
Abstract
Summary
Vitamin K and D deficiency and decreased bone mineral density (BMD) were highly prevalent in patients with inflammatory bowel disease (IBD), especially Crohn’s disease (CD). Dietary intakes of these vitamins, however, were above the Japanese adequate intakes in IBD patients, suggesting that malabsorption is the basis for hypovitaminosis K and D and decreased BMD.
Introduction
We have studied the possible involvement of vitamin K and D deficiency in the pathogenesis of decreased BMD in IBD.
Methods
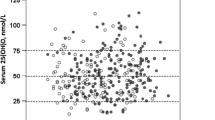
Seventy patients with IBD were evaluated for their BMD; plasma levels of vitamin K; phylloquinone (PK), menaquinone-7 (MK-7), and 25OH-D; serum PTH, protein induced by vitamin K absence (PIVKA-II), and undercarboxylated osteocalcin (ucOC) levels; and their food intake.
Results
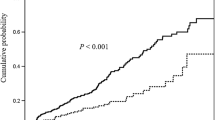
Compared with ulcerative colitis (UC) patients, CD patients had significantly lower plasma vitamin K and 25OH-D concentrations; significantly higher serum levels of PTH, PIVKA-II, and ucOC; and significantly lower BMD scores at almost all measurement sites. More IBD patients were vitamin K deficient in bone than in liver. Multiple regression analyses revealed that low plasma concentrations of vitamin K and 25OH-D were independent risk factors for low BMD and that they were associated with the patients’ fat intake, but not with their intake of these vitamins.
Conclusion
IBD patients have high prevalence of decreased BMD and vitamin K and D deficiency probably caused by malabsorption of these vitamins.
Similar content being viewed by others

References
Compston JE, Judd D, Crawley EO et al (1987) Osteoporosis in patients with inflammatory bowel disease. Gut 28:410–415
Bjarnason I, Macpherson A, Mackintosh C et al (1997) Reduced bone density in patients with inflammatory bowel disease. Gut 40:228–233
Ardizzone S, Bollani S, Bettica P et al (2000) Altered bone metabolism in inflammatory bowel disease: there is a difference between Crohn’s disease and ulcerative colitis. J Intern Med 247:63–70
Bjarnason I (1999) Metabolic bone disease in patients with inflammatory bowel disease. Rheumatology 38:801–804
Bartram SA, Peaston RT, Rawlings DJ et al (2006) Multifactorial analysis of risk factors for reduced bone mineral density in patients with Crohn’s disease. World J Gastroenterol 12:5680–5686
Schoon EJ, Müller MC, Vermeer C et al (2001) Low serum and bone vitamin K status in patients with longstanding Crohn’s disease: another pathogenetic factor of osteoporosis in Crohn’s disease? Gut 48:473–477
Vermeer C (1990) γ-Carboxyglutamate-containing proteins and the vitamin K-dependent carboxylasa. Biochem J 266:625–636
Booth SL (1997) Skeletal functions of vitamin K-dependent proteins: not just for clotting anymore. Nutr Rev 55:282–284
Feskanich D, Weber P, Willett WC et al (1999) Vitamin K intake and hip fractures in women: a prospective study. Am J Clin Nutr 69:74–79
Booth SL, Tucker KL, Chen H et al (2000) Dietary vitamin K intakes are associated with hip fracture but not with bone mineral density in elderly men and women. Am J Clin Nutr 71:1201–1208
Booth SL, Broe KE, Peterson JW et al (2004) Associations between vitamin K biochemical measures and bone mineral density in men and women. J Clin Endocrinol Metab 89:4904–4909
Szulc P, Chapuy M-C, Meunier PJ et al (1993) Serum undercarboxylated osteocalcin is a marker of the risk of hip fracture in elderly women. J Clin Invest 91:1769–1774
Cockayne S, Adamson J, Lanham-New S et al (2006) Vitamin K and the prevention of fractures: systematic review and meta-analysis of randomized controlled trials. Arch Intern Med 166:1256–1261
Bernstein CN, Bector S, Leslie W (2003) Lack of relationship of calcium and vitamin D intake to bone mineral density in premenopausal women with inflammatory bowel disease. Am J Gastroenterol 98:2468–2473
Duggan P, O’Brien M, Kiely M et al (2004) Vitamin K status in patients with Crohn’s disease and relationship to bone turnover. Am J Gastroenterol 99:2178–2185
Abreu MT, Kantorovich EA, Vasiliauskas EA et al (2004) Measurement of vitamin D levels in inflammatory bowel disease patients reveals a subset of Crohn’s disease patients with elevated 1,25-dihydroxyvitamin D and low bone mineral density. Gut 53:1129–1136
Driscoll RH, Meredith SC, Sitrin M et al (1982) Vitamin D deficiency and bone disease in patients with Crohn’s disease. Gastroenterology 83:1252–1258
Jahnsen J, Falch JA, Mowinckel P et al (2002) Vitamin D status, parathyroid hormone and bone mineral density in patients with inflammatory bowel disease. Scand J Gastroenterol 37:192–199
Vogelsang H, Klamert M, Resch H et al (1995) Dietary vitamin D intake in patients with Crohn’s disease. Wien Klin Wochenschr 107:578–581
Silvennoinen J (1996) Relationships between vitamin D, parathyroid hormone and bone mineral density in inflammatory bowel disease. J Intern Med 239:131–137
Bikle DD (2001) Osteoporosis in gastrointestinal, pancreatic, and hepatic diseases. In: Marcus R, Feldman D, Kelsey J (eds) Osteoporosis. 2nd edn. Academic, San Diego, CA, pp 237–258
Haderslev KV, Jeppesen PV, Sorensen HA et al (2003) Vitamin D status and measurements of markers of bone metabolism in patients with small intestinal resection. Gut 52:653–658
Lo CW, Paris PW, Clemens TL, Nolan J, Holick MF (1985) Vitamin D absorption in healthy subjects and in patients with intestinal malabsorption syndromes. Am J Clin Nutr 42:644–649
Krasinsk SD, Russell RM, Furie BC et al (1985) The prevalence of vitamin K deficiency in chronic gastrointestinal disorders. Am J Clin Nutr 41:639–643
Suhara Y, Kamao M, Tsugawa N et al (2005) Method for the determination of vitamin K homologues in human plasma using high-performance liquid chromatography-tandem mass spectrometry. Anal Chem 77:757–763
Kanis JA, Melton LJ 3rd, Christiansen C et al (1994) The diagnosis of osteoporosis. J Bone Miner Res 9:1137–1141
Todd KS, Hudes M, Calloway DH (1983) Food intake measurement: problems and approaches. Am J Clin Nutr 37:139–146
Davies M, Berry JL, Mee AP (2005) Bone disorders associated with gastrointestinal and hepatobiliary disease. In: Feldman D, Pike JW, Glorieux FG (eds) Vitamin D. 2nd edn. Academic, San Diego CA, pp 1293–1311
Holick MF (2007) Vitamin D deficiency. N Engl J Med 357:266–281
Ministry of Health, Labour, and Welfare, Japan (2005) Dietary reference intakes for Japanese. Daiichi Shuppan, Tokyo
Silvennoinen JA, Karttunen TJ, Niemelä SE et al (1995) A controlled study of bone mineral density in patients with inflammatory bowel disease. Gut 37:71–76
Motley RJ, Clements D, Evans WD et al (1993) A four-year longitudinal study of bone loss in patients with inflammatory bowel disease. Bone Miner 23:95–104
Sambrook PN (2006) Glucocorticoid-induced osteoporosis. In: Favus MJ (ed) (2006) Primers on the metabolic bone diseases and disorders of mineral metabolism. 6th edn. American Society for Bone and Mineral Research, Washington DC, pp 296–302
Nemetz A, Tóth M, García-González MA et al (2001) Allelic variation at the interleukin 1β gene is associated with decreased bone mass in patients with inflammatory bowel diseases. Gut 49:644–649
Moschen AR, Kaser A, Enrich B et al (2005) The RANKL/OPG system is activated in inflammatory bowel disease and relates to the state of bone loss. Gut 54:479–487
Sylvester FA, Wyzga N, Hyams JS et al (2002) Effect of Crohn’s disease on bone metabolism in vitro: a role for interleukin-6. J Bone Miner Res 17:695–702
Héla S, Nihel M, Faten L et al (2005) Osteoporosis and Crohn’s disease. Joint Bone Spine 72:403–407
Schurgers LJ, Teunissen KJ, Hamulyák K et al (2007) Vitamin K-containing dietary supplements: comparison of synthetic vitamin K1 and natto-derived menaquinone-7. Blood 109:3279–3283
Kaneki M, Hedges SJ, Hosoi T et al (2001) Japanese fermented soybean food as the major determination of the large geographic difference in circulating levels of vitamin K2: possible implications for hip-fracture risk. Nutrition 17:315–321
Beavan SR, Prentice A, Stirling DM et al (2005) Ethnic differences in osteocalcin γ-carboxylation, plasma phylloquinone (vitamin K1) and apolipoprotein E genotype. Eur J Clin Nutr 59:72–81
Tsugawa N, Shiraki M, Suhara Y et al (2006) Vitamin K status of healthy Japanese women: age-related vitamin K requirement for γ-carboxylation of osteocalcin. Am J Clin Nutr 83:380–386
Booth SL, Martini L, Peterson JW et al (2003) Dietary phylloquinone depletion and repletion in older women. J Nutr 133:2565–2569
Vermeer C, Gijsbers BL, Crācium AM et al (1996) Effects of vitamin K on bone mass and bone metabolism. J Nutr 126:1187S–1191S
Tangpricha V, Koutkia P, Rieke SM et al (2003) Fortification of orange juice with vitamin D: a novel approach for enhancing vitamin D nutritional health. Am J Clin Nutr 77:1478–1483
Bernstein CN, Blanchard JF, Leslie W, Wajda A, Yu N (2000) The incidence of fracture among patients with inflammatory bowel disease. A population-based cohort study. Ann Intern Med 133:795–799
Acknowledgement
This study was supported by the Health and Labor Science Research Grant entitled “Studies on the Dietary Reference Intakes (Recommended Dietary Allowance) for Japanese” (principal investigator, Professor Katsumi Shibata, The University of Shiga Prefecture, Shiga, Japan) from the Ministry of Health, Labor and Welfare, Japan.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kuwabara, A., Tanaka, K., Tsugawa, N. et al. High prevalence of vitamin K and D deficiency and decreased BMD in inflammatory bowel disease. Osteoporos Int 20, 935–942 (2009). https://doi.org/10.1007/s00198-008-0764-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-008-0764-2