Article Text

Abstract
This prospective service evaluation aimed to determine if integrated psychological support for patients with inflammatory bowel disease (IBD) enhanced outcomes. 75 patients were assessed and treated by a specialist liaison psychiatric service between 2015 and 2017; 43 received psychiatric intervention alone, 32 were referred for psychological intervention by clinical health psychologist; 26 completed this. Pre–post data (n=15 available) included global impression, quality of life, and psychiatric and IBD symptom scores. Referrer/patient satisfaction and cost-effectiveness were retrospectively calculated. Psychological intervention led to reductions in IBD symptoms (ΔSIBD; p=0.003), alongside improvements in depression scores (ΔPHQ-9, p=0.006) and global impression (ΔCGI; p=0.046). Patient/referrer satisfaction was very high. Indicative data comparing service utilisation 1 year before and after engagement found reductions in outpatient appointments and in imaging. This small study suggests consideration of increased access to integrated psychological support services to improve outcomes and gather further evidence of efficacy.
- inflammatory bowel disease
- psychology
- health service research
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Inflammatory bowel disease (IBD) is a lifelong condition. Estimated annual incidence in Europe is 24.3 and 12.7 per 100 000 person-years for ulcerative colitis and Crohn’s disease, respectively. It can occur at any age, but is more common in younger people. Education, work, social and family life can all be disrupted by the unpredictable nature of debilitating and embarrassing symptoms. There is no ‘complete’ cure for IBD and many patients are on medications with unpleasant side effects, yet despite this end up needing invasive surgery with considerable impact on quality of life. Comorbid mood disorder can affect quality of life in patients with IBD.1 Unsurprisingly, patients with IBD are twice as likely to suffer from depression and are also more likely to have an anxiety disorder than other people.2 IBD standards have previously stated that a psychologist or counsellor is among the ‘essential supporting services’ that the IBD team should have access to.3 Furthermore, this has been identified locally at a trust level by the IBD Patient Panel as an area of priority need. Despite this, growing evidence suggests that psychological stress can increase activity of IBD.4 However, there is insufficient access to psychological support services for patients with IBD in the UK. Current evidence demonstrates that psychological therapies improve quality of life in the short term and supports the efficacy of antidepressant medication in improving disease activity.
The aim of this pilot service (named Psychological Support Service for Patients with Inflammatory Bowel Disease (PSSPIBD)) was to introduce integrated multidisciplinary psychiatric and psychological support for patients with IBD. It was hoped that by providing high-quality mental health support, we would improve patients’ psychological wellbeing, how they interact with services (by reducing inappropriate service use) and their quality of life. This service evaluation assessed the key assumption that providing tailored psychological support to patients with IBD will result in improved outcome measures across a ‘balanced scorecard’ of four dimensions: clinical effectiveness, cost-effectiveness, patient satisfaction and referrer satisfaction. Thus, it was our aim to demonstrate
Clinical effectiveness prospectively using validated questionnaires pre–post specialist psychological intervention
Cost-effectiveness retrospectively by indicatively evaluating service use prior to and after engagement with the service (PSSPIBD)
Patient satisfaction by the use of qualitative feedback.
Referrer satisfaction by the use of qualitative feedback.
Methods and participants
A digestive disease centre at a teaching hospital secured funding to pilot a PSSPIBD, to provide outpatient psychiatric and psychological support to patients with IBD. Between October 2015 and March 2017, 75 patients were assessed and treated by PSSPIBD, staffed by a liaison psychiatrist (0.1WTE) and a band 7 clinical health psychologist (0.3WTE) with special interests in IBD, enhanced by a shadowing period spent within the centre. Referrals were made for patients experiencing psychological difficulties related to their IBD by medical staff IBD nurses, pharmacists and stoma nurses; either by letter or discussion with the liaison psychiatrist in the weekly IBD multidisciplinary meeting. The service was open to all patients with IBD using the centre for management of IBD.
All patients referred were seen for an initial assessment unless they were already under the care of secondary mental health services.
The most common reason for referral into the service was support adjusting to IBD and its symptoms (eg, pain, fatigue, incontinence, tolerating uncertainty) (39%), followed by anxiety (31%) and low mood (8%) (figure 1A). Seventy-one per cent of patients seen were women.
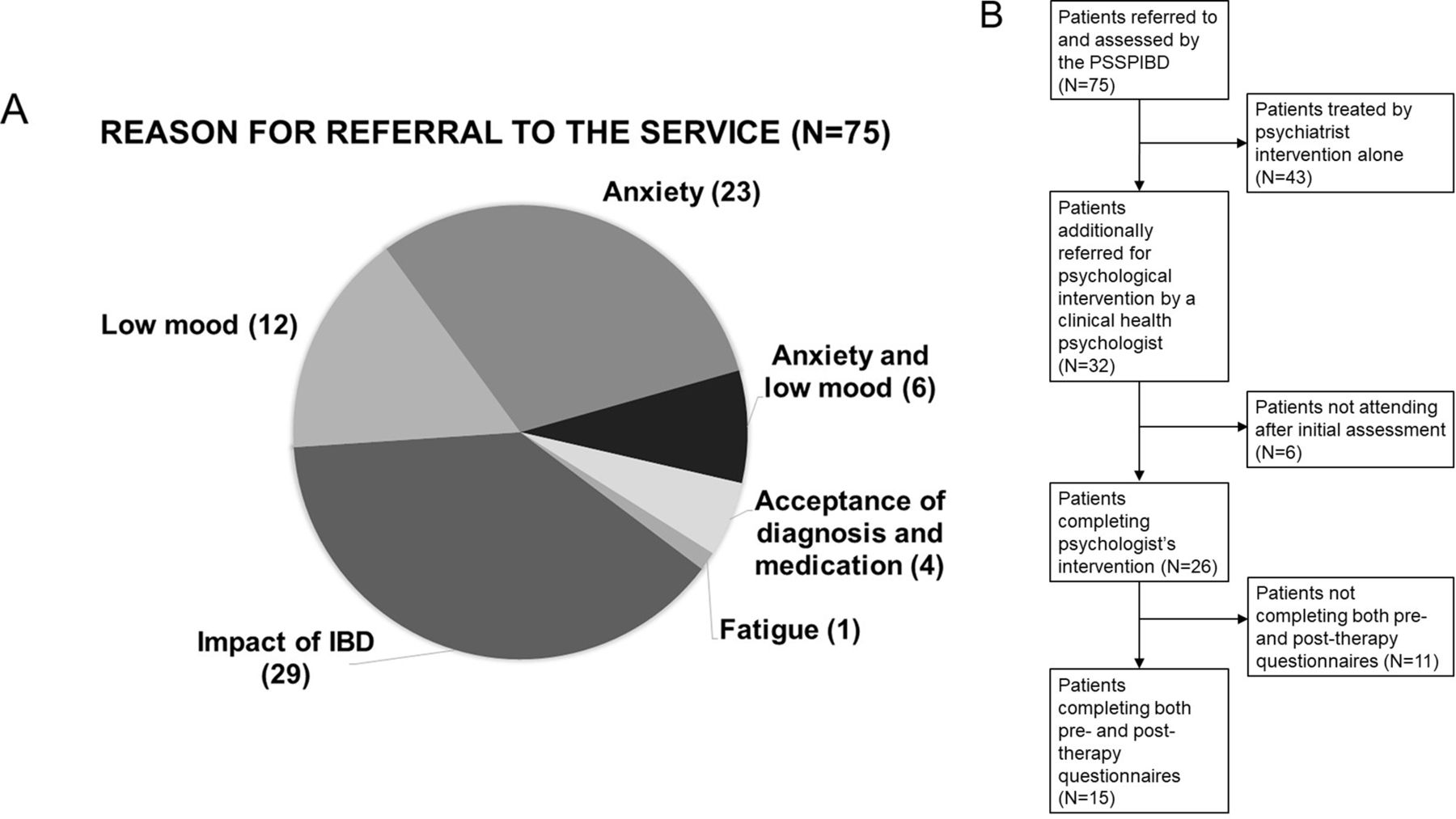
Reasons for referral into the service (1A), patient flow diagram (1B). PSSPIBD, Psychological Support Service for Patients with Inflammatory Bowel Disease.
A subgroup (n=15) of the service had complete questionnaire measurements before and after receiving psychological intervention by a clinical health psychologist. Cognitive-behavioural therapy (CBT) was offered to support a range of difficulties, including lifting low mood, tolerating uncertainty, overcoming phobias and pain management. On average, patients received five sessions of CBT, although in practice this ranges from 1 session to 11 sessions. Validated questionnaires collected prospectively measured quality of life (EUROQoL), depression (Patient Health Questionnaire, PHQ-9), anxiety (GAD-7) and IBD symptoms (SIBD). In addition, clinicians rated patients globally (Clinical Global Impression, CGI).
Given the small numbers, analysis of effectiveness of intervention of therapy (clinical and cost) was conducted by a related samples Wilcoxon signed-rank test in SPSS V.25 for Mac. Change in outcome scales were correlated using Spearman correlation. Cost-effectiveness was determined by indicative data comparing service use in 1 year before and after engaging with the PSSPIBD from one clinician using the service (MAS). This explored inpatient stays, emergency department attendance, radiological imaging, endoscopy and outpatient appointments pre–post. For statistical tests, a significance level of p≤0.05 was used. Patient and referrer feedback were assessed by invited questionnaire to all patients and referrers.
Results
Figure 1B explains the flow of patients assessed and treated by the service.
Clinical effectiveness
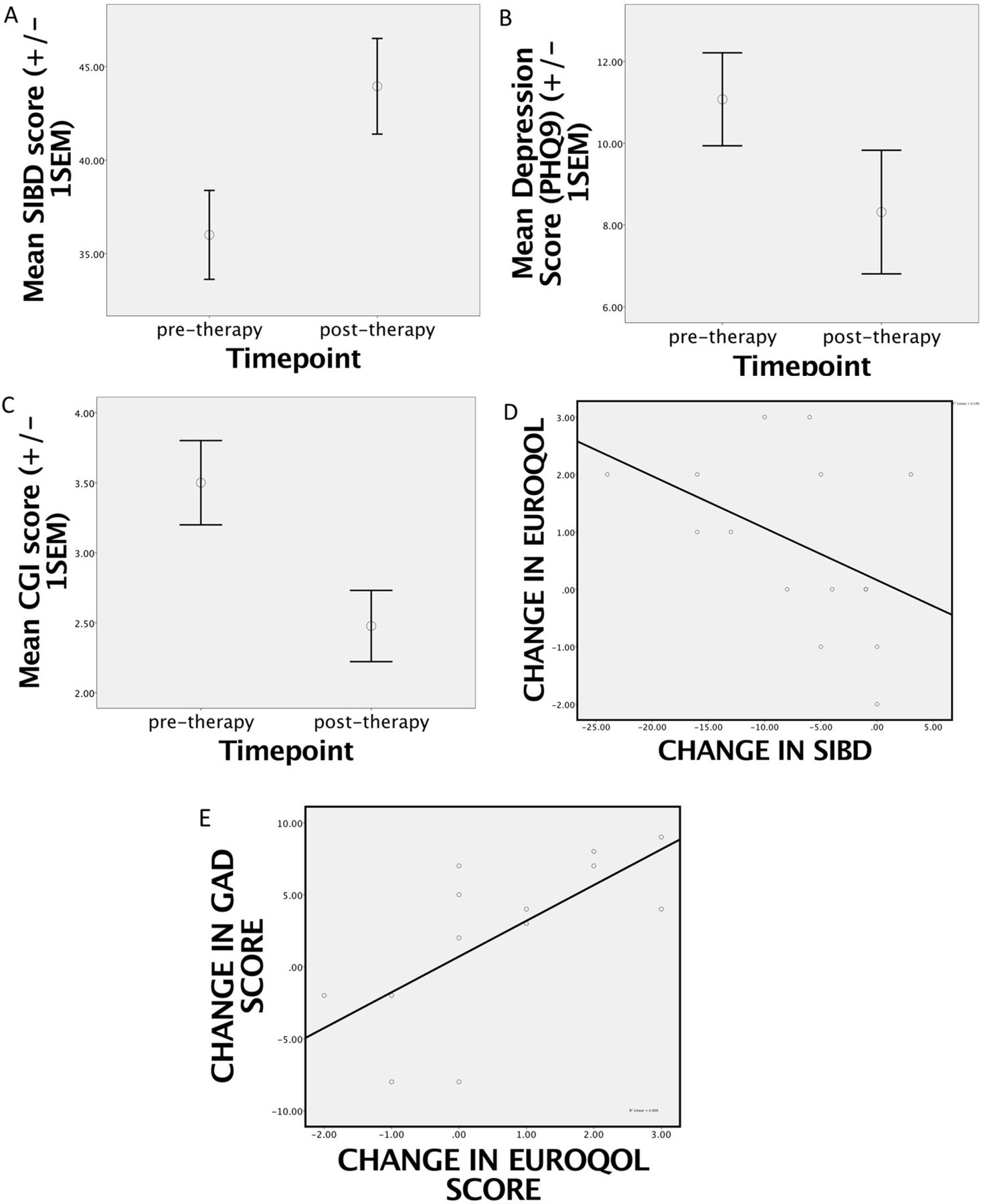
Short IBD Questionnaire (SIBD) scores pre-psychological and post-psychological therapy showed significant reductions in symptoms across all domains (p=0.003) with notable trend to improvement in bowel (p=0.067) and systemic symptoms (p=0.085) and significant improvements in emotional (p=0.004) and social functioning (p=0.046). Statistically significant improvements were seen in PHQ-9 depression score (p=0.006) and CGI (p=0.046), and there was a trend towards improvement in quality of life (EuroQoL) (p=0.058) (figure 2A–E).

Clinical effectiveness: statistically significant changes in patient outcomes post therapy: 1A mean SIBD (IBD symptoms) score (±1 SEM), 1B mean PHQ-9 (depression) score (±1 SEM) and 1C mean clinical global improvement (±1 SEM). Positive correlations 1D between improvement in quality of life and improvement in bowel symptoms and positive correlation 1E between reduction in anxiety and improvement in quality of life.
Reduction in anxiety correlated with improvement in quality of life (r, 0.728 p=0.005) (figure 2E). There was a trend towards improvement in quality of life correlating with change in IBD symptoms (r, 0.502, p=0.056) (figure 2D).
Service utilisation
Indicative data comparing service use in 1 year before and after engaging with PSSPIBD found a statistically significantly reduction in outpatient appointments by 62.5% (p=0.010) and a strong trend in reduction of CT and MRI scans by 76.2% (p=0.058). No significant differences were found for inpatient bed days, emergency visits or endoscopy visits.
Patient and referrer satisfaction
Patient and referrer satisfaction with the service were very high: 90% of patients and all referrers completing the feedback rated the service as excellent (figure 3A,B).
{kind=link}
{kind=link}
{kind=link}
Patient (A) and referrer (B) satisfaction with the service.
Discussion
The pilot service demonstrated significant improvements across all symptoms domains in patients with IBD, notably IBD and psychiatric symptomatology. This improvement is arguably comparable with that found with use of biologic agents.5 We demonstrated potential cost-effectiveness and high patient and referrer satisfaction.
Our findings are in keeping with the literature that demonstrates a high degree of psychiatric and psychological morbidity in patients with IBD. Sadly, only a low proportion of patients with IBD have access to specialist psychiatric consultation and psychological therapy, with reasons being stigma of receiving a mental health service, lack of expertise and training in psychological assessment for many practitioners, and commissioning structures separating physical and mental health outcomes. To date, only three long-term conditions have an established evidence base of psychological need and care and psychological service innovations to meet such need: diabetes, chronic obstructive pulmonary disease and coronary heart disease. It is anticipated as the evidence for psychological need and psychological effectiveness with patients with IBD grows, so too will the financial investment.
Limitations
The major limitation to this study is the small numbers and missing data. This is a problem with conducting rigorous service evaluation in a busy unit without dedicated research infrastructure support. There is a possibility of referral bias.
In terms of bias, those patients with the most regular contact with the IBD team were perhaps more likely to be referred. This group will contain those who had more active IBD, but also those with health-related anxiety and potentially medically unexplained symptoms. We do not feel that this in any way invalidates the results as these are exactly the patients that we wanted to reach with this service and which other units would want to see results for.
We believe there should be increased access to specialist integrated psychological support services across gastroenterology with the aim of gathering further evidence of success across all domains.
Footnotes
Twitter @bendybsms
Presented at This study has previously been presented as a poster at the 13th Congress of ECCO (European Crohn’s and Colitis Organisation)—Inflammatory Bowel Diseases 2018, Vienna (Austria), 14–17 February 2018, and as an oral communication at the British Society of Gastroenterology Annual Meeting 2018, Liverpool (UK), 4–7 June 2018, where it was selected as the Frontline Gastroenterology prizewinner for best patient benefit in gastroenterology.
Contributors JG set up the service with contribution from LAP and MAS. JAE, JG and AL collected the data. JAE contributed to the design, acquisition, analysis and interpretation of data, drafted the final manuscript and is the manuscript’s guarantor. EH, ASJ, RM, AA, LAP, MAS and JG contributed to the interpretation of the data, and contributed to drafting the final manuscript. All authors provided final approval of the final version.
Funding JAE is supported by the National Institute of Health Research (CL-2015-27-002). This service evaluation was conducted at the Digestive Diseases Centre at Brighton and Sussex University Hospitals NHS Trust. The Centre received a grant from Abbvie which supported the salary of AL. Abbvie had no influence over the design or interpretation of the service evaluation.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon request
Linked Articles
- UpFront