Article Text

Abstract
A frequent dilemma faced in the inflammatory bowel disease (IBD) clinic is how to best treat a patient with a previous cancer diagnosis. The changing demographics of our patient population will make this quandary more common. Previous guidance has emphasised the importance of lengthy postcancer drug holidays and cautious use of IBD therapies. However, accumulating evidence suggests this approach may be unnecessarily conservative. This review considers recent evidence on the safety of IBD drugs, cancer and recurrent cancer risk in patients with IBD and provides a framework for shared decision making involving patient, gastroenterologist and oncologist.
- inflammatory bowel disease
- cancer
- adverse drug reactions
- clinical decision making
Statistics from Altmetric.com
Key points
Patients with previous cancers are becoming increasingly common in the inflammatory bowel disease (IBD) clinic.
Exclusion of patients with prior cancers from trials and potential treatment selection bias in real-world data can make treatment decisions challenging.
Immunosuppression-related risk of cancer recurrence may be lower than perceived.
Risk of cancer recurrence and risk of unfavourable IBD outcomes must be considered when determining treatment strategy.
Patient perception and acceptance of risk varies and must be respected.
Introduction
The number of people living with inflammatory bowel disease (IBD) is growing, and that population is ageing. A Scottish study quantified IBD prevalence of 1.26% among people in their 70s, compared with a rate of 0.47% in people in their 20s.1 As people live longer with IBD, comorbidity is acquired, and people with comorbidity develop IBD. IBD treatment decisions for patients with a cancer diagnosis are challenging.
IBD requires optimal long-term treatment to improve and maintain quality of life and reduce the accumulation of disease-related complications including cancer. IBD-associated colorectal cancer (CRC) is defined by the inflammation–dysplasia–carcinoma sequence. Chronic inflammation leads to genetic and epigenetic changes resulting in chromosomal instability,2 and therefore control of inflammation should reduce the risk of CRC. The immune dysregulation associated with IBD and other inflammatory conditions may also promote extracolonic malignancy.3 In addition, history of prior malignancy in patients with IBD is associated with higher risk of new or recurrent cancer,4 potentially reflecting common genetic background risk variants for IBD.5 In parallel, IBD therapies, due to direct or indirect effects on the immune system, could promote malignancy.6 Current ‘treat-to-target’ approaches propose clinical, endoscopic, inflammatory and quality-of-life objectives.7 8 This may result in earlier introduction of immunosuppression to achieve optimal outcomes at the expense of earlier or prolonged introduction of any associated risk.
Estimates suggest only 31% of IBD clinic patients would meet inclusion criteria for the rigorous randomised controlled trials required to assess treatment efficacy.9 Blanket exclusion of patients with prior cancers leads to difficulties in extrapolating any identified risks and benefits. Here ‘real-world’ evidence aims to assist us.10 These observational data from clinical practice (records, registries and surveys) offer insights into treatment performance, be it efficacy or safety. It does however reflect only existing practice. If a physician is concerned that a treatment may provoke cancer, they will not use it in those they perceive as at risk, introducing significant bias, and therefore data will not provide a true reflection of the scale of any potential hazard.
Sebastian and Neilaj’s excellent review from 201911 summarises evidence on cancer risk with many existing IBD drugs along with practical guidance on prescribing in patients with cancer. This paper updates the evidence, including data for the more novel therapies.
IBD therapies and cancer risk
Low/no-risk therapies
There is no evidence of cancer risk with mesalazine therapy and instead indirect evidence to support a reduced risk of advanced colorectal neoplasia.12 No studies associate risk with exclusive enteral nutrition. Although corticosteroids are not a long-term IBD therapy, short courses are generally considered low risk from a cancer point of view13 14; however, a link between frequent prescriptions and non-melanoma skin cancers (NMSCs) and non-Hodgkin's lymphoma has been suggested.15
Thiopurines
Thiopurines exert their anti-inflammatory effect by T-cell suppression16; however, they may also have carcinogenic properties. They can cause mutations in tumour suppressor genes, increase sensitivity to UV light and appear to specifically deplete natural killer cells which play a crucial role in the immune response to Epstein-Barr virus (EBV), leading to serious infection and virus-related lymphoproliferative disorders.11 17
A large prospective study associated thiopurine use with lymphoproliferative disorders (HR 5.28, 95% CI 2.01 to 13.9).18 More recent meta-analysis confirmed excess risk in particular of NMSC (relative risk 1.88, 95% CI 1.48 to 2.38).19 A recent retrospective study of thiopurines noted a significantly increased risk of non-Hodgkin's lymphoma and leukaemia.20 It did, however, note that thiopurine use in IBD conveyed a lower risk of malignancy when compared with post-transplant patients, but a higher risk compared with patients with rheumatoid arthritis (RA). In contrast, a French retrospective study of specifically elderly-onset IBD found that while risk of lymphoproliferative and myeloproliferative cancers was increased, this was not associated with thiopurine use.21 A further prospective case–control study found that immunomodulators neither increased the risk of CRC or extracolonic cancer (ECC) nor showed a statistically significant association with their use and skin cancers.3
Methotrexate
Methotrexate is used widely as an anti-inflammatory for multiple diseases and also as an antineoplastic agent. Anti-inflammatory properties are thought to be multimodal, including inhibition of folate enzymes, accumulation of adenosine and blockade of inflammatory cytokines.22
Methotrexate use was linked with lymphoma as it was thought to adversely affect recognition of EBV-infected B lymphocytes; however, this evidence focused on patients with RA (where the risk of lymphoma is increased) often compared against the general population.23 A further retrospective study did, however, identify methotrexate as a risk factor for lymphoproliferative disorders versus non-use.24 Ultimately, there is little evidence to support that methotrexate alone is associated with malignancy in the context of IBD, although this may relate to small numbers of patients using this as monotherapy.25
Antitumour necrosis factor (TNF)
TNF, with its pivotal role in initiating the proinflammatory cascade,26 is an attractive therapeutic target in immune-mediated inflammatory conditions such as IBD. As TNF has both tumour-promoting and tumour-inhibiting effects, the risk of malignancy in patients receiving anti-TNFs can be difficult to predict.
Determining specific cancer risk of anti-TNF therapy is complicated as it is often prescribed in combination, usually with thiopurines. Initial studies suggested a small increased risk of lymphoma with anti-TNF usage27; however, subsequent systematic review has found this not to be the case with monotherapy.28 When used in combination with thiopurines, there is an increased lymphoma risk,28 with hepatosplenic T-cell lymphoma distinctly associated with this combination.29 Initial reports of increased risk of melanoma have not been confirmed in meta-analysis,30 and overall malignancy does not appear to be associated with anti-TNF monotherapy.31
A systematic review and meta-analysis of observational studies found no significant difference in the risk of new or recurrent cancer in patients with previous cancer exposed to anti-TNF therapy compared with controls.32 This is supported by a further large Danish cohort study including patients with IBD and other inflammatory conditions.33
Newer biologics
Newer drugs have had less opportunity to accumulate real-world experience to guide practice. Here we can ‘borrow’ risk evidence from other inflammatory conditions where there are a greater number of patient-years’ experience to draw on. This, of course, assumes equivalent cancer risk and immunosuppressive effects between inflammatory-mediated disorders and may not be directly applicable to IBD-specific dosing regimens or gut-specific agents.
Ustekinumab is a humanised monoclonal antibody that manipulates the interleukin (IL)-12/IL-23 axis by binding their common p40 interleukin subunit.34 Initially developed for use in psoriasis, where IL-12/IL-23 neutralisation reduces cytokine expression, it is also effective in CD35 and UC.36 IL-12 and IL-23 have potentially conflicting roles in carcinogenesis; therefore, neutralising p40 could have a protumour effect.37 In psoriasis and psoriatic arthritis, recent meta-analysis did not find an increased risk of cancer biologic drugs collectively (including ustekinumab).38 One of the contributing studies did separate out drugs used and found no increased risk in patients receiving either anti-TNF agents or ustekinumab compared with conventional immunosuppression.39 Similarly, Wu et al 40 found no increased risk of malignancy in patients receiving biologics including ustekinumab compared with conventional immunosuppression. Within the IBD literature, evidence of ustekinumab safety comes from combined phase II/III trials and confers no increased cancer risk.41 Of note, the follow-up period here was short (1 year), and most of the patients who developed a cancer had previously received at least one other biologic. As the trials exclude patients with previous cancers, no further conclusion can be drawn on recurrence risk. An observational cohort study is recruiting patients to assess long-term safety, primarily incidence of malignancy, in patients with IBD receiving usekinumab compared with other biologics (NCT04372108).
Vedolizumab is a gut-selective antibody that blocks trafficking of a4b7 integrin-expressing lymphocytes from the systemic circulation.42 In a large long-term safety study covering 1785 patients with at least 1 year of follow-up, numbers of malignancies observed were similar to those expected compared with matched patients from a large IBD database.43 This study also reviewed postmarketing reporting of malignancies which also found no risk signal. Vedamurthy et al 44 focused their biologics use cohort study on the tricky-to-treat population with a prior history of cancer. They included 96 patients receiving vedolizumab after a prior diagnosis of cancer and compared new or recurrent cancers with 184 patients exposed to anti-TNF and 183 exposed to no immunosuppressive therapy over a median of 6.2 person-years of follow-up. New cancers or recurrence was identified in the vedolizumab group at a rate of 22 per 1000 person-years after cancer diagnosis. This was similar to anti-TNF or no immunosuppression. Additional reassurance is suggested by a further two recent studies that have reported that use of ustekinumab or vedolizumab45 or vedolizumab or anti-TNF46 for IBD therapy in patients with a prior history of cancer does not appear to be associated with an increased risk of new or recurrent cancer.
Small molecule inhibitors
Small molecule therapies are attractive as they are orally bioavailable and not subject to immunogenicity. Cytokines principally exert their function by signalling to immune cells via JAK/STAT pathways, making this an enticing treatment target. In addition, given the key role of JAK/STAT in IBD–CRC tumorigenesis, the potential of impacting this with therapies is intriguing.2
Tofacitnib is a JAK inhibitor predominantly active at the JAK3 receptor with proven efficacy in moderate–severe UC.47 Reports from the initial tofacitinib trials covering 4.4 years of follow-up48 and patients receiving the drug exclusively for UC with 6.8 years of follow-up49 found no increased risk of malignancy (excluding NMSC) or NMSC, or malignancy (excluding NMSC), respectively. The last year has seen two meta-analyses of real-world experience with tofacitinib in IBD. The first reported serious adverse event rate in the analysed studies of 4.4%; however, the number of malignant events was not further described.50 The second identified one case of malignancy (metastatic breast cancer) among the reported adverse events over a median follow-up of 31 weeks.51 This case was attributed to high prior immunosupressive load.52 Ytterberg et al 53 have recently reported their randomised, open-label safety trial in patients with RA looking at tofacitinib associated cancer and cardiovascular risk over 6.2 years of follow-up.14 Cancer rates with tofacitinib exceeded rates with anti-TNF (HR 1.48, 95% CI 1.04 to 2.09). The study involved patients aged over 50 with at least one additional cardiovascular risk factor and therefore bears closer resemblance to some of the real-world clinic. This study has led to Medicines and Healthcare products Regulatory Agency/Commission on Human Medicines (MHRA/CHM) advice that tofacitinib should not be used in patients over 65, current or past smokers, or those with other malignancy risk factors unless no suitable alternatives are available. Of note, the real-world IBD tofacitinib studies and trial data encapsulated a younger population (mean age approx. 40).48 51
There are as yet no cancer risk data available on the other small molecules under development in IBD. JAK inhibitor filgotinib is associated with a similar malignancy rate as other JAK inhibitors in RA.54 Tyrosine kinase inhibitor decruvacitinib remains in phase II trials. Sphingosine-1-phosphate inhibitors such as ozanimob, now approved for UC, have been used more widely in multiple sclerosis where safety data so far show no increased rate of incident cancers compared with other treatments.55
Making treatment decisions
Much of the evidence regarding cancer recurrence risk in immunosuppressed patients comes from post-transplantation data sets.56 Twenty per cent of cancers recur in renal transplant recipients, usually within the first 2 years. Risk factors included level of immunosuppression and cancer type. Low recurrence risk cancers included lymphoma and cervical cancer, medium risk was attributed to breast and colon and high risk to melanoma, NMSC, lung and urinary tract cancers. The European Crohn's and Colitis Organisation (ECCO) guidance on postcancer drug holidays recommends 2 years before recommencing immunosuppressive IBD treatment.25 With intermediate and higher recurrence risk cancers 5 years is suggested.
In patients with IBD, with previous cancer, the risk of a new or recurrent cancer is increased twofold compared with patients without prior malignancy, but this risk was found to be independent of drug use.4 A large study of patients with previous cancer and RA, IBD or psoriasis involving over 11 000 patients with 31 000 person-years follow-up found no increased risk of cancer recurrence comparing anti-TNF, conventional immunosuppression and no immunosuppression other than an increase in NMSC in patients receiving thiopurines.57 As discussed previously, recent data do appear to be broadly supportive that anti-TNF therapy and the newer biologics do not appear to be associated with an increased risk of new or recurrent cancer in IBD.31 Evidence emerging since the ECCO drug holiday guidance suggests it may be unnecessarily conservative, especially when considering the risk of not treating IBD effectively. The BSG 2019 IBD guidance, while acknowledging the ECCO statement on drug holidays, stresses biologics should not be considered contraindicated in patients with prior malignancy and instead advise individualised decisions.58 This recognises broadly reassuring emerging evidence and better aligns with the more pragmatic current clinical practice in many units where additional factors are scrutinised when deliberating when to start or restart treatment and risk trade-offs are considered (see box 1).
Factors to consider in IBD treatment decisions in patients with previous cancer
IBD factors
Evidence of disease activity.
IBD phenotype? aggressive/high risk?
Previous treatment requirements (eg, anti-TNF).
Cancer factors
Cancer type and stage.
Time since diagnosis.
Recurrence risk.
Cancer risk with IBD treatment.
Current systemic anticancer therapy?
Patient factors
Patient risk preference.
Patient comorbidity.
In a study of patients with IBD and a new diagnosis of solid organ cancer, 17% developed a flare within 6 months of stopping IBD therapy. The likelihood of flare could be predicted by the typical ‘high-risk’ features such as younger age and previous requirement for anti-TNF therapy.59 Interestingly, among patients with active IBD at the time of cancer diagnosis, cytotoxic cancer treatment resulted in remission in 2/3, cancer treatment in itself obviating the need for specific therapy. This study was performed before the era of treat-to-target, and we now have more comprehensive tools to identify deep remission and predict IBD relapse.60
There is emerging evidence to support that aggressive IBD phenotype may be a risk factor in itself for cancer development. Inflammation is a critical initiating factor for the dysplasia IBD–CRC sequence; however, risk appears to extend beyond the digestive tract. In an extension of their initial 3-year case–control study,61 Biancone et al 3 examined risk factors for the development of cancer in patients with IBD. Over 6-year follow-up digestive system cancers were the the most common type (32%), and further analysis was performed separating CRC from ECCs. Development of ECC was associated with aggressive IBD phenotype (more extensive vs distal disease in UC and fistulating disease in CD) rather than treatment history (immunomodulators and anti-TNF). Recognising the increased cancer risk raises to the fore our role in promoting cancer vigilance (see box 2).
Cancer vigilance in the IBD clinic
IBD–CRC screening.
EBV status in pretreatment screens.
Drug-specific advice.
For example, thiopurines—high-factor SPF, sun avoidance and skin surveillance.
Consideration of compound risk factors and risk factor reduction, for example, smoking status.
Encourage engagement with national schemes.
Promotion of HPV vaccination in appropriate age groups.
BCSP.*
Cervical screening.
Breast screening.
Phase of cancer treatment is an important consideration. ECCO advise in the case of active melanoma, anti-TNF use may be associated with risk of progression and advise avoidance.25 It is worth noting, though, that anti-TNF (infliximab) and vedolizumab are both used in the management of checkpoint inhibitor colitis (ie, disease secondary to anticancer immunotherapy).62 Head-to-head trials for these agents in patients with genitourinary cancer and melanoma are ongoing (NCT04407247).
An interesting study looking at patients with IBD facing hypothetical treatment decisions identified heterogeneity of risk preference regarding medication efficacy and risk of harm.63 Patients who valued symptom avoidance over treatment risk tended to be younger and have lower Crohn's Disease Activity Index (CDAIs), whereas the most treatment risk avoidant groups were older and had higher CDAIs. Those in the risk avoidant group equated a 5% risk of cancer with losing 16 months of symptom-free time versus the remainder of the study population who assigned this risk a value of 4 months of symptom-free time. This study serves to remind us that the values we assign to risk and benefits within a multidisciplinary team (MDT) discussion may not align with those of the patient.
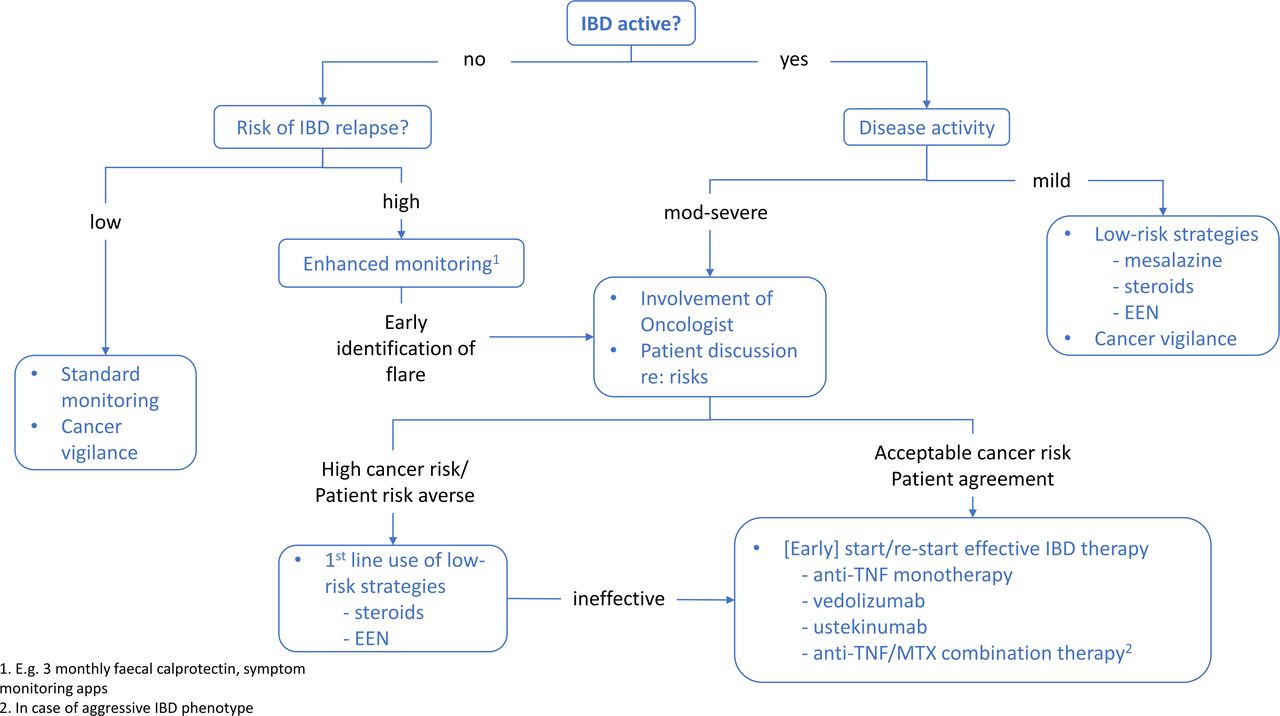
Sebastian and Neilaj11 propose treatment algorithms that focus on time since cancer diagnosis and use of lowest risk treatment options first line. We propose that further reassuring (although imperfect) evidence supports that cancer recurrence risks with many of our current agents are probably acceptable, and the risks of ineffective IBD therapy must be considered too. Our proposed algorithm focuses on identification of IBD flare, early involvement of the oncologist to stratify cancer risk, involvement of patients in discussion of risks and benefits of differing treatment strategies and avoidance of delay in commencing effective therapies in aggressive IBD phenotypes (see figure 1). We would consider ustekinumab risk as commensurate to anti-TNF or vedolizumab, but there are insufficient data to support the use of novel small molecule agents in this setting.

{kind=link}
Suggested algorithm for treatment decisions in patients with IBD and prior cancer. EEN, exclusive enteral nutrition; IBD, inflammatory bowel disease; MTX, methotrexate; TNF, tumour necrosis factor.
Conclusion
The trend towards earlier use of immunosuppressive therapy is coinciding with growing prevalence of IBD in elderly and comorbid populations and the widening gap between trial subjects and typical clinic patients. Absence of robust safety data in these challenging groups fuels hesitancy to prescribe drugs associated with the best IBD-related outcomes. Similarly, oncologists fear immunotherapy may worsen IBD or provoke IBD flare and deny life-saving drugs. Collaborative working offers the most objective perspective on risks and benefits.
Other chronic inflammatory conditions such as psoriatic arthritis and RA are associated with a higher risk of cancer that is not increased by biologic use.38 64 Similarly, there appears to be an increased cancer risk in patients with IBD linked to more severe inflammatory phenotypes and not limited to the digestive tract.3 Inflammatory burden and common genetic or environmental factors may be important. Pooled data from patients with previous cancer and an inflammatory disorder were found to have no increased recurrence comparing anti-TNF, conventional immunosuppression and no immunosuppression other than an increase in NMSC in patients receiving thiopurines.57
The recent IBD literature focuses on the need for optimal control of inflammation. Treatment-related risks are probably low but not accurately quantified over long durations of treatment. As more patients now receive multiple agents sequentially over many years, determining risk of each treatment is a challenge. It may be that the differing mechanisms of therapeutic immune modulation are more associated with one cancer type than another and when all drugs or all cancers are grouped any hazard signal lost.
To answer how best to treat patients with previous cancers, we need to study patients with previous cancers. Retrospective analysis of patients with IBD with previous cancer receiving anti-TNF, ustekinumab or vedolizumab44–46 and pooled data on cancer recurrence in patients with inflammatory conditions receiving immunosuppression57 go some way to provide reassurance that we may overestimate treatment-related risks. However, we must recognise the potential for treatment selection bias in retrospective data when the factors determining that treatment choice are unknown; those seen most at risk of recurrence may not have been given perceived higher-risk treatments. The ongoing prospective IBD Cancer and Serious Infections in Europe study aims to further assess concerns among patients taking anti-TNFs and/or thiopurines (NCT02377258). The extent to which patients with prior cancers are represented remains to be seen. Ultimately, long-term prospective studies including representative patients are needed.
Until that time, crucially our specialist IBD/cancer MDT decisions should aim to bring together patient preferences and expectations guided by the combined clinical expertise of the gastroenterologist and oncologist.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
SD acknowledges the support of NHS Research Scotland via NHS Lothian.
References
Footnotes
Contributors SEM-L and SD conceived the article. SEM-L, ZA and SD researched and prepared the manuscript. SC provided critical feedback and helped shape the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.
Linked Articles
- UpFront