Article Text

Abstract
Background Therapeutic drug monitoring (TDM) by measuring infliximab (IFX) trough levels and antibodies to infliximab (ATI) is used to optimise treatment in inflammatory bowel disease. We aimed to explore the clinical outcomes of TDM for patients with Crohn’s disease on IFX in real life setting.
Methods This is a retrospective observational study. Primary outcomes were the clinicians’ response to each TDM result and the rate of IFX discontinuation due to secondary loss of response or serious adverse event. Secondary outcomes included the intestinal surgery rate after IFX initiation and remission 6 months after TDM. Multivariate logistic regression was performed to identify factors associated with IFX discontinuation and abdominal surgery.
Results 291 patients were included. 238 (81.8%) patients were tested for TDM at least once during their follow-up with 672 TDM results. 95/238 patients (39.9%) had undetectable levels and 76 (31.9%) had positive ATI at least once. The median infliximab trough level was 3.4 µg/mL. IFX was discontinued in 109 patients (37.5%). 526/672 (78.3%) TDMs results were not followed by altered patient management. Treatment was discontinued in 40 (75.5%) patients never tested for TDM compared with 69 (29.0%) of those tested (p<0.01). Fewer TDM tested patients (29; 12.2%) required intestinal surgery post IFX initiation compared with TDM not-tested (15; 28.3%). Not being TDM tested was independently associated with IFX discontinuation and abdominal surgery.
Conclusions IFX discontinuation and intestinal surgery were significantly less frequent with TDM. TDM requested to investigate loss of response resulted in change in patient management.
- ibd
- ibd clinical
- health service research
- infliximab
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The use of infliximab (IFX) for Crohn’s disease (CD)1 has evolved shifting from episodic to scheduled therapy, monotherapy to combination with immunomodulators and unguided dose escalation to adjustment based on drug levels.2 3 Twenty per cent of patients present primary non-response (PNR) and 25%–40% secondary loss of response (SLR).4 SLR is managed by dose escalation, addition of immunomodulator or switch to another biologic.5 The evidence to guide decisions for dose intensification and switch to a different biologic is evolving.6
Measurement of serum trough level and antibodies to infliximab (ATI) in SLR has a role in guiding management. Adequate levels are associated with higher remission rates.7 Increase in trough levels after dose intensification is associated with better clinical response,8 whereas ATI with poorer outcomes.9 The TAXIT study was the first trial to compare concentration and clinically-based dosing showing a short lived benefit for concentration-based dosing.10
The usefulness of therapeutic drug monitoring (TDM) depends on the indication. Most clinical evidence is about drug adjustment for PNR or SLR (reactive TDM).6 The role of routine TDM irrespective of clinical status remains unclear.6 In this study, we aim to describe the use of TDM in everyday clinical practice. Specifically we aim to:
Describe the indications for request, the clinicians’ response and the patient outcomes 6 months after TDM.
Evaluate whether patients who initiated IFX in the post-TDM era discontinued treatment because of SLR or serious adverse events (SAE) less frequently compared with those who initiated in the pre-TDM era.
Evaluate whether TDM tested patients discontinued treatment due to SLR or SAE less frequently compared with those who never had TDM.
Methods
Study design
This was a retrospective observational study.
Setting
Our inflammatory bowel disease (IBD) service manages a cohort of local and tertiary referrals. Patients receiving biologics are entered onto the IBD audit database.11 Details on the clinical management were available on our electronic clinical information system.
Patient population
We included all patients who initiated IFX between January 2007 and July 2016. We excluded patients who were lost to follow-up within 3 months of initiation, had ulcerative colitis, indeterminate colitis or pouchitis, received less than three or episodic infusions.
Patients initiating IFX received induction dose of 5 mg/kg at weeks 0, 2, 6 and 8-weekly thereafter.
Intervention—TDM service
TDM was introduced to our institution in September 2013 using the lab of Sandwell and West Birmingham NHS Trust. Patients who started IFX before introduction of TDM (pre-TDM era), underwent TDM testing after its introduction.
TDM was undertaken prior to infusion at week 14 and week 50, at diagnosis or suspicion of SLR and to investigate SAEs or guide treatment discontinuation. Additionally, TDM was requested at the discretion of clinicians at any point for non specific reasons (‘routine testing’). It is likely that at the start of TDM service there was uncertainty about its application and routine testing may have been for reassurance that clinical benefits reflected adequate dosing and/or there may have been an intention to adjust therapy that was not pursued.
Application of TDM results to guide therapy in SLR
Dose escalation was offered for undetectable drug trough levels without ATI with evidence of active disease (raised CRP, calprotectin or evidence on imaging or endoscopy). Patients with undetectable trough levels with ATI were switched to different anti-TNF, whereas treatment was changed to a non anti-TNF biologic when the trough levels were therapeutic and there was active disease. The above represented a guide rather than a strict protocol. The final decision was at the discretion of clinicians.
Infliximab trough levels and ATI
Infliximab levels were measured by an ELISA assay as per Barlow et al. 12 Serum was added to a TNF-a coated plate and a detector was added to detect the IFX/TNFa complex. The reaction was detected with a fluorescent substrate.12 The cost was £60 per assay.
TDM Measurements and terminology
Infliximab trough levels were expressed in μg/ml. ATI were reported qualitatively as ‘positive’ when ATI were and ‘negative’ when ATI were not detected. The ATI assay is not drug tolerant and would only detect ATI in the absence of detectable infliximab. Trough levels below 1 µg/mL are classified as ‘undetectable’ and equal to or above 1 µg/mL as therapeutic.
Patients who had TDM at least once are reported as ‘TDM tested’ and those who never had TDM as ‘TDM never-tested’. Undetectable trough level at least once is captured as ‘undetectable levels episode’, ATI positive at least once as ‘ATI episode’ and dose intensification at least once as ‘dose intensification episode’.
Data extraction and definitions
Demographic (age, sex) and disease-specific (Montreal Classification (MC),13 duration) data were extracted.
Disease activity was defined according to physician’s global assessment (PGA) as active or inactive and was recorded from the consultation letters. PNR was defined at week 14 according to PGA for luminal disease as complete absence of clinical improvement and for perianal CD as failure to reduce the number of draining fistulas by 50%.14 SLR was defined according to PGA as worsening of symptoms after an initial response to IFX and raised CRP, calprotectin and/or endoscopic activity.
Infliximab trough level was the level measured on a sample drawn just prior to dosing. SAE was defined as any acute or delayed infusion reaction necessitating infliximab discontinuation.15
Outcome measures
Our primary outcome measures were: The clinicians’ response to each TDM requested and treatment discontinuation because of SLR or SAE.16 Secondary outcome was the need for surgery (small bowel resection, colectomy or stricturoplasty) after the initiation of infliximab. Outcomes were compared between patients whose treatment was initiated before (pre-TDM era) or after the implementation of TDM (post-TDM era) and also between TDM tested and TDM never tested patients.
An additional secondary outcome was the proportion of clinical remission episodes 6 months after every TDM result.
Statistical analyses
Data were analysed with the Statistical Package for Social Sciences (SPSS V.17) and Prism Graphpad V.7. Continuous variables were expressed as median (IQR) and compared using the Mann-Whitney U test. Categorical variables were expressed as absolute numbers n (percentage of population) and compared using the χ² test. Multivariate logistic regression was used to identify factors associated with drug discontinuation due to SLR/SAE and surgery. In the multivariate analysis (MVA) were entered all the variables that were significantly associated with our outcome on univariate analysis (UVA) (p value threshold 0.05). Kaplan-Meier curves and the log rank test compared the IFX discontinuation free and surgery-free survival between groups. Analyses were two-tailed and p<0.05 were considered significant.
Ethical considerations
TDM in our practice constitutes a new clinical service (‘TDM service’) and this study was done as service evaluation. The care provided to patients was part of standard care. Therefore, formal ethics approval was not required. We received approval from the Research and Development (R&D) department of London North West Healthcare NHS Trust (SE16/042) as per Trust Policy.
Results
Population
Total 517 patients were identified on our database. From these, 226 were excluded for various reasons (figure 1). Total 291 patients were included.

Study population. IFX, infliximab; UC, ulcerative colitis.
The median (IQR) patient age was 35.0 (21.0) years with disease duration 89.95 (157.2) months prior to IFX. The MC and IFX indications are described on table 1. The duration of follow-up was 44.7 (40.3) months.
Baseline demographic and disease specific characteristics of patients on infliximab
Total 161 (55.3%) patients initiated IFX in the pre-TDM era and 238 (81.8%) were TDM tested. From these, 95 (39.9%) had an undetectable levels episode and 76 (31.9%) an ATI episode. Total 199 (83.6%) had at least one routine TDM.
IFX was discontinued due to SLR or SAE in 109 patients (37.5%) and 39/109 (35.8%) had at least one routine TDM. Of these 39, 18 (46%) had undetectable trough levels, 5 (13%) levels of 1–3 µg/mL, 16 (41%) levels of 3.1–10 µg/mL and 17 (44%) had ATI prior to discontinuation. Surgery was required in 44 patients (15.1%). Total 62 patients (21.3%) had their dose intensified.
Effect of TDM results on clinical management
Total 672 TDM tests were requested for 238 patients. The median (IQR) IFX trough level was 3.4 (5.4) μg/mL. IFX trough levels were undetectable in 154 (22.9%) samples, between 1 and 3 µg/mL in 161 (24%), between 3.1 and 10 µg/mL in 356 (53%) and above 10 µg/mL in 1 (0.1%). Total 118 (17.6%) TDM samples were ATI positive. The time from IFX initiation to first TDM was 12.5 (30.2) months and the first and subsequent trough levels were 3.7 (5.3) μg/ml and 3.2 (5.5) μg/mL, respectively.
Total 469 (69.8%) routine TDM assays were undertaken. The second most common indication was SLR in 180 (26.8%) (table 2).
Clinical management changes within 6 months of therapeutic drug monitoring (TDM) tests
Most TDMs (526/672; 78.3%) were not followed by change in patient management. Total 58 (8.6 %) TDMs were followed by dose intensification, 40 (6.0%) by switch to alternative anti-TNF, 12 (1.8%) to non-anti-TNF biologic, 10 (1.5%) by addition of thiopurine, 9 (1.3%) by dose de-escalation and 17 (2.5%) by biologic discontinuation. Total 78 (32.8%) TDM tested patients had management modifications as a result of TDM. When TDM indication was PNR or SLR, change in management occurred after 54.6% (100/183) of levels compared with 9.4% (46/489) for other indications (p<0.01).
Total 411 (61.3%) assays were followed by clinical remission after 6 months. When TDM was requested for PNR or SLR, the 6 months remission rates were similar irrespective of whether change in patient management followed (49 (52.1%)) or not (36 (45.0%)) (p=0.35). The median (IQR) trough level followed by remission 6 months after testing was 4.3 (5.4) μg/mL compared with 2.3 (4.7) μg/mL for assays followed by active disease (p<0.01).
Initiation of IFX in the pre-TDM or post-TDM era: patient characteristics and outcomes
The age of patients initiated on IFX in the pre-TDM era was 37.0 (19.0) compared with 33.0 (23.0) years for patients of the post-TDM era (p<0.01). The duration of follow-up was 62.3 (36.5) months for the former and 25.7 (14.5) for the latter (p<0.01). Perianal and penetrative disease were more prevalent among pre-TDM era patients. Previous exposure to biologic was noted in 7 (4.3%) patients of the pre-TDM era and 17 (13.1%) of the post-TDM era (p<0.01). 111 (68.9%) patients of the pre-TDM era had TDM compared with 127 (97.7%) of the post-TDM era (p<0.01). More patients of the post-TDM era had an ATI episode (32.3% vs 21.1%, p=0.03).
IFX was discontinued due to SLR or SAE in 69 (42.9%) patients of the pre-TDM era compared with 40 (30.8%) of the post-TDM era (p=0.03). The median (IQR) time to discontinuation was 48.0 (40.1) and 19.4 (16.8) months, respectively (p<0.01). The rate of intestinal surgery after initiation of IFX and time to surgery did not differ between groups (online supplementary table 1).
Supplementary file 1
Disease outcomes and patient characteristics for TDM tested and TDM never tested patients
There was no difference in the age, disease duration and MC between groups. The duration of follow-up was 37.4 (31.6) months for the TDM tested and 67.0 (53.6) for the TDM never tested. More patients of the former group (24 (10.1%)) compared with the latter (0 (0%)) received IFX as second line biologic (p=0.02) (online supplementary table 2).
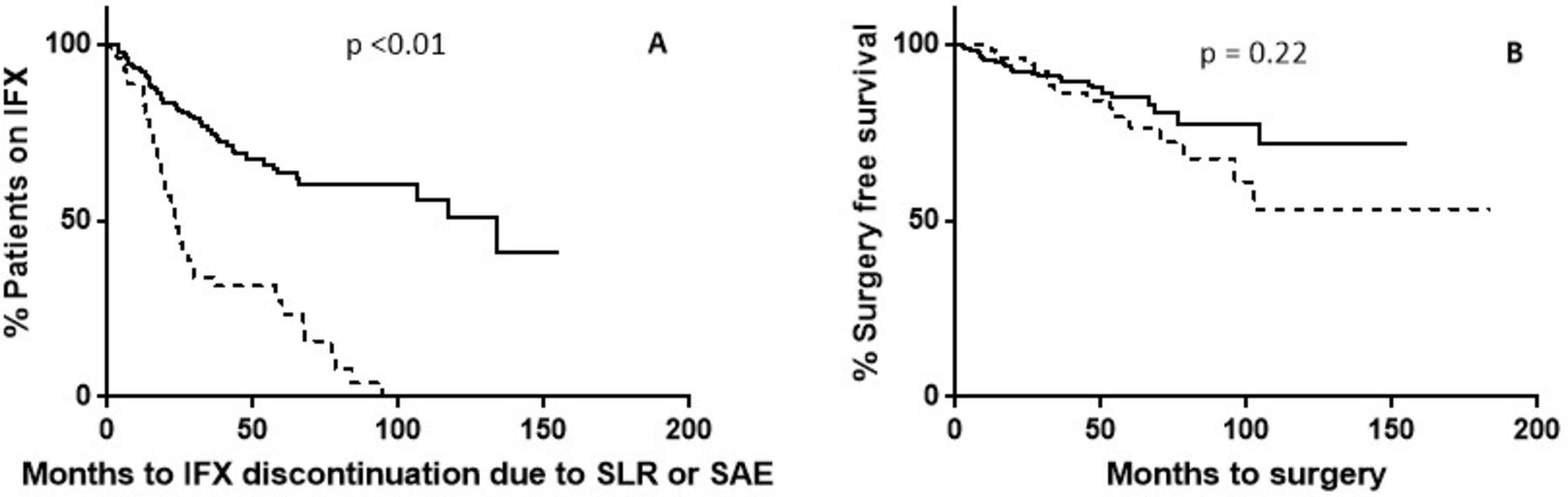
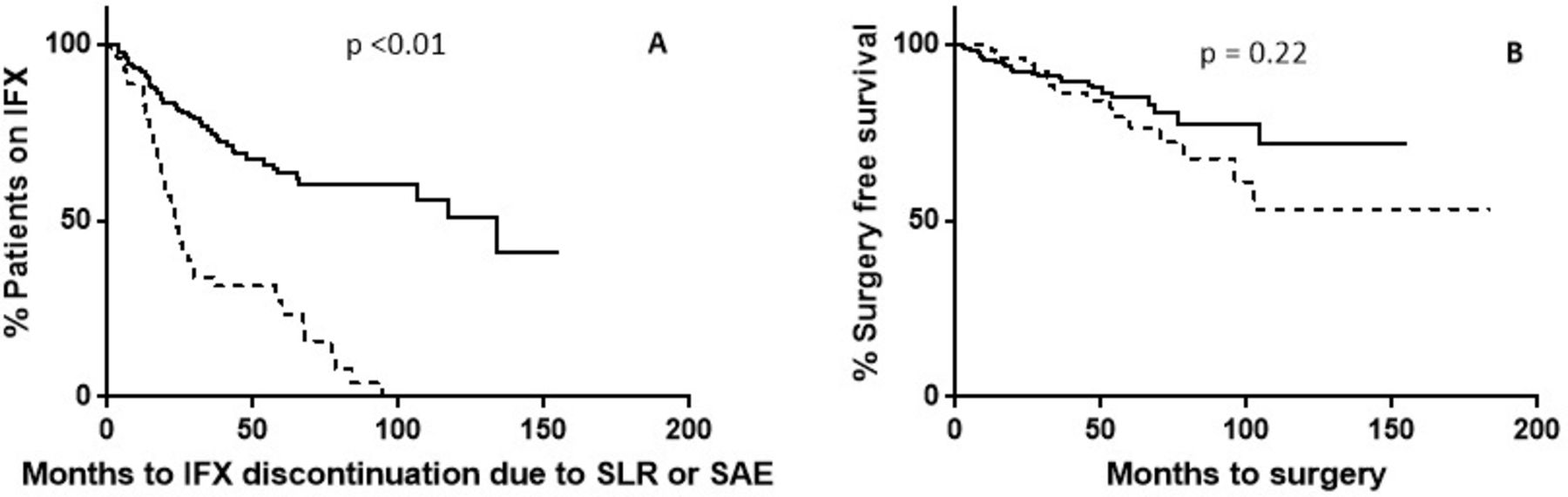
IFX was discontinued due to SLR or SAE in 69 (29.0%) TDM tested patients and 40 (75.5%) TDM never tested (p<0.01) and the discontinuation free survival was longer for the former (32.9 (35.1) months) compared with the later (19.9 (22.8) months) (p<0.01) (figure 2A). Less TDM tested patients (29; 12.2%) required surgery compared with TDM never tested (15; 28.3%) (p<0.01) (table 3). Time to surgery did not differ between groups (online supplementary table 2, figure 2B).
{kind=link}
{kind=link}
Survival analysis of the time to drug discontinuation due to SLR or SAE (A) and time to surgery for IBD (B). The dotted line and the solid line represent the ‘TDM never tested’ and the ‘TDM tested’ group, respectively. IBD, inflammatory bowel disease; IFX, infliximab; SAE, serious adverse event; SLR, secondary loss of response; TDM, therapeutic drug monitoring.
Multivariate analysis of factors associated with infliximab discontinuation due to SLR or SAE
Factors associated with IFX discontinuation due to SLR or SAE
The UVA of factors associated with discontinuation of IFX due to SLR or SAE identified that the overall duration of follow-up, previous exposure to biologic, initiating treatment in the post-TDM era and being TDM never tested were associated with higher rates of discontinuation due to SLR or SAE (online supplementary table 3).
MVA (OR (95% CI), p value) showed that being TDM never tested (8.0 (3.8, 17.0), <0.01) and having previously been exposed to a biologic (4.4 (1.8, 10.7), <0.01) were associated with IFX discontinuation (table 3).
Factors associated with intestinal surgery after IFX initiation
The UVA of factors associated with surgery identified that the overall duration of follow-up, being TDM never tested and previous exposure to biologic, are associated with higher rates of surgery after initiation of IFX (online supplementary table 4).
MVA showed that being TDM never tested (2.5, (1.1, 5.7), 0.03) and previous exposure to biologic (4.3 (1.6, 11.8), <0.01) are associated with surgery after initiation of IFX (table 4).
Multivariate analysis of factors associated with IBD-related abdominal surgery after infliximab initiation
Discussion
In this study, we showed that only 22% of TDM requests were followed by change in patient management. Where the indication was PNR or SLR, the impact was greater. Moreover, the TDM never tested group showed an 8-fold risk of drug discontinuation and a 2.5-fold risk of surgery.
With the expansion biologics and the rising awareness of immunogenicity, research focused on methods to optimise their effects. TDM was initially described in clinical trials as a secondary observation17 but slowly entered clinical practice in a non-standardised way. The American Gastroenterological Association published a technical review of TDM and the evidence was graded as low quality.6 However, a few lessons can be learnt from our results.
Key results and interpretation
Infliximab discontinuation due to SLR or SAE
Our results are similar to others’. 37.5% of our patients discontinued IFX. Similarly, recent studies quoted that 27% of patients have poor outcomes including treatment discontinuation and surgery at 1 year18 and 54% discontinue treatment at 24 months after initiation.17 Others reported similar discontinuation rates with Adalimumab.19
Fifteen per cent of patients had surgery after IFX initiation. Surgery was more likely among patients who never had TDM. Surgery rate in our patients appears close to that quoted by Ederhardson et al 20 but is lower compared with other reports where 26% of patients underwent surgery.21 This may reflect the shift of clinical practice towards elective surgery21 and the availability of non-surgical interventions including double balloon enteroscopy,22 endoscopic balloon dilatation22 and endoscopic submucosal dissection.23
Our results suggest that both surgery and treatment discontinuation are more likely among TDM never tested patients. This reflects management planning according to TDM as more likely to be beneficial. It is challenging to suggest whether the change in management directed by TDM results in better outcome or whether TDM creates reasoning grounds to persevere with optimisation of the same agent.
Impact of TDM in clinical decision making
We found that 22% of TDM resulted in change in patient management as the predominant indication was routine TDM. Clinicians undertaking TDM in the context of loss of response have a clear goal. The rational of routine TDM seems unclear and may have arisen in early days of TDM when there was less understanding of how to use it. It would have been interesting to explore the reasons further, but this was beyond our scope. For 469 routine assays, the cost was estimated about £28 000 and only 1 in 10 routine tests resulted in management change. Our new protocol discourages the use of routine TDM.
The published literature on the impact of TDM on decision making is limited. In a paediatric population,24 TDM resulted in change in management in 34% of cases. Another study of 71 patients reported a change in management for 37% of cases after TDM for SLR.9
However, emerging evidence suggests that proactive TDM followed by dose adjustment to target levels above 5 µg/mL is associated with less treatment failure and need for surgery,25–27 suggesting that proactive TDM should be followed. In our study, it is speculative whether treatment failure may have been avoided for patients who underwent routine testing, had clinicians adjusted the dose to reach a target concentration. Our finding that remission at 6 months after TDM was associated with higher IFX trough level supports this.
Strengths
Our study has several strengths. Patients were identified through a prospectively built database capturing consecutive patients. Therefore, we report on a large number of patients and TDMs. Second, all tests were undertaken by the same laboratory with identical technique. Last, although the overall duration of follow-up was greater for TDM tested patients and patients of the pre-TDM era, this was not a significant prognostic factor in the MVA, therefore our results do not reflect lead time bias.
Limitations
This is a retrospective study and data collected on clinical outcomes rely record keeping. We used the PGA as a measure of clinical remission. This may be subject to interpretation bias. Second, our results may be subject to tertiary centre bias. Although the majority of patients represent our local area, our outpatient clinic includes tertiary patients who have more complex disease. Although there were no significant differences in the MC among groups, this may be inadequate to describe disease complexity which is better reflected by the level of intestinal damage (Lemann classification).28 Last, we use the endpoints of drug discontinuation due to SLR or SAE and surgery; however, we acknowledge the fact that it is not uncommon to stop IFX for ongoing abdominal pain, without formal assessment of activity. Similarly surgery may not reflect active inflammation or stricturing disease.
Conclusion
We report our experience with TDM and outcomes for patients with CD on IFX. We show that treatment discontinuation due to SLR or SAE and surgery is less likely when TDM is undertaken. However, the majority of TDM was done routinely and not followed by change in clinical management. A reactive indication (PNR or SLR) was more likely to result in change in management. There is evidence suggesting that proactively dose adjusting to reach a target level, results in better outcomes.27 Therefore, unless routine testing is undertaken with the intent to proactively dose adjust, due to the cost implications and in the face of our observations, we should limit TDM to reactive testing while taking the opportunity to design studies with longitudinal follow-up.
Significance of this study
What is already known on this topic
Therapeutic drug monitoring (TDM) for infliximab is a useful tool when managing secondary loss of response (SLR).
The TAXIT study has shown that continued dosing of infliximab aiming to reach a target trough concentration results in better outcomes at 1 year.
The pattern of TDM use in everyday clinical practice and its influence in the patient management and longer term outcomes have not been described.
What this study adds
TDM when requested routinely in everyday clinical practice did not change the patient management in most cases, while it did when requested reactively to primary non-response (PNR) or loss of response.
Patients who have TDM measured during their course of treatment are less likely to have their treatment discontinued due to treatment failure or serious adverse events or to have surgery for inflammatory bowel disease.
How might it impact on clinical practice in the foreseeable future
More clinicians and clinical centres will adopt the use of TDM as this study shows that TDM is not only a research or clinical trial tool but has a value that benefits patients in real life clinical practice.
Clinicians will be encouraged to use TDM for clear indications (PNR, SLR) rather than routinely to maximise the benefit from TDM and minimise the associated cost.
References
Footnotes
Contributors NK conceived the study, collected a part of the data, analysed the data and prepared the manuscript. PM, TT and IS collected data for the study. NA supervised the study design, conduct of the study and results and reviewed and edited the manuscript.
Funding NK received funding from St Mark’s Foundation to support his salary during this project.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There are no additional unpublished data from this study.
Patient consent for publication Not required.
Linked Articles
- UpFront
- Commentary