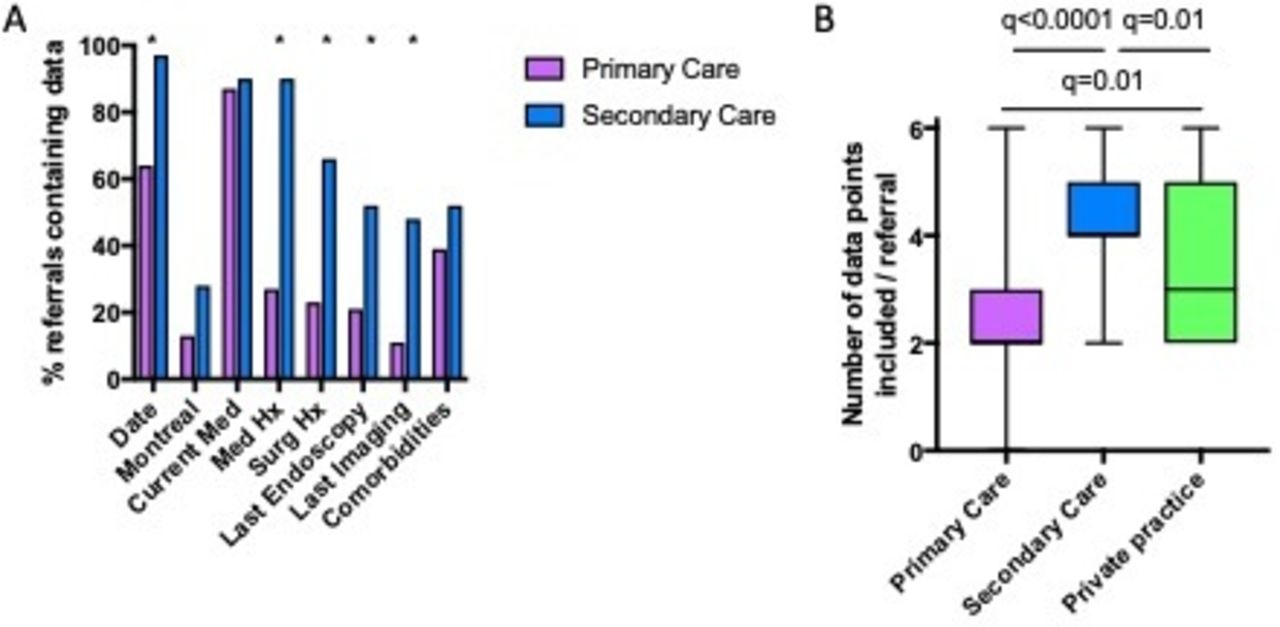
(A) Bar chart showing the proportion of letters which included each of eight data points identified as required, grouped by referral source. (date denotes the date of diagnosis; Montreal denotes sufficient information to establish Montreal classification; current med denotes current medication; last endoscopy denotes the last endoscopy report; last imaging denotes the last imaging report; comorbidities). Analysed by Fisher’s exact test. *P<0.05. Only statistically significant differences are displayed on the graphs. (B) Box plot showing the total number of data points included in each referral grouped by referral source. Hx, history; Med Hx, medication Hx. Surg Hx, surgical history.
Overall referral letters contained a median of three (IQR 2–4) data points per letter. The median number of data points was significantly higher in referrals from secondary care (n=4, IQR 4–5) compared with those from primary care (n=2, IQR 2–3, q<0.0001) and private practice (n=3, IQR 2–5, q=0.01) (figure 3B). Hence, while primary care performs the majority of such referrals, the data supplied from secondary care are in most cases significantly more complete than those from primary care.
Outcomes in the 6 months after a consultation following referral
Patient records were assessed for evidence of adverse outcomes in the 6 months after initial outpatient clinical review. A poor outcome was defined as having any one of a clinically diagnosed disease flare, steroid prescription, emergency department attendance or hospitalisation.
Overall, 36 (26%) patients experienced at least one adverse event, meeting the definition of a ‘poor outcome’. Twenty-seven patients (19%) were diagnosed with a disease flare; 20 (14%) required a steroid prescription; 11 (8%) had a documented attendance to an emergency care department; and 9 (6%) required hospital admission.
When the reason for transfer of care was analysed by outcome, a poor outcome was demonstrated in 5 patients (36%) referred for a tertiary opinion, 23 (31%) referred due to moving area, 4 (17%) referred from the private sector, 2 (10%) referred due to the patient seeking a second opinion and 2 (40%) with unknown reason for transfer. There was no significant difference in the proportions experiencing a poor outcome between each of these groups (p=0.193).
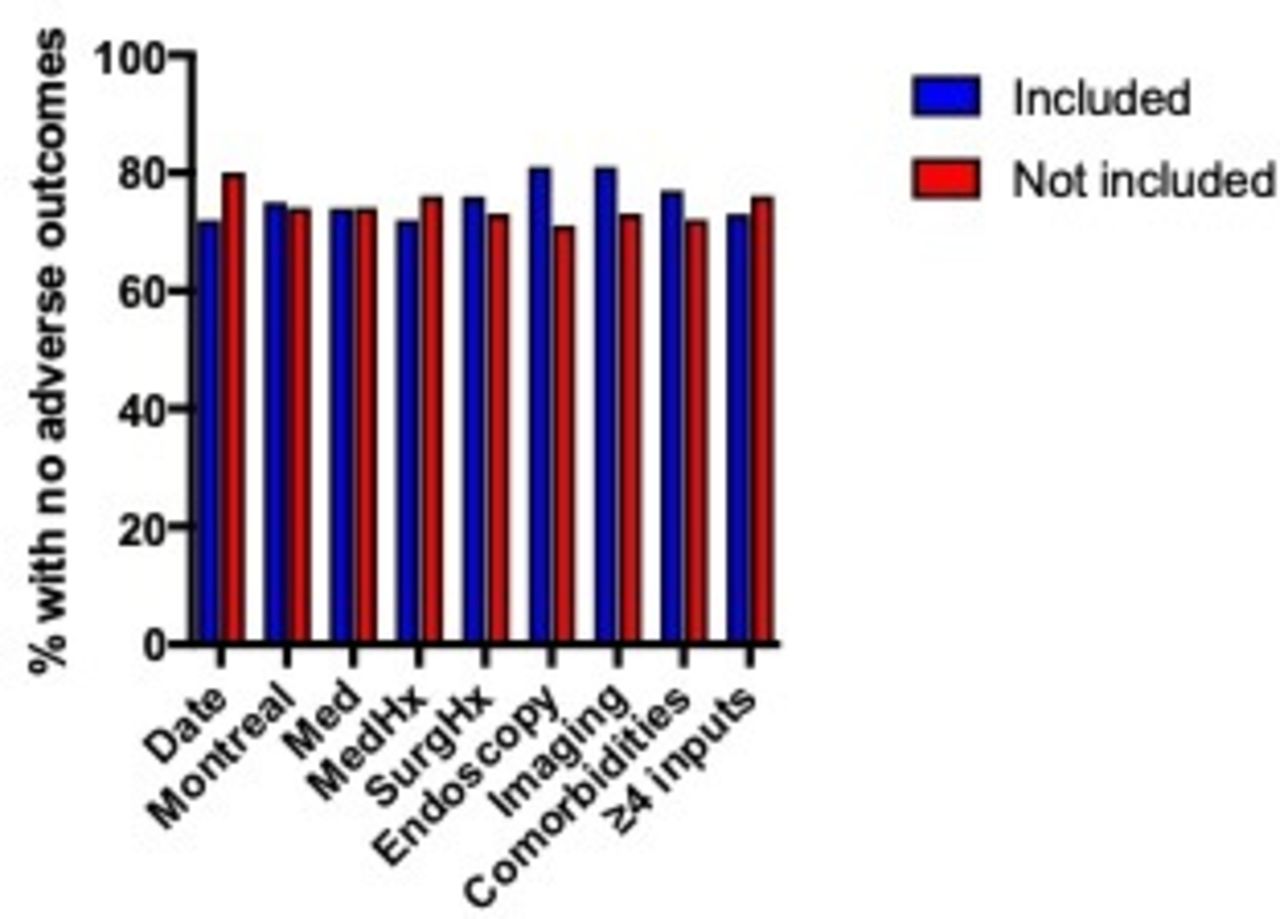
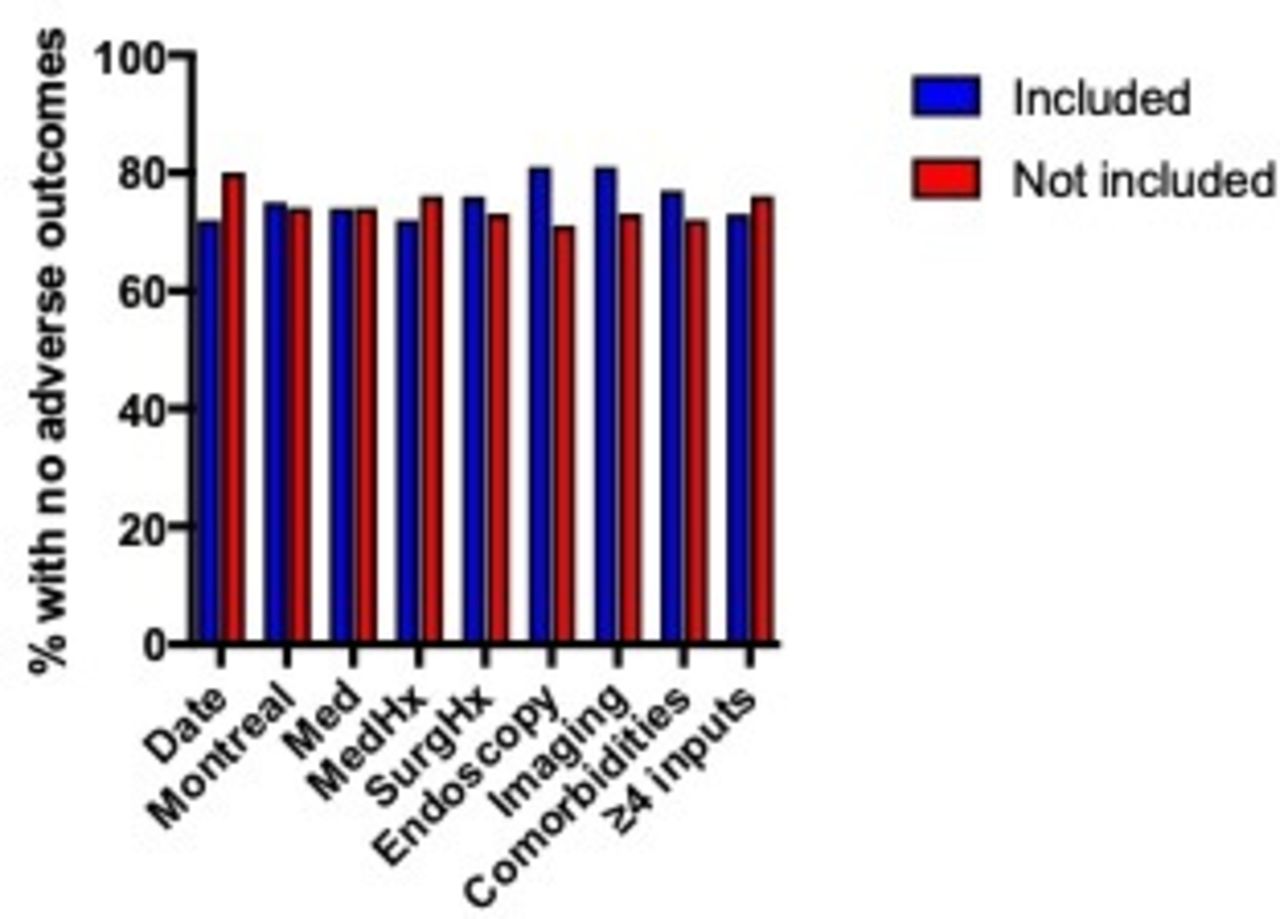
Each of the eight data points of interest in the referral letter was analysed by outcome (figure 4). No statistical difference was found in the proportion of patients experiencing a good outcome when comparing those in whom each data point was included versus not included. There was also no statistical difference in the proportion of patients experiencing a good outcome when comparing those in whom the referral letter had included four or more data points with those in whom less than four had been included.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Bar chart showing the percentage of patients experiencing adverse outcome grouped according to whether each required data point was included or not included, and whether four or more data points were included or not included. There were no statistically significant differences found.
Discussion
This is the first study to our knowledge exploring the transfer of care for adult patients with an established diagnosis of IBD within providers in the UK. Using a large network of London-based gastroenterology trainees, we were able to collect data from both secondary and tertiary hospitals serving a culturally diverse population. We found that relocation was the predominant reason for change of healthcare provider. Interestingly, most referrals were facilitated by primary care despite previous follow-up by another secondary care provider, and these referrals appeared to lack key clinical information. Escalation of therapy and other metrics of disease complications were identified in a quarter of the referred patients regardless of aetiology of provider change.
There were a large number of patients transferring their care into hospitals in the Greater London region during the 2-month period of our study. On an annual basis, there are likely to be almost 1000 patients transferring their care into or between these London hospitals. These were predominantly young adults who may be moving to study or to take up new employment in the capital. Although it is not clear whether these figures can be extrapolated nationally, it appears that the young IBD population is mobile. Secondary care providers may not always be aware of a patient’s intentions to move providers, which would limit their ability to provide a smooth transition to the receiving team. We believe it is therefore essential to empower patients to take ownership of their continuity of their care, and the emerging use of ‘app’ technology and data centralisation may have a role in this.
Most of the literature relating to transfers of IBD care describes the transition of adolescent patients from paediatric to adult services. Transfers of care in this context are also associated with increased health services use, with increased outpatient and emergency department visits.7 There are less data on the impact of adult patients moving between services, although recent studies in the UK and the USA have shown that fragmentation of IBD care—the use of more than one secondary care service—is common. In a retrospective study of administrative data in the UK, 17% of adult patients with IBD accessed a second outpatient IBD service within 2 years of their diagnosis.8 Younger patients and those living in metropolitan areas had higher rates of this care fragmentation.8 The use of multiple inpatient IBD services is also common. In another administrative dataset, from the USA, up to 33% of inpatients with IBD were readmitted to a different IBD service within 90 days.9 Again, younger patients were more susceptible to this care fragmentation, which was associated with worsening lengths of stay and in-hospital mortality.9
We found that, regardless of the reason for care transfer, the responsibility for the majority of referrals largely fell to primary care. Compared with direct referrals from gastroenterologists, referrals from primary care were less comprehensive. Lack of education on the essential clinical information for IBD-related continuity of care may be one of the contributing factors explaining this observation, but it is also possible that access to results of imaging and endoscopy in primary care is limited by insufficient communication. Barriers to clinical data access across healthcare providers in the UK remain a problem.10 Digital health technologies allowing for personal clinical information control may be one of the potential answers to this problem and would also allow for patient autonomy and smoother care transfer.10 11
Care transfers and care fragmentation for adult patients in IBD have been an under-researched field. Currently, there is no validated evidence to define continuity of care as a process measure of importance in IBD.12 The non-profit organisation Cornerstones Health sought to address this with an expert-informed checklist, documenting important elements of the IBD disease phenotype and treatment history.6 The checklist has not previously been used as a research tool to grade quality of care. Future work should evaluate the metrics that best categorise continuity of care in IBD and whether a supported implementation of the checklist improves those process outcomes.
Aiming to reduce variation in data collection, we implemented a strict data collection and data curation protocol as described in methodology. However, we were unable to access primary care records directly, basing our findings on hospital records in secondary and tertiary care. As a result, we were not able to fully describe the clinical characteristics of the population and to identify factors associated with poor outcomes relating to disease activity. Furthermore, other outcomes that were not investigated include patient satisfaction and increased cost and discomfort from repeat investigations. This study aimed to investigate the primary communication between referrer and receiving team; attempts by the receiving team to retrospectively obtain the information were not captured. However, this represents extra time and work for the receiving team, something that may be avoided by improving initial referrals. Further limitations include the fact that in some UK hospitals, referral straight from the private sector is not allowed, placing the onus back on to primary care, where access to all information may not be available.
Conclusion
In conclusion, our study highlights the previously underappreciated frequency of transfer of care between care providers for adult patients with an established diagnosis of IBD. In all settings, primary care appears to be the main facilitator of care transfer, but the lack of inclusion of significant metrics of care suggests they are less well equipped to manage this process. We believe that good communication between the patient, gastroenterologists and primary care is essential to facilitate smooth transfer of care, and that the use of digital health technologies may enable patients to take individual ownership of the transfer process. Wherever possible, we believe that gastroenterologists working in secondary care and in the private sector should take a proactive role in ensuring high-quality referral to the patient’s receiving team.
Acknowledgments
The authors thank Guts UK for the award of a grant to support the set-up and running costs of the Gastroenterology London Investigative Network for Trainees research network. We also thank Professor Anton Emmanuel for his support and supervision.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @GLINT_Research
Collaborators This work was undertaken by the Gastroenterology London Investigative Network for Trainees Research Network, which comprises Faisal Abbasi, Jane Abbot, Omer Ahmad, Ali Akram, Maria Aslam, Homira Ayubi, Jennifer Clough, Robin Dart, Angad Dhillon, Jonathan Digby-Bell, Robert Eckersley, Tareq El Menabawey, Jemima Finkel, Rishi Fofaria, Radha Gadhok, Shraddha Gulati, Richard Hackett, Joy Harris-Folb, George Hiner, Hein Htet, Sunjae Hwang, Nishani Jayasoorina, Misha Kabir, Rawen Kader, Jonathan King, Teo Lopez Bernal, James Maurice, Susanna Meade, Sam Pannick, Mihir Patel, Raj Patel, Polychronis Pavlidis, Sam Powles, Rebecca Preedy, Rohit Rao, Srivasthan Ravindran, Mark Samaan, Gregory Sebepos-Rogers, Jonathan Segal, Mentaj Sehmbhi, Chehkuan Tai, Holly Theaker, Zohib Tariq, Hannah Walton and Allan Xu.
Contributors OFA, HA, JC, RD, RG, SP, PP, JS and PS have all reviewed the literature and prepared the manuscript. All have written and contributed to critical revisions of the manuscript and are listed in alphabetical order according to surname. GP provided senior review and supervision. All Gastroenterology London Investigative Network for Trainees contributors collected the data.
Funding Ths study was funded by Guts UK (grant number RE15696).
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.