Article Text

Abstract
Patients with intestinal failure (IF) and home parenteral nutrition commonly develop abnormal liver function tests. The presentations of IF-associated liver disease (IFALD) range from mild cholestasis or steatosis to cirrhosis and decompensated liver disease. We describe the reversal of IFALD in an adult patient with IF secondary to severe Crohn's disease and multiple small bowel resections. The patient developed liver dysfunction and pathology consistent with IFALD. Multiple causal factors were implicated, including nutrition-related factors, catheter sepsis and the use of hepatotoxic medications. Multidisciplinary treatment in a tertiary IF referral centre included aggressive sepsis management, discontinuation of hepatotoxic medications and a reduction of parenteral nutrition dependency through optimisation of enteral nutrition via distal enteral tube feeding. Upon this, liver function tests normalised.
- CROHN'S DISEASE
- DRUG INDUCED HEPATOTOXICITY
- INTESTINAL FAILURE
- ENTERAL NUTRITION
- PARENTERAL NUTRITION
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Patients with intestinal failure (IF) usually require home parenteral nutrition (HPN).1–3 Although lifesaving, HPN carries an increased risk of complications, including catheter sepsis, venous thromboembolic disease and IF-associated liver disease (IFALD).3 ,4
The risk of liver pathology in IF is well recognised.5 Causal factors include sepsis, hepatotoxic drugs, gallstones, small intestinal bacterial overgrowth and nutrient-specific factors such as lipid amount or composition.5 Typically, adult patients with IF who develop liver dysfunction present with mild cholestasis or steatosis. This may progress to overt liver disease and eventually fibrosis and cirrhosis. IFALD remains a primary indication for small bowel transplantation.6 If recognised early and managed appropriately, IFALD is treatable and potentially reversible.
Here, we describe the multifactorial nature of IFALD and the normalisation of liver function tests in an adult patient with IF following multidisciplinary treatment, including optimisation of non-nutrient and nutrient-related factors.
Case presentation
A 25-year old man, diagnosed in 2003 with Crohn's disease, was referred to our IF unit following repeated small bowel resections, complicated by intra-abdominal sepsis and enterocutaneous fistulae. His final surgery in 2007 left him with 40 cm small bowel from the duodeno–jejunal flexure to a loop jejunostomy and 180 cm distal small bowel in continuity with the colon (figure 1). His short proximal segment left him highly fluid and calorie dependent. He was established on a PN regimen of five nights with 4 L glucose bags and two nights with 2 L 20% intralipid bags, each with 2400 kcal and 13.5 g nitrogen and appropriate electrolytes, vitamins and trace elements.

A diagram of the patient's intestinal anatomy (left) was drawn from barium follow-though imaging (right) and surgical notes from extensive bowel surgery with complications.
Cross-sectional imaging revealed multiple small bowel strictures distally to the loop jejunostomy (figure 1). In order to reduce PN dependency, strictures were dilated endoscopically, and medical treatment was intensified by adding methotrexate.
After 3 months follow-up, abnormal liver function tests led to termination of methotrexate and change of his HPN formulation from intralipid to clinoliec 20%, containing 80% refined olive oil and 20% soybean oil. During the following years, he was reviewed at his local hospital since he remained reluctant to further assessment for enteral nutrition or reconstructive surgery at our centre.
In February 2012, the patient presented with a fungal catheter infection and abnormal liver function tests and was readmitted. On admission, bilirubin was 96 μmol/L, alanine aminotransferase (ALT) 161 IU/L and alkaline phosphatase (ALP) 300 IU/L. Amphotericin B was given, and because line salvage in fungal line sepsis is rarely—if ever—successful,7 his central catheter was removed. Tests for viral and autoimmune hepatitis and cross-sectional imaging including magnetic resonance cholangiopancreatography were normal except for liver steatosis. A liver biopsy revealed focal interface hepatitis and perivascular cholestasis, consistent with IFALD.
Following central catheter removal and antifungal therapy, the patient was switched from clinoleic to SMOF lipid 20%, a mixture of soybean (30%), medium-chain triglycerides (30%), olive oil (25%) and fish oils (15%). With these multifactorial interventions, his clinical status, sepsis and liver function tests slowly improved. His course was complicated by cryptogenic Guillain Barré syndrome (GBS) requiring immunoglobulin treatment with a subsequent rise in ALT and bilirubin, the latter peaking above 200 μmol/L. Following recovery, distal end tube feeding (DETF) was introduced and gradually built up to 1800 mL Vital 1.5 (2700 kcal and 125 g protein) given over 18 h, with 30 mL saline flushes pre and post feed. After a gradual increase in flow rate, the patient ultimately managed an infusion rate of 100 mL/h over 10 h, allowing a decrease in his PN demands to 750 kcal with 9 g nitrogen in glucose bags only, with additional electrolytes to replace the fluid losses from his high-output proximal stoma. Levels of conjugated bilirubin, ALT and ALP normalised and remained within the normal ranges.
The patient gradually improved and was discharged on combined DETF and HPN. For immunosuppression, azathioprine was given via the distal limb, with concomitant thiopurine metabolite monitoring to verify absorption. When fully recovered from GBS, he will undergo reconstructive surgery in order to restore intestinal continuity.
Discussion
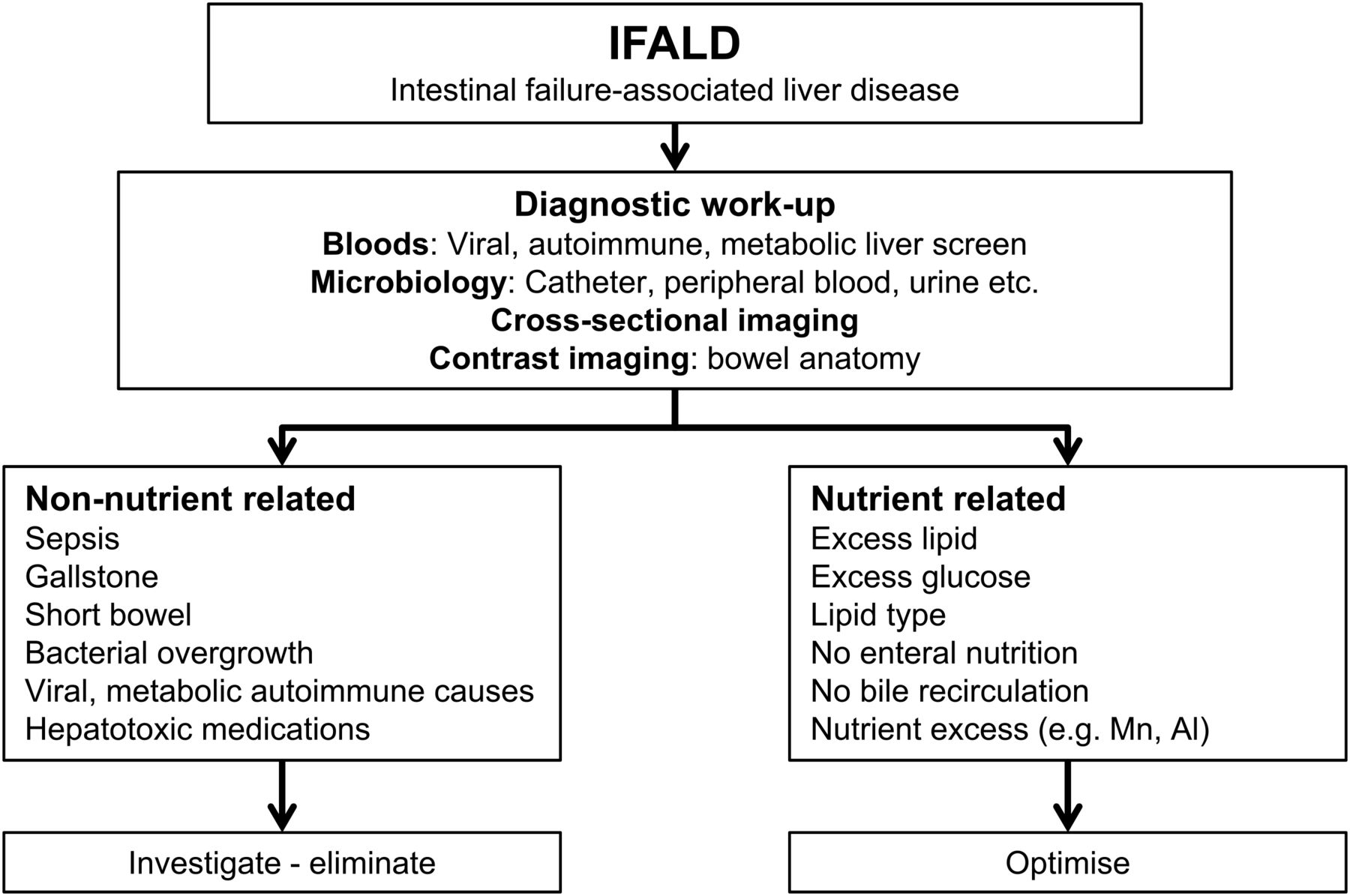
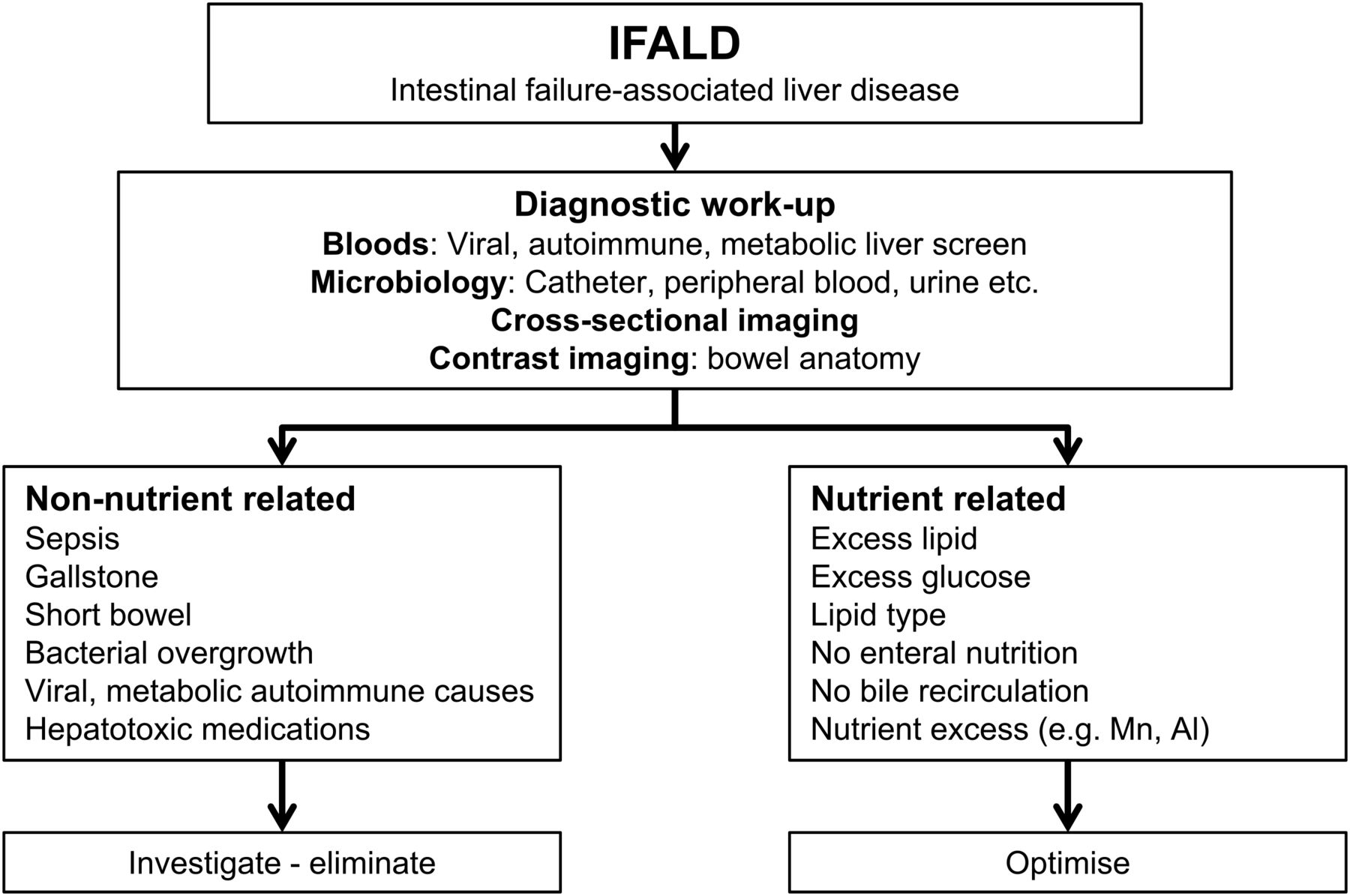
The multidisciplinary treatment of IFALD targets both non-nutrient and nutrient-related factors (figure 2). When treated proactively, IFALD is potentially reversible.
{kind=link}
{kind=link}
Important diagnostic investigations and non-nutrient and nutrient related causal factors implicated in intestinal failure-associated liver disease (IFALD).
Sepsis: The relation between sepsis and jaundice is well known.8 In patients with HPN, sepsis may explain up to half of the episodes of abnormal liver function tests.5 Because patients with HPN with relapsing sepsis frequently develop cholestasis, sepsis prevention and prompt management remain pivotal. In IF, sepsis is most often caused by catheter-related blood stream infections, and securing central catheter integrity is essential. Strict adherence to catheter care protocols, management by specialist nutrition teams, and maximal sterile barrier precautions all reduce the risk of catheter-related infections.9 In this patient, fungal line sepsis led to catheter removal.
Parenteral nutrition: Excess calorie feeding, from lipid and/or glucose, is associated with PN-related liver complications.10 ,11 Emerging data support the use of novel lipid emulsions with medium-chain triglycerides, monounsaturated fatty acids and fish oil. Several case series demonstrated improved liver function tests following the substitution of soybean-based lipids with fish oil-based preparations.12–14 Hybrid intravenous fats such as SMOF may provide a clinical benefit, as indicated by case series and small prospective studies.15 ,16
Enteral nutrition: Enteral feeding allows a reduction of the calorie load provided via PN17 and may help prevent IFALD development.18 It prevents gut atrophy and loss of gut mucosal immunity, thereby potentially preventing a microbiota imbalance which may promote endotoxaemia and hepatic injury.19 ,20 Obviously, enteral feeding requires a functional gastrointestinal tract. DETF, or fistuloclysis, requires 75 cm of viable small bowel and involves feed infusion via the distal limb of a loop stoma or enterocutaneous fistula. It allows the reduction of PN calories and may eventually replace PN in selected patients.21 The re-infusion of filtrated stoma content restores bile acid recirculation and is advocated by some authors,22 but it may be regarded impractical and was not necessary in this case.
Hepatotoxic drugs: Both methotrexate and thiopurines may increase ALT,23 ,24 but discontinuation should be balanced with the risk of relapse. In this patient, distal administration and metabolite monitoring allowed thiopurine dose optimisation.24 Antifungals may increase both ALT and bilirubin, and levels more than 3× for ALT or 2× for bilirubin usually define hepatotoxicity.25 Amphotericins and azoles cause similar degrees of hepatotoxicity, and careful dosing regimens and close monitoring are mandatory during antifungal treatment. In this patient, catheter removal was essential.
Underlying liver disease, notably bile duct pathology, may explain up to 24% of episodes with worsening liver function tests.5 Viral, autoimmune and metabolic liver disease should be considered in all patients and tests repeated when relevant.
In conclusion, IFALD is multifactorial and requires multidisciplinary treatment. Patients may benefit from care in a dedicated IF unit, and even advanced liver disease may be reversible.
References
Footnotes
Contributors CH participated in outpatient clinical review and wrote the manuscript. EN and KK participated in inpatient treatment and contributed to the manuscript. SH evaluated liver biopsy and participated in discussion of the patient's history and contributed to the manuscript. KF participated in inpatient treatment and contributed to the manuscript. AA participated in inpatient treatment, provided imaging copies, contributed to the manuscript. SL conceived the study, had overall responsibility for patient treatment, and contributed to manuscript.
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.