Article Text

Statistics from Altmetric.com
Introduction
July’s Twitter debate took place in the aftermath of record-breaking temperatures in the UK, part of a worrying trend which brings the need to consider the environmental impact of our practice into sharp focus. The data are stark: the healthcare sector is responsible for 4.4% of all greenhouse gas emissions worldwide.1 The NHS was the first health system in the world to commit to net zero targets, aiming for net zero emissions by 2040 with an 80% reduction between 2028 and 2036.
Gastroenterology has been at the forefront of the drive for sustainability, with the British Society of Gastroenterology (BSG) Climate Change and Sustainability Strategy launched in November 2021,2 and the BSG conference hosting its first Sustainability Symposium in 2022. The BSG has moved to decarbonise its financial investments and to set up paperless working processes in its offices. While endoscopy is an obvious source of waste production in gastroenterology practice, there are other areas that are also ripe for green overhaul. We brought together experts in the field to discuss how we might bring about change and how to embed sustainable processes in our places of work.
Conferences
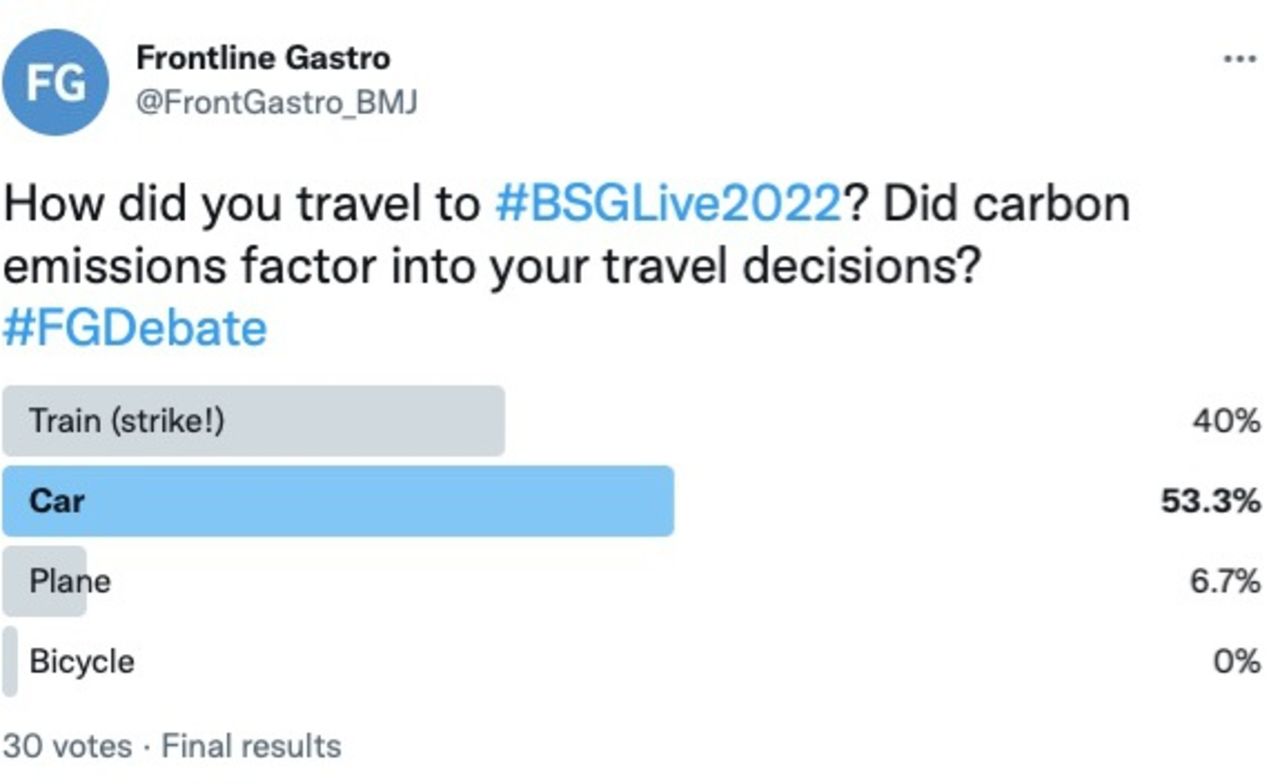
After the COVID-19 restrictions had been lifted, many were relishing the prospect of networking with colleagues from across the UK at BSG 2022, but is the waste generated by face-to-face conferences justifiable? In studies modelling the travel to Canadian national gastroenterology conferences, the average CO2 emitted per delegate was 0.54 tonnes, equivalent to over 250 OGDs!3 While the distance travelled for UK delegates is likely to have been shorter, rail trikes put a spanner in the works for many when it came to travelling to Birmingham this year, with 53.3% (16/30) poll respondents reporting they travelled by car (figure 1). If the results of this small poll are representative of the 1943 in-person attendees, this represents over 1000 car journeys, with a mile driven by car roughly equivalent to a mile flown in terms of CO2 emitted. Of course, many British gastroenterologists also travel regularly to international conferences.

A poll of mode of travel to BSG Live 2022.
Most participants in the debate strongly felt that the value of a face-to-face conference was sufficient to warrant travel, though many respondents still felt the option of a hybrid meeting was a desirable hangover of the changes brought about by COVID-19. If large in-person conferences continue, it is vital that we offset the wastage.
The BSG demonstrated a strong commitment to sustainability considerations in planning BSG Live 2022, choosing a venue with a ‘zero to landfill policy’, ensuring that all packaging would be recycled and any leftover food donated.4 With as much as half of catered food typically ending up in landfill,5 these are important concerns. A move to a plant-based diet is widely accepted as a straightforward measure to reduce emissions, and 56.7% (17/30) of the participants polled in our #FGDebate would be satisfied with an entirely plant-based culinary offering at future conferences (figure 2). Additional measures taken by the BSG included ensuring minimal conference material were produced, with a non-plastic lanyard, and increasing reliance on technology rather than paper handouts to help delegates navigate the event. International speakers were invited to present virtually rather than travel to the conference.

{kind=link}
{kind=link}
A poll of dietary preferences at gastroenterology conferences.
Endoscopy
Endoscopic activity is clearly a significant producer of waste, estimated to be within the top three biggest waste-producing healthcare practices by procedure.6 A US-based study found that the average amount of waste generated by each endoscopy procedure was 2.1 kg.1 For a typical 10-point endoscopy list, the waste generated would dwarf the waste produced by a patient spending 24 hours in intensive care (estimated to be 3.37 kg/bed/day).7 With 2.1 million endoscopy procedures performed in the UK in 2019, this would translate to a staggering 4.4 million kg waste each year. Recognising the importance of addressing this, the Joint Advisory Group has now included sustainability metrics in the Global Rating Scale for endoscopy units.
In studies of waste disposal, 64% of endoscopy waste typically ends up in landfill.1 Only 9% was recycled, despite 48% of waste being potentially recyclable. Improper waste segregation also contributes significantly to CO2 production, with high-temperature incineration of 1 tonne of waste generating approximately 1 tonne of CO2. Ensuring considered waste disposal requires buy-in from hospital waste disposal teams as well as training of endoscopy unit staff. Unfortunately, recycling options for contaminated clinical waste remain extremely limited, although there are processing methods which can significantly reduce the risk of biological contamination of single-use endoscopy instruments, rendering them recyclable.6
Simple measures to reduce waste include distributing paperwork electronically where possible and printing double-sided if absolutely necessary. Working with local pathology services to develop protocols which reduce the number of biopsy pots required for multiple samples can have a significant impact, as the amount of CO2 produced in the manufacture of three biopsy pots is roughly equivalent to driving two miles in an average petrol car.8 Manufacturers of endoscopy equipment also have an important role to play in terms of reducing packaging volume and using recycled materials. It is worth checking with local suppliers to see whether single-use items, such as biopsy forceps, can be returned to the manufacturer for component recycling.
Importantly, the biggest waste is an unnecessary endoscopic procedure; vetting all referrals to ensure they are clinically necessary and useful is essential. A process whereby patients can have scans the same day for newly diagnosed cancers or incomplete procedures can save on patient travel. Similarly, in some circumstances, an alternative test may be considered appropriate, for example, faecal calprotectin to monitor inflammatory bowel disease activity in place of a colonoscopy.9 A summary of measures to consider to improve your endoscopy unit’s green credentials is presented in box 1.
A summary of measures to consider in improving your endoscopy department’s green credentials
Steps to creating a sustainable endoscopy environment
Create a dedicated ‘sustainable endoscopy’ team with accountability.
Involve the Endoscopy Users Group, link nurses, Green Champions, waste management teams.
Recycle non-patient-contact materials.
Choose sustainable equipment, for example, consumables made from recycled materials.
Distribute reports electronically where possible.
Where there is a need to print, use recycled paper and print double-sided.
In collaboration with pathology, develop local protocols for biopsies which minimise pot usage.
Consider water usage: is local tap water quality sufficient replace bottled sterile water for flushing?
Lobby industry for recyclable packaging and reuse equipment where possible within infection control measures.
Streamline patient pathways to allow same-day endoscopy where possible.
Telemedicine follow-up of endoscopy results.
Reflecting on personal choices
Climate change has been described as the ‘biggest global health threat of the 21st century’,10 and as healthcare professionals, it is our business to reduce the burden of disease. Do we, therefore, have a moral obligation to consider the climate impact of decisions we make in our personal lives? Several participants in the Twitter debate described a number of changes they had made to their daily routines, including commuting by public transport or cycling, making the decision to eat less meat or the purchase of an electric car. In line with this, a recent survey of gastrointestinal leaders demonstrated that 49% had made changes towards sustainability in their personal lives.11
The choices we make in our home lives are mostly dwarfed by the carbon footprint of our healthcare and work choices, with the notable exception of air travel. Flying accounts for approximately 2.4% of global CO2 emissions per year—more than the contribution of many individual countries.12 The demand for flying is also highly unequal, with 70% of flights in the UK taken by just 15% of the population. It has been estimated that committing to taking no more than one short-haul return flight every 3 years or one long-haul flight every 8 years would have a huge impact on the demand for air travel and could stall the contribution of flying to global temperature increases. Perhaps it is time to reconsider that weekend city break?
Despite the necessary changes needed by governments and industry, research suggests that to meet targets for reducing global warming, a huge and immediate reduction is needed by those who are comfortably off. Making change does not have to be either/or, and personal shifts can collectively have a massive impact. As gastroenterologists, what is good for the environment can also be good for us and for our patients, with studies consistently demonstrating that reducing meat consumption and increasing dietary plant fibre fosters a healthy gut microbiome13 and can reduce the risk of developing diverticulitis.14
Conclusion
As health professionals, we have a vital role in mitigating the impact of healthcare systems on the environment and protecting patients from the health impacts of climate change. A survey by NHS Sustainable Development Unit reported that 98% of NHS staff believe that health and care systems should work in ways which support the environment,9 and the majority (86%) of leaders in international gastroenterology believe that climate change represents a crisis.11 It is encouraging that global GI leadership recognises sustainability as a critical issue, and large organisations are increasingly considering their responsibilities to minimise climate impact.
How, then, do we make the change from concern to action? To do so, we must acknowledge financial, systemic and psychological barriers to change,11 building a team of like-minded individuals and seeking engagement and ideas from stakeholders. The measures required to reduce our climate impact are likely to appeal to NHS Trust budget holders, especially with concerns around the escalating costs of energy provision. Consideration as to the ongoing role of telemedicine, including for activities as specialised as liver transplant assessment, can significantly reduce travel-associated emissions.15 July’s Twitter debate allowed us to share examples of good practice and to direct individuals to resources and data to support them to make changes in their place of work. Undoubtedly, we still have a long way to go in achieving our green aims, but we hope that the debate has motivated colleagues to put sustainability at the forefront of our practice.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
We are grateful to all the participants in the #FGDebates.
References
Footnotes
Twitter @IBDdoc
Contributors JC drafted the initial manuscript. LD, DL and B'HH critically appraised and revised the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests BH reports grants from Fujifilm Europe, Ampersand Health and Surgease Medical outside the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.