Article Text

Abstract
Objective To describe the patient characteristics, diagnoses and clinical outcomes of patients presenting with acute upper gastrointestinal bleeding (AUGIB) in the 2007 UK Audit.
Design Multi-centre survey.
Setting All UK hospitals admitting patients with AUGIB.
Participants All adults (>16 years) presenting in or to UK hospitals with AUGIB between 1 May and 30 June 2007.
Results Data on 6750 patients (median age 68 years) was collected from 208 participating hospitals. New admissions (n=5550) were younger (median age 65 years) than inpatients (n=1107, median age 71 years), with less co-morbidity (any co-morbidity 46% vs 71%, respectively). At presentation 9% (599/6750) had known cirrhosis, 26% a history of alcohol excess, 11% were taking non-steroidal anti-inflammatory drugs and 28% aspirin. Peptic ulcer disease accounted for 36% of AUGIB and bleeding varices 11%. In 13% there was evidence of further bleeding after the first endoscopy. 1.9% underwent surgery and 1.2% interventional radiology for AUGIB. Median length of stay was 5 days. Overall mortality in hospital was 10% (675/6750, 95% CI 9.3 to 10.7), 7% in new admissions and 26% among inpatients. Mortality was highest in those with variceal bleeding (15%) and with malignancy (17%).
Conclusions AUGIB continues to result in substantial mortality although it appears to be lower than in 1993. Mortality is particularly high among inpatients and those bleeding from varices or upper gastrointestinal malignancy. Surgical or radiological interventions are little used currently.
- Acute gastrointestinal bleeding
- gastrointestinal endoscopy
- bleeding peptic ulcer
- aspirin
- audit
- gastrointesinal endoscopy
- gastrointestinal bleeding
Statistics from Altmetric.com
- Acute gastrointestinal bleeding
- gastrointestinal endoscopy
- bleeding peptic ulcer
- aspirin
- audit
- gastrointesinal endoscopy
- gastrointestinal bleeding
Significance of this study
What is already known about this subject?
Acute upper gastrointestinal bleeding (AUGIB) is a common medical emergency and is associated with a high mortality in those with significant medical co-morbidity, especially in those already hospital inpatients.
Since the previous large UK study in 1993, there have been substantive attempts to reduce the risk of AUGIB from peptic ulcer disease (Helicobacter pylori eradication, co-prescription of proton pump inhibitors), but also a rise in excess alcohol consumption in the UK.
What are the new findings?
Bleeding from varices appears to have become more common, accounting for 11% of cases and 20% of new admissions aged <60 years.
Surgical intervention is now uncommon, occurring in <2% of all cases of AUGIB.
Overall mortality remains significant at 10%, 7% in new admissions and 26% for inpatients.
How might it impact on clinical practice in the foreseeable future?
The implications for clinical practice are self-evident.
In many low-risk cases of AUGIB hospital admission might be avoided.
Introduction
Acute upper gastrointestinal bleeding (AUGIB) continues to be the most common gastrointestinal emergency and accounts for over 9000 deaths a year in the UK.1 The first nationwide audit of its management in the UK was carried out in 1993/4 and involved four English NHS health regions covering a population of about 16 million. Overall mortality was 14%, 11% for patients admitted with bleeding, rising to 33% for inpatients and appeared high compared to some but not all reports from other countries.2–5
Fourteen years on there have been important changes in aetiological factors as well as improvements in diagnosis and treatment of AUGIB. Strategies for decreasing toxicity from non-steroidal anti-inflammatory drugs (NSAIDs), Helicobacter pylori eradication and widespread use of proton pump inhibitor drugs (PPIs) have reduced the prevalence of peptic ulcer.6–9 The increasing prevalence of alcohol-related liver disease and the increasing age of the population (with associated co-morbidity) tend to worsen prognosis while these might be offset by increasing use of high dependency care and improvements in endoscopic haemostatic techniques.10–12
The second nationwide audit of the management of AUGIB, sponsored by the British Society of Gastroenterology and the National Blood and Transplant Service, was carried out in 2007 and attempted to cover the whole of the UK.13 This paper reports on the patient characteristics, endoscopic diagnoses and outcomes, including further bleeding, need for surgical or radiological intervention, length of stay and in-hospital mortality.
Methods
Participants
Two hundred and fifty-seven UK NHS hospitals accepting acute medical admissions were invited to participate. Hospitals were recruited by contacting the Medical Director and hospital Chief Executive in December 2006. Repeat invitations were sent to non-responders in February 2007. The study was advertised to gastroenterologists at the British Society of Gastroenterology (BSG) annual conference in March 2007, and further details were provided on the BSG and NHS Blood and Transplant (NHSBT) audit websites. Medical Directors were asked to confirm participation by supplying the name and contact details of the clinical lead for endoscopy in each hospital. In each hospital clinical leads then recruited and co-ordinated teams of case identifiers and data collectors and interacted with their clinical audit departments. A list of participating hospitals is given in online appendix 1.
Hospitals were asked to identify all cases of AUGIB in persons aged 16 years or over during a 2 month period, from 1 May to 30 June 2007. Both new admissions and patients who bled while in hospital for another reason were recruited. Case ascertainment occurred in two stages. First, case identifiers identified potential cases of AUGIB soon after presentation from hospital admissions units, endoscopy departments, blood transfusion laboratories, direct contact with wards and by staff response to posters. Second, sometime later, usually when a patient had been discharged or had died, data collectors abstracted the relevant data from the hospital records. At this point cases not meeting the entry criteria were excluded. For valid cases data were then entered on a secure website which could only be accessed using unique hospital identifiers and passwords. No patient identifying data were collected and the central investigators had no access to any patient records. To ensure that the methods of case ascertainment and data collection were robust and reliable they were piloted in six hospitals prior to the start of the study. Demographic data, clinical details, laboratory results, endoscopy reports and details of management including fluid and blood administration, endoscopic therapy, surgery and radiology details were obtained for each patient. Further details of the data collected are available at http://www.bsg.org.uk/clinical/general/uk-upper-gi-bleeding-audit.html.
Definitions
Definitions used in the study are provided in box 1. Significant co-morbidities affecting multiple systems were defined and quantified (graded 1–3) using criteria described in box 2. Particular care was taken to document the presence and severity of any co-morbidity, since this has been shown to be closely related to clinical outcome in AUGIB.14–16
Definitions used in study
Acute upper gastrointestinal bleeding
Haematemesis, the passage of melaena and/or firm clinical evidence and laboratory support for acute blood loss from the upper gastrointestinal (UGI) tract. Patients presenting with iron deficiency anaemia without evidence of acute upper gastrointestinal bleeding (AUGIB) were excluded.
Haematemesis
Vomiting of blood or blood clots. ‘Coffee ground’ vomiting only were included if it was witnessed by medical or nursing staff.
Melaena
The passage of dark tarry stools witnessed by medical or nursing staff, or discovered on rectal examination.
Alcohol excess
Consumption of more than 21 units per week for males and more than 14 units per week for females.
Rebleeding (further bleeding)
Further haematemesis, passage of fresh melaena, continuing or recurrent hypotension and tachycardia +/− fall in haemoglobin after the first endoscopy.
All cause mortality
Death occurring within the hospital admission up to 30 days post index AUGIB.
Definitions used to grade severity of co-morbidity
Ischaemic heart disease
Previous myocardial infarction, angina, cardiac arrhythmia, coronary intervention, coronary artery bypass graft.
Grade 1: more than 3 months ago
Grade 2: within 1–3 months
Grade 3: within the last month
Cardiac failure
Grade 1: documented history; unlimited exercise tolerance
Grade 2: breathless on exertion
Grade 3: breathless at rest
Respiratory disease
Chronic
Pulmonary fibrosis/chronic obstructive pulmonary disease/asthma/previous lobectomy/penuemonectomy/cystic fibrosis/fibrosing alveolitis/pulmonary hypertension/bronchiectasis/neuromuscular disease affecting pulmonary function (eg, motor neuron disease, myaesthenia gravis).
Grade 1: unlimited exercise tolerance when well
Grade 2: breathless on exertion
Grade 3: breathless at rest
Acute
Pneumonia/pulmonary embolus/pneumothorax/exacerbation of pre-existing chronic lung disease
Grade 2: admitted to general ward; not requiring ventilatory support
Grade 3: admitted to level 2 (HDU) or 3 (ICCU) care and/or requiring ventilatory support including non-invasive ventilation
Cancer
Grade 1: current diagnosis OR surgery or treatment for cancer in last 12 months AND no evidence of metastases or local recurrence
Grade 2: current diagnosis AND recent surgery, chemo- or radiotherapy (in last 12 weeks) or be undergoing investigation for metastases
Grade 3: current diagnosis; disseminated or incurable metastatic disease/palliative treatment
Stroke
Grade 1: stroke (>3 months ago), no significant deficit
Grade 2: stroke (>1 month ago) with significant neurological deficit (hemiparesis, dysphasia, hemianopia) OR stroke within 1–3 months with or without deficit
Grade 3: cerebrovascular event within 1 month (with or without significant deficit)
Dementia
Grade 1: documented dementia, living at home not requiring care package (independent) and or documented mini mental state examination (MMSE) score 26–30
Grade 2: documented dementia, living at home but requiring care package and or documented MMSE score 20–25
Grade 3: documented dementia, requiring full care package (dependent for activities of daily living) and or in residential or nursing care because of dementia AND OR documented MMSE <20 or abbreviated mental test score <6
Renal disease
Documented in admission or previous medical notes and not a diagnosis based on admission or presentation blood tests.
Cirrhosis
Previously documented in the medical notes (more than a history of alcohol excess or abnormal liver function tests on admission or at this presentation required).
Data handling
Data were exported electronically from the website into SPSS (Statistical Package for Social Sciences). Any duplicate cases were identified and removed from the data set prior to analysis. Dates (eg, date of admission, date of endoscopy, date of discharge) were checked and free-text comments about presentation and diagnoses were reclassified where possible. Clinical leads were contacted for clarification when necessary.
Risk assessment
Using the data submitted for each patient a pre-endoscopy (clinical) Rockall score based upon age, haemodynamic status and co-morbidity was calculated and for those undergoing endoscopy, a complete (post-endoscopic) Rockall score was calculated.14
Statistical methods
Data are presented as percentages with numerator/denominator and as summary statistics of median and inter-quartile ranges (IQR) or mean (SD) as appropriate. To adjust for similarities in practice and management within hospitals binary regression methods (using the ‘binreg’ command STATA 8, College Station, Texas, USA) were used throughout to calculate risk ratios and 95% CIs when assessing the association of clinical factors with outcome (inpatient mortality, re-bleeding, red blood cell transfusion). Risk ratios for type of admission, co-morbidity, history of alcohol abuse, were computed after adjusting for patient age (which was categorised automatically into quintiles for this purpose, cutting the data at 45, 61, 75 and 84 years).
Results
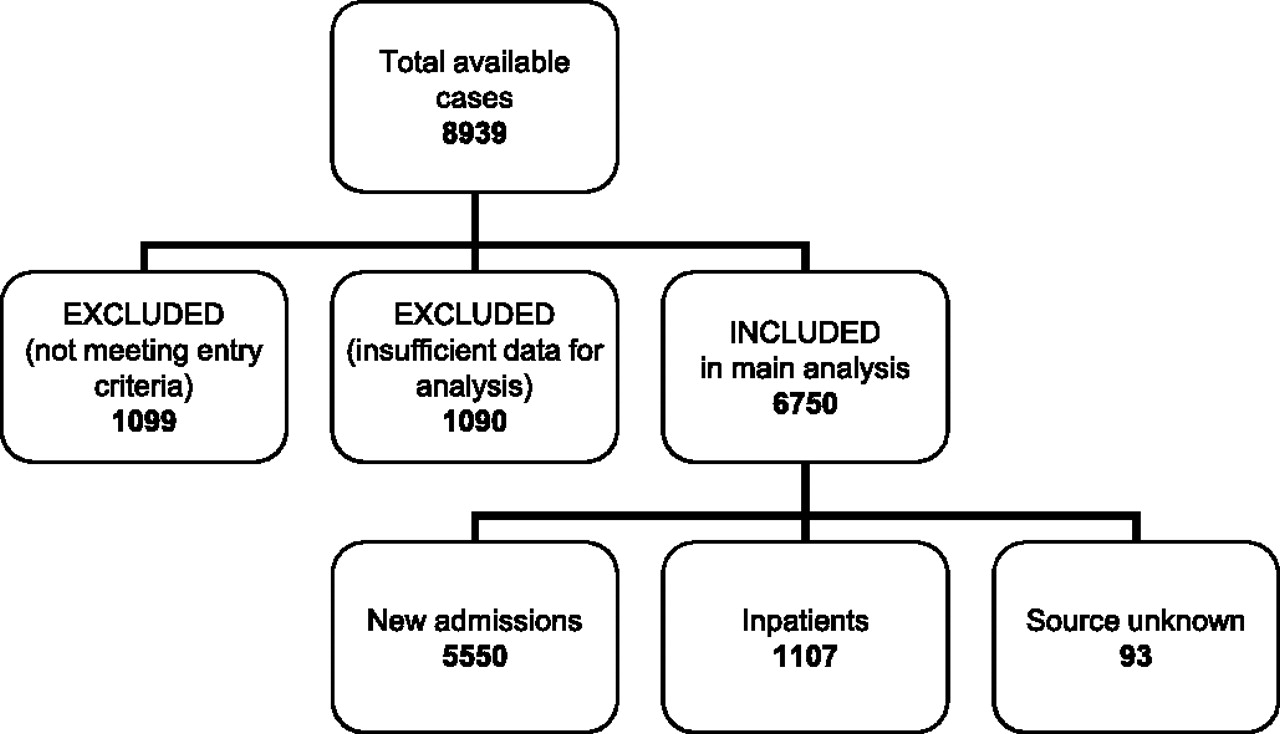
In all, 217/257 of the hospitals invited (84% of all acute admitting units in the UK) identified and registered 8939 cases or potential cases of AUGIB. Of these, 1099 were subsequently found not to meet entry criteria and were excluded by the local clinical leads (figure 1). A further 1090 cases were excluded because submitted data were incomplete; in 890 of these there were insufficient data to be able to confirm that gastrointestinal bleeding had occurred and in the other 200 only minimal data were submitted. Direct correspondence with hospitals submitting these cases revealed that time pressure, loss of case records or late realisation that entry criteria had not been met were the main reasons for incomplete data entry. A total of 6750 eligible cases from 208 hospitals therefore comprise the study sample for analysis. There were no major differences in age (median 68 vs 71 years) or gender (59% vs 55% male) between cases included (6750) and those excluded due to insufficient data (1090).
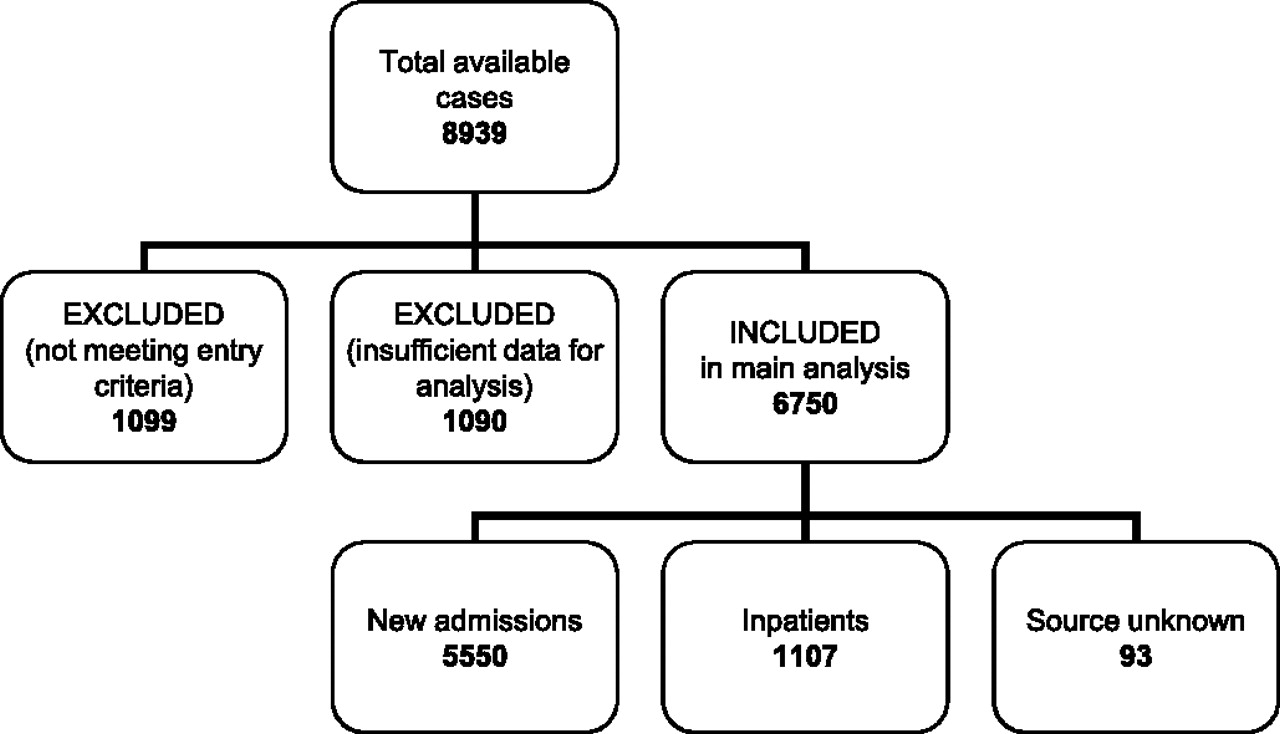
Flow chart showing numbers of excluded and included cases.
Missing data
For some cases included there was some data missing but not sufficient to preclude inclusion. For 93 (1.4%) patients it was not known whether they were a new admission or an inpatient at the time of presentation. There was no record of medication being taken at presentation for 285/5550 (5.1%) new admissions and 58/1107 (5.2%) inpatients. In 15 of the 5004 patients who underwent endoscopy there was no record of the endoscopic findings.
Patient characteristics
Patient characteristics including co-morbidity, magnitude of haemodynamic disturbance, laboratory findings and Rockall scores are summarised in table 1.
Patient characteristics
Patients admitted to hospital were younger than those already inpatients (median 65 vs 77 years), more frequently reported alcohol excess (28% vs 15%), but generally had less co-morbidity (46% vs 71%), were less shocked and had lower (better) pre-endoscopy Rockall scores than inpatients. The median (IQR) pre-endoscopy Rockall score (range 0–7) for all patients was 3 (IQR 1–4); for new admissions was 2 (IQR 1–4); and for inpatients was 4 (IQR 2–5).
Diagnoses
Upper gastrointestinal (UGI) endoscopy was performed in 74% (5004/6750) of patients during their hospital stay; In a further 1409 (21%) their audit record states that endoscopy was planned as an outpatient procedure.17 A cause of bleeding was identified from endoscopy in 83% (4139/5004). 30% (1526/5004) had more than one endoscopic diagnosis (table 2). Peptic ulcer disease was the commonest diagnosis (36%). Varices were the cause of bleeding in 11% (544/5004) although other endoscopic findings (particularly portal hypertensive gastropathy) were frequently also reported in this group of patients (345/544). Portal hypertensive gastropathy was reported in 275 but in only 25 was this an isolated finding and none of these patients died. Diagnostic findings varied by age, though age-specific diagnostic rates were broadly at similar levels for new admissions and inpatients.
Main endoscopic diagnoses by age group and type of presentation
Drug use
As shown in table 1 28% of all AUGIB patients had been taking aspirin at the time of presentation and 11% an NSAID. In the 4109 endoscoped new admissions 27% had been taking aspirin or an NSAID and of these 50% were also taking a PPI. Table 3 shows the pattern of use of aspirin, NSAIDs and PPI's according to endoscopic diagnoses.
Drug use recorded in new admissions endoscoped (n=4109)
Table 1 also shows that 7% were taking warfarin at time of presentation. In 30% (128/430, data missing in 43) the INR was recorded as being ≥5. Warfarin was stopped in 87% (400/549) and 50% (225/451) were given vitamin K in the first 24 h. Fresh frozen plasma was given at some point during their admission to 28% (133/473); in 23% of these cases the fresh frozen plasma (FFP) was recorded as being given alone. The endoscopic diagnoses in those on warfarin are shown in table 3.
Further bleeding (rebleeding)
Clinical evidence of further bleeding was reported in 13% (668/5004, 95% CI 12 to 14%) of patients following the first endoscopy and 183 of these (27%) died. Further bleeding rates for patients on aspirin (13%, 196/1479), warfarin (13%, 51/387) and NSAIDs (12%, 71/603) were similar to further bleeding rates in patients not taking any of these medications (14%, 389/2813). Rates of further bleeding and mortality according to diagnosis and drug use are shown in supplementary tables 10 and 11.
Surgery
Surgery was performed on 1.9% (127/6750, 95% CI 1.6 to 2.2%) of patients for AUGIB. The mean age was 69.4 years, 60% were male and the median (IQR) complete Rockall score for these patients was 6 (IQR 5–8). Most (82%, 104/127) had surgery for further bleeding with most of the remainder having surgery because of an associated perforation (12%) and malignancy (4%). Two-thirds (83/127) had over-sewing or under-running of an ulcer performed and over a half (69/127) of these operations were performed out of hours. Post-operative mortality was 30% (38 deaths following 127 operative procedures, 95% CI 22 to 38%).
Interventional radiology
Eighty-four patients (1.2%) underwent interventional radiology for AUGIB. Twenty-two patients underwent mesenteric angiography and embolisation for non-variceal bleeding and six underwent trans-jugular intrahepatic porto-systemic shunt (TIPSS) insertion for variceal bleeding. The median post-endoscopy Rockall score for patients undergoing any interventional radiological therapeutic procedure was 5 (IQR, 3–7). Mortality was 17% (14/84).
Blood transfusion
Forty-three per cent (2922/6750) of patients received a red blood cell (RBC) transfusion for AUGIB and in 33% (2241/6750) of cases this was within 12 h of presentation (77% (2241/2922) of all transfusions).18
Duration of stay
The median length of stay (LOS) to discharge was 5 days (IQR, 2–12) for new admissions and 18 days (IQR 8 to>28) for inpatients. Figure 2 shows the relationship between median length of stay and complete Rockall score for all patients.

The relationship between complete Rockall score and length of stay following presentation (new admissions and inpatients combined who were discharged alive).
Hospital mortality
Unadjusted mortality was 10% (675/6750, 95% CI 9.3 to 10.7%); 6.8% (379/5550, 95% CI 6.2 to 7.5%) for new admissions and 26% (288/1107, 95% CI 23 to 29%) for inpatients. Of the deaths, 45% (304/675) occurred in patients who did not have UGI endoscopy. Mortality among patients undergoing endoscopy was 7.4% (371/5004, 95% CI 6.7 to 8.1%). The relative excess mortality for inpatients was at a similar level irrespective of whether patients had an endoscopy (table 4).
Crude mortality by endoscopic diagnosis
The majority (1266/1745) of those with a history of alcohol excess were under 60 years of age. The age-adjusted mortality ratio overall for those with such a history was 1.80 (95% CI 1.49 to 2.17) and was highest in those with cirrhosis. For other co-morbidities, grade 3 cardiac failure, respiratory disease, stroke and malignancy were associated with a twofold or higher risk of death.
Clinical outcomes and Rockall scores
Mortality was strongly associated with increasing clinical (pre-endoscopy) and complete Rockall scores as shown in tables 5 and 6 and figure 3. High complete Rockall scores were also associated with further bleeding (table 6 and figure 3). A low clinical and complete Rockall score reliably identified those at low risk of a poor outcome whereas high scores identified up to a 33-fold increase in risk of in-hospital mortality and up to a 7.52-fold risk of further bleeding (table 6). Of the five deaths in patients with a clinical Rockall score of zero further enquiry revealed that in three the score was correct but in the other two mention of serious co-morbidity had been omitted from the data submitted to the website resulting in a falsely low score.
Mortality by pre-endoscopy (clinical) Rockall score, all patients
Mortality, further bleeding and red blood cell (RBC) transfusion rates by complete Rockall score (patients undergoing inpatient endoscopy)

{kind=link}
{kind=link}
{kind=link}
The relationship between complete Rockall scores and further bleeding, red blood cell (RBC) transfusion, crude mortality rates.
There was a fivefold difference in transfusion rates between patients with a low and high Rockall score. While over 70% of patients with a complete score greater than five received a RBC transfusion 27% (379/1408) of patients with a complete Rockall score of 2 or less also received transfusion even though further bleeding was only noted in 5% (69/1408) and only 13 (0.9%) died (table 6).
Discussion
This is the largest survey of AUGIB yet performed in the UK and has defined its causes and outcomes in 2007. Many of the findings were expected; for example, patients were generally elderly, with a median age of 68 years and one in four were aged over 80 years. Almost half of the patients had significant co-morbidity; ischaemic heart disease was particularly common, being present in almost a fifth of patients, while respiratory, renal and neurological diseases were also prevalent. One in three new admissions was taking aspirin, clopidogrel or warfarin. Many patients had multiple co-morbidities placing them at particularly high risk of death. As anticipated, there was a strong association between the severity of co-morbidities and mortality. The study confirmed the well-established observations that death following AUGIB is unusual in the absence of co-morbidity and that mortality is very low in otherwise healthy individuals aged less than 60 years. The much higher mortality observed in patients who bled as in patients compared to those who were admitted because of bleeding reflects this.
Perhaps surprising was the observation that 9% of cases occurred in patients already known to have cirrhosis. This has considerable service implications since patients who bleed in association with liver disease tend to be sicker, develop more complications and have a longer hospital stay than patients who do not have liver disease. The most frequent cause of liver disease in this series was almost certainly alcohol abuse with 28% of all new admissions with AUGIB admitting to drinking more than the recommended safe amounts of alcohol.
It may also seem surprising that only 74% of cases underwent endoscopy during their hospital admission. There appeared to be two reasons for this. First, in a significant number endoscopy was thought futile or inappropriate. In 7% (125/1746) the hospital records stated that no active investigation or treatment was indicated and, compared with those who did undergo endoscopy, a greater proportion of those who did not undergo endoscopy suffered from dementia (11% vs 4%), and stroke (10% vs 7%).17 Second, in many low-risk patients endoscopy was planned after hospital discharge. We were unable to collect data on how often this actually occurred but this was the stated intention in 22% (389/1746). In a further 5% (96/1746) patients discharged themselves before endoscopy was performed.
The commonest endoscopic diagnosis was peptic ulcer bleeding; the observed figure of 36% in this survey is similar to that reported in earlier series of AUGIB.5 19–23 This contrasts with the dramatic fall in prevalence of uncomplicated peptic ulcer and presumably reflects the widespread use of aspirin for vascular disease rather than NSAID use for which the prevalence of use was low at only 12%.8 9 24 Perhaps less expected is that variceal bleeding now accounts for 11% of all cases and was found in 20% of new admissions aged <60. The frequency of variceal bleeding has more than doubled since the last AUGIB audit of 1995, almost certainly the consequence of alcohol abuse in the UK.10 The 17% with no abnormality found at endoscopy is lower than the 25% figure reported in the 1993 audit (table 7) but is still almost twice that reported from most UK centres with units dedicated to AUGIB19–22 although not all.23 Endoscopy will have been performed more promptly in these hospitals so reducing the possibility of normal findings.25
Comparison of first and second UK audits
Re-bleeding or further bleeding was noted in 13%, a figure which is a little lower than the 16% recorded in the 1993 audit but similar to that reported in other recent series, recognising that this outcome is based on clinical assessment.5 21 23 25 Nevertheless, rebleeding rates of 20–30% were commonly reported in studies from more than 20 years ago suggesting that measures to prevent further bleeding have had an impact on mortality even though only a third of the deaths in this audit were attributed to AUGIB by the clinicians involved26–29 There was a strong relationship between increasing complete Rockall score and further bleeding as well as with mortality. As expected, patients with the highest Rockall scores (and co-morbidity) were more likely to have red cell transfusion. However, after adjusting for Rockall scores an intriguing outcome from this audit reported elsewhere was that red cell transfusion was associated with a higher risk of re-bleeding and death.18
Fewer than 2% of patients underwent a surgical operation and only a handful of cases was subjected to an interventional radiological procedure. This is especially remarkable considering that surgical rates of over 20% were commonplace in the 1970s and as recently as 20 years ago rates of 15–20% were being reported.19 27 30 31 The decline in surgery appears to coincide with the increasing availability and use of therapeutic endoscopy. This implies that many patients who re-bled received successful endoscopic therapy and/or effective drug therapy since it is well established that a significant proportion of patients who re-bleed do not achieve spontaneous haemostasis.19 30 Surgery has become a last resort measure with a predictably high mortality. Nevertheless, the high post-operative mortality reported in this series (30%) must raise questions as to the timing (and possibly the expertise) of surgical intervention. While the efficacy of arterial embolisation for peptic ulcer bleeding has been demonstrated in several case series, it was striking that interventional radiological procedures were minimally used.32 33 This may reflect a lack of availability of appropriate radiological facilities and expertise, particularly out of normal working hours.
Comparison of the findings of the current audit with those of the first UK audit is inevitable and unavoidable. Before such comparisons are made it is important to recognise the differences in methodology and scope of the two studies. The earlier audit was paper based, relied on hospital audit staff for much of the data collection, used less detailed and precise recording of co-morbidity, covered only four English regions and included a greater proportion of patients living in deprived areas. The current audit included far more patients, data collection was undertaken by specific clinical staff, documentation of co-morbidity and laboratory findings was more assiduous and the study group was demographically wide. Nonetheless, it is probable that some cases of AUGIB were not captured in the current audit since the number of recorded cases varied greatly between contributing hospitals with some institutions collecting relatively small numbers of patients in comparison to other hospitals that served similar populations. Despite these differences, the age ranges, distribution of Rockall scores and endoscopic diagnoses were remarkably similar (table 7). The striking changes are the lower overall mortality for both new admissions and inpatients in 2007 as well as the greater proportion with variceal bleeding but with a lower mortality for variceal bleeding.
Do these changes reflect real improvements in prognosis or might they be explained by incomplete and variable AUGIB case ascertainment in some hospitals? To explore how incomplete case ascertainment might have influenced our conclusions, mortality was recalculated after removing data from hospitals that submitted the fewest cases. Removing in turn the lowest 5% (n=10), 10% (21) and 25% (52) of the 208 hospitals that submitted cases resulted in no change of overall mortality and a less than 1% reduction in mortality after risk adjustment.34 Three studies using UK hospital episode statistics (HES) provide support for at least some of the reduction in mortality being real. Using the Scottish HES Kang et al found that between 1982 and 2002 mortality (case-fatality rates) almost halved for gastric and peptic ulcer bleeding, although for duodenal ulcer bleeding the picture was mixed with declines seen in men but not women.35 More recently, Crooks et al have analysed mortality trends in similar data for England for 1999–2005 and found small declines in the younger age groups after adjusting for sex and co-morbidity but not in those aged 80 years or more.1 A similar HES analysis for Wales has found that their age and sex adjusted case-fatality rates have declined from 11.4% in 1999–2000 to 8.6% in 2006–2007.36
It is likely therefore that the outcome of patients developing AUGIB has improved in the 14 years between the two audits. This has occurred despite an increase in variceal bleeding and suggests that improvements in management have translated into lower mortality. It is obviously not possible to determine whether any one change in practice is most important, but it is reasonable to speculate that reduction in the need for surgery, with the inevitable risk of post-operative complications, by appropriate pharmacological and endoscopic therapies has been a major factor. The UK cannot, however, be complacent about such improvements, whether or not they reflect better training and service provision: the overall mortality remains appreciably higher than the best outcomes reported from some large population-based studies from other countries.37–40
Acknowledgments
The authors are grateful to the NHS Blood and Transplant Service and the British Society of Gastroenterology for funding the clinical research fellow to undertake this study. We would also like to thank Professor Tim Rockall for his input into the initial design of this study and recommendations for analyses.
References
Supplementary materials
Online only appendix
Files in this Data Supplement:
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online tables
Footnotes
Funding The clinical research fellow was funded by NHS Blood and Transplant and the British Society of Gastroenterology. No other funding was obtained. Professor M Murphy and Dr K Palmer are representatives of the NHS Blood and Transplant Service and the British Society of Gastronenterology, respectively, and were instrumental in obtaining the funding for the clinical research fellow for this audit to be conducted. The participating hospitals and clinicians received no funding.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.