Article Text

Abstract
Objective To determine the impact to date of the ongoing Crohn’s & Colitis UK inflammatory bowel disease (IBD) clinical nurse specialists (CNS) campaign.
Methods A survey-based design was used. 2 questionnaires were sent to the UK IBD nursing community and promoted via nursing and clinical networks. Respondents were asked to provide data at both an individual and trust level about their nursing services.
Results 394 IBD CNS posts were identified across the UK, with a 32% increase in posts since the start of the campaign. 27% felt the campaign had been influential in securing new posts. Greater numbers of posts were reported in England when compared with the devolved nations. Most services remain below the UK standards recommendation of 2.5 IBD CNS per 250 000 patient population. Cross site working was reported in 59% of services. 45% of respondents were non-medical prescribers, with 13% educated to MSc level. High levels of stress were reported by IBD CNS associated with managing advice line services.
Conclusions Crohn’s & Colitis UK’s ‘More IBD Nurses–Better Care’ campaign has contributed to the numbers of CNS posts in IBD continuing to rise, but they remain lower than the recommended standard of 2.5 IBD CNS per 250 000. Educational and career pathways are not clearly defined, and aspects of the role such as advice line provision contribute to stress within the workforce. The ongoing aims of the charity campaign hope to address these issues by improving access to formal education pathways with peer support for IBD specialist nurses, and advice line training, in addition to supporting trusts and services throughout the UK to reduce the workforce deficit with effective business cases.
- inflammatory bowel disease
- crohn's disease
- ulcerative colitis
Data availability statement
Data are available upon reasonable request. Further access to data submitted for this paper can be accessed on request.
Statistics from Altmetric.com
Significance of this study
What is already known on this subject
Inflammatory bowel disease (IBD) clinical nurse specialist (CNS) posts within secondary care provide education, access, continuity and support for people living with Crohn’s disease and ulcerative colitis. Numbers of IBD CNS posts are less than the UK recommended standard of 2.5 whole time equivalent (WTE), and many patients report not having access to an IBD CNS
What this study adds
This paper reports on the results of a UK wide survey looking at IBD CNS workforce, demonstrating an increase of 32% in posts since the launch of the ‘More IBD Nurses–Better Care’ campaign was launched by Crohn’s & Colitis UK in 2016. IBD CNS roles are becoming more complex, with higher numbers of nurse prescribers and cross site working. Overall, IBD CNS numbers remain below the 2.5 WTE recommendations.
How might it impact on clinical practice in the foreseeable future
With IBD CNS numbers increasing and becoming more complex in nature, there is a need to ensure access to appropriate training and support for those IBD CNSs currently in post, and any future nurses. More work remains to be done to meet the UK national standards for workforce numbers, and the charity’s aim of >95% of their supporters reporting access to an IBD CNS.
Background
An estimated 500 000 people in the UK live with inflammatory bowel diseases (IBD) with numbers affected rising.1 Often diagnosed younger in age, these conditions are lifelong, relapsing and remitting and cost the National Health Service (NHS) in the region of £1 billion annually.2
IBD (IBD) clinical specialist nurses (CNS) are an essential part of an IBD service, where their role includes provision of cost-effective patient education, disease management and therapy monitoring, patient support, continuity of care, audit and rapid access for advice and review during disease flares.3 They lead patient centred service redesign, support research activity, improve quality of care and represent value for money.4–7
Patients report greater satisfaction of care with an IBD CNS in their team, citing improved access to better coordinated care, and better education and support for them and their families/carers.7 In addition, services with IBD CNSs as part of their core multi-disciplinary team (MDT) have been shown to have fewer hospital admissions, better access to self-management approaches for disease control, and greater choice regarding delivery of follow-up care for patients.5–7
Crohn’s & Colitis UK is the leading national charity for people living with Crohn’s and Colitis, working to improve diagnosis and treatment, and to fund research into a cure; to raise awareness and to give people with the conditions hope, comfort and confidence to live freer, fuller lives. In 2016, they launched the ‘More IBD Nurses–Better Care’ campaign to increase IBD CNS posts across the UK, aiming for at least 95% of their membership to be able report contact with a named IBD CNS at their hospital.8
Previous surveys of IBD CNS numbers in the UK published by the Royal College of Nursing (RCN) in 20129 and Crohn’s & Colitis UK in 2016 informed the campaign. These demonstrated higher numbers of posts in England (80%) than in the devolved nations, and only 16% of services UK wide meeting the then minimum national standards for IBD nursing numbers of 1.5 WTE per 250 000 patient population. 29 vacant IBD CNS posts were identified, with 8 (4.7%) services reporting difficulties in recruiting suitably trained and experienced nurses into these posts.8
Between 2016 and 2019, the campaign focused on raising awareness of IBD as a speciality within nursing, identifying current nurses in post and supporting them to better promote their roles, and analysing workforce data, as summarised in table 1.
Summary of Crohn’s & Colitis UK ‘More IBD Nurses–Better Care’ campaign activities 2016–2019
This paper outlines results from surveys conducted by Crohn’s & Colitis UK to measure the impact of their ‘More IBD Nurses–Better Care’ campaign to date, with discussion around the implications of the results and planned next steps.
Methods
Two surveys, with content developed from the previous 2012 and 2016 audits, were sent out by Crohn’s & Colitis UK using SurveyMonkey Audience (www.surveymonkey.com/mp/audience) at the end of 2018 to IBD CNSs throughout the UK, using the charities database to identify contacts.
Survey one: asked for workforce data from IBD nursing services at individual trusts across the UK, focusing on numbers of nurse posts, and whether this establishment has increased or decreased since the start of the ‘More IBD Nurses–Better Care’ campaign in 2016. One nurse per trust was asked to provide this data. (see online supplementary data for questions included).
Supplemental material
Survey two: focused on individual nurses, concerned with pay scales, length of time in post, clinical responsibilities and service provision. (see online supplementary data for questions included).
All respondents to the 2016 audit of UK IBD nurses were contacted individually and sent links to the surveys, and both surveys were additionally promoted nationally via the RCN IBD Special Interest groups and through the secure IBD Nurses Facebook page to try and capture those nurses new in post since the previous audit.
Between December 2018 and May 2019, targeted reminders were sent, including direct calls and emails where possible, and the survey was publicised and promoted at appropriate meetings and within the nursing press to try and increase return rates.
Where 2019 data regarding workforce was not submitted by a service (survey non-response), the most up to date workforce data available from the 2016 survey results was used to calculate overall numbers of nursing posts.
Results
Two hundred and seventy-four individual responses were received from individual nurses from 149 trusts/sites across the UK.
Service data
One hundred and forty-nine services submitted workforce data. Three hundred and ninety-four individual whole time equivalent (WTE) IBD CNS posts were identified across the UK in total, representing an increase in overall workforce since 2012 of 98%, with a 32% increase reported between 2016 and 2019.
39.6% (59/149) of services reported an increase in nursing establishment since 2016 (figure 1), of those that reported an increase, 27% felt the ‘More IBD Nurses–Better Care’ campaign from Crohn’s & Colitis UK had been influential in securing their new posts.
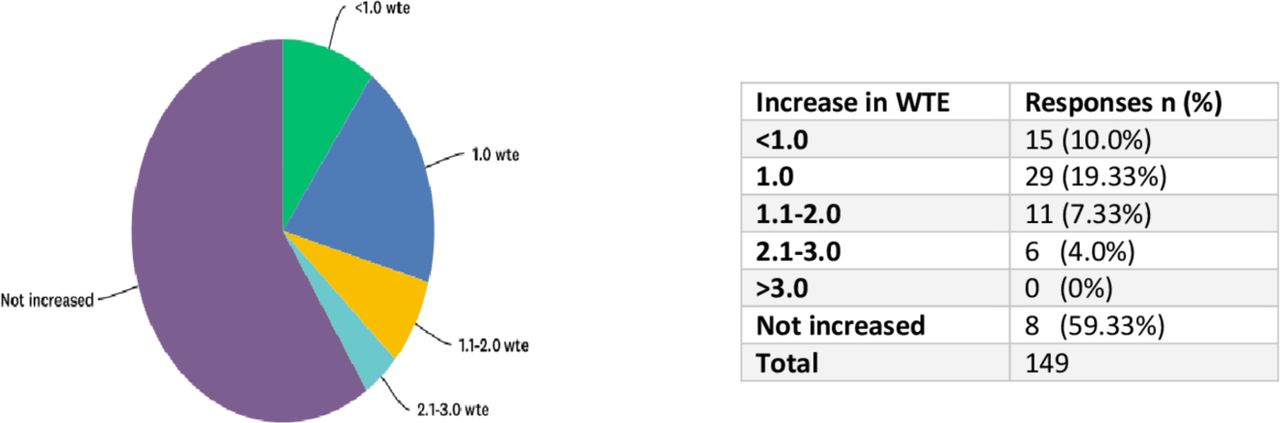
Increase in establishment by number of whole time equivalent (WTE) posts.
59% (88/149) IBD services provide nursing services over more than one site, with 10% (16/149) providing services over more than three sites.
Nursing establishment decreased in 6% (9/149) by at least 0.5 WTE, 14.7% (22/149) of services reported current vacancies with 6% (9/149) reporting problems recruiting to new posts. None of the respondents reported nursing establishments meeting the current minimum standard of 2.5 WTE/250 000 population recommendation from IBDUK.
Individual nurses
Two hundred and seventy-four (69.5%) nurses completed individual data.
Sixty two per cent (170/274) were working at Band 7, making this the most prevalent pay band. Banding ranged from Band 6 (28%) to Band 8 c (1.82%).
Fifty six per cent (153/274) of respondents had been in post for less than 5 years.
Seventy per cent work solely within the specialty of IBD, however, 28% describe other clinical responsibilities within their role, including more general gastroenterology, nurse endoscopy, ward working and research.
Forty five per cent (122/274) have a non-medical prescribing qualification, with 13% (35/274) educated to MSc level.
Advice line/patient access
Ninety eight per cent (269/274) of IBD CNS deliver or manage advice line access for patients as part of their service. Of these, 10% (28/269) felt they had received formal training in advice line provision. Thirty two per cent (87/274) receive regular supervision or support for this aspect of their role. A simple rating scale was used to self-report levels of stress as perceived by individual respondents. Seventy five per cent rated stress levels associated with advice line provision as >8 (0–10 with 10 most stressful).
Thirty two per cent of advice line services were reduced or suspended entirely in the IBD CNS absence.
Managing biologic therapy pathways
The roles of IBD CNSs within the prescribing, delivery and management of biological therapies, including anti-tumour necrosis factor alpha(TNFa), vedolizumab and ustekinumab are summarised in figure 2, and include identification, counselling, independent prescribing and monitoring of patients on biological therapies as well as negotiating with funding providers to access treatment.

Nursing roles in management of biological therapies in inflammatory bowel disease.
Sixty eight of 149 (45%) services currently run regular virtual biologic review clinics.
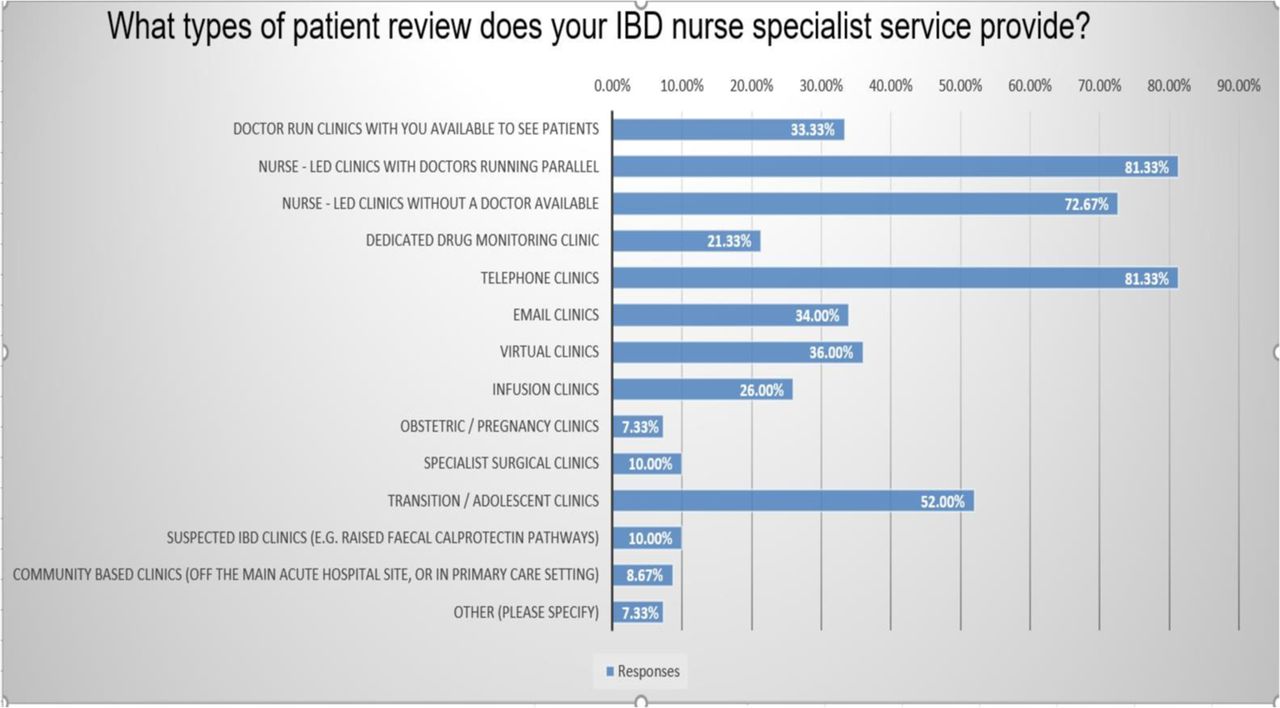
Outpatient work
Methods of clinical review undertaken by IBD CNSs within the outpatient setting are summarised in figure 3 and include both face to face and telephone review.

{kind=link}
{kind=link}
{kind=link}
Outpatient work undertaken by IBD CNSs.
Ten per cent (15/274) regularly see people with suspected IBD prior to diagnosis, 8% (13/274) review patients in a community setting.
Thirty five per cent (97/274) of CNS services have access to dedicated administrative support, of those, 36% (35/97) stated their administration establishment had increased in the last 2 years.
Discussion
Specialist IBD nursing posts continue to increase throughout the UK, with a 32% increase since the start of the Crohn’s & Colitis UK ‘More IBD Nurses–Better Care’ campaign in 2016. There is an increase in nurses working solely within IBD, rather than in more general gastroenterology posts, with roles themselves becoming ever more complex in nature as demonstrated by the numbers of non-medical prescribers increasing, and cross site working. Notably, the IBD CNS workforce itself remains relatively junior, with significant variations in experience and qualifications reported.
The IBD CNS workforce remains significantly under the IBDUK 2019 Standards recommendation. The rate of increase in posts continues to be slower within the devolved nations. Across all four UK countries, and within both adult and paediatric services, there is a need to continue to work towards meeting the recommended minimum number of 2.5 full time IBD CNSs per 250 000 population, with a maximum of 500 patients per full time nurse.1
Feedback from both our survey and within the IBD community itself has been positive toward the impact of the ‘More IBD Nurses, better care’ campaign, with use of online resources developed to assist in business case planning and of the Facebook peer support and networking opportunities. The Crohn’s & Colitis UK ‘Find an IBD Nurse Map’ resource demonstrates good coverage nationally, and continues to be accessed regularly, both by patients and IBD services, averaging just over 2500 unique views per quarter.
Nurse Specialist roles in general remain unregulated and somewhat unstructured throughout the NHS. Lack of development and training opportunities have been recently cited in a workforce report by Macmillan Cancer CNSs as a reason for nurses leaving the both the specialty and profession owing to lack of structure and support leading to increased levels of stress and lower job satisfaction.10 Health Education England recommend that nurses working at an advanced level of practice should hold a minimum of an MSc in advanced practice.11 The number of nurses currently working within IBD CNS nursing posts that meet this standard remains low. Cost and lack of time are often cited by nurses as barriers to undertaking study and this needs to be addressed if we are to develop a workforce which offers comparable standards of care to patients with IBD wherever they live in the UK, as recommended by the 2019 IBD Standards.1 A clearly defined career pathway for all grades of nurses working within IBD care, with sufficient resourcing for all IBD CNSs to work towards Masters level nursing qualifications is essential to retain high calibre nurses and encourage more nurses into the specialty.
In 2019, Crohn’s & Colitis UK launched their Crohn’s & Colitis UK Specialist Nurse Programme to bring together a community of IBD CNSs under a clearly defined pathway. The programme includes funding for completion of an MSc in advanced clinical practice or RCN advanced nursing practice credentialing.
While recognised as of great importance and benefit to both individuals living with Crohn’s and Colitis, and IBD services, advice lines have been identified by many IBD CNSs as a source of stress and anxiety due to ‘unseen workload’ and increasing numbers of contact.12–14
Explanations for the increasing stress levels associated with advice line provision include lack of dedicated time within job plans and clarity as to the purpose of the service, resulting in potentially unrealistic expectations about what the advice line can deliver.
Crohn’s & Colitis UK have developed advice line training programmes, free at the point of delivery, for all IBD CNSs, commenced in January 2020. Content includes development of locally agreed protocols and pathways for advice line management in addition to training in call management and self-care which aim to reduce the levels of stress and anxiety around advice line delivery.
There are several limitations to our study. With no formal register of IBD CNSs, we are unable to be completely sure we are accurately reporting numbers of IBD CNS posts. Due to differences in the data collection methods between the 2016 and 2019 surveys, direct comparisons in data was not possible, this has been mitigated for by the authors reviewing the data and seeking confirmation and clarification from centres on WTE numbers wherever possible. Further, there is currently no single incontrovertible figure for numbers of people living with IBD that conflate primary and secondary care datasets. This is compounded by the fact that ‘IBD’ is not consistently recorded by MDTs on datasets as patients may be categorised under other co-morbidities. Thus, the level of ‘need’ may be grossly underestimated which may in part explain why when nurses make IBD more accessible by offering advice lines, ‘real need’ emerges contributing to high levels of stress. This requires further research and investigation to understand how IBD nurses can be better supported by NHS managers.
As IBD treatments and management pathways become increasingly complex and strategic, incorporating management of high cost therapies, cross site working and new ways of working, it is essential that appropriate and comparable training and support is available for IBD nurses practising at a specialist level throughout the UK. There is emerging evidence that innovative ways of working such as the introduction of remote surveillance through IBD advice lines can be cost effective and resource efficient for the NHS as well as improving patient outcomes. However, this needs to run hand in hand with NHS managers improving data collection to record ‘need’ and supporting IBD nurses with high volumes of workload to ensure levels of stress do not continue to escalate leading to burn out, nurses leaving the profession and deepening the current workforce crisis in the NHS.
Conclusion
Our surveys demonstrate the positive impact of the Crohn’s & Colitis UK ‘More IBD Nurses–Better Care’ campaign to date with an increase in numbers of IBD CNS posts reported over the last 3 years. National initiatives have been implemented to raise the profile of the specialty within the nursing community, and to support services seeking to increase their establishment of IBD CNSs posts.
Crohn’s & Colitis UK has committed to continuing to support the education and support of IBD CNSs and development of new posts where needed as part of their 5-year strategy for high quality clinical care. By doing so, it is hoped adequately resourced services meeting the recommended standard of 2.5 IBD CNS per 250 000 can be achieved nationally.
Data availability statement
Data are available upon reasonable request. Further access to data submitted for this paper can be accessed on request.
Acknowledgments
Sophie Basil, Press Officer, Crohn’s & Colitis UK for their support in preparing this manuscript.
Footnotes
Twitter @IBDUKTEAM
Contributors IM & RK developed the study. IM designed the surveys. LY & IM undertook the survey. LY analysed responses. LY, IM and RK drafted the paper. SB assisted with formatting tables and graphs.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- UpFront