Article Text

Statistics from Altmetric.com
Biological therapy has been introduced in the late nineties and has significantly improved outcome of many chronic inflammatory conditions such as rheumatoid arthritis, spondylarthritis, Crohn's disease and ulcerative colitis (UC), psoriasis and psoriatic arthritis. The loss of efficacy of biological therapy over time, however, has proved to be the Achilles heel of this treatment. Loss of response is in most cases due to neutralising antibodies and low trough levels. Other reasons for lower response rates theoretically include other immune pathways driving the inflammation or absence of residual lesions although no studies have systematically investigated the reasons for loss of response in a consecutive cohort of patients. Mainly in patients with symptoms but no signs of inflammation in the blood, new imaging is recommended to rule out other reasons for loss of response such as symptoms due to irritable bowel syndrome, bile salt malabsorption and/or underlying strictures.1 ,2
Loss of response due to immunogenicity is usually managed clinically by decreasing the interval between infusions or injections, by increasing the dose, by adding immunomodulatory agents (methotrexate, azathioprine) or by switching within the same class to more humanised or human antibodies. However, these therapeutic interventions are often done in vain, only leading to higher costs and a potential increasing risk for side effects. Thus, despite interventions, a significant proportion of patients still drop-out per year.3
A drug can only exert its full effect when the lowest level (ie, level measured just before the next scheduled administration of medicine (=also called trough level (TL))) is sufficiently high. Thus optimal use of the drug implies the correct dosage which also means that peak levels and average levels should not exceed concentrations which are associated with increased toxicity. Therapeutic drug monitoring (TDM) with measurements of TL at regular intervals is routinely carried out in the treatment with small molecules. Surprisingly this TDM is still not used routinely to optimise treatment with therapeutic antibodies to biological targets. Furthermore, immunogenicity of the therapeutics causes patients to develop anti-drug antibodies (ADA) which leads to a decrease of the active drug concentration and to the formation of drug-antibody complexes taken up by liver and spleen enhancing drug clearance.
A number of retrospective studies have demonstrated that in patients suffering from chronic inflammatory bowel diseases under anti- tumour necrosis factor (anti-TNF) treatment, sustained good anti-TNF TL are associated with better mucosal healing rates and a better long term outcome and will lead to a better quality of life, less disease-related surgeries and less hospitalisations.4–7
Preliminary evidence suggests that high TL might also correlate with side effects: high levels were seen in anti-TNF treated patients who developed skin manifestations as psoriasiform eczema and in patients who developed arthralgia.8 ,9 Moreover, lowering the dose in patients with supratherapeutic levels could lead to less side effects and a lesser cost for the healthcare payer. Nonetheless, comparative randomised prospective trials should be conducted to prove that TDM results in a treatment benefit the patients. To our knowledge, only one group, active in the field of arthritis, published a small (n=32) prospective study in which the infliximab (IFX) dose of refractory spondylarthritis patients was adapted based on TL and ADA measurements.10 They observed a trend towards an inverse relationship between IFX TL and the Bath ankylosing spondylitis disease activity index. Our group initiated in August 2011 a randomised prospective TL monitoring study with real-time therapeutic adaptations (trough level adapted infliximab treatment scheme (TAXIT)) in which 275 Crohn's Disease/ulcerative colitis patients under IFX maintenance therapy were included.11 Patients in TAXIT were first dose optimised to a TL between 3–7 µg/ml before randomisation to either a control arm in which treatment scheme adaptations are made based on clinical grounds (symptoms, C-reactive protein) or an active arm in which treatment scheme adaptations are done according to a developed algorithm with the aim to keep all patients in the 3–7 µg/ml TL window. The latter implies both increases as well as decreases of the dose and frequency of the infusions. The study has a duration of 12 months from randomisation onwards. The primary aim is to assess the impact of personalised TDM and dose optimisation on clinical and biological remission rates after 12 months. Secondary aims include safety, efficacy and tolerability issues. More prospective studies (eg, Tailorix, an investigator-initiated multicentre study from Holland, Belgium and France) are underway.
Another issue that needs to be addressed is the comparability of assays and the utility of general reference values. A number of groups have developed different types of assays (ELISA, bridging ELISA, Radio-immuno assay (RIA), mobility shift) to determine TL as well as ADA levels.12 All assay formats have their merits and disadvantages. A good comparison between the different assays is currently lacking. Recently, a round robin experiment was performed in which 36 samples from patients treated with IFX and 26 IFX calibration samples were analysed both in the Laboratory for Pharmaceutical Biology of KU Leuven (ELISA (TL) and bridging ELISA (ADA)) and at Sanquin, Amsterdam, the Netherlands (ELISA (TL) and RIA (ADA)) revealing a very good correlation between IFX TL and ADA levels. The samples were also analysed in Groningen using the commercially available LISA-TRACKER Premium IFX kit (BMD Biomedical Diagnostics, Marne La Vallée, France). Using the LISA-TRACKER, detectable TL were measured in six quality control samples that did not contain IFX demonstrating the discrepancy between different platforms and the need for standardisation (paper submitted for publication). The recently-introduced fluid-phase mobility shift assay can measure ADA in the presence of drug. A recent study presented at this year's Digestive Diseases Week showed that in a cohort of >1.400 maintenance samples, approximately 10% were positive for both ADA and TL.13 An interesting finding was that an association with high C-reactive protein (CRP) was seen in these samples, suggesting that when high CRP is seen during maintenance IFX therapy and good TL are found, the knowledge of ADA would be important. At this stage, confirmation of these findings is needed before the mobility shift assay can be widely recommended over ELISA and/or RIA.
Although the values obtained with the different assays are not fully comparable yet, we have two reasons to argue why TDM of therapeutic antibodies should be performed and dosing regimen should not be based on weight only: (1) the pharmacokinetics of therapeutic antibodies vary highly across individuals due to patient characteristics (eg, genetic background), disease features (eg, high vs low inflammatory burden) and use of concomitant drugs and (2) due to the immunogenicity of the therapeutic antibodies it is important to determine if undetectable TL are associated with antibody formation. Moreover, two independent groups have recently shown that in some patients antibodies to IFX can disappear over time14 and might induce an acute severe infusion reaction.2 ,15
A recent post hoc analysis of ACCENT1 re-analysed the sustained response rates in function of week 14 serum IFX TL.16 In patients with sustained response, the median week 14 IFX TL was 4.0 μg/ml and in patients without sustained response, it was only 1.9 μg/ml (p=0.0331), suggesting that measuring trough level (TL) early after induction has a prognostic value. Based on receiver operating characteristic (ROC) analysis, a week 14 IFX TL of 3.5 μg/ml discriminated best the sustained response with sensitivity, specificity, positive and negative predictive value of 0.54, 0.72, 0.39 and 0.82, respectively.
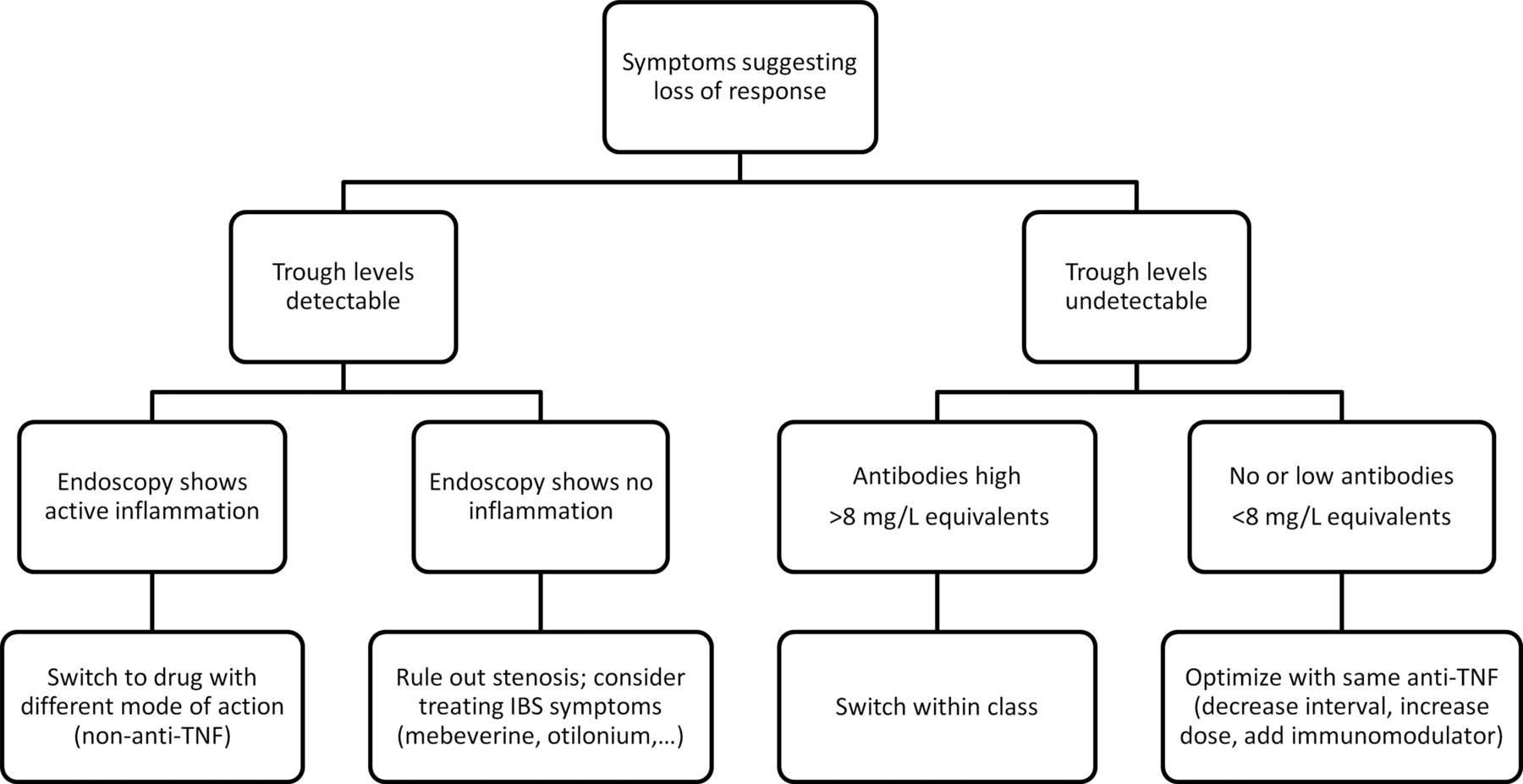
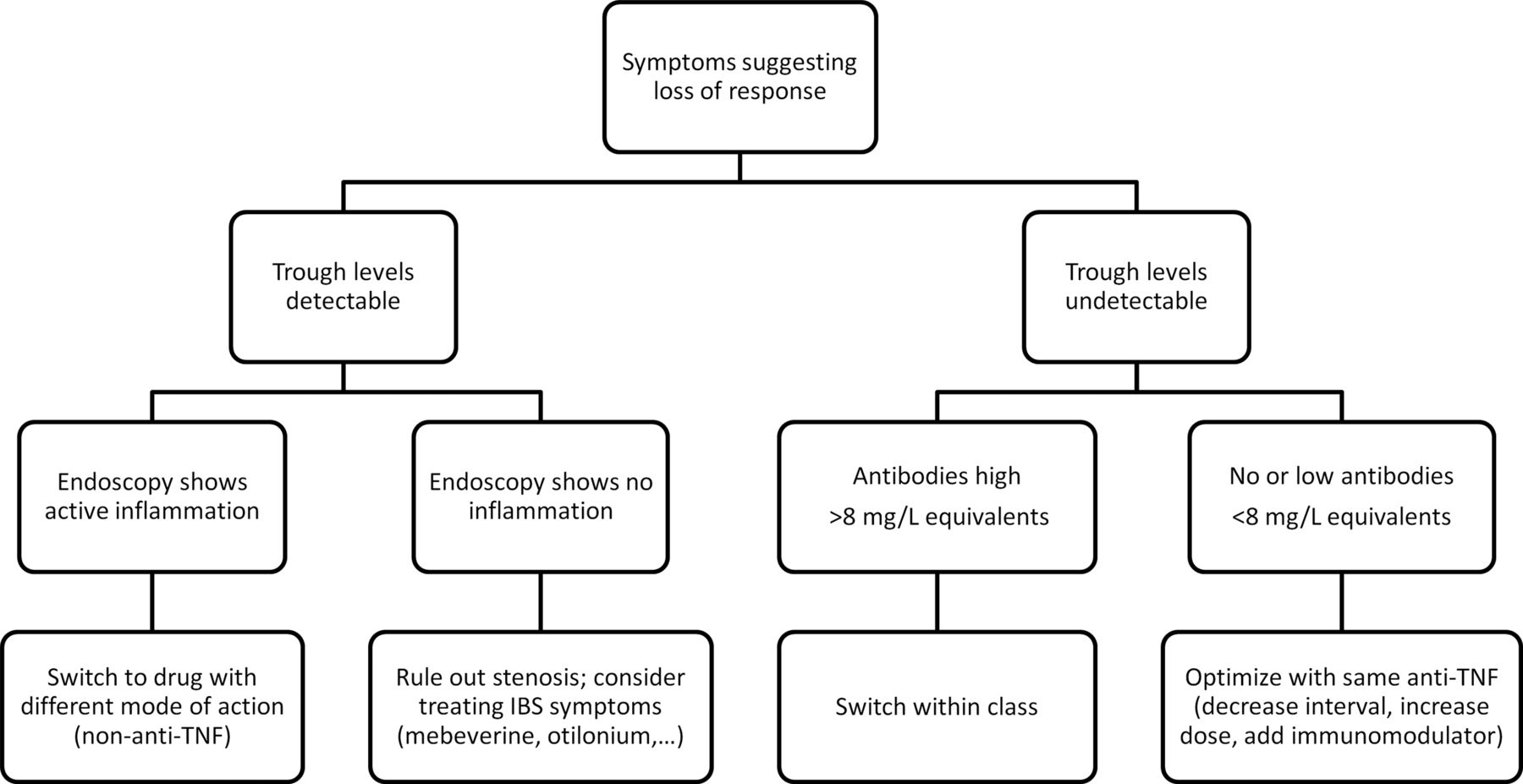
At present, without data to support that measuring levels in the absence of symptoms is cost effective, routine measurements of TL and ADA levels cannot be recommended. However, based on the data from ACCENT I, we do recommend to measure TL early after induction and to optimise already early on if needed. We further recommend—if feasible—to collect serum samples at regular time points in order to analyse consecutive serum samples when patients do report a decreased response. When patients treated with anti-TNF are reporting symptoms, determining TL and, when no TL are detected, measuring ADA, is helpful. As proposed in figure 1, patients with undetectable TL and low ADA should be optimised with the same drug. The most efficient way of dose optimisation (decreasing interval, increasing dose, adding immunomodulator) is unclear at present.17 Patients with undetectable TL and high ADA however, should be switched within class. In the case of symptoms with adequate TL, endoscopy should be checked, and if lesions are confirmed, therapy should be stopped and a switch to a drug with a different mode of action, if at all possible, is the preferred option. A wide implementation of TL and ADA determinations in clinical practice however, requires a rapid assay that is standardised, validated and easy to interpret and an algorithm to follow.
{kind=link}
Algorithm in patients under anti- tumour necrosis factor (anti-TNF) who present with symptoms suggestive of loss of response.
References
Supplementary materials
Test
Footnotes
-
Contributors Both authors fulfil the criteria of authorship and are responsible for the overall content as guarantors.
-
Competing interests SV has received research grants and served on the speaker's bureau of Centocor, MSD, Abbott and UCB. AG has received speaking fees from MSD and Pfizer.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Open Access This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/