Article Text

Statistics from Altmetric.com
Key messages
Rumination syndrome should be considered in any patient who presents with recurrent regurgitation without associated retching or significant nausea.
Behavioural therapies including diaphragmatic breathing and biofeedback are effective treatments for rumination syndrome and have the largest evidence bases.
Following treatment, most patients have large reductions in their frequency of regurgitation.
Introduction
When translated into English, the Latin word ruminor means to chew over again.1 This word has been used to describe the behaviour of a class of herbivorous mammals who, due to the indigestibility of the foods they eat, require that food is regurgitated and rechewed before being reswallowed to aid its breakdown and subsequent digestion.2 3 In certain herbivorous animals,3–5 rumination is, therefore, a normal, voluntary activity whereby gastric contents are brought up and rechewed as often as needed to optimise digestion.2 6 By contrast, rumination in humans, which was first described in 1618,4 is pathological as omnivores have no need of chewing the cud and fermenting the resultant matter within the stomach.
In humans, rumination is thought to be an acquired behavioural disorder.7 It is often unconscious and can occur in both children and adults.8 9 Although individuals with learning difficulties10 or eating disorders11 can suffer from rumination syndrome, it can and indeed often occurs in otherwise healthy individuals.9
Depending on whether children or adults are being studied, the prevalence of rumination syndrome ranges from 0.1% to 4%12 13 in children and 0.8% to 8%14 15 in adults. In a recent Rome Foundation global epidemiological study, rumination syndrome was found to have an overall worldwide prevalence of 2.8% with women having a slightly higher prevalence (3.1%) than men (2.5%).16 A higher prevalence of rumination syndrome has been noted in those with eating disorders (20%)17 18 and those with fibromyalgia (8%).14
Despite rumination syndrome being a relatively common disorder of gut–brain interaction, evidence suggests it is not well understood, resulting in patients often having to visit a number of clinicians and undergo several investigations before a diagnosis is eventually reached.19 Consequently, a formal diagnosis can be delayed, leading to weight loss and malnutrition.19
This paper aims to set out the key diagnostic features of rumination syndrome, important differential diagnoses to consider, useful investigations to help dispel uncertainty and current evidence-based therapies.
Clinical features
Diagnostic criteria for rumination syndrome feature in the literature from three sources. First, the Rome IV diagnostic criteria for gastroduodenal disorders,20 the International Classification of Diseases21 or the Diagnostic and Statistical Manual for mental Disorders22 (table 1).
Comparative Rome IV, ICD-11 and DSM-5 definitions of rumination syndrome20–22
The key feature of rumination syndrome is the effortless regurgitation of recently ingested food or fluids which results in patients either masticating and reswallowing the regurgitant or spitting it from their mouths.20 Importantly, this behaviour is not preceded by nausea or retching. Furthermore, it must have occurred on numerous occasions for weeks to months prior to diagnosis.20
Food and fluids can be repeatedly regurgitated for up to 2 hours after initial ingestion.23 In addition, the regurgitant is undigested and non-acidic,19 hence the reswallowed material often retains an inoffensive taste. Acidification of the regurgitant as digestion occurs often causes the regurgitation to stop.20
Invasive investigations are not usually required to establish the diagnosis of rumination syndrome. A comprehensive history to elicit the key clinical features (table 1) is sufficient in the majority of cases. Instead, focused investigations are often used where there is diagnostic uncertainty, significant weight loss or to exclude important differential diagnoses—which in the case of postprandial regurgitation are gastro-oesophageal reflux disease (GORD) with regurgitation, achalasia and eating disorders.
Pathophysiology
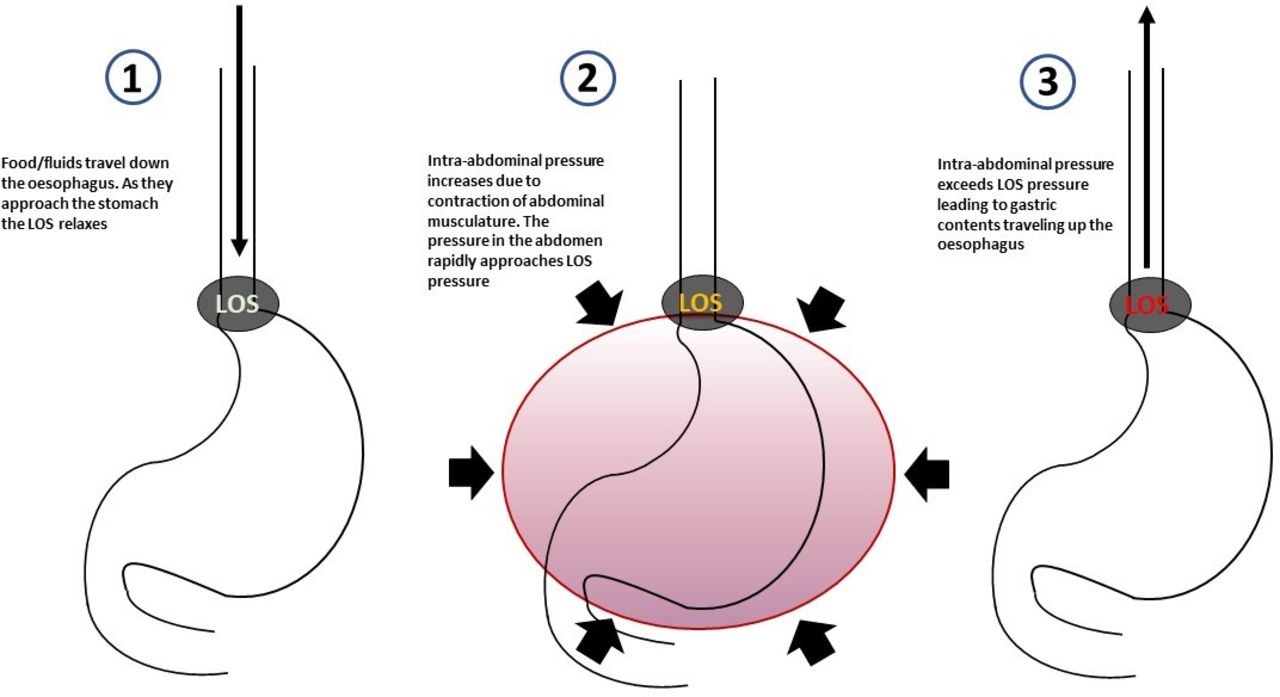
Studies have shown that following the ingestion of food or fluids, patients with rumination syndrome frequently subconsciously and habitually contract their intercostal and anterior abdominal muscles.24 Contraction of the intercostal muscles results in costal expansion, while contraction of abdominal muscles including the rectus sheath and internal and external obliques increases intra-abdominal pressure. In conjunction with this, the lower oesophageal sphincter (LOS) relaxes.25–27 This is a reversal of the normal gastro-oesophageal pressure profile where at rest, intragastric pressure is normally low and LOS pressure is high. These resultant pressure changes result in gastric contents being propelled cranially into the oropharynx (figures 1 and 2).28

Illustration of the sequence of events that occur in rumination syndrome. LOS, lower oesophageal sphincter.

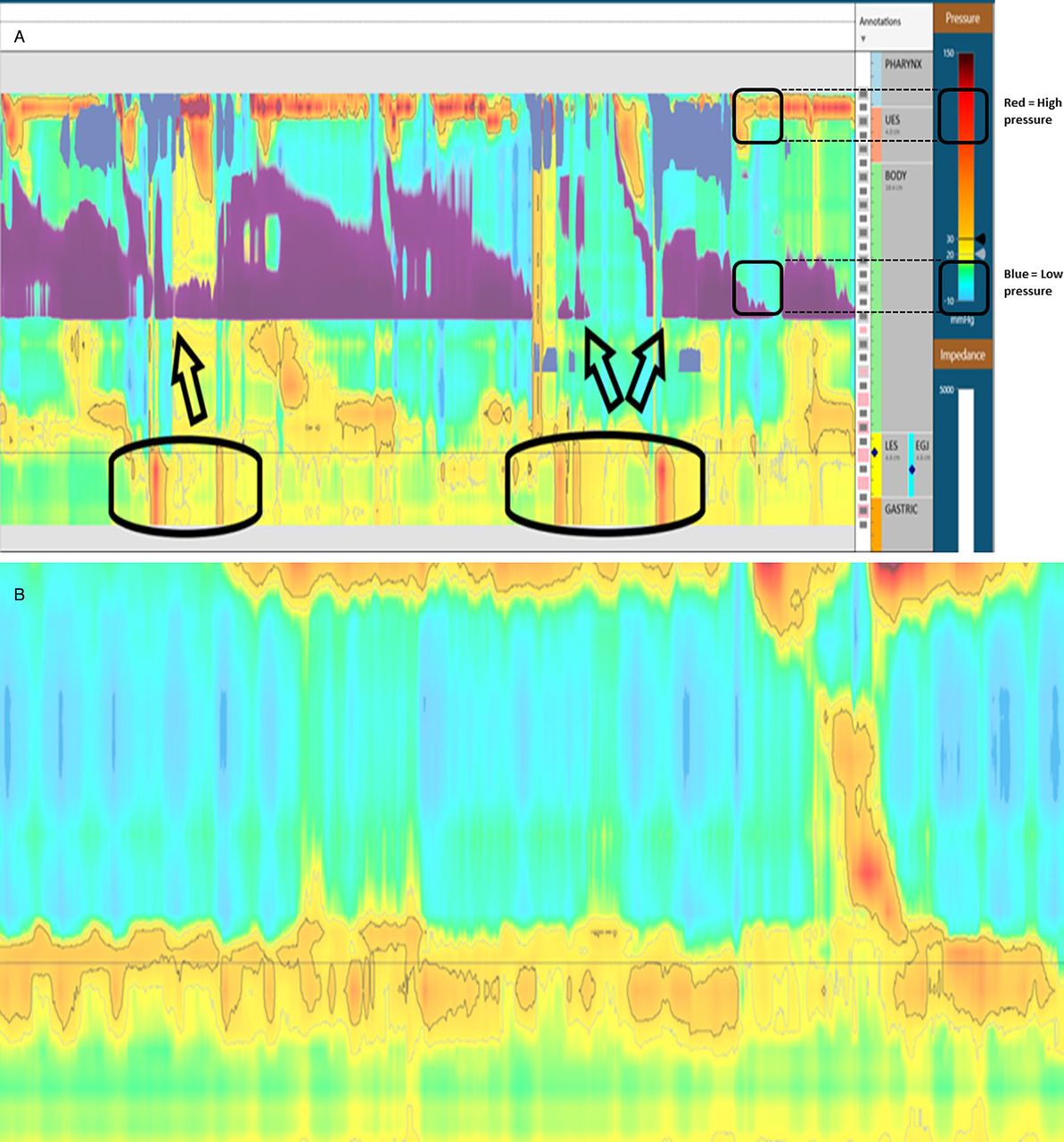
A simplified illustration of pressure and impedance traces during an episode of rumination. As can be seen, there is a postprandial increase in gastric pressure and a decrease in impedance (demonstrating cranial movement of gastric contents).
Rumination syndrome is an acquired behavioural disorder and, in some cases, a detailed history can reveal a particular priming episode of psychological stress or gastrointestinal (GI) upset (eg, gastroenteritis) which occurred prior to rumination being noticed.29 30 This event may be relatively minor and swiftly forgotten but it is theorised it prompts patients to tense their abdominal walls in order to relieve discomfort.7 This initial priming episode, later maintained and reinforced, leads to patients habitually tensing their abdomen postprandially.24 While rumination is almost always a primary condition, it is recognised that rumination can occasionally be a secondary response to gastro-oesophageal reflux episodes (secondary rumination), where the rumination behaviour is thought to be a conditioned, maladaptive response to oesophageal discomfort caused by GORD.26 Similarly, patients with established rumination often report postprandial fullness or discomfort occurring before their episodes of regurgitation.7 Subsequent abdominal tensing and regurgitation may also be due to a subconscious, maladaptive method of discomfort reduction.
Complications
When severe, rumination syndrome can lead to malnutrition and dehydration which, in turn, can lead to electrolyte imbalances and the occurrence of refeeding syndrome when nutrition improves.31–33 Malnutrition and dehydration arise due to either a possible reduced desire to eat or drink so as to avoid episodes of regurgitation or spitting of food and fluids, reducing nutritional intake below what is required for good health.31
Additional complications in children and adults include failure to thrive,34 dental erosions,35 an increased likelihood of aspiration,23 halitosis36 37 and stigma due to the rumination itself or its associated complications.38
Differential diagnoses
While there is a long list of potential differentials for patients presenting with recurrent episodes of regurgitation, a few key conditions need to be excluded if, after a history is obtained, there remains a degree of uncertainty (table 2). GORD, achalasia, gastric outlet obstruction and gastroparesis can present with recurrent regurgitation although often with other symptoms including nausea and dysphagia. From a mental health standpoint, bulimia nervosa can mimic rumination syndrome, and an early psychiatric opinion should be sought if there is a suspicion of an eating disorder.17
Differential diagnoses and important clues for rumination syndrome
Investigations
Usually, in the context of recurrent episodes of regurgitation, an oesophagogastroduodenoscopy (OGD) and/or a barium study will have been performed to exclude structural pathology in the upper GI tract. This would be mandatory prior to proceeding to oesophageal physiology testing as per national guidelines to exclude any contraindications to the passage of probes for motility studies.39
The gold standard investigation for rumination syndrome, in cases where a history is insufficient to make a firm diagnosis, is high-resolution oesophageal manometry (HROM) with concurrent impedance monitoring. The manometric aspect of the investigation enables visualisation of the abrupt rise in gastric pressure and subsequent postprandial relaxation of the LOS, while the concurrent impedance monitoring demonstrates the regurgitated material25 (figure 3A). Gastric pressures increase by ≥30 mm Hg followed by cranial movement of gastric contents.26 HROM involves a manometry catheter, containing >30 pressure sensors interspersed at 1 cm intervals,39 being inserted transnasally before patients are asked to either lie supine (classically) or sit upright. The catheter is positioned so that its tip is roughly 5 cm below the LOS. Some advanced oesophageal high-resolution manometry systems have in-built combined oesophageal impedance capability which is ideal for the purpose of investigation for rumination. In the absence of a system with combined impedance/manometry, a second catheter in the opposite nostril for concurrent pH/impedance recording is often required. During a test for suspected rumination, patients are often instructed to consume a ‘test meal’ such as a cereal, and during the stationary manometry study monitoring is usually extended for up to 3 hours postprandially. During the test, oesophageal pressure and impedance traces can be visualised providing visual cues to demonstrate observed abnormalities to patients (figure 3A). This can help improve understanding and acceptance of the diagnosis.40 Episodes of rumination often occur sporadically, and can be influenced by an individual’s social setting or level of distraction. As a result, longer studies with ambulatory 24-hour HROM, despite not being widely available, may have the potential to improve the diagnostic yield.41

Pre and post behavioural treatment manometry findings in a patient with Rumination Syndrome. (A) High-resolution manometry showing postprandial abdominal contractions (circle) and proximal regurgitation (arrows). Red areas are areas of high pressure while blue areas are areas of low pressure. (B) Elimination of rumination-like behaviour during biofeedback and diaphragmatic breathing.
Management
Explaining the diagnosis
Following a positive clinical diagnosis of rumination syndrome, one of the most crucial aspects of treatment is an effective doctor–patient interaction. This should include a detailed explanation to educate the patient on the nature and pathophysiology of the condition with reassurance. A sympathetic approach, explaining that the regurgitation is caused by an involuntary habit, leading to subconscious tension of the abdominal muscles is often extremely beneficial and therapeutic.42 These explanations can be reinforced by the provision of a patient information leaflet recently developed by Guts-UK (https://gutscharity.org.uk/advice-and-information/conditions/rumination-syndrome/).
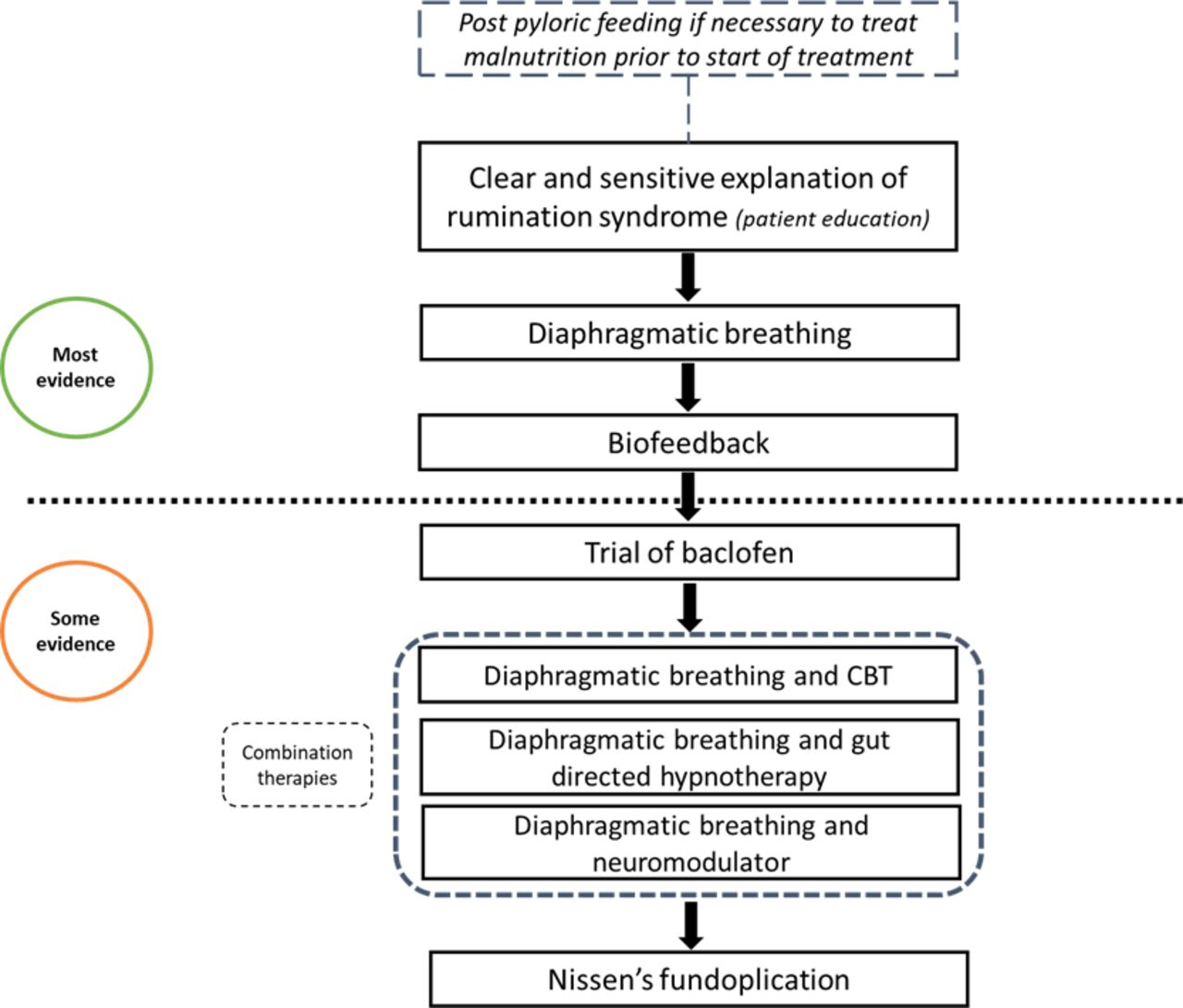
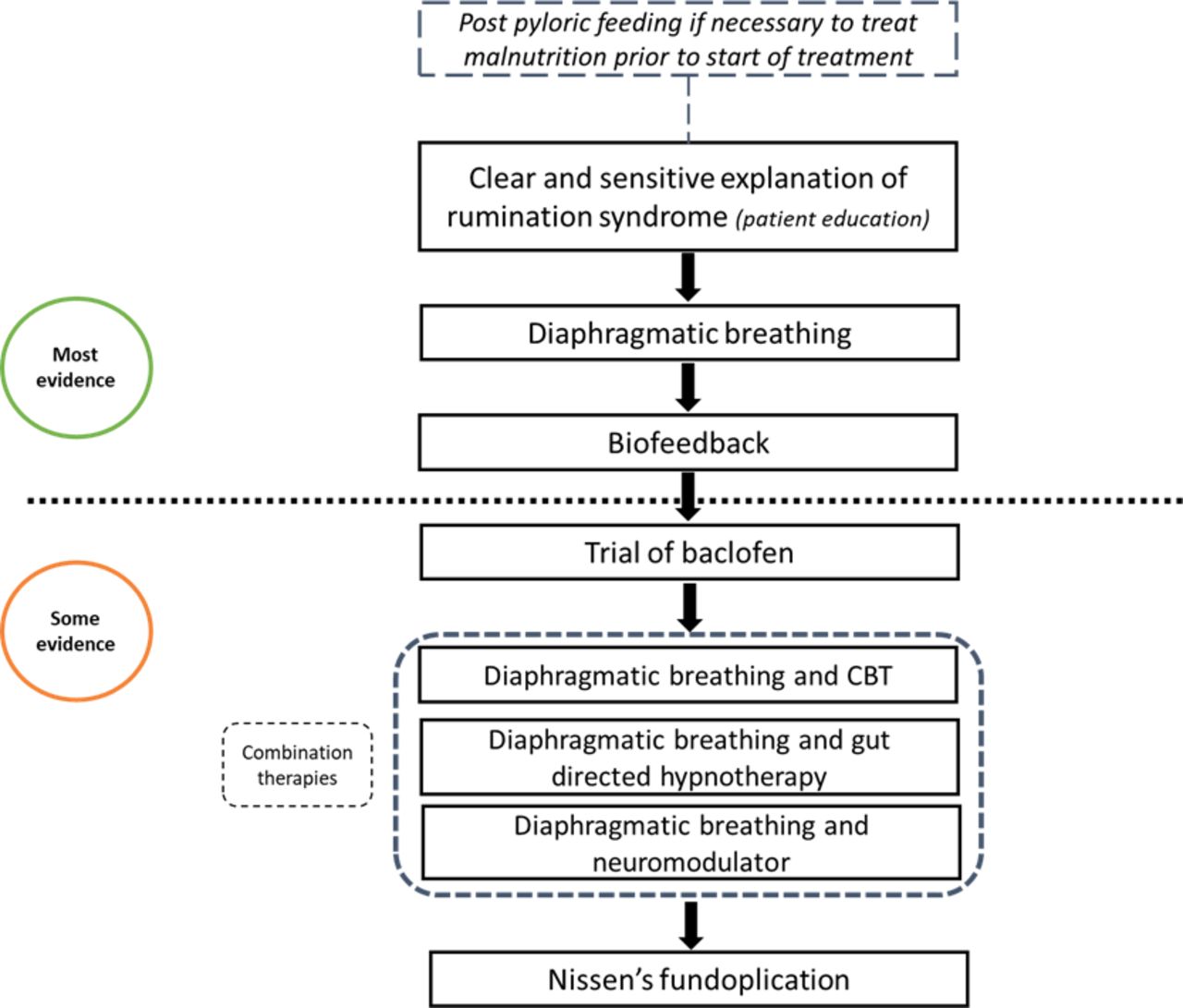
Armed with the knowledge of why they regurgitate, and reassurance that a sinister cause has been confidently excluded, many patients may not need any further intervention. However, should they require further treatment, the treatment options, summarised in figure 4, include behavioural and to a lesser extent medical approaches which are often used in combination in refractory cases.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Rumination syndrome management flow chart. CBT, cognitive–behavioural therapy.
Nutritional considerations
Prior to receiving a formal diagnosis and treatment plan, patients with suspected rumination syndrome can be at risk of malnutrition. A comprehensive nutritional assessment is required to assess for features of malnutrition, and some patients with features of malnutrition may need consideration for a period of nutritional support with nasojejunal/post-pyloric feeding prior to the commencement of definitive rumination treatment. While a detailed review of nutritional assessment and management is beyond the scope of this article, this has been covered in a recent comprehensive review on the indications and role of post-pyloric feeding in this context.43
Behavioural therapy
Behavioural interventions have the greatest evidence base for the treatment of rumination syndrome. The two interventions most often used are diaphragmatic breathing and biofeedback.
Diaphragmatic breathing can be taught at the bedside by clinicians, nurse specialists, speech and language therapists or behavioural therapists. It involves instructing patients to breathe by expanding and contracting their abdomen, as opposed to the normal pattern of chest wall movements with respiration.44 Essentially, patients are asked to place one hand on the anterior aspect of their chests and one hand on their abdomen. They are then asked to breathe in such a way that their abdominal hand rises and falls while their chest hand remains still. This technique is thought to work by disrupting the postprandial abdominal contractions which cause regurgitation.28 Diaphragmatic breathing has been shown to significantly reduce the frequency of regurgitation, increase the pressure at the oesophagogastric junction and reduce intragastric pressure.28 Furthermore, it is can be easily learnt by participants, taking roughly 5 min.28 When patients are taught to breathe in this manner, they are initially asked to lie flat with their knees bent so as to relax their abdomen. Over time, as this type of breathing becomes easier to perform, patients can be encouraged to perform diaphragmatic breathing while seated upright. Patients should be advised to practise diaphragmatic breathing for 5–10 min whenever regurgitation occurs. This can be done during or following each meal. However, should they experience any regurgitation between meals, they are advised to perform additional diaphragmatic breathing. The aim is to promote this type of breathing to become the normal type of breathing practised during the postprandial period in order to suppress rumination behaviours. An educational video demonstrating diaphragmatic breathing has been produced by the authors to compliment this article and can be accessed online via weblink (https://youtu.be/h46ZsxfpSOU).
When the response to diaphragmatic breathing is incomplete, more advanced behavioural therapy with biofeedback may be an effective tool for rumination syndrome. The principles of biofeedback for rumination are to promote behavioural modification and improve the efficacy of diaphragmatic breathing by visually demonstrating the physiological abnormalities to the patient and how they can be corrected in real time (figure 3). Formal biofeedback using this approach either with electromyography or HROM can be effective in teaching patients how to relax their abdominal wall musculature after eating using visual cues resulting in a significant reduction in the frequency of regurgitation (figure 3B).24 45 While the availability of formal biofeedback programmes for this condition in the UK is limited, a brief intervention can readily be delivered by any clinician able to teach diaphragmatic breathing during a diagnostic concurrent HROM/impedance study in patients with positive manometry findings for rumination. In the authors’ experience, this type of brief intervention at the end of a diagnostic test can be very beneficial in helping the patient optimise their diaphragmatic breathing technique46 and improving symptom control.
Recent evidence suggests that diaphragmatic breathing and biofeedback are not only beneficial for treating primary rumination,26 but may also be effective in treating secondary rumination associated with acid reflux, either with or without antacid therapy, due to the positive effects of diaphragmatic breathing on reducing acid reflux events and acid exposure times.26 47
In a similar behavioural vein, there is some evidence from paediatric case reports that chewing gum after meals reduces the frequency of regurgitation.48 This is thought to work by distracting patients. Additionally, a recent study by Murray et al used cognitive–behavioural therapy (CBT) to supplement diaphragmatic breathing. Following dual behavioural therapy, participants had greater reductions in regurgitation than following diaphragmatic breathing alone.49 Where available, gut-specific behavioural techniques such as CBT, or gut-focused hypnotherapy, a technique that often incorporates diaphragmatic breathing, may therefore have an adjunctive role,50 and their additional benefit should be investigated in future studies.
Pharmacological therapy
There are very few studies on effective medical therapy for rumination syndrome. Baclofen may however be a reasonable option as second-line management option following behavioural approaches. Baclofen works by increasing the resting tone of the LOS thereby reducing the ease of reflux of gastric contents.51 Unfortunately, it is known to cause various side effects, which commonly include drowsiness, dizziness and headaches.52 Despite these side effects, studies using baclofen to treat GORD have shown that it is well tolerated when taken at low doses.53 Two small studies have shown that baclofen can be used to treat rumination syndrome with promising results. The first was by Blondeau et al in 2012 in a sample of 12 patients,54 where 10 mg of baclofen administered three times per day was shown to increase lower oesophageal sphincter tone and reduce episodes of regurgitation. These findings were confirmed in 2018 by Pauwels et al in a group of 20 patients.55
Furthermore, a study by Robles et al combining diaphragmatic breathing with a tricyclic antidepressant as a gut–brain neuromodulator showed large reductions in postprandial regurgitation,56 suggesting that the addition of a neuromodulator may augment the effects of behavioural therapy.
Surgical intervention
Limited evidence from case series23 suggests that in refractory cases, rumination syndrome can be treated with Nissen’s fundoplication in order to enhance the resting pressure of the LOS and to partially negate the intragastric propulsive force provided by contraction of anterior wall musculature by reducing concurrent LOS relaxation. Due to the lack of high-quality evidence, the role of surgery remains unclear, and should only be considered on a case-by-case basis, when there is a firm diagnosis of severe rumination, refractory to all the recommended behavioural and medical options, and with ongoing inadequate oral intake. There may however be a stronger case for anti-reflux surgery in patients where secondary rumination events have been shown to be triggered by acid reflux events on impedance/manometry traces without response to anti-reflux medications. In the rare setting when surgery is considered for severe, refractory, primary rumination, the diagnosis should ideally be supported by positive impedance and manometry studies. In summary, further research is required to firmly establish the role of invasive surgery in this acquired behavioural condition.
Rumination clinical scenarios
Scenario 1
A young patient with no significant medical history was referred with reflux symptoms for a second opinion. The patient had been investigated elsewhere with a normal upper GI endoscopy. On further questioning, the patient reported a long history of postprandial effortless regurgitation. There was no associated nausea, vomiting, dysphagia or weight loss. The regurgitated material was often reswallowed but on occasion spat out.
A diagnosis of rumination syndrome was discussed and explained to the patient, who agreed with the diagnosis and was reassured by this. A trial of diaphragmatic breathing during mealtimes and in the postprandial period was advised which resulted in significant symptom improvement.
This case highlights that in some cases of rumination syndrome, explanation of the condition, along with reassurance, is all that is required.
Scenario 2
A patient with a history of vomiting shortly after eating was referred to gastroenterology clinic. On detailed questioning, the patient reported almost immediate regurgitation of food and medications shortly after swallowing. There was no nausea, vomiting or weight loss. A small hiatus hernia was noted on OGD.
HROM with concurrent impedance demonstrated evidence of intragastric pressurisation throughout the study with evidence of retrograde bolus flow regurgitation. The findings were consistent with rumination syndrome. Diaphragmatic breathing was advised but had limited effect. Therefore, the patient was referred for HROM-directed biofeedback with diaphragmatic breathing which successfully eliminated the rumination-like behaviour.
Conclusion
Rumination syndrome is a poorly recognised, infrequently diagnosed, yet easily manageable disorder of gut–brain interaction. Greater awareness among medical professionals will ensure prompt diagnosis, prevent malnutrition and reduce inappropriate referrals for psychiatric assessments or invasive investigations.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
References
Footnotes
Twitter @hasan20187, @DisneyBen, @DipeshVasant
Contributors AS drafted the manuscript and performed literature review. BRD reviewed and helped write the manuscript and provided original figures. SSH reviewed the paper, contributed to the section of behavioural therapies and helped produce supplementary educational material on diaphragmatic breathing. DHV conceived the paper, searched the literature and helped write and review the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Highlights from this issue