Article Text

Abstract
Objective Alcohol-related admissions are increasing. A significant number of these admissions are attributable to a small number of complex patients with other comorbidities who do not engage well with mainstream services. Assertive outreach teams have been used in the field of psychiatry to engage patients who are poorly compliant. This study examines whether an alcohol assertive outreach team (AAOT) can engage with this group and reduce hospital admissions.
Design The AAOT is a multidisciplinary team with medical, psychiatric, substance misuse, psychology, nursing and social work specialists. The team worked with patients with the highest number of alcohol-related admissions and case managed in a community setting for 6 months. The admission and emergency department attendances of the cohort were compared for the 3-month period before and after the intervention. Christo inventory for substance misuse services (CISS) scores were determined pre and post the intervention period.
Results 54 patients were case managed. The total number of admissions in 3 months fell from 151 prior to the intervention period to 50 following the intervention. Emergency department attendances also fell from 360 in 3 months to 146 following the intervention period. CISS scores fell from 11 preintervention to eight postintervention.
Conclusions An AAOT model appears to reduce hospital admissions and emergency department attendances in a complex group of patients that display high alcohol-related admissions.
- Alcohol
- Health Economics
- Psychology
- Quality Of Life
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
Introduction
In the UK NHS, a continued rise in alcohol-related admissions is clearly seen. The current costs for alcohol-related admissions in England are estimated at £1.2 billion.1 Within this general rise, there is a cohort of patients who frequently attend the emergency department and have high levels of repeated hospital admissions. This group have complex physical health, psychiatric and social needs, but the most common factor is high levels of alcohol use.2 Within this group, there are a high proportion of ‘dual diagnosis’ patients: those with both mental health and alcohol problems. Unfortunately, they do not interact well with mainstream services and higher death rates are seen.3
Previous studies have looked at strategies to impact patients who are frequent attenders at emergency departments. Patient care plans have been used to reduce emergency department attendances with mixed results.4–6 These plans involve a specific management plan that is implemented when the patient attends the emergency department. Case management strategies have also been used.7 ,8 This involves an ongoing clinical interaction which extends beyond the hospital into the community. Case management involves multidisciplinary teams usually comprising psychiatric, social work, substance misuse, nursing and medical specialists.
In mental health services, assertive outreach teams have become well established in the last 2 decades. These are multidisciplinary teams which work with people with complex health needs, drug, alcohol, mental health and housing issues. They have been shown to be effective in patients with high levels of inpatient bed use.9 These teams are commonly targeted at people who engage poorly with services. Assertive outreach teams are typically defined by workers with a low caseload, usually 10 patients per worker, assertive engagement mechanisms and a high proportion of contact within the community.10 Recent work has demonstrated the use of assertive treatment methods to improve engagement in alcohol services and to improve rates of patients entering recovery.11
In view of the high levels of alcohol-related admissions seen in the North West of England, the North West Chief Executives’ Challenge, led by David Dalton and other experts, developed strategies to improve the quality of alcohol care. The two initiatives modelled were the development of an alcohol assertive outreach team (AAOT) and a 7-day alcohol specialist nurse service.12 An AAOT was developed to work with two separate cohorts of patients. The first group are patients with alcohol-related liver disease who are increasingly using hospital services and exceed the threshold of two admissions wholly attributable to alcohol. The second group is the ‘Top 30’ patients with the highest number of alcohol-related admissions. The aim of this study is to establish whether an AAOT is an effective model for reducing hospital admissions and emergency department attendances in the top 30 most frequently admitted patients.
Methods
The study was carried out between January 2011 and July 2012 at the Salford Royal NHS Foundation Trust. This is an inner city hospital in the North West of England. The study was a retrospective cohort analysis of the effects of assertive outreach methods on the admission rates pre and post the intervention period. The AAOT comprised a consultant in emergency medicine, a consultant psychiatrist specialising in addiction disorders, an emergency department nurse, a social worker, a psychologist, an alcohol worker, a support worker and an administrator.
In the UK, a national audit system exists to record the number of alcohol-related admissions to each hospital. Each patient admission is coded objectively and an alcohol attributable fraction is attributed. A database was created to identify the adult patients with the highest number of alcohol-related unscheduled care admissions. The top 30 patients were identified and they were case managed by the AAOT. There were no exclusion criteria. Patients were case managed for a period of 6 months; after this time the database was refreshed. A new cohort of patients was then case managed for the subsequent 6 months.
To case manage the patients, case profiles were initially formed by information gathered from the patient, the acute trust, mental health trust, community alcohol team, primary care services, council and criminal justice services. Individualised plans were then developed and implemented. The face-to-face interaction as part of the case management was organised in the community away from the hospital. This involved a highly personalised response to the patient's needs. Common strategies were fast access to alcohol detoxification; appropriate referral to outpatient specialities and support in getting there; alcohol and psychological support; facilitating housing solutions; and robust responses to violence and aggression. A part of the case management involved the production of individual care plans that would be implemented when a patient attended the emergency department. The plans were immediately available to the emergency department staff at the point of triage and helped produce a consistent coordinated response whenever patients interacted with the hospital. The patients were intensively case managed for a period of 6 months. Assertive outreach approaches were used including repeat phone calls, letters and home visits. The team also performed a liaison function and coordinated responses with other services.
The primary outcome measure was the number of admissions per month in the 3-month period immediately before and after the 6 months of case management intervention. Emergency department attendances were also recorded during these periods. At the start and end of the 6-month case management period, Christo inventory for substance misuse services (CISS) scores were calculated.13 This is a subjective score that reflects a patients social functioning, psychological and general health, compliance, drug and alcohol use and criminality. The score is a 0–20 score, with lower scores reflecting better outcomes (above 11 reflects high problem severity). The score has been previously validated.13
Ethics approval was not required as this study fulfils the criteria for service evaluation. Statistical analysis was performed with non-parametric statistical analysis as the CISS scores, admissions and attendance rates were not normally distributed. Medians are quoted and the Wilcoxon rank sum test was used for comparing effects between groups.
Results
The team was established and began to case manage patients in April 2011. Due to delays in fully establishing the team, only 24 patients were case managed in the initial cohort. A further 30 patients were case managed in the 6-month period starting in October 2011.
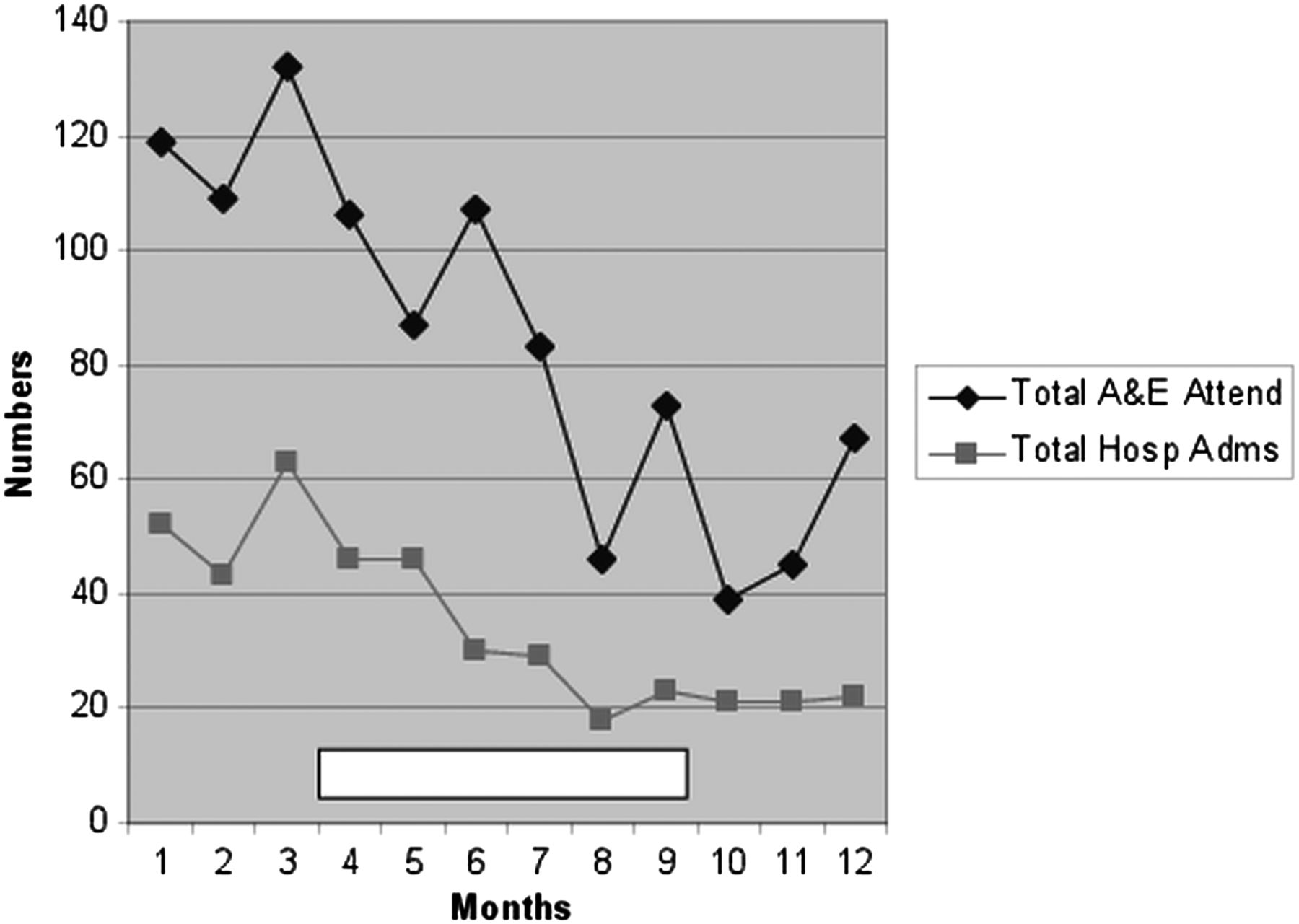
A significant reduction in hospital admissions was seen in the 3 months following case management as compared with the 3-month period immediately prior to the start of case management. The total number of hospital admissions were 151 prior to case management, reduced to 50 following the case management period (w=2070, p<0.001). A similar significant reduction was also seen in the total number of emergency department attendances in the 3-month periods before and after intervention (360 reduced to 146, w=2215, p<0.001). The time scale of effect is seen in figure 1.
{kind=link}
Monthly admissions and attendances. The white bar represents the 6-month period in which the team actively case managed 54 patients.
There was a significant reduction in the CISS scores at the start as compared with the end of the case management period (median 11 reduced to 8, p<0.001). There were no deaths in the study group during the period of case management and up to 3 months after. However, one patient left the local area and contact was not able to be maintained. There was loss of engagement with a second patient who did remain within the local area.
Discussion
This study demonstrated that case management using the alcohol assertive outreach model can reduce emergency department attendances and hospital admissions. This study is unique in that the focus is on patients with high level of alcohol admissions rather than frequent emergency department attendances alone. While these groups share similar complexity, this is a slightly different cohort than the traditional group of emergency department regular attenders. Our pilot work demonstrated a lower level of homelessness in this group in contrast to our most frequent emergency department attenders. Our high admissions group had more stable accommodation and we were able to remain in contact and engage in the outreach aspect of the team's work. However, we had no exclusion criteria and homeless patients were included in the study.
A second reason for addressing a high admissions group rather than frequent emergency department attenders was the perceived cost benefit of reducing admissions rather than emergency department attendances alone. Based on national indicators and length of stay costs, an average alcohol-related admission costs a primary care organisation £1824 and an alcohol-related emergency department attendance costs £80.14 In the 3-month period after the end of case management alone, we demonstrated a reduction in admissions from 151 to 50. Taking into account the reductions in admissions and attendances seen during the first year of the team alone, the cost reductions cover the £300 000 required to establish the service. These initial cost reductions do not take into account any ongoing reduction in admissions and subsequent savings.
Previous studies using care plans and case management strategies have shown mixed outcomes in emergency department frequent attenders. Studies from the UK, Australia and the USA have all demonstrated reduction in emergency department attendances,2 ,4 ,5 ,8 ,15 but other teams have reported no benefit6 ,16 or even an increase in emergency department use.7 There is less evidence on the effects on admission rates. A UK study reported a good impact on admission rates,4 but this was not repeated in other healthcare systems. A US randomised control trial reported no impact on admissions with case management;8 however, increased admissions were seen in an Australian trial.7
Traditional clinical approaches to medical, alcohol and psychiatric disorders are effective when a single disorder is identified. Unfortunately, when complex comorbidity is present, patients tend to fall between the gaps between services and commonly present and are admitted to inpatient hospital beds. We found that through effective multidisciplinary working, the AAOT could more effectively support these complex individuals. The most important factor that increased the effectiveness of the team was the creation of an extensive case profile for each patient from a wide ranging variety of information sources. This permitted the team to plan effective interventions which supported the patient's medical, psychiatric, substance misuse and social difficulties in a coordinated fashion.
As with all projects that impact the frequent users of emergency departments, there has to be concern that patients are not simply being diverted to other emergency departments. This is true especially with homeless emergency department regular attenders who commonly move between areas. We lost communication with two of the cohort, both of whom were homeless. One undoubtedly had moved out of the area and was likely to have attended other emergency departments. The second patient remained within the local area but the team was not able to engage with him. For the rest of the patients, the ongoing community engagement allowed us to be confident that they remained within the locality of the hospital. Indeed, the reduction in the CISS scores that are demonstrated point to improved functioning and a reduction in problem severity. The postintervention CISS score remains high in comparison with other settings such as abstinence based treatment centres or outpatient alcohol services, but this reflects the severity of the cohort that this group comprises.
Assertive outreach is a UK term to refer to the North American assertive community treatment for psychiatric care. Implementation of this strategy in UK psychiatric care has seen inconsistent results. It is more successful when hospital use is high.9 Assertive approaches to engagement in UK community alcohol work have demonstrated to be beneficial. Passetti et al11 set up a clinic which targeted patients with a history of disengagement. They used an assertive approach and saw more people completing withdrawal treatment and entering an aftercare placement. We needed to modify the original model to adapt to our local application, but maintained the fidelity of the assertive approach.10 This was defined by a small caseload with 10 patients per worker, backed by a multidisciplinary team with psychiatry, nursing and substance misuse workers, and uses assertive engagement mechanisms and focuses on community engagement.
One limitation of this study is based on the design. We used a preintervention and postintervention comparison whereby all patients were used as their own control. Some of the effects could be attributed to a natural reduction in emergency department attendances and admissions over time. This effect has been previously noted in two US studies,6 ,8 but it is not a consistent effect with studies demonstrating no reduction16 or even an increase in emergency department attendance and admissions over time.7 A multicentre randomised controlled trial would be needed to adequately power a study to address this issue. However, this was not possible initially due to the novelty of the approach. We took a pragmatic approach in using a prestudy and poststudy to describe the effects of alcohol assertive outreach work in reducing admissions in this cohort. The main clinical findings of this study describe an AAOT approach to the support and management of a cohort of patients who demonstrate high numbers of alcohol-related admissions to a UK inner city hospital. This approach appears to reduce admissions, emergency department attendances and improves social functioning.
What is already known on this topic
-
A complex group of patients with high levels of repeat alcohol-related admissions are well recognised, but difficult to impact
What this study adds
-
An alcohol assertive outreach team can engage with this complex patient group and reduce hospital admissions
How might it impact on clinical practice in the foreseeable future
-
Alcohol assertive outreach teams provide a solution for reducing alcohol-related admissions in the highest users of inpatient services
References
Footnotes
-
Contributors Conception and development of the model: NRH, MS, AMD, JB, MW, SMD and DD. Conception and Development of the case management and care plan strategies: NH, NG, CS, HN, NRH, BM and AR. NRH is the guarantor and responsible for the overall content.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Open Access This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/