Article Text

Abstract
Alcohol consumption affects the risks of approximately 230 three-digit disease and injury codes in the International Statistical Classification of Diseases and Related Health Problems-10th Revision. The United Nations Sustainable Development Goals comprise 17 challenging goals with 169 targets, which the 193 Member States aim to achieve by 2030. Action to reduce the harmful use of alcohol, especially addressing global health inequalities, will contribute to achieving many of the health-related goals and targets. Alcohol care teams, mainly developed in acute UK hospitals, reduce acute hospital admissions, readmissions and mortality, improve the quality and efficiency of alcohol care, and have 11 key evidence-based, cost-effective and aspirational components. A clinician-led, multidisciplinary team, with integrated alcohol treatment pathways across primary, secondary and community care, coordinated alcohol policies for emergency departments and acute medical units, a 7-day alcohol specialist nurse service, addiction and liaison psychiatry services, an alcohol assertive outreach team, and consultant hepatologists and gastroenterologists with liver disease expertise facilitate collaborative, multidisciplinary, person-centred care. Quality metrics, national indicators, audit, workforce planning, training and accreditation support research and education of the public and healthcare professionals. Hospitals should collaborate with local authorities, public health, clinical commissioning groups, patients and key stakeholders to develop and disseminate cost-effective prevention and treatment strategies. Globally, alcohol care teams can support the achievement of the United Nations Sustainable Development Goals, and should be advocated and implemented through the WHO global alcohol strategy. This requires collaborative care planning by key stakeholders, a skilled workforce, targeted financial resources and dedicated political commitment.
- alcohol
- care
- teams
- alcohol strategy
- sustainable development goals
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known on this topic?
Alcohol care teams (ACTs), mainly developed in acute UK hospitals, reduce acute hospital admissions, readmissions and mortality, and improve the quality and efficiency of alcohol care.
Specialist alcohol care can pull people back from the brink of the devastating consequences of alcohol misuse, improve their health and well being and restore their dignity.
What this study adds
In the past decade, there has been a major increase in the number of ACTs in UK hospitals. However, many hospitals are not resourced to provide an optimal 7-day service. Moreover, there is a crisis in addiction services, which reach only 18% of the in-need dependent population in England.
The enhanced evidence-base for the 11 key components of the UK model ACT, including a lead clinician, co-ordinated prevention and treatment alcohol policies, alcohol specialist nurses, addiction and liaison psychiatry, outreach, and hepatology services, will be disseminated internationally.
Significance of this study
How might it impact on clinical practice in the future?
This study will support UK clinicians in developing business cases and also policy makers in the implementation of the 2019 NHS Long Term Plan for England, which aims to roll out ACTs in NHS hospitals.
This study makes 14 key recommendations for global implementation of ACTs, to be advocated and implemented through the WHO global alcohol strategy, and support achievement of the United Nations Sustainable Development Goals, especially to reduce health inequalities.
Global context
Alcohol consumption affects the risks of approximately 230 three-digit disease and injury codes in the International Statistical Classification of Diseases and Related Health Problems-10th Revision.1 2 Alcohol use causes three million deaths per year, and is responsible for 5.1% of the global burden of disease expressed in disability-adjusted life years.3 In September 2015, the 193 United Nations Member States adopted a set of Sustainable Development Goals (SDGs) to end poverty, protect the planet and ensure prosperity for all.4 These consist of 17 challenging goals with 169 targets to try to achieve by 2030.4
Alcohol is specifically mentioned under health target 3.5:
3.5 Strengthen the prevention and treatment of substance abuse, including narcotic drug abuse and harmful use of alcohol.
3.5.1 Coverage of treatment interventions (pharmacological, psychosocial and rehabilitation and aftercare services) for substance use disorders.
Europe has the highest consumption, but Africa bears the heaviest burden of disease and injury.3 Harm per litre is greatest for poorer drinkers and their families.5 6 Action to reduce the harmful use of alcohol will contribute to achieving many SDGs and targets, especially SDG 10, which aims to reduce health inequalities.
UK context
Alcohol care teams (ACTs) were defined in a 2010 publication by the British Society of Gastroenterology, Alcohol Health Alliance UK and the British Association for the Study of the Liver, which made key evidence-based recommendations for integrated primary, secondary and community alcohol care, based around a typical UK district general hospital, serving a population of around 250 000.7
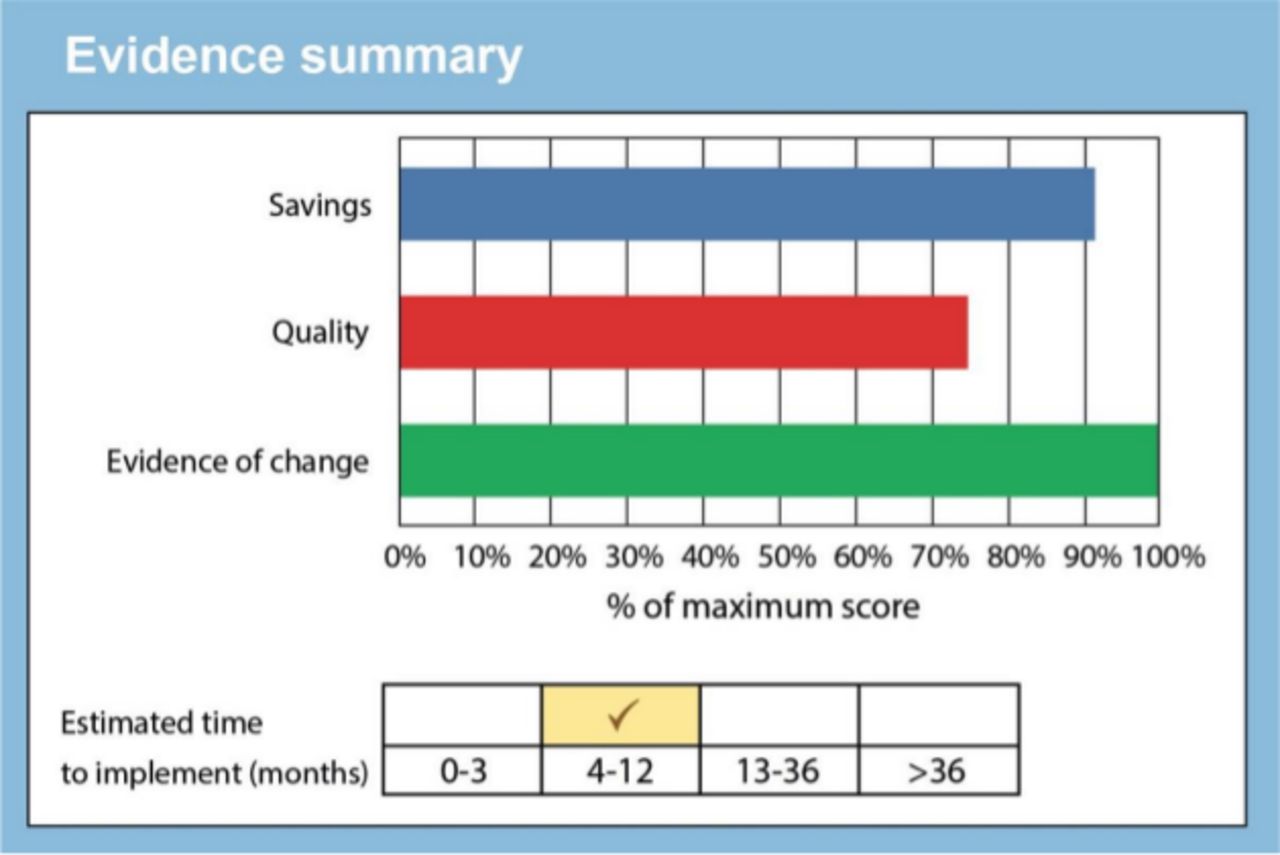
In 2011, NHS Evidence and the National Institute for Health and Care Excellence (NICE) commissioned the lead author to publish a Quality, Innovation, Productivity and Prevention (QIPP) case study on the role of ACTs in reducing hospital admissions, readmissions and mortality. NICE scored the QIPP highly on savings, quality and evidence of change, and estimated that hospitals could implement an ACT in 4–12 months (figure 1). Subsequently, the evidence base has been updated in four iterations of this QIPP, most recently in 2016.8

The NHS Evidence and National Institute for Health and Care Excellence Quality, Innovation, Productivity and Prevention case study scores for savings, quality, evidence of change and estimated time to implementation of an alcohol care team.8 NHS, National Health Service.
The 2019 NHS Long Term Plan for England aims to roll out ACTs in NHS) hospitals.9 The comprehensive UK model ACT comprises 11 key components (box 1).7 8 10 This review provides the evidence base for these components, and also makes key recommendations for global implementation of ACTs to support achievement of the SDGs.
Alcohol care team: key components of the UK model
A clinician-led, multidisciplinary alcohol care team, with integrated alcohol treatment pathways across primary, secondary and community care
Coordinated alcohol policies for emergency departments and acute medical units
A 7 day alcohol specialist nurse service
Addiction and liaison psychiatry services
An alcohol assertive outreach team for frequent hospital attenders
Specialist consultant hepatologists and gastroenterologists with expertise in liver disease
Collaborative, multidisciplinary, person-centred care
Quality metrics, national indicators and audit
Workforce planning, training and accreditation
Research, education and health promotion for the public and healthcare professionals
Formal links with local authority, public health, clinical commissioning groups, patient groups, and other key stakeholders
ACTs: key components of the UK Model
A clinician-led, multidisciplinary ACT, with integrated alcohol treatment pathways across primary, secondary and community care
Each acute hospital should establish a multidisciplinary team, led by a consultant hepatologist, gastroenterologist, psychiatrist, emergency department (ED) or acute medicine physician, or nurse. The ACT should collaborate across hospitals, primary, secondary and community care to develop integrated alcohol treatment pathways and prevention programmes and expertise to local and national policy makers.
One acute UK hospital established a model ACT. Around 50% of the gastroenterology ward inpatients had alcohol-related problems, mainly alcohol-related liver disease (ARLD). Historically, there were the traditional two consultant gastroenterologist ward rounds per week. However, since 2009, the consultants have devoted 2-week blocks solely to inpatient care. Daily consultant ward rounds and multidisciplinary meetings (Monday to Friday) were commenced. Subsequently, gastroenterology ward inpatient mortality was reduced from 11.2% to 6.0%, and the length of stay from 11.5 to 8.9 days, with a 37% increase in ward discharges.11 A 7-day service has since been established.
Primary care
In Bolton, UK, large-scale screening of the adult population, using the short Alcohol Use Disorders Identification Test (AUDIT-C) questionnaire,12 has been ‘systematically applied’ and ‘industrially-scaled’ to ask all adult patients about alcohol consumption, facilitating early identification and appropriate treatment of problem drinkers.13
The Lancet Commission on Liver Disease in the UK prioritises early detection and treatment of liver disease, since most patients currently present with advanced disease and cirrhosis.10 A liver nurse in primary care practices, using case finding, serum liver fibrosis markers and transient elastography, yielded increased new diagnoses of liver disease, with virtual review by a consultant hepatologist.14
Identification and Brief Advice and Brief Intervention
Identification and Brief Advice (IBA) is a single-session intervention, lasting 5–15 min,15 16 involving alcohol screening and structured brief advice. It requires minimal training and can be delivered by a healthcare or related professional. IBA can use the AUDIT-C, followed by the full AUDIT12 when the AUDIT-C is positive.
Brief Intervention (BI) is delivered empathically by trained staff in a single or several sessions. The motivationally based sessions take 20–40 min, and aim to help people to reduce consumption and risk-taking behaviour, or to consider abstinence. BI is recommended for hazardous and harmful drinkers, who have not responded to IBA, or for those requesting support in reducing consumption. However, the evidence base for IBA and BI has some limitations.17
In primary healthcare in the UK, Europe and the USA,18–22 and in ED settings,23 IBA reduced harmful alcohol consumption and had a high cost-effectiveness ranking in 25 US primary care services evaluated.24 Electronic IBA can be effective and reach large populations.25–27
Integrated alcohol treatment pathways between primary, secondary and community care
Integrated alcohol treatment pathways describe the nature and anticipated course of a personalised, planned treatment, driving the shift from secondary to community care.28
Coordinated alcohol policies for EDs and acute medical units
St Mary’s Hospital, London designed the 1 min Paddington Alcohol Test (PAT), and trained ED staff to identify and deliver IBA to patients presenting with an alcohol-related problem, ‘The Teachable Moment’.29 Referrals to their alcohol specialist worker (ASW) for BI increased 10-fold, with a 43% reduction in alcohol consumption. Every two BIs resulted in one fewer reattendance during the following 12 months.30 If appointments were offered on the same day, two-thirds attended, but if delayed for 48 hours only 28% attended.31
In 2012, the Rapid Access to Alcohol Detoxification Acute Referral (RADAR) service developed a pathway, across all 12 Greater Manchester EDs, to deliver rapid 168 hours per week transfer of suitable patients, to a bespoke alcohol detoxification, intervention and aftercare programme. In the first 2 years, RADAR transferred 636 patients and 95% completed detoxification. Independent evaluation estimated savings of £1.30 million per year in healthcare costs alone.32
A 7-day alcohol specialist nurse service
Alcohol specialist nurses (ASNs), unlike ASWs without nursing skills, can manage patients with liver disease and other comorbidities, and achieve accreditation to prescribe medications, especially for detoxification. In the Royal Bolton Hospital, four ASNs, with a blend of alcohol, liver and mental health expertise, provide collaborative, holistic inpatient and outpatient care.33
In Nottingham, an ASN-led service, compared with conventional physician-led care, improved the health outcomes of patients admitted for detoxification and for alcohol-related cirrhosis. Admissions were reduced by two-thirds. In the detoxification cohort, 36.4 bed days per month were saved. In the cirrhotic cohort, bed occupancy was reduced from 6.3 to 3.2 days per month. Clinical incidents were reduced by 75%, and gamma-glutamyl transpeptidase abnormalities halved (figure 2).34

{kind=link}
{kind=link}
Impact of ‘nurse-led’ alcohol care team compared with conventional ‘physician-led’ care on (A) self-reported alcohol intake and (B) the liver enzyme gamma-glutamyl transpeptidase (gamma GT), showing halving of alcohol intake and liver damage. 34Reproduced from Ryder SD, Aithal GP, Holmes M, Burrows M, Wright NR. Effectiveness of a nurse-led alcohol liaison service in a secondary care medical unit. Clin Med 2010; 10:435-40. Copyright © 2010 Royal College of Physicians. Reproduced with permission.
Systematic screening of 50 000 acute medical admissions, by trained general nurses, using a modified electronic PAT, identified ‘high risk’ patients. Further ASN assessment showed that 81% of these had a high dependency score, with frequent ED attendances and admissions, and a greater likelihood of ARLD.35
The NHS national Commissioning for Quality and Innovation scheme, which includes an alcohol metric that incentivises identification of alcohol use disorders, was implemented in secondary care in 2018–2019.36 For 2019–2020, hospitals receive financial reimbursement for screening 80% of adult inpatients, with 90% of those identified as drinking above low risk given IBA or offered specialist referral. ASNs can train staff to achieve these targets.35
Addiction and liaison psychiatry services
Addiction psychiatrists provide substance misuse services mainly in specialist psychiatry units. Liaison psychiatrists treat hazardous and dependent drinkers in acute hospital and community settings. Addiction and liaison services can link in hospitals and the community by providing psychosocial interventions, relapse prevention work, education and training. However, there are no agreed, standardised addiction or liaison services to acute hospitals. Collaborative psychiatry and medical links facilitate assessment, especially of drinkers with ARLD and cognitive impairment.33
The Birmingham Rapid Assessment, Interface and Discharge (RAID) liaison psychiatry service delivered a 24-hour, 7-day service, and a comprehensive range of mental health specialties. Alcohol-related problems comprised 13% of their study population.37 In the Birmingham City Hospital, the RAID service closed 60 of the 600 beds, through linking patients to appropriate community care pathways. The internal review estimated financial savings of £4–£6 million per year. The London School of Economics estimate was £3.55 million per year.38
Public Health England (PHE) has evaluated the public health burden of alcohol and performed an evidence review of the effectiveness and cost-effectiveness of alcohol control policies.39 40 ACTs were a cost-effective option for NHS Sustainability and Transformation Partnerships to reduce harm.41 Moreover, ACTs, IBA, alcohol assertive outreach teams (AAOTs) and specialist treatment for dependent drinkers were cost-effective; every £1 invested brings an annual return of £3, which rises to £26 over 10 years.42 Psychosocial interventions for dependent drinkers can save the overall UK economy £5 for every £1 invested.43
An alcohol assertive outreach team for frequent hospital attenders
The pioneering Salford AAOT comprised medical, psychiatric, substance misuse, psychology, nursing and social work specialists. The AAOT case-managed 54 complex, poorly compliant ‘frequent attenders’ in community settings for 6 months. Hospital admissions were reduced by 67%, and ED attendances by 59%, with savings of £607 000 and patients moved into supported, community environments. The team also works proactively with patients who have had two recent alcohol-related admissions, the so-called ‘fast risers’.44
In England, 9% of people with alcohol dependence account for 59% of all alcohol-attributable hospital admissions.45 These 54 369 patients accounted for 365 000 admissions and 1.4 million bed days, costing £848 million.45 A randomised controlled trial of an AAOT showed, after 6 months, an increase in abstinent days from 14% to 68%, and inpatient bed days reduced from 26.8 to 1.2, compared with controls.45 The roll-out of AAOTs to care for these 54 369 patients has an estimated implementation cost of £161 million, with cost savings of around £575 million, the return on investment being £3.42 for every £1 spent.45 This compares favourably with screening and brief intervention, with a saving of £1.23 for every £1 spent.45 The rate of high-need, high-cost hospital attenders is strongly correlated with the Index of Multiple Deprivation (r=0.74).46 AAOTs can reduce health inequalities, address dual diagnosis and homelessness, and in-reach into prisons.47
In the USA, outreach services increased primary care use among homeless veterans.48 One Canadian shelter-based programme for homeless drinkers stabilised alcohol intake and decreased ED visits and police encounters.49 In Canada’s indigenous communities, outreach healthcare teams improved engagement through education.50
Specialist consultant hepatologists and gastroenterologists with expertise in liver disease
Lancet Liver Commission in the UK
In 2013, the National Confidential Enquiry into Patient Outcome and Death ‘Measuring the units: a review of patients who died with alcohol-related liver disease’ strongly advocated the establishment of ACTs in all acute UK hospitals to address the major deficiencies in acute and critical care of the more than 50% of patients who died.51 Consequently, in 2014, the Lancet Liver Commission was established and published a blueprint for future standards of excellence in healthcare for patients with liver disease, including ARLD.10 Subsequently, there have been four annual progress reports.13 52–54 Key recommendations include that acute hospitals should have a ‘liver champion’ and ASNs with liver and psychiatry expertise.
Collaborative, multidisciplinary, person-centred care
Collaborative care is a multidisciplinary team approach to assessing, planning, implementing and evaluating care, together with the patient and family.33 The episode of care is developed around an anticipated length of stay. Patients are empowered to make lifestyle changes, especially regarding alcohol consumption. The initiative involves hospital, community, voluntary and social services (box 2).
Collaborative, multidisciplinary, person-centred care
Key elements of the Royal Bolton acute UK hospital model.
A lead alcohol clinician, specialist consultant gastroenterologist and hepatologist, and addiction and liaison psychiatry teams provide joint inpatient and outpatient care.
A daily, specialist consultant-led, multidisciplinary meeting, with all healthcare professionals writing in the same notes.
Daily consultant gastroenterologist/hepatologist input to the acute medical units and wards facilitates the rapid triage and clinical and endoscopic management of liver and gastroenterology emergencies, and transfer to gastroenterology and critical care wards.
Four alcohol specialist nurses, with a blend of alcohol, liver and mental health expertise, with daily input to the emergency department, acute medical units and wards.
Access to Brief Intervention within 24 hours of detection of alcohol-related problems.
Alcohol specialist nurses supervise detoxification regimens throughout the hospital, guiding ward nurses and doctors about medication regimens, risk management, assessment of capacity, safeguarding and Deprivation of Liberty Safeguards.
Telephone hotline, rapid access for general practitioners and primary care healthcare professionals, patients, families and carers, to the alcohol specialist nurses, secretaries or ward, nurtures a close relationship.
Alcohol specialist nurse-led, day-case admissions for drainage of ascites.
A social worker facilitates discharge to an appropriate environment, especially for the homeless, rough sleepers and patients with alcohol-related brain damage, including Wernicke-Korsakoff syndrome, for whom there is a major shortage of suitable long-term care.
Close liaison with regional liver and national liver transplant units, especially about escalation of care for patients with acute and severe liver disease.
End-of-life care discussions with the multidisciplinary team prior to sensitive and personalised conversations with the patient, family or carers.
Close working relationships with regional addiction psychiatrists who provide inpatient psychiatric care in residential settings.
Unified and seamless primary, secondary and community alcohol care.
Joint ‘One-Stop’, outpatient clinics, by a consultant, alcohol specialist nurse and psychiatry team member can unify care and reduce non-attendance (DNA) rates.
Partnership with link and community workers to overcome the alcohol stigma, especially in our ethnic communities.
Health promotion, education, training, audit and research.
Transparent, no-blame clinical governance meetings.
Quality metrics, national indicators and audit
These should include mandatory targets, and systematic service evaluation by commissioners, providers, patients, families and carers. Managed clinical networks establish databases which capture activity and outcomes. The Royal College of Physicians of London has established an accreditation scheme for hospital care, Improving Quality in Liver Services.55
Workforce planning, training and accreditation
The Secretary of State at the Department of Health and Social Care (DHSC) has identified workforce concerns. A qualified workforce is essential to recovery56 and a predictor of success.57 The PHE enquiry into the reduction in numbers of people in alcohol treatment found that integration of alcohol and other drug services had led to non-specialist staff delivering treatment interventions, and to alcohol specialists, with mixed case loads, having less time to deliver effective alcohol interventions.56 Health professionals must be trained and accredited to provide joined-up services.
A Royal College of Psychiatrists survey found a 60% reduction in addiction psychiatry trainees, compounded by insufficient training frameworks, between 2006 and 2016.58 Competent addiction workers, clinical psychologists59 and social workers60 are essential. Health Education England, PHE and the DHSC should develop an Alcohol Workforce Strategy, alongside the National Alcohol Strategy, just as the Mental Health Workforce Strategy accompanied the Five Year Forward View for Mental Health.61
Alcohol and other drugs’ core competencies for healthcare professionals
Modular training, with assessment and accreditation of competencies in alcohol, other substance misuse and addiction, must be developed. PHE and the Royal College of Nursing (RCN) published an excellent guidance for commissioners, providers and clinicians on the competencies and potential roles for nurses in alcohol and other drug treatment.62 The Department of Health and RCN also published a competence framework for liver specialist nurses.63 Encouragingly, 13 UK medical and surgical colleges and faculties developed a consensus on core competencies in knowledge, skills, behaviour and attitudes, to be incorporated into postgraduate curricula.64 Undergraduate curricula are introducing similar training.
Research, education and health promotion for the public and healthcare professionals
Research
There needs to be a UK research programme into the causes, prevention and treatment of alcohol use disorders, especially ARLD.7 13 52–54 Acute, non-teaching hospital ACTs should partner with teaching hospitals in recruiting patients for clinical trials.
Education and health promotion of the public and healthcare professionals
Education programmes must address low levels of public and government awareness of alcohol-related disease and injury. Many people, including doctors, are judgemental, viewing alcohol as a taboo, ‘self-inflicted’ lifestyle choice, rather than a disease, often prejudicing treatment, employability and social standing, and exclusion from a place of worship.65 One ACT has partnered link and community workers, organising patient fora to address this stigma.33
Formal links with local authority, public health, clinical commissioning groups, patient groups and other key stakeholders
Close partnerships should be established, comprising commissioners, providers and users of alcohol, and liver and bloodborne viruses’ services, to optimise commissioning arrangements, care pathways, and prevention and treatment strategies.8
In January 2019, the Liverpool Centre for Alcohol Research was launched. The University of Liverpool, Liverpool John Moores University, Clinical Research Network North West Coast, and Liverpool Health Partners, which represents nine primary and secondary care organisations, cocreated a centre focusing on the development and application of research and innovation in alcohol-related disease. This aims to better understand the drivers and consequences of alcohol misuse, develop new treatments, interventions and policies, and to become a world-leading research centre, which will improve population health locally, nationally and internationally. This venture is a paradigm for future collaborative initiatives.
Alcohol care teams in the UK
In 2001, the Royal College of Physicians of London Working Party produced a seminal evidence-based blueprint, introducing the concept of ACTs, and making key recommendations for acute hospitals receiving unselected alcohol-related admissions, national policy, research and education.66 In 2008, 78% of the costs of alcohol to the NHS were incurred by hospitals, inpatient costs alone accounting for 45%.67 Alcohol causes a major burden in four areas, crime and social disorder, families and family networks, the workplace, and health. PHE estimated the annual cost in England to be between £27 billion and £52 billion.39 ACTs are cost-effective in all four areas.
Since 2010, there has been a major increase in the number of ASNs and lead alcohol clinicians in UK hospitals. In a 2009 survey in London hospitals, only 42% had ASNs and 10% a clinician lead.68 In 2016, 83% of UK hospitals had ASNs.13 However, many hospitals are not resourced to provide an optimal 7-day service. Since 2014, PHE has collated data on ASNs and ACT clinician leads.69 In 2019, around 60% have a clinician lead.
Public Health Post-2013,70 published by the House of Commons Health Select Committee, shows how local authorities have undergone cuts to public health budgets year-on-year, after assuming responsibility from the NHS. The paper includes a survey, commissioned by the Association of Directors of Public Health, which shows that local alcohol and drug treatment services face the biggest public health cuts of all. The Commons Committee highlighted the government’s pledge to reduce health inequalities and that these cuts would undoubtedly increase inequalities. NHS England recommends that local authorities, clinical commissioning groups (CCGs) and provider trusts should jointly fund alcohol services. In June 2019, the Secretary of State at the DHSC reaffirmed that the primary responsibility will remain with local authorities. Lack of agreement over funding responsibilities presents a major threat to the ongoing provision of specialist hospital alcohol services, especially when local authorities are forced to make further budget cuts. The NHS Long Term Plan emphasises that the health inequalities funding supplement, paid to CCGs, can be used for the development of ACTs. The Wales Liver Plan has funded ACTs, clinical leads and ASNs.13
In England, between the periods 2013–2014 and 2017–2018, there was a reduction of 18% in local authority funding for addiction services, 12% in the number of people in contact with specialist alcohol treatment and 19% in the number of new patients presenting for treatment.71 Services currently reach only 18.3% of the in-need dependent population.72 In 2016–2017, the ratio of F10 alcohol admissions to treatment access was best in Scotland (1.1), with Wales (1.2), England (2.4) and Northern Ireland (3.9).54 Funding streams must ensure equity of access.
ACTs and potential global impact
In 2016, many developing countries had no written alcohol policy, 80 countries had written national policies, 8 had subnational policies, while 11 banned alcohol completely.3 73 The non-communicable disease action plan ‘best buys’ include the provision of brief psychosocial interventions for persons with hazardous and harmful alcohol use.74 75 However, treatment coverage for alcohol dependence is unknown in most countries and varies considerably worldwide. Encouragingly, there has been significant progress in the delivery of IBA and BIs in primary care settings, although this was mainly in the more affluent countries.3
However, while the United Nations SDGs and WHO Global Status Report on Alcohol and Health 2018 describe cost-effective alcohol policies relating to pricing, taxation, marketing regulation of availability and licensing,3 there is no mention of the major potential role of multicomponent, multidisciplinary ACTs to reduce global alcohol-related harm. This review makes 14 key recommendations for global implementation of ACTs (box 3). Implementation, depending on national and local priorities, developmental levels, capacities and resources to address the needs of specific communities, at local, regional, national and international levels, would play a major role in achieving the SDGs.
Alcohol care team: key recommendations for global implementation
Each country should appoint a government minister and ministry, ideally the Department of Health, with overall responsibility for public health advocacy, and obtaining the resources to implement cost-effective alcohol policies, prevention and treatment interventions, and integrated care pathways to support the achievement of the United Nations Sustainable Development Goals by 2030.
Each country should appoint a national clinical alcohol champion, who would be directly accountable to, and collaborate with, the ministry, with the remit to establish a network of the appropriate and realistic components of the UK model alcohol care team.
Each district should appoint a community lead to train and support healthcare workers in delivering Identification and Brief Advice.
Digital technology with smartphones should be rolled out to reach geographically remote areas and communities.
Alcohol specialist nurses should be trained to establish clinical and community networks, and provide clinical leadership, mentoring, live video and digital communication, with regular visits to support healthcare leads in their communities.
Addiction psychiatry services should be established, especially to address the stigma associated with addiction and mental health comorbidity.
Assertive outreach healthcare services, with the appropriate skill mix to provide medical and social care, including for people with alcohol problems, should be established, especially in the most isolated geographical communities.
Regional alcohol and hepatology clinical champions should be appointed to implement and oversee service delivery and development.
Collaborative care planning to address the medical, psychiatric and social aspects of alcohol-related harm should be established at national, regional and local levels.
Monitoring and surveillance of key indicators to identify the impact of alcohol policies and interventions must be a national priority.
Workforce planning, training and continuing professional development for generic and specialist healthcare workers must be established and resourced.
National and international research partnerships should be established to assess cost-effective interventions and to train healthcare workers in research methodology.
Education and health promotion campaigns, at all levels, should specifically address the alcohol-associated stigma, and highlight the additive and synergistic harmful effects of alcohol with bloodborne viruses, obesity and smoking.
Partnerships between developed and developing countries should be established, with dedicated resource provision and bidirectional exchange schemes to identify and train future leaders, and to share mutual expertise and skills.
The WHO, United Nations, non-governmental organisations, governments and healthcare organisations must prioritise and implement cost-effective alcohol control measures and interventions. Unfortunately, failure is the norm, due to lack of financial and workforce resources, geographical inaccessibility, engrained drinking cultures, or limited political will and commitment of governments, influenced by strategic, global lobbying and marketing from the alcohol industry.3 The Institute for Fiscal Studies Deaton Review highlights that ‘inequalities exist not just in income and living standards, but in wealth, health, family environments, life chances and political influence’.76 One cause for deep concern is a rise in ‘deaths of despair’, a term coined by Case and Deaton,77 to include deaths from suicide, drug and alcohol overdose, and ARLD.
Alcohol care, both prevention and treatment, especially addressing inequalities, is a barometer for the health of a nation and also for the commitment of governments to public health, nationally and globally.
Alcohol care and ACTs are evidence-based and cost-effective, and are enhanced by their person-centred, qualitative and aspirational components. They are also a wise and compassionate investment, with potential, profound, long-lasting financial and humanitarian benefits to individuals and societies. Specialist alcohol care can pull people back from the brink of the most devastating consequences of alcohol misuse, improve their health and well-being, and restore their dignity.
Acknowledgments
The author is grateful to Ms Paula Elliott and the librarians at Bolton NHS Foundation Trust for the literature search and checking of references, and to Andrew Powell for the figures.
References
Footnotes
Contributors KJM conceived the review and is the sole author.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- UpFront