Article Text

Abstract
Objective Endoscopy departments have experienced considerable challenges in the provision of endoscopy services since the start of the COVID-19 pandemic. Several studies have reported a reduction of procedures performed by trainee endoscopists during the pandemic. The aim of this study was to assess the impact on colonoscopy training and quality in an academic centre throughout successive waves of the pandemic.
Methods This was a single-centre, retrospective, observational study comparing colonoscopies performed at a tertiary endoscopy centre in Ireland at different stages of the pandemic with those performed during a similar time frame prepandemic. Data were collected using electronic patient records. Primary outcomes were procedure volumes, adenoma detection rate and mean adenoma per procedure.
Results In the prepandemic period, 798 colonoscopies were performed. During the same period in 2020, 172 colonoscopies were performed. In 2021, during the third wave of the pandemic, 538 colonoscopies were performed. Percentages of colonoscopies performed by trainees were 46.0% (n=367) in 2019, 25.6% (n=44) in 2020 and 45.2% (n=243) in 2021. Adenoma detection rate was 21.3% in 2019, 38.6% in 2020 and 23.9% in 2021. Mean adenoma per procedure was 0.45 in 2019, 0.86 in 2020 and 0.49 in 2021. Caecal intubation rate was 90.74% in 2019, 90.9% in 2020 and 95.88% in 2021.
Conclusion The COVID-19 pandemic initially had a negative impact on overall colonoscopy volumes and training. Despite a reduction in procedural volume, key performance standards were maintained by trainees. Maintenance of hands-on training is essential to allow trainees achieve and retain competency in endoscopy.
- ENDOSCOPY
- COLONOSCOPY
- COVID-19
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known about this subject?
Maintenance of hands-on training for gastrointestinal (GI) trainees is crucial to achieve and maintain skills in a procedural specialty. Achievement and maintenance of competency in endoscopy for GI trainees during the pandemic has been a focus of concern. Several studies have reported a reduction of endoscopic procedures performed by trainee endoscopists in the early months of the pandemic. There is little published data on the recovery of trainee endoscopic experience as the pandemic has progressed.
What are the new findings?
A marked reduction in colonoscopy case volume was observed in the first wave. Following a review of trainee experience in 2020, measures were put in place to protect endoscopy training volumes for trainees in our department. Despite the high incidence of COVID-19 during the third wave in Ireland (Winter 2021), a much smaller reduction in the number of colonoscopies performed by trainees was observed in comparison with the first wave in our institution.
How might it impact on clinical practice in the foreseeable future?
Safeguarding endoscopy training is essential to allow GI trainees achieve and maintain competency in endoscopy and to provide a steady stream of trained endoscopists to support healthcare systems into the future.
Practical measures to supplement hands-on endoscopy training
Interactive online sessions and small group tutorials focusing on;
Knowledge of equipment—including individual endoscopes, endoscopy stack units, snares, clips, diathermy units…
Technical theory—for example, theory of managing loops, use of snares, application of clips…
Pathology recognition—for example, polyp classifications (morphology and pit architecture), commonly used endoscopic scoring systems (Barrett’s oesophagus, oesophageal varices, inflammatory bowel disease)…
Small group review of live-recorded clinical case-based vignettes.
Introduction
In Spring 2020, guidelines for the safe practice of endoscopy during the COVID-19 pandemic were introduced in Europe.1–3 Endoscopy units transformed to comply with guidelines to prevent the spread of COVID-19 and to protect patients and staff. Many units experienced a marked decrease in case volume,4–8 prioritising urgent and emergent patients. Efforts were made to reduce staff numbers in procedure rooms because of concerns about continued supply of personal protective equipment (PPE) and safety of endoscopists. These adjustments resulted in reduced opportunities for endoscopy training during the first wave.9 Endoscopy units have adjusted to ensure continued focus on high-quality procedures. While early data suggest that this has been maintained,10 further data are needed, particularly considering clear evidence of delays in colorectal cancer (CRC) diagnosis and management11 and data projections suggesting these delays will have an impact on cancer related mortality for up to 5 years.12 It is therefore imperative that all endoscopy units focus efforts on maintaining procedure volumes, quality and training to mitigate this effect as much as possible.
Many countries worldwide have experienced multiple waves of the virus, causing repeated interruptions to healthcare. Although we have become more experienced in dealing with COVID-19 and its management as a result of improved knowledge of its virulence and pathophysiology,13 elective healthcare provision remains a considerable challenge.
In Ireland, routine elective care was cancelled during the Spring 2020 and Winter 2021 surges. Staff shortages were widespread due to COVID-19 precautions. Redeployment of non-consultant hospital doctors, including gastroenterology trainees, to care for and manage patients with COVID-19-related illness was implemented.
The endoscopy training environment has changed dramatically. Redeployment of staff, a sustained reduction in endoscopy procedures, cancellation of routine elective care, and early concern in relation to possible shortages of PPE have led to considerable challenges for the continuation of endoscopy services across Europe since the start of the pandemic.
The aim of this study was to assess the impact on colonoscopy training and quality in an academic centre over the course of successive waves of the COVID-19 pandemic.
Methods
This was a single-centre, retrospective, observational study comparing colonoscopies performed at a high-volume tertiary endoscopy centre in Ireland at different stages of the COVID-19 pandemic with those performed during a similar time frame prepandemic. The first date of implementation of COVID-19 endoscopy precautions represents the start date of the 2020 data set (16 March 2020). The length of this time period reflects the duration of the first wave in Ireland (March to June 2020), with the end point corresponding with a decline in national COVID-19 case numbers and associated easing of restrictions as lockdowns were slowly reversed. The 2019 time period mirrors the 2020 dates (March to June 2019). The third period studied correlates with the third wave of the pandemic in Ireland (January to March 2021).
Colonoscopies were performed by gastroenterology consultants, trainees under consultant supervision and nurse endoscopists. Gastrointestinal (GI) trainee assisted colonoscopies were colonoscopies that required hands-on assistance from a supervising consultant.
Data, including patient demographics, endoscopist key performance indicators (KPIs), pathology yields and histology, were collected using electronic patient records. Primary outcomes were procedure volumes, adenoma detection rate (ADR) and mean adenoma per procedure (MAP). ADR was defined as the proportion of colonoscopies during which one or more adenoma(s) was biopsied or removed. MAP was calculated by dividing the total number of adenomas detected by the total number of colonoscopies in each time period. Sessile serrated lesions detected were included with traditional adenomas for these calculations.
In an attempt to compensate for reduced exposure to hands-on training, we delivered a number of consultant-led online and small group teaching sessions, focusing on endoscopy theory, technical aspects of common scenarios (eg, management of looping, use of snares), pathology recognition and appropriate use of common endoscopic scoring systems.
Study outcomes are reported in accordance with STROBE guidelines for observational research.14
Results
During the reference period (March to June 2019), 798 colonoscopies were performed. During the same period in 2020, 172 colonoscopies were performed. In 2021, during the third wave of the pandemic, 538 colonoscopies were performed (table 1, figure 1).

Comparison of colonoscopy volumes in pre-pandemic and pandemic periods, GI, gastrointestinal.
Baseline characteristics of colonoscopies performed by GI trainees
The majority of colonoscopies were performed by a consultant (2019: n=402, 50.4%; 2020: n=126, 73.3%; 2021: n=289, 53.7%). The percentages of colonoscopies performed by trainees were 46.0% (n=367) in 2019, 25.6% (n=44) in 2020 and 45.2% (n=243) in 2021 (figure 1). Levels of endoscopic experience varied from year 1 (novice <50 procedures) to year 5 (independent with >400 total colonoscopies with direct observation of procedural skills assessments completed to satisfactory level). Exact procedure numbers for individual trainees were not available, but the three time periods reviewed included procedures performed by 16 trainees; 5 of whom were year 1, 5 year 2, 1 year 4, 4 year five and 1 postcompletion of specialist training endoscopy fellow.
A subgroup analysis of colonoscopies performed by trainees compares patient characteristics, casemix and indications for colonoscopies performed during each time period (table 1). Baseline patient characteristics were comparable across all three groups. A change in case-mix was observed in the first wave of COVID-19 (2020) compared with the prepandemic period (2019) and the third wave (2021). In the first wave of the pandemic, 50.0% (n=44) of colonoscopies were performed for inpatient referrals. In 2019 and 2021, the majority of cases (95.6% (n=351) and 89.7% (n=218), respectively) were day case outpatient procedures.
The main indications for colonoscopy in the prepandemic period were polyp or CRC surveillance (21.0%), diarrhoea or alternating bowel habits (18.0%), anaemia (17.7%) and family history of polyps or CRC (17.2%). In 2020 and 2021, fewer surveillance colonoscopies were performed. The main indications included anaemia (2020: 43.2%; 2021: 18.1%), diarrhoea and alternating bowel habits (2020: 18.2%; 2021: 25.1%), and rectal bleeding (2020: 15.9%; 2021: 22.2%).
Table 2 illustrates colonoscopy KPIs for trainees and pathology yields across the three time periods. KPIs included sedation rates, quality of bowel preparation, caecal intubation rates and withdrawal times (WT).
The comparison of GI trainees’ KPIs and pathology identified
Overall, 327 polyps were detected in colonoscopies performed by GI trainees in 2019. In 2020 and 2021, 54 and 186 polyps were detected, respectively. The ADR was 21.3% in 2019, 38.6% in 2020 and 23.9% in 2021. The MAP was 0.45 in 2019, 0.86 in 2020 and 0.49 in 2021.
Discussion
The effect of the COVID-19 pandemic on the healthcare system and procedure waiting lists presents a significant challenge. With a reduction in endoscopy list size and cancellation of routine elective care intermittently throughout the pandemic, waiting lists have increased. The consequences of this are likely to be far reaching and long term.11 12
In the first wave of the pandemic, there was a significant reduction in outpatient colonoscopies performed in our unit with a marked increase in the proportion of colonoscopies performed for inpatient referrals. This change in casemix corresponds to the cancellation of routine elective care with strict COVID-19 restrictions placed on endoscopy units. Outpatient numbers were reduced to allow for social distancing in the department, including the waiting room, preprocedure waiting area and postprocedure recovery area. In the early stages of the pandemic, a downtime period was observed in each endoscopy room between procedures to allow for cleaning. These necessary safety measures impacted negatively on the endoscopy list capacity. Despite a much higher incidence of COVID-19 infection nationally during the third wave, outpatient colonoscopy volumes did not decrease as significantly as during the first wave (table 1). Endoscopy guidelines have adapted over time,15 16 allowing for more efficient management of endoscopy lists, while continuing to provide a safe environment for patients and staff. PPE is more widely available. There is a greater awareness of the virus and how to manage it, as well as the availability of vaccines with most healthcare workers in Ireland receiving first doses during the month of January 2021. COVID-19 safety questionnaires are now completed by patients in advance of their appointments.
The indications for colonoscopy differed between the prepandemic and pandemic time periods. The change of indications seen during the pandemic surges also reflects the suspension of routine elective care. Clinically urgent and time sensitive referrals were prioritised. The top three indications in 2020 and 2021 were related to higher risk symptoms, while fewer surveillance colonoscopies were performed.
Colonoscopies performed under the national CRC screening programme were not included in our subgroup analysis as these procedures do not involve endoscopy trainees. While this programme was paused during the first wave of the pandemic in March 2020, it was re-commenced in June 2020 and continued through the second wave in 2021.17
Bowel preparation scores were below the recommended level.18 The omission of screening and surveillance colonoscopies and the higher percentage of inpatients and symptomatic outpatients on the trainee lists may account for suboptimal preparations.
Mean WT was significantly longer than the minimum 6 min standard recommended.18 WT is automatically calculated by our endoscopy reporting system and does not factor in procedural time (eg, polypectomy). A subgroup analysis of colonoscopies where no polypectomy was performed showed WTs to be shorter but still comfortably above the minimum standard (data not shown). It remains possible that an increased focus on theoretical training resulted in enhanced focus on quality for our trainees; although, we did not study this directly.
Across all three time periods, ADRs were above recommended thresholds18; indicating the preservation of quality despite challenges encountered. There was a reduction in the number of polyps identified in 2020 due to reduced overall procedure volume. Fewer large polyps (>1 cm) were identified. For these reasons trainees had less exposure to standard and advanced polypectomy techniques, an important component of core colonoscopy training. Despite a reduction in overall polyp numbers, MAP in 2020 was almost twice that observed in 2019 and 2021. This no doubt reflects the narrower range of indications for colonoscopy during the first COVID-19 wave. There are clearly lessons to be learnt in terms of referral validation as we hopefully move out of the pandemic, including efforts to improve the specificity of our referral pathways by prioritising higher risk clinical indications and increasing availability of non-invasive methods (such as faecal immunochemical testing and calprotectin) as an adjunct to inform validation of referrals.
The collateral damage of the pandemic in terms of non-covid related health outcomes is yet to be quantified. In their population-based study in 2020, Maringe et al 12 estimated that there will be a 15.3%–16.6% increase in CRC related mortality in the UK due to diagnostic delays associated with the pandemic. Our efforts to compensate for these delays and address the unavoidable care gaps already being experienced by patients will rely on a well-trained body of skilled endoscopists. Those currently in training are expected to play a central role. Several studies have reported a reduction of endoscopic procedures performed by trainee endoscopists in the early months of the pandemic. An international survey of 770 trainees across 63 countries published in April 2020 reported a median percentage reduction of 99% in the total procedures performed by the respondents compared with a prepandemic period.9 Similarly, a British Society of Gastroenterology survey distributed to UK trainees described a mean percentage reduction of 96.0% for all trainee procedures,19 with colonoscopies associated with the greatest mean percentage reduction (97.2%). Barriers to training identified in the literature include institutional policies to minimise staff in procedure rooms, reduced procedure volume and shortages of PPE.9 19–21
Achievement and maintenance of competency in endoscopy for GI trainees during the pandemic has been a focus of concern.19 20 22–24 A reduction in case volume for trainees is associated with reduced opportunities to develop technical diagnostic and therapeutic procedural skills, including polypectomy, during a finite period of training. It is also associated with reduced exposure to the organisation and management of the endoscopy unit and the care of patients periprocedurally; aspects of endoscopy training that should not be overlooked. Ensuring adequate training is important to endoscopy services and is a key feature of endoscopy unit accreditation programmes.25 Strategies to safeguard endoscopy training during the pandemic have been proposed.26–28
There is little published data on the recovery of trainee endoscopic experience as the pandemic has progressed. In this study, a marked reduction in colonoscopy case volume was observed for our trainees in the first wave. Following a review of trainee experience in 2020, measures were put in place to protect endoscopy training volumes for trainees in our department as well as supplementing hands-on training with video-based vignettes, web-based and small group lectures, focusing on pathology recognition, technical theory and endoscopic non-technical skills. Videos of live cases and samples of equipment were used as visual aids outside of the endoscopy room. Teaching sessions were led by gastroenterology consultants and were interactive. Formal assessment on the educational benefit of these interventions is ongoing. We propose to maintain and further develop these measures as an adjunct to hands on training in line with the National Endoscopy Programme’s training structures29 going forward.
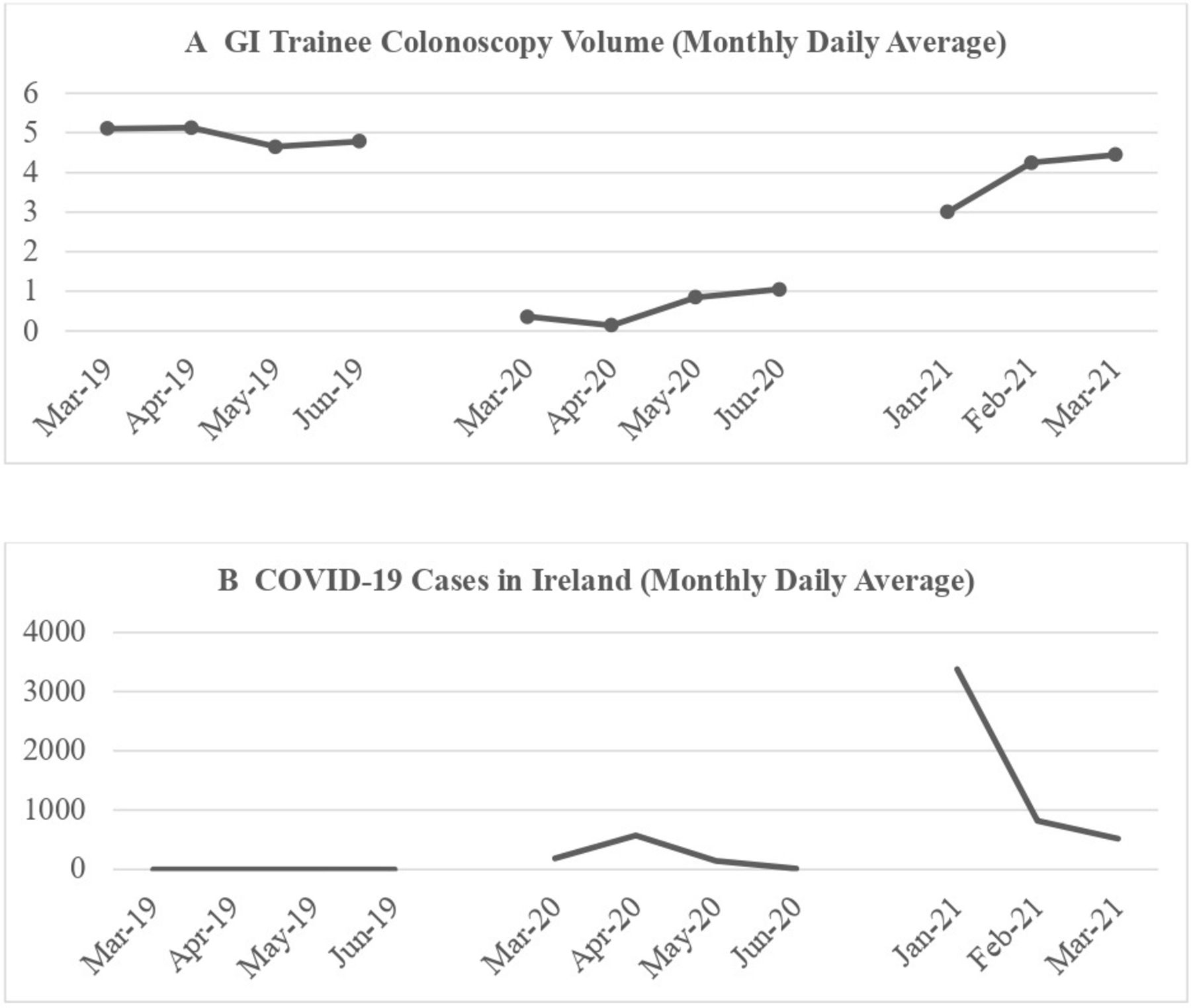
Despite the high incidence of COVID-19 nationally during the third wave, a much smaller reduction in the number of colonoscopies performed by trainees was observed in comparison with the first wave (table 1, figure 1), with a similar monthly daily average of colonoscopies performed by trainees towards the end of the third wave as compared with 2019 (figure 2). An increase in supervised procedures was observed in 2021, suggesting an improved training environment.
{kind=link}
{kind=link}
The monthly daily average of colonoscopies performed by GI trainees (A) compared with the monthly daily average of COVID-19 cases in Ireland (B). GI, gastrointestinal.
Six of the 16 trainees (38%) included in this study have since completed their specialist training. The remainder are still in training. While it appears that the most junior trainees were more severely affected by COVID-19 precautions in the endoscopy department during the first wave of the pandemic, with first year trainees initially excluded from lists to prevent prolonged procedures, it remains to be seen whether this will result in delays for these trainees reaching endoscopic competence. Our ability to adapt our training model and maintain quality is reassuring and it is clear that procedure volumes for all trainees have now recovered. The long-term impact of the pandemic on endoscopy training should be a focus for further study. It remains imperative that we continue to support all aspects of endoscopy training to ensure these trainees achieve competency on schedule.
Conclusion
Our data illustrate the negative impact the pandemic has had on overall colonoscopy volumes and training. Encouragingly, it does appear that the impact is lessening as we adapt to new ways of working. Safeguarding endoscopy training is essential to allow GI trainees achieve and maintain competency in endoscopy and to provide a steady stream of trained endoscopists to support healthcare systems in their efforts to regain lost ground and move forward.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the local research ethics committee at the Mater Misericordiae University Hospital, Dublin (ref. CA21-075).
References
Footnotes
Contributors CC reviewed the literature, collected data and drafted the manuscript. JC collected data and drafted the manuscript. NMF, ER, TD, DG and SM collected data. BK, SS, JL and CL were involved in endoscopy training throughout the pandemic and measures to support endoscopy trainees. CL supervised data collection and drafted the manuscript and is the guarantor. All authors approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.