Article Text

Abstract
Thiopurines are proven agents in the treatment of Crohn’s disease. While pancreatitis is recognised as an adverse event associated with therapy, the effect size and morbidity of thiopurine-induced pancreatitis is not known. The aim of this systematic review and meta-analysis was to quantify the risk of pancreatitis with azathioprine and 6-mercaptopurine (6-MP) within Crohn’s disease. We searched six electronic databases from inception to 29 October 2019. The primary outcomes measures were the occurrence of pancreatitis. We calculated pooled OR with corresponding 95% CIs for risk of pancreatitis. A number needed to harm analysis was performed. The search identified 4418 studies, of which 25 randomised controlled trials met the criteria for inclusion. The number of patients treated with azathioprine to cause an episode of pancreatitis was 36 (induction of remission) and 31 (maintenance of remission).The risk of pancreatitis in patients receiving azathioprine across all contexts was 3.80%, compared with a control risk of 0.2% (placebo) and 0.5% (5-aminosalicylic acid agents). There was no difference seen between 6-MP and placebo, although this was a low certainty result due to imprecision from very low event numbers and patient numbers. There is a probably increased occurrence of pancreatitis when azathioprine is used in Crohn’s disease (moderate certainty), with incidence overall approximately 3.8%. Most cases are mild and resolve on cessation of therapy and no mortality was reported. There was no increased occurrence seen when using 6-MP, although this is a low certainty finding. PROSPERO prior to the study (CRD42019138065).
- 5-aminosalicylic acid (5-ASA)
- crohn's disease
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Corticosteroids, representing the mainstay of induction treatment for moderate-to-severe Crohn’s disease (CD), are inappropriate long-term agents in the maintenance of remission due to their adverse effect profile.1 Furthermore, corticosteroid dependency following induction with steroids in patients with CD occurs frequency. Population-based studies evaluating the natural history of steroid-treated CD identified that 28%–36% of patients are steroid dependent at 1 year, with a further 20%–22% labelled as steroid resistant.2 Corticosteroid dependency in patients with CD is a major clinical problem, in which immunomodulation therapy with purine analogue therapy represents standard practice for maintenance of remission.3 4 Azathioprine (AZA) and its metabolite 6-mercaptopurine (6-MP) are therapeutic agents with proven efficacy in this context for treating CD,5 6 through their ability to obstruct rapid cellular proliferation in lymphocyte differentiation, thus limiting inflammatory response.7
Well-recognised dose-dependent adverse events associated with AZA and 6-MP include myelosuppression and hepatotoxicity, which often resolve with dose reduction. These adverse events rarely necessitate termination of therapy.8 Idiosyncratic adverse drug reactions (ie, intractable nausea, malaise, fever without leucopenia, arthralgia and acute pancreatitis), while more common in frequency than dose-dependent reactions, often demand discontinuation of the offending medication.4
Pancreatitis has long been considered in the context of purine analogue use for CD. While the exact mechanism of AZA-induced pancreatitis remains unknown, the relationship appears to be dose-independent (idiosyncratic) with no correlation to myelosuppression, suggesting the aetiology is independent of thiopurine methyltransferase activity. A delayed type II or IV allergic reaction or immune-mediated genetic disposition has been postulated, with the former supported by the fact rechallenge of AZA results in recurrence of symptoms.9 Of interest, when AZA is used within other clinical settings, acute pancreatitis is seldom seen. AZA is not reported to induce pancreatitis when used in the context of renal transplantation, rheumatoid arthritis, autoimmune hepatitis, lupus erythematous, lupus nephritis or antineutrophil cytoplasmic antibodies (ANCA)-positive vasculitis.10–15
International guidelines recommend the fulfilment of two criteria from the following as diagnostic for acute pancreatitis: abdominal pain consistent with the diagnosis, serum lipase/amylase values exceeding three times the upper limit of normal, and radiological imaging of the abdomen consistent with pancreatitis.4 16 17
A large-prospective trial conducted in Denmark between 1977 and 1992 (n=15 526) identified the incidence of acute pancreatitis to be 4.3 times more frequent in those with CD, and 2.1 times more frequent in those with ulcerative colitis, as compared with healthy counterparts.18 Weersma et al reported an incidence of 4.9% in a retrospective review of 224 patients with CD,19 and more recently Teich et al prospectively detected a 8.9% incidence rate of pancreatitis in 338 Crohn’s patients.4
The natural course of AZA-induced pancreatitis is often mild,18 as was the case in all patients in both these recent studies, developing approximately 3–4 weeks after initiation of treatment.4 19 In general, the risk of repeat pancreatitis with thiopurine rechallenge or thiopurine switch is high; as such, rechallenge in the context of pancreatitis is not recommended and therefore occurrence of pancreatitis will necessitate permanent cessation of purine therapy. Tioguanine as an alternative to AZA and 6-mercaptopurine has been noted as successful in avoiding pancreatitis.20
In reviewing the clinical recommendations, as published by seven leading national and international expert groups, five recognise pancreatitis as a side effect of AZA and 6-MP,21–26 with two making no reference.27 28 None of the publications estimate the burden or attempt to quantify the effect size of thiopurine-induced pancreatitis and not all advise what to do after such an adverse event has occurred. While it is unequivocal thiopurines are associated with pancreatitis within the context of CD, an accurate estimation of the risk in different clinical scenarios is not known. The reported morbidity and mortality associated with such cases is also not clearly established.
The objective of this systematic review is to determine, based on the available randomised controlled trial (RCT) evidence, the risk of pancreatitis with thiopurines within CD across a number of common clinical situations within CD.
Methods
A systematic review, completed in-line with the Cochrane methodology and reported in-line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement is presented.29 30 The research protocol was registered with PROSPERO prior to the study (CRD42019138065).31
Criteria for considering studies for this review types of studies
RCTs were considered for inclusion.
Types of participants
Patients of any age with CD having therapy for induction or maintenance of remission were considered for inclusion.
Types of interventions
Studies that evaluated AZA or 6-MP in comparison to placebo, no intervention or any other pharmacological agent were eligible for inclusion. The study follow-up period was required to be at least 3 months.
Types of outcome measures
Primary outcomes
The primary outcome measure was the occurrence of pancreatitis, as defined by the reporting study. Explicit reference to the incidence of pancreatitis was not a prerequisite for inclusion within this review.
Secondary outcomes
Secondary outcomes included withdrawal of therapy due to pancreatitis and pancreatitis-related mortality.
Search methods for identification of studies
Electronic searching
We searched the following electronic databases from inception to 29 October 2019 for relevant studies: PubMed, MEDLINE, EMBASE, Cochrane Central Register of Controlled Trials, ClinicalTrials.gov and the WHO trial registry. The search strategy was not limited by language. The search strategy used for each database is reported in online supplementary appendix 1.
Supplemental material
Searching other resources
The references of all identified studies were scrutinised to identify further studies for inclusion.
Data collection and analysis
The abstracts identified from the searches were reviewed by two authors (CG-C and MG). If the reference appeared potentially relevant, a full copy of the study was obtained.
Selection of studies
Papers (or abstracts) that appeared to be potentially relevant were identified by two authors (CG-C and MG). The authors (CG-C and MG), after reading the full texts, independently assessed the eligibility of all trials identified using the inclusion criteria above. Disagreement among authors was discussed and agreement reached by consensus.
Data extraction and management
A data extraction template was developed to extract information on the characteristics and results of included studies. Two authors (CG-C and MG) independently extracted and recorded data. In situations where the study reports on adverse events associated with treatment but fails to report on the incidence of acute pancreatitis, then the incidence of pancreatitis was inferred to be zero.
Assessment of risk of bias in included studies
The methodological quality of the included studies was independently evaluated by two authors (CG-C and MG) using the Cochrane risk of bias tool.32 Disagreements were resolved by consensus. The overall quality of the evidence supporting the primary outcomes was evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach,32 which appraises the quality of a body of evidence based on the extent to which one can be confident that an estimate of effect or association reflects the item being assessed. The different quality ratings are interpreted as the likelihood that future research would change the effect estimate. The overall quality of the evidence for each outcome was determined after considering each of these factors and graded as high (further research unlikely to change confidence in the estimate of effect), moderate, low or very low (any estimate of effect is very uncertain).
Statistical analysis
The Cochrane Collaboration review manager (RevMan) software (V.5.3.5) was used for data analysis. We calculated the OR and corresponding 95% CI for dichotomous outcomes. We pooled studies for meta-analysis when treatment context and interventions were deemed to be sufficiently similar (as determined by consensus) using a random-effects model. An intention-to-treat analysis was performed, including all randomised patients in analysis. However, as the focus was on a specific adverse effect (pancreatitis), and trial governance would dictate the reporting of such serious adverse events, all drop-outs were not assumed to have withdrawn due to pancreatitis. The number needed to harm in relation to the primary outcome was calculated using the method as outlined in the Cochrane methodological handbook.33
When cross-over trials were included, data from the first phase of the study were extracted for analysis (ie, before the cross-over occurred), provided that the primary outcomes presented were delineated temporally between precross-over and postcross-over checkpoints. Separate analyses were conducted for comparisons between AZA or 6-MP versus placebo, and AZA or 6-MP versus individual active comparators (eg, infliximab, mesalazine and methotrexate).
Assessment of heterogeneity
Heterogeneity among trial results was assessed by visual inspection of forest plots and by calculating χ2 (a p<0.10 was regarded as statistically significant heterogeneity). The I2 statistic was calculated to quantify the effect of heterogeneity across studies. We conducted sensitivity analyses as appropriate to investigate heterogeneity. For example, if pooled analysis showed statistically significant heterogeneity and a visual inspection of the forest plot identified studies that may have contributed to this, then the analysis was repeated excluding these studies to see if this explained the heterogeneity.
Subgroup analysis
Subgroup analyses were performed to reflect the different clinical contexts in which thiopurines are used within the management of CD, in which three patient groups were identified as being clinically distinct, as determined through consensus. Group 1 includes non-surgical patients receiving treatment with thiopurines for the maintenance of remission in whom disease management was purely pharmacological. Group 2 includes patients with disease in remission at the onset of the trial following surgery for CD. Group 3 includes non-surgical patients receiving treatment with thiopurines for active CD, in whom disease management was pharmacological.
Results
Description of studies
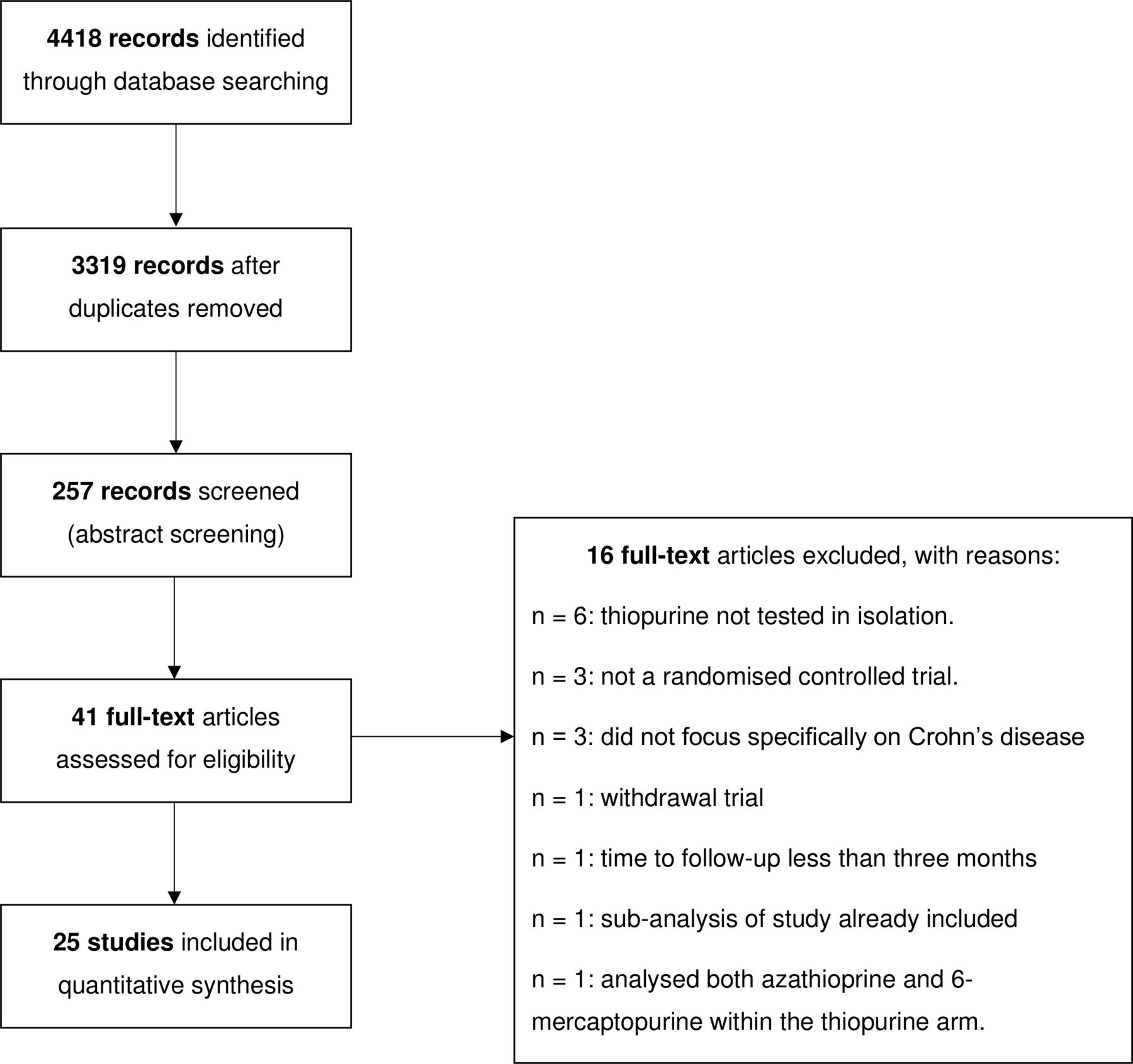
The results of the electronic search conducted on the 29 October 2019 are reported in the PRISMA flow diagram (figure 1). A total of 4418 studies were identified from the search. Following removal of duplicates, 3319 studies were screened, of which 257 proceeded to abstract screening. Of these, 41 studies were judged to be potentially relevant and subjected to full text review. A total of 25 studies were found to meet the inclusion criteria.34–58 Sixteen studies were excluded at the full-text review. Six studies failed to investigate a thiopurine in isolation.59–64 Three studies did not focus specifically on Crohn’s as a disease entity.65–67 Three studies failed to demonstrate randomised controlled study methodologies.68–70 A further four studies were excluded due to being a withdrawal trial, time to follow-up of less than 3 months, reporting a subanalysis of a study already meeting the inclusion criteria, and analysing both AZA and 6-MP within the thiopurine arm.71–74
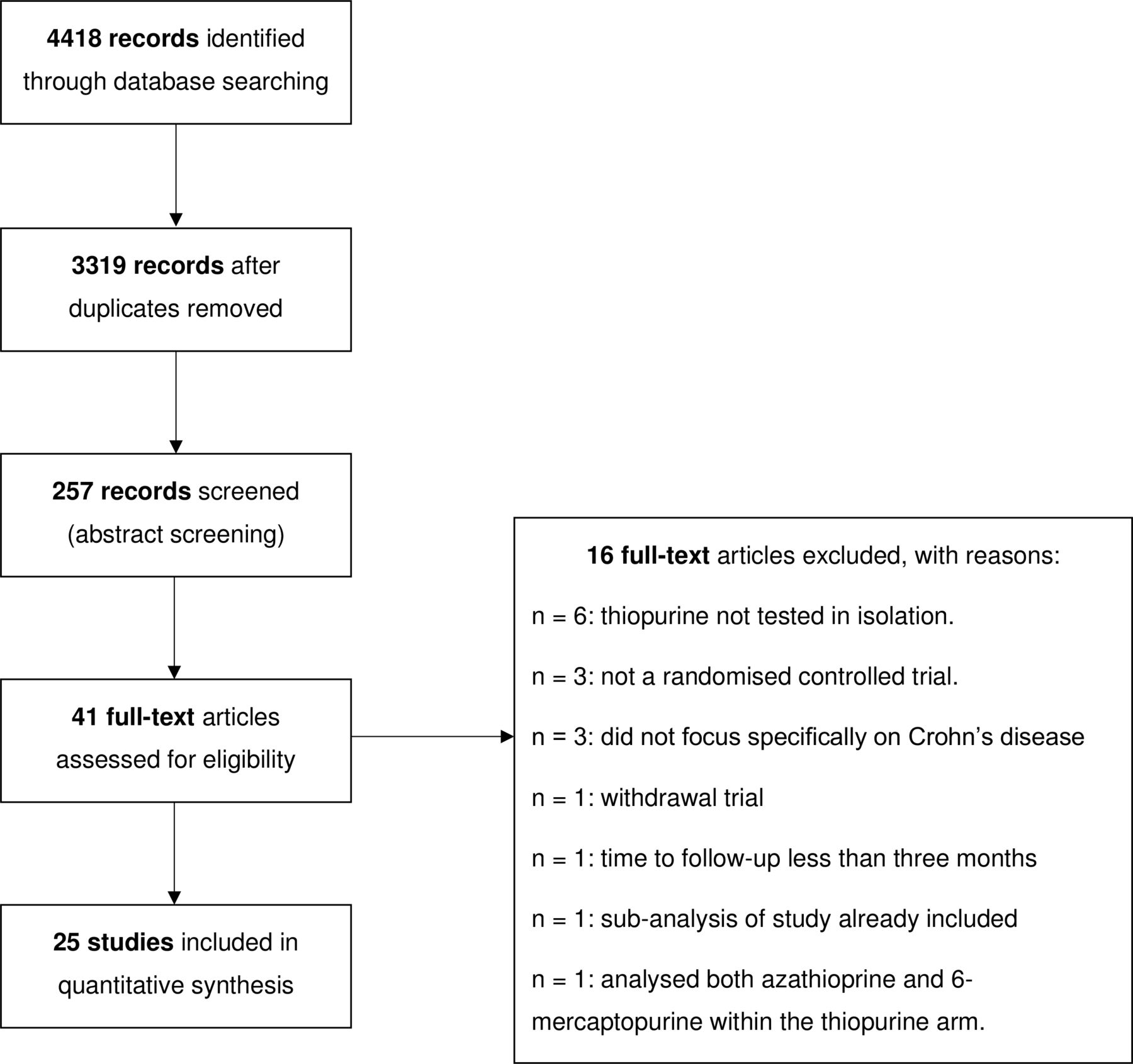
PRISMA study flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Twenty-one studies compared AZA to a comparator. Eleven studies compared AZA to placebo.34 35 38–42 44 50 52 56 Four studies compared AZA to mesalazine.43 46–48 Two studies compared AZA to infliximab.36 49 One study compared AZA to budesonide37; to adalimumab53 and to methotrexate.54 The study reported by Savarino included three intervention arms: AZA, mesalazine and adalimumab.57
Four studies compared 6-MP to a comparator. Three studies study compared 6-MP to placebo.51 55 58 The study reported by Hanauer et al compared 6-MP to both placebo and mesalazine in a three-armed trial.45
Across the 25 RCTs meeting the inclusion criteria, a total of 2399 participants were included (thiopurine arm=1151, comparator arm=1248). All but one trial included adult patients with CD, with only the trial reported by Markowitz focusing on a paediatric population (average age=13.2 years).55 Eleven studies focused on patients with active disease, and the aim of treatment was induction of remission, followed by maintenance of remission (nine AZA vs comparator studies; two 6-MP vs comparator studies).34 39 41 42 48–50 52 54 55 58 Seven studies focused on non-surgical patients in remission, and the aim of treatment was maintenance of remission (seven AZA vs comparator studies; zero 6-MP vs comparator studies).35 37 38 40–42 44 Nine studies focused on the maintenance of remission postsurgery (seven AZA vs comparator studies; two 6-MP vs comparator studies).35 36 43 45–47 51 53 57
Risk of bias
Details of the risk of bias assessment for each study are presented within the online supplementary materials. The risk of bias related to random sequence generation (selection bias) was deemed to be ‘low risk’ in 15 studies (60%) and ‘unclear risk’ in 10 studies (40%). The bias attributed to allocation concealment (selection bias) was classified as ‘low risk’ in 12 studies (48%) and ‘unclear risk’ in 13 studies (52%). Blinding of participants (performance bias) was deemed to be ‘low risk’ in 13 studies (52%), ‘unclear risk’ in three studies (12%) and ‘high risk’ in nine studies (36%). The reason for such ‘high risk’ classifications included failing to blind the participants and/or investigators to the intervention.35–37 43 48 53 54 56 57 Incomplete outcome data (attrition bias) was deemed to be ‘low risk’ in 22 studies (88%) and ‘unclear risk’ in three studies (12%). The bias attributed to selective reporting (reporting bias) was classified as ‘low risk’ in 23 studies (92%), ‘unclear risk’ in one study (4%) and ‘high risk’ in one study (4%). The study as reported by López-Sanromán et al was found to be at ‘high risk’ of reporting bias by failing to report on all outcomes as prespecified in trial protocol.53 In summary, 5 studies were assessed to be at a ‘low risk’ of bias,39 45 46 49 51 11 were ‘unclear risk’,34 38 40–42 44 47 50 52 55 58 and the remaining 9 were at a ‘high risk’ of bias.35–37 43 48 53 54 56 57
Supplemental material
Primary outcome: incidence of pancreatitis
Two of the 25 included studies provided a case definition of acute pancreatitis.39 41 Panés et al defined pancreatitis as ‘elevation of amylase and lipase levels and cross-sectional imaging consistent with the diagnosis’.39 Summers et al defined pancreatitis as ‘elevated serum amylase or lipase during an episode of abdominal pain’.41 The remaining 23 studies failed to provide a case definition of pancreatitis, even if pancreatitis was listed as a recorded adverse event of therapy. Eighteen studies (72%) explicitly state the incidence of pancreatitis within both treatment arms.34 35 37 39 41 43–45 47 48 51 52 54–58 Seven studies (28%) provide no reference to acute pancreatitis when reporting adverse events36 38 40 42 49 50 53; and did not respond to requests for further information. As such, the incidence was inferred to be zero episodes in all treatment arms (table 1) given the strict governance reporting requirements of such studies.
Thiopurine versus comparator. incidence of pancreatitis (main results)
Safety analysis
A summary of results for AZA versus comparator studies is presented in table 2 and summary of findings in table 3. Across all patient groups, those receiving AZA had 21 episodes of pancreatitis, compared with one episode occurring in the placebo group, which was a statistically significant finding (OR 8.92, 95% CI 2.61 to 30.54, p=0.0005; figure 2).
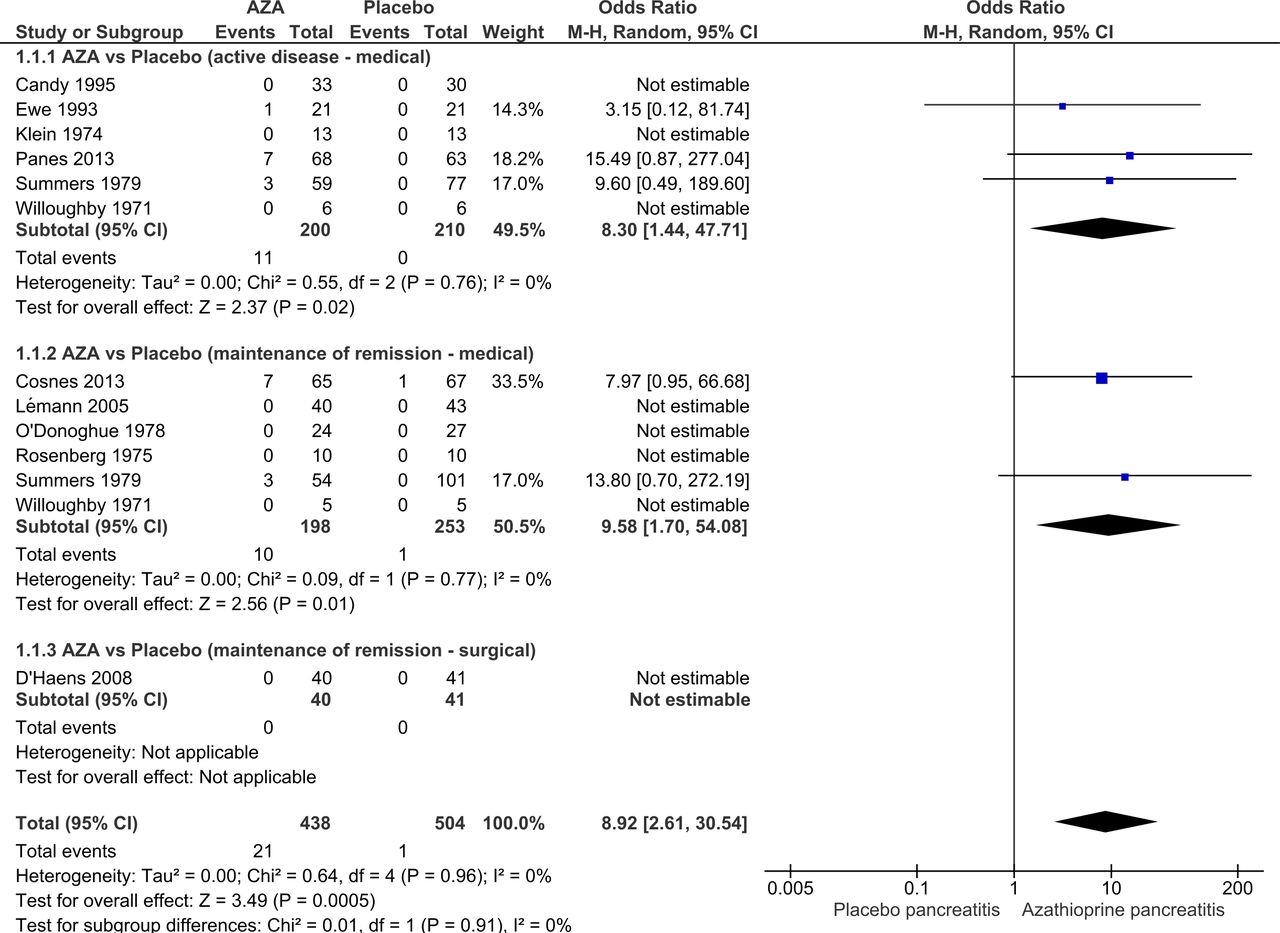
Forest plot—azathioprine versus placebo. AZA, azathioprine.
Azathioprine versus comparator
GRADE summary of findings
For patients receiving AZA for induction of remission, there were more cases of pancreatitis in those receiving AZA compared with placebo (OR 8.30, 95% CI 1.44 to 47.71, p=0.02, low certainty evidence downgraded one level due to sparsity of data and one level due to inconsistency due to the short treatment lengths for induction of remission, see tables 2 and 3 and figure 2). The number needed to harm was 32. For patients receiving AZA for maintenance of medically induced remission, there were more cases of pancreatitis in those receiving AZA compared with placebo (OR 9.58, 95% CI 1.70 to 54.08, p=0.01, moderate certainty evidence, downgraded one level due to sparsity of data, see tables 2 and 3 and figure 2). The number needed to harm was 36. There was only one study considering postsurgical maintenance with no cases of pancreatitis, so no effect estimate could be calculated (table 2).
When comparing AZA to 5-aminosalicylic acid (5-ASA) agents, across all patient groups, AZA resulted in 11 episodes of pancreatitis, compared with one episode occurring in the mesalazine group, which was not found to be statistically significant (OR 3.42, 95% CI 0.85 to 13.78, p=0.08, low certainty evidence, downgraded two levels for imprecision due to low patient numbers, low event numbers and inconsistency due to variability in CIs, see table 2 and figure 3). Similarly, AZA when compared with budesonide, infliximab, adalimumab and methotrexate, failed to demonstrate statistical significance in favour of increased incidences of AZA-induced pancreatitis. There were two episodes of pancreatitis with AZA compared with no episodes in the budesonide arm (OR 5.41, 95% CI 0.25 to 116.5, p=0.28, see table 2). There we no episodes of pancreatitis in either the AZA or infliximab treatment arms. One episode of pancreatitis was found with AZA in comparison to zero episodes in the adalimumab treatment arm (OR 3.00, 95% CI 0.11 to 79.13, p=0.51, see table 2). One episode of pancreatitis was found with AZA in comparison to zero episodes occurring with methotrexate treatment (OR 3.11, 95% CI 0.12 to 79.87, p=0.49, see table 2).
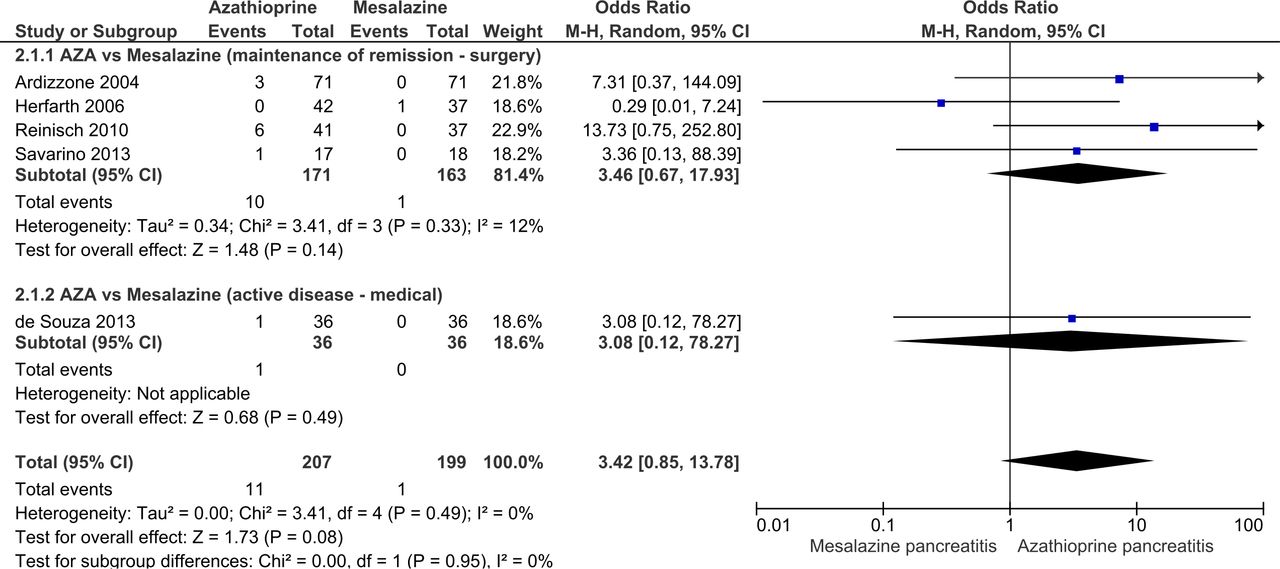
Forest plot—azathioprine versus mesalazine. AZA, azathioprine; M-H, Mantel-Haenszel.
Across all studies comparing AZA to comparator, there were 36 episodes of pancreatitis occurring in 947 participants receiving AZA (incidence 3.80%), in comparison to 2 episodes of pancreatitis occurring in 1010 participants receiving comparator treatment (incidence 0.20%). The number needed to harm was 27.8.
6-MP-induced pancreatitis
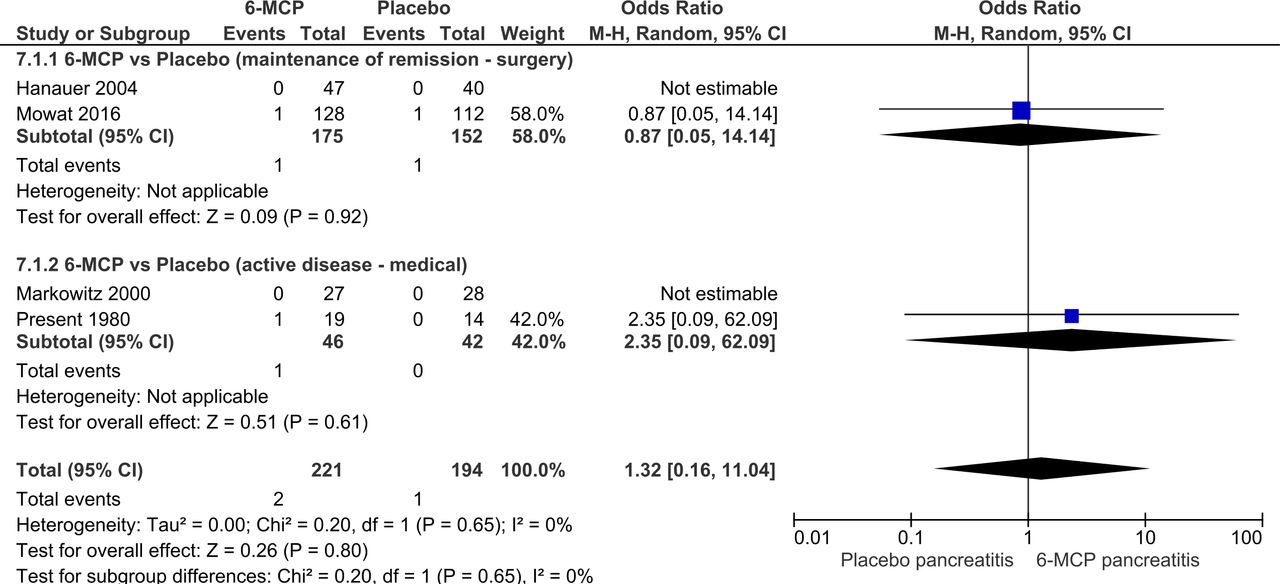
A summary of findings for 6-MP versus comparator studies is presented in table 4. Across all patient groups, there were two episodes of pancreatitis in participants receiving 6-MP, in comparison to one episode occurring in participants receiving placebo. This was not found to be statistically significant (OR 1.32, 95% CI 0.16 to 11.05, p=0.80, see table 4 and figure 4). Subgroup analysis did not show significance in patients with active disease treated medically (OR 2.35, 95% CI 0.09 to 62.09, p=0.61) or in patients in remission post-surgery (OR 0.87, 95% CI 0.05 to 14.14, p=0.92). There were no studies comparing 6-MP to comparator in the context of maintaining medically induced remission, thus no effect estimate could be calculated.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot—6-mercaptopurine (6-MCP) versus placebo. M-H, Mantel-Haenszel.
6-mercaptopurine versus comparator
Across all studies comparing 6-MP to comparator, there were two episodes of pancreatitis occurring in 268 participants (incidence 0.75%), in comparison to one episode of pancreatitis occurring in 238 participants receiving comparator treatment (incidence 0.42%). The number needed to harm was 303.
Secondary outcomes
Withdrawal of therapy due to pancreatitis
Across the 36 participants reported to have developed pancreatitis secondary to AZA use across all clinical contexts, 28 participants were withdrawn from the trial due to this event. In the trial reported by Cosnes et al, six of the seven cases of AZA-induced pancreatitis continued follow-up in their respective trials; however, treatment with AZA was stopped and the participants were commenced on methotrexate therapy.35 One of the six patients with AZA-induced pancreatitis reported by Summers continued AZA due to normalisation of abdominal pain and serum amylase levels.41 The patient with pancreatitis in the trial as reported by Ewe et al continued within the trial as he remained asymptomatic.52 The two participants with pancreatitis occurring in the comparator arms were withdrawn from the trials.35 46
In the two episodes of pancreatitis occurring in participants receiving treatment with 6-MP, only one participant reported by Mowat et al remained in the trial, despite developing ‘mild’ pancreatitis.51 The one comparator participants with pancreatitis was withdrawn from the trial.51
Pancreatitis-related mortality
There were no reported deaths as a result of thiopurine or comparator-induced pancreatitis across all included studies. Further details relating to the presentation, clinical course and sequelae of all 38 thiopurine-induced pancreatitis cases is presented in table 4.
Of note, only nine of the included 25 studies explicitly state in the research methodologies that lipase and/or amylase levels were assessed during treatment.37 43 45 47 52 54 55 57 58 Episodes of pancreatitis were identified within trial participants in seven of these nine studies.37 43 47 52 54 57 58 Of the 16 studies not explicitly declaring lipase and/or amylase monitoring during treatment, episodes of pancreatitis were identified in only six studies.35 39 41 46 48 51
Discussion
This review has shown with moderate certainty that the use of AZA to induce remission and maintain medical induced remission in CD is probably associated with increased occurrence of pancreatitis. This GRADE rating suggests the results are probably unlikely to change with future studies. The number of patients treated to cause an episode of pancreatitis for induction therapy was 36 and for maintenance therapy was 31 patients. In the 947 participants receiving treatment with AZA, 36 patients developed pancreatitis, corresponding with a pancreatitis incidence of 3.80%, compared with a control risk in placebo patients of just 0.2% and 0.5% in 5-ASA patients. For every 33 patients treated with AZA for CD, an extra episode of thiopurine-induced pancreatitis would be expected. Within all these reported episodes, there was no reported mortality and while clarity of diagnostic criteria was difficult to ascertain, it appears that most cases were mild. As such, the clinical implications of these findings are to clarify the potential incidence of pancreatitis associated with AZA use and that in those cases withdrawal of therapy is likely, but the course otherwise appears to be mild.
The findings in 6-MP were different. In the postsurgical remission context where there are two large trials by Hanauer et al and Mowat et al with 327 participants showed no difference in pancreatitis incidence,45 51 with just one case in the 6-MP and placebo groups, respectively. In induction of remission, there was a difference based on one case occurring in the 6-MP group and none in the placebo. This led to no significant difference in incidence, However, as the numbers of studies and participants were much lower, this is a low certainty finding based on a difference in just one case of pancreatitis. It is nevertheless difficult to ignore the stark difference between this and AZA.
Our findings provide clarity following a range of previously published observational studies suggesting the incidence of thiopurine-induced pancreatitis to be as high as 8.9%. The results of this systematic review and meta-analysis reveal a lower than previously demonstrated incidence of AZA-induced pancreatitis with a reasonably mild course, as well as what appears to be a better profile with 6-MP. It is not possible to tell whether in clinical practice cessation of therapy would be needed, as the study protocols of most trials require any such biochemical changes to lead to cessation, regardless of clinical symptoms.
The strength to this review is that all included studies were RCTs; as such, many of the biases limiting the generalisability of the previously discussed observational studies are reduced, meaning the results are more directly aligned with the scientific truth. Furthermore, this review provides insight into the risks for specific groups of patients, such as postsurgery and in the induction of remission. It is worth noting that the use of purine analogues to induce remission is controversial in current practice but given the significant RCT evidence base included in this review, inclusion of these studies was deemed to be appropriate.
In May 2019 and June 2019, both the National Institute for Health and Care Excellence and the British Society of Gastroenterology published their most up-to-date consensus-based clinical guidelines on the management of CD and inflammatory bowel disease, respectively (table 5).21 22 Both guidelines recognise that thiopurines are contraindicated in patients who have previously experienced pancreatitis, and should be avoided even at low doses.21 Neither guidelines quantify the effect size of thiopurine-associated pancreatitis risk for those without previous incidence and therefore do not propose surveillance or cessation of therapy if such primary cases occur. Similarly, in clinical guidelines published in 2018 by the American College of Gastroenterology and the Japanese Society of Gastroenterology, while pancreatitis is recognised as an adverse effect, no effect size estimate is provided.23 24 The most recent guidelines published by the World Gastroenterology Organisation and the American Gastroenterological Association fail to make any reference to AZA-induced pancreatitis.27 28 The British National Formulary did mention the risk of pancreatitis as uncommon with AZA, which according to their guidance suggests the incidence is between one in 100 and one in 1000 dose administrations, and is therefore not aligned with our findings.75 Review of this manuscript in draft has already led to a change in the guidance within the UK British National Formulary in January 2020, now regarding the incidence of pancreatitis with AZA use as common. As with most treatments in CD, the benefits of therapy outweigh potential risks of adverse events and so this simply accurately reflects the incidence of this side effect with other well-recognised effects.
Thiopurine-induced pancreatitis in leading Crohn’s disease guideline publications
Purine analogues remain a mainstay treatment in CD as advocated by national and international societies.21 23–25 These findings are unlikely to lead to change in recommendations for their use. By the deployment of a robust systematic review methodology and the use of GRADE to assess the certainty of these key findings, we believe these results can be used by international societies and guideline committees to highlight this risk when counselling patients about other well-recognised adverse events, with a reliable incidence rate and associated clarity as to the likely severity of the course and its implications.
These conclusions are obviously limited by key elements within this review. First, the overall patient and event numbers led to a downgrading of the certainty of the findings due to imprecision. It is hard to justify future trials for just this purpose and this is a common issue with the GRADING of such adverse effect findings, but future updates of this review may use trials of efficacy to inform revisions of this finding. This is particularly pertinent in the context of 6M6, which had far less trials, but appears to have a much better profile. Second, our analysis assumed all patients who left the trial and not explicitly stated to have pancreatitis did not in fact have the condition. This is not the usual position when considering drop-outs, but due to the clear governance on safety within randomised trials, this was believed to be a reasonable assumption, but this may have had an impact on the results. Third, the paper has focused on CD. While these medications are used for ulcerative colitis, as they are not key therapeutics for the condition, this has not formed a focus for the study. Finally, there has been a distinction made between the use of these medications as induction and maintenance therapy. To clinical readers, this may not seem clinically useful, but as research papers tend to define studies with one of these two purposes, we have had to specifically subgroup studies in this way. Finally, exploration of the specific risk factors or patient characteristics that predispose to such side effects would be useful, but reporting was limited and this was not possible.
Future research may seek to clarify the severity of such cases of pancreatitis and study authors are encouraged to report these in line with the international criteria, as well as other confounding factors that may increase risk. While pancreatitis is only one of several idiosyncratic adverse events related to thiopurine intolerance, there may be elements of overlap with AZA-associated fever, arthritis and septic-shock clinical pictures following re-exposure. Human leukocyte antigen (HLA)-typing has been demonstrated to be an important and accurate predictor of pancreatitis risk, which may represent an opportunity to more precisely advise patients prior to starting AZA.26 76 An understanding as to why thiopurine-induced pancreatitis is seen in the context of CD and not with similar increased incidence when purines are used in other contexts or appears less frequent with 6-MP is needed. The use of serum metabolite testing during purine use is common and included in a number of international guidelines. Exploration as to whether such monitoring reduces risk of such side effects is also needed.
Conclusion
This is the first Cochrane format systematic review to consider pancreatitis as an adverse event associated with purine analogue use in CD. The estimated the overall incidence of AZA-induced pancreatitis in randomised trials of Crohn’s patients to be nearly 4% in patients receiving treatment, compared with a baseline risk of just 0.2%, with most cases mild and resolving after cessation of therapy. The difference between 6-MP and placebo was not significant. This finding should be of interest to patients, prescribers and policy-makers.
Ethics statements
Ethics approval
None as secondary systeamtic review
References
Footnotes
Contributors MG agreed to act as the guarantor of the article. MG, CG-C and AA designed the research study. CG-C registered the study with PROSPERO. CG-C and MG collected and analysed the data. CG-C and MG wrote the manuscript. AA, JM, NC, SH and IA inputted into subsequent revisions of the manuscript. All authors approved the manuscript submitted.
Funding The initial Cochrane review that inspired this work was funded by an NIHR Cochrane Programme Grant and MG has some funding for time as part of the programme used for this review.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- UpFront