Article Text

Statistics from Altmetric.com
Clinical presentation
A 54-year-old woman presented with a 1-week history of a rash starting in her feet. This was associated with arthralgia and myalgia. Her bowel habit was initially unchanged; however, she developed bloody diarrhoea shortly after admission to the hospital. She had no constitutional symptoms. Her medical history included myocardial infarction, hypothyroidism and a pituitary cyst.
On examination, there was a widespread non-blanching rash affecting her legs, feet, trunk, arms and palmar creases (figure 1). She had no fever or signs of meningism. Her abdomen was soft and non-tender. Laboratory tests revealed raised inflammatory markers (WCC 19.1×109/L and C reactive protein 84 mg/L). Lactate was normal (1.1 mmol/L). Haemoglobin was 167 g/L; platelet count and coagulation profile were normal. Renal function and a vasculitis screen were unremarkable. Stool cultures were negative. Urine dipstick was negative for protein.

Medical photography of purpuric rash affecting the limbs.
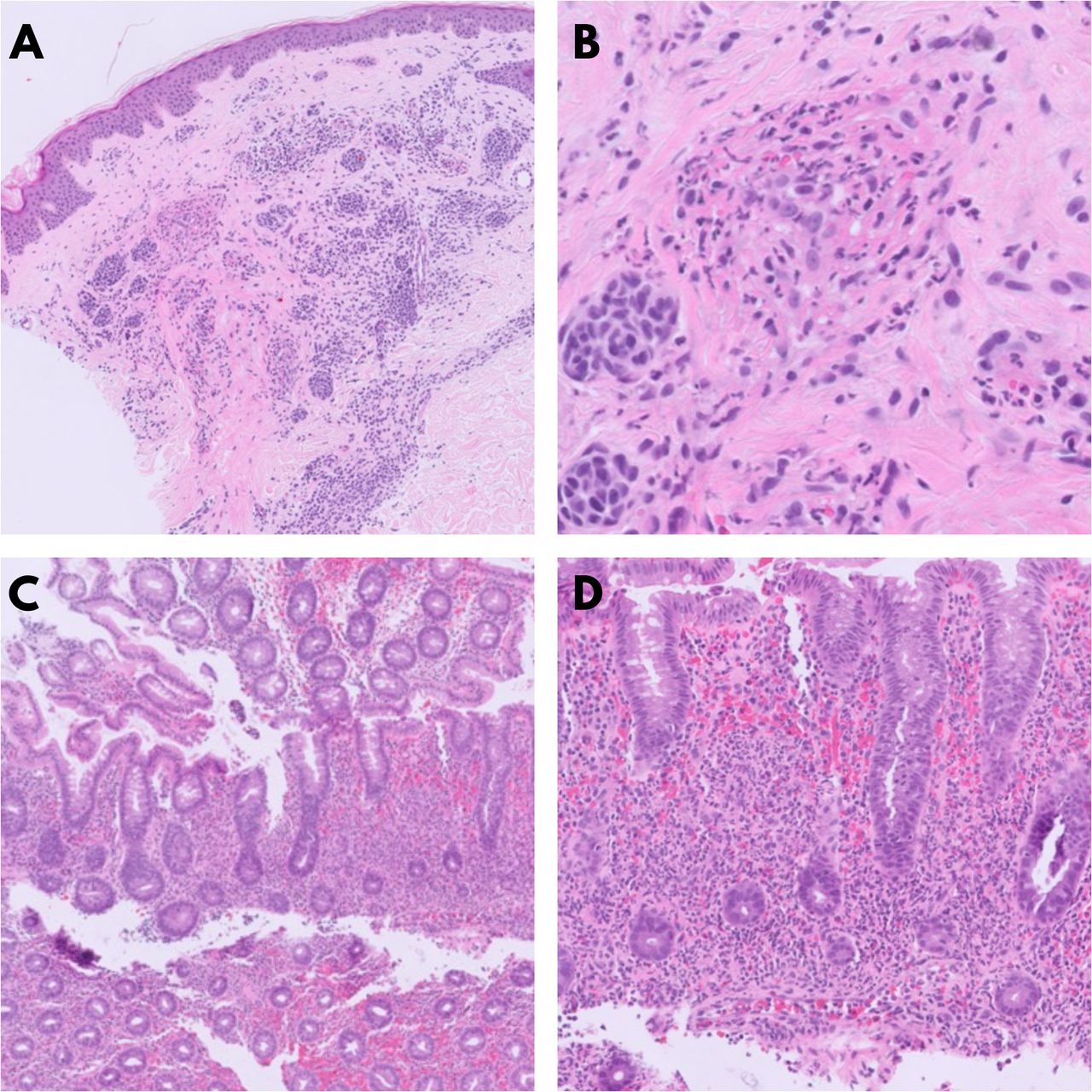
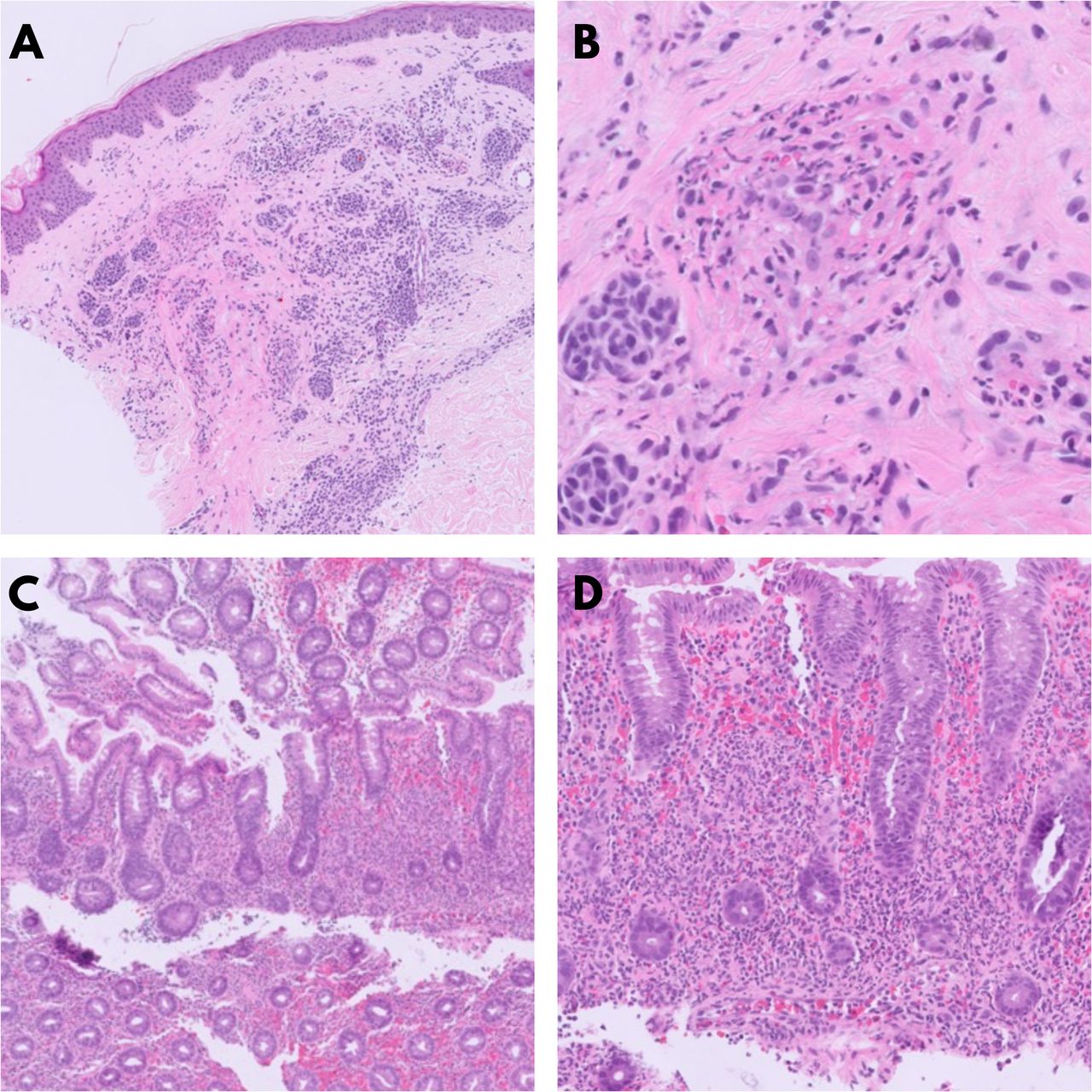
A CT scan of the abdomen revealed extensive inflammation extending from the distal ileum to the distal transverse colon. Flexible sigmoidoscopy showed purpuric lesions and patchy colitis (figure 2). Biopsy of the rash demonstrated acute perivascular inflammation and red cell extravasation (figure 3A,B). Biopsies of the large bowel showed focal cryptitis and an acute neutrophilic inflammatory infiltrate within the lamina propria (figure 3C,D).

(A) Endoscopic view of the splenic flexure. (B) Endoscopic close-up view of the purpuric lesions in the splenic flexure. (C) Endoscopic view of patchy colitis in the distal descending colon. (D) Endoscopic view of patchy colitis in the proximal sigmoid colon.
{kind=link}
{kind=link}
{kind=link}
(A) Histological examination of skin biopsy showing perivascular dermal inflammation admixed with an intradermal naevus. (B) Skin histology showing perivascular inflammation and fibrinoid necrosis of a vessel wall. (C) Colonic mucosa specimen showing acute inflammation and withered crypts within the lamina propria. (D) Acute neutrophilic inflammation with red cell extravasation in the lamina propria.
Question
What is the diagnosis? How would you treat it?
Answer
Histological description of skin biopsies is consistent with leucocytoclastic vasculitis, which is diagnostic of IgA vasculitis (formerly known as Henoch-Schönlein purpura) in the right clinical context. European League Against Rheumatism (EULAR) 2010 revised criteria1 for IgA vasculitis requires the mandatory presence of purpura and one of the following four: abdominal pain, supporting histopathology, arthralgia/arthritis and renal involvement. IgA vasculitis is the most common type of vasculitis and usually affects children; however, it is more severe in adults.2
Gastrointestinal manifestations are seen in 50%–75% of patients, including diffuse abdominal pain, vomiting and rectal bleeding.3 Biopsy helps confirm the diagnosis, but negative biopsy does not exclude the disease.4 EULAR guidelines 20195 on IgA vasculitis recommend considering corticosteroids in severe gastrointestinal symptoms;however, the evidence is limited to case series. Recommended doses are 1–2 mg/kg/day for oral prednisolone and 10–30 mg/kg for pulsed IV methylprednisolone, depending on severity. Our patient received intravenous hydrocortisone before the diagnosis was clear and completed reducing prednisolone course with excellent clinical recovery. Differentiating IgA vasculitis from other causes of acute bloody diarrhoea such as inflammatory bowel disease has long-term implications. We highlight the clinical features of the disease with gastrointestinal involvement and advocate endoscopic examination in hospitalised patients.
Ethics statements
Patient consent for publication
Footnotes
Contributors GK collected data, produced answer/discussion section of the manuscript, prepared figures 1 and 2, edited the manuscript and approved the final version. RC collected data, produced question/clinical presentation section of the manuscript, approved the final version. DM planned the project, revised and edited the manuscript and approved the final version. RGB prepared the histology slides and corresponding figure 3, provided commentary, edited the manuscript and approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.