Article Text

Statistics from Altmetric.com
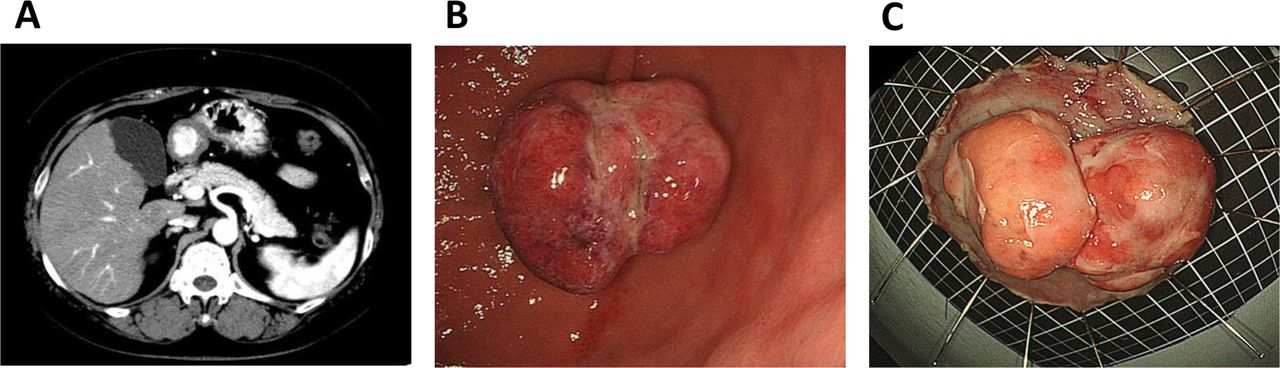
A 60-year-old woman was referred to our department for an incidental finding of gastric polypoid lesion on enhanced CT (E-CT) (figure 1A). She had a medical history of hepatocellular carcinoma (HCC) treated 3 years prior with transcatheter arterial chemoembolisation. E-CT is routinely performed once a year for the surveillance post HCC therapy. No obvious recurrence was detected in the liver. Upper gastrointestinal endoscopy revealed a 30 mm pedunculated gastric polypoid lesion on the greater curvature of the antrum (figure 1B).

CT scan revealing a gastric hypervascular tumour in the stomach (A). Upper gastrointestinal endoscopy showing a 30 mm pedunculated gastric polypoid lesion on the greater curvature of the antrum (B). Endoscopic submucosal dissection was performed for pedunculated polypoid lesion resection (C).
All blood test results were nearly normal: haemoglobin, 11.2 g/dL; platelets, 125 000/mm3; bilirubin, 0.7 mg/dL; aspartate aminotransferase, 51 U/L; alanine aminotransferase, 39 U/L; alkaline phosphatase, 166 U/L; gamma-glutamyl transpeptidase, 32 U/L; and prothrombin index, 98%; alpha-fetoprotein, 62 ng/mL; des-gamma-carboxy prothrombin, 37 mAU/mL. The hepatitis C virus had been eliminated 6 months before this examination and the test for hepatitis B virus was negative. Endoscopic ultrasonography revealed a heterogeneous and hypoechoic internal echo. There was no obvious tumour invasion into the muscular layer. Therefore, endoscopic submucosal dissection (ESD) was performed for pedunculated polypoid lesion resection (figure 1C).
Question
What is the diagnosis?
Answer
Gastric metastasis from HCC.
Histological analysis after ESD revealed pedunculated gastric metastasis from HCC (figure 2A) with CK20 (+) (figure 2B), hepatocyte (+) (figure 2C), and CK7 (−), ly (+), v (+), HM0 and VM0; hence, anticancer therapy was initiated. She was discharged 5 days postoperatively.

{kind=link}
{kind=link}
Histological findings after endoscopic submucosal dissection revealed pedunculated gastric metastasis from hepatocellular carcinoma (A) with CK20 (+) (B), hepatocyte (+) (C).
Gastric metastasis from HCC is extremely rare. In most of those cases, gastric metastasis was detected using CT,1 upper gastrointestinal bleeding2 or autopsy.3 In this study, we accidentally detected a gastric hypervascular tumour in the stomach using dynamic CT (figure 1A). Regarding the transfer form to the stomach from the liver, direct invasion was mainly detected. Patients with gastric metastasis often undergo surgical resection-121 or transcatheter chemoembolisation.2 In our case, the shape of the gastric metastatic lesion was unusual: the pedunculated polypoid type. The patient also underwent ESD, since the depth of invasion seemed submucosal on the pre-ESD endoscopic ultrasonography. This lesion was solitary metastasis and serum AFP level became normal after ESD. No obvious recurrence was detected in this lesion 6–12 months following ESD.
To our knowledge, this is the first report wherein ESD was performed for pedunculated gastric metastasis from HCC. Our case suggests that an enhanced gastric tumour after HCC treatment could be metastasis from HCC and a careful approach is essential to prevent gastrointestinal bleeding.
Ethics statements
Patient consent for publication
Acknowledgments
The authors thank Kyoko Oura and Tomoko Tadokoro for the technical assistance.
Footnotes
Contributors AM and JT treated a patient and collected data. AM wrote a draft and TM revised it.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.