Article Text

Abstract
Introduction In pancreatic cancer, preoperative biliary drainage (PBD) increases complications compared with surgery without PBD, demonstrated by a recent randomised controlled trial (RCT). This outcome might be related to the plastic endoprosthesis used. Metal stents may reduce the PBD-related complications risk.
Methods A prospective multicentre cohort study was performed including patients with obstructive jaundice due to pancreatic cancer, scheduled to undergo PBD before surgery. This cohort was added to the earlier RCT (ISRCTN31939699). The RCT protocol was adhered to, except PBD was performed with a fully covered self-expandable metal stent (FCSEMS). This FCSEMS cohort was compared with the RCT’s plastic stent cohort. PBD-related complications were the primary outcome. Three-group comparison of overall complications including early surgery patients was performed.
Results 53 patients underwent PBD with FCSEMS compared with 102 patients treated with plastic stents. Patients’ characteristics did not differ. PBD-related complication rates were 24% in the FCSEMS group vs 46% in the plastic stent group (relative risk of plastic stent use 1.9, 95% CI 1.1 to 3.2, p=0.011). Stent-related complications (occlusion and exchange) were 6% vs 31%. Surgical complications did not differ, 40% vs 47%. Overall complication rates for the FCSEMS, plastic stent and early surgery groups were 51% vs 74% vs 39%.
Conclusions For PBD in pancreatic cancer, FCSEMS yield a better outcome compared with plastic stents. Although early surgery without PBD remains the treatment of choice, FCSEMS should be preferred over plastic stents whenever PBD is indicated.
Trial registration number: Dutch Trial Registry (NTR3142).
- ABDOMINAL SURGERY
- PANCREAS
- ADENOCARCINOMA
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Hyperbilirubinemia is associated with postoperative morbidity and mortality.
Early surgery is the standard preference in most patients suffering from jaundice with a resectable pancreatic tumour.
Uncovered metal stents are used frequently as palliative treatment in patients suffering from jaundice with non-resectable pancreatic cancer.
What are the new findings?
Fully covered self-expandable metal stent (FCSEMS) are superior to plastic stents during preoperative biliary drainage.
Occlusion and stent exchange is rare when using FCSEMS during preoperative biliary drainage.
How might it impact on clinical practice in the foreseeable future?
This study provides evidence that an FCSEMS should be used routinely during preoperative biliary drainage.
Introduction
For decades, there has been debate among gastroenterologists and surgeons as to whether patients suffering from jaundice with a resectable periampullary or pancreatic tumour should undergo preoperative biliary drainage (PBD) to reduce postoperative morbidity and mortality associated with hyperbilirubinemia.1–5 With regard to the ongoing controversy between the benefits and adverse effects of PBD, a multicentre randomised controlled trial (RCT) (ISRCTN31939699) was conducted comparing a strategy of endoscopic PBD followed by surgery, with a strategy early surgery, which was published in 2010.6 Significantly more serious complications occurred in patients who underwent PBD (74%) compared with those who went for early surgery (39%). This difference in overall complication rate was largely due to a high rate of complications owing to PBD. In this regard, criticism towards the RCT concentrated on the technique of PBD; according to clinical practice at the time the RCT was performed, plastic stents were used, while currently self-expandable metal stents (SEMS) are considered superior.7–10 Most studies reporting on the use of SEMS to relieve jaundice, however, deal with non-surgical patients receiving palliative treatment.11 Studies on SEMS usage in surgical patients are limited, small and retrospective.12–18
There is evidence in favour of early surgery as the standard treatment in patients without extreme hyperbilirubinemia who will not undergo neoadjuvant treatment, as confirmed by a recent Cochrane review and meta-analysis.3 ,19 However, implementation of these results is not fully completed; some hospitals not performing pancreatic surgery still refer patients after they performed PBD. Further work is needed. Initiating new randomised trials comparing PBD with SEMS followed by surgery versus early surgery (without drainage) with the same inclusion criteria (limiting bilirubin levels) would be considered controversial by most since these patients would be withheld from the preferred treatment. However, early surgery is not feasible in all patients. Performing a methodological sound prospective study, superior to other existing retrospective studies, will allow a better management for these patients. Therefore, this multicentre prospective cohort study was performed, including patients suffering from jaundice undergoing PBD with fully covered self-expandable metal stents (FCSEMS) and incorporating the cohort from the previous RCT with identical inclusion criteria. The aim of this study was to establish the superiority of SEMS during PBD compared with the plastic stents, with respect to PBD-related complications. After this study, the possibility of new randomised trials in selected patients on the potential value of SEMS in the preoperative setting in patients can be explored.
Methods
Study design
Patients with obstructive jaundice due to a resectable periampullary or pancreatic tumour scheduled to undergo PBD before curative resection were included. Inclusion criteria were identical to the criteria used in the RCT in order to create a similar cohort:6 ,20 serum bilirubin level of 40–250 µmol/l before inclusion or on the day of inclusion, CT without evidence of distant metastases or extensive local tumour ingrowth into portal or mesenteric vessels (ie, maximum 180° of the circumference) and scheduled for surgical treatment in one of the participating centres. Patients over the age of 85 years, with a Karnofsky index<50%, who had undergone previous endoscopic or percutaneous PBD with stent placement, who were to receive neoadjuvant chemotherapy or who suffered from severe gastric outlet obstruction were excluded.20
Indication for resection was set during a patient’s visit to the outpatient clinic in hospitals performing pancreatic surgery, the patient was discussed in a multidisciplinary team and a decision was made on the recommended treatment. When a pancreaticoduodenectomy was indicated in a jaundiced patient, early surgery without prior drainage was the preferred treatment. patients suffering from jaundice were only eligible for the current trial and underwent PBD in case inclusion criteria were met and they could not undergo early surgery: due to logistical hurdles (waiting list, referral pattern, diagnostics). These patients were treated with an FCSEMS to alleviate the biliary obstruction. Because pathological conformation was not a requirement for inclusion and around 7% of the patients, who had a high suspicion for malignant obstruction on imaging, appear to have benign disease during the course,21 an FCSEMS has been chosen as these stents can always be removed in case needed.
In the previous RCT, patients suffering from jaundice were randomised and assigned to either preoperative drainage followed by surgery or early surgery. In the present study, the FCSEMS cohort was added to the preoperative drainage versus early surgery cohorts of the RCT. Comparison was made between the current FCSEMS group and the historical RCT plastic stent group. This comparison was justified based on the similar inclusion criteria used keeping baseline patient characteristics similar. Primary outcome measure was the PBD-related complication rate.
Study oversight
This was a prospective observational multicentre cohort study using a historical cohort conducted in the Netherlands by three regional and four academic hospitals that were also involved in the previous preoperative drainage versus early surgery trial. A local study coordinator responsible for recruiting patients according to the inclusion criteria was appointed in every hospital.
Endoscopic PBD and surgery
In both academic and regional hospitals, experienced gastroenterologists performed the endoscopic PBD by placing a fully covered biliary stent (WallFlex stent, Boston Scientific). Performing a papillotomy and the length of the FCSEMS was decided upon by the treating physician and tailored to the length of the stricture. Unsuccessful endoscopic retrograde cholangiopancreatography (ERCP) was followed by a second attempt with plastic stent or a percutaneous transhepatic cholangiography with biliary drainage. In line with the previous RCT, successful drainage was defined as a decrease of 50% of the serum bilirubin within two weeks following PBD. No per-protocol criteria were set for SEMS size as this depended on the stricture. The plastic biliary stent was 10 Fr in size.6
Surgery was performed in hospitals performing >20 resections per year according to the new regulations for pancreatic surgery in the Netherlands, being the same hospitals as in the preoperative drainage versus early surgery RCT. Pylorus preserving pancreatoduodenectomy or Whipple–Kausch pancreatoduodenectomy was performed in case no metastases or arterial involvement was evident. In case of (limited) portal venous involvement, resection of the vein was performed.22 ,23 After resection, a pancreaticojejunostomy (PJ), hepaticojejunostomy (HJ) and gastro or duodenoenterostomy were performed. A silicon drain was placed near the PJ and HJ. If metastases or local unresectability were encountered during surgery, biopsies were taken and a palliative bypass procedure was performed. Definitive diagnosis was based on pathology examination of biopsies performed during surgery, the resection specimen or biopsies performed preoperatively.
Evaluation of outcome
Definition of complications and outcome parameters were equal to those in the preoperative drainage versus early surgery RCT.20 The primary outcome parameter was the rate of preoperative drainage-related complications after endoscopic drainage using FCSEMS during the interval period up to surgery (pancreatitis, cholangitis, perforation, haemorrhage, stent exchange or occlusion). Secondary endpoints were other complications up to 120 days after inclusion. These included PBD-related complications and surgical complications being anastomotic leakage, intra-abdominal abscesses, delayed gastric emptying, wound infection, portal vein thrombosis, readmission due to surgical complications, mortality and any complications requiring reintervention. Complications other than these were defined as complications outside protocol. Data were derived from patients’ charts.
Sample size and statistical analysis
The expected PBD-related complication rate when using SEMS was based on a meta-analysis of palliative drainage comparing covered and uncovered SEMS in non-surgical patients.24 Average complication rate of preoperative drainage by using SEMS was around 26% and 46% by using a plastic stent, as derived from the RCT. With nQuery Advisor, a post hoc power analysis was performed with the number of patients included in this study and the drainage-related complication rate, using a continuity corrected χ2 test.25
FCSEMS versus plastic stent: A per-protocol comparison of the primary outcome PBD-related complications between the FCSEMS cohort and the plastic stent cohort was performed using a two-sided χ2 test. P values, 95% CI and relative risks were given. Fisher's exact was shown in case cell count was <5.
FCSEMS versus plastic stent versus early surgery: A comparison of secondary outcomes (overall complications) between the FCSEMS group, plastic stent group and early surgery group was also performed, with the connotation that the sample size was not powered to detect significant differences in this three-group comparison.
Kaplan–Meier estimates were used to depict the longitudinal incidence rate of complications during follow-up of both the FCSEMS and the plastic stent cohorts. Categorical data were analysed using χ2 test, and Student's t test and Mann–Whitney U were used for analysing continuous data. A logistic regression analysis was performed, adjusted for age, gender, body mass index, bilirubin level and pathology, to denote the risk of PBD-related complications in the FCSEMS group compared with the plastic stent group and limit the influence of confounding. A p value of <0.05 was considered significant.
Results
Between 2011 and 2014, 53 patients were examined for eligibility. Prior to any analysis, four patients were wrongfully included; they did not match the eligibility criteria. One patient was considered not resectable, one patient had severe comorbidity precluding operation and two patients were enrolled in a neoadjuvant therapy protocol (NTR3709). The remaining 49 patients were included for analysis; all patients completed follow -p of 120 days. A post hoc power calculation with a power of 80% and a two-sided α of 0.05 and assuming a 46% proportion in group 1 with a group size of 102 (plastic stent group) and a group size for the second group of 49 (metal stent group), we can detect a significant difference from 46% if the percentage in group 2 (metal stent group) is ≤21.5%. Patients who underwent PBD with FCSEMS were compared with patients assigned to PBD with plastic stents (n=102) in the preoperative drainage versus early surgery RCT. In this trial, 202 patients underwent randomisation, 102 patients were assigned to preoperative drainage followed by surgery, 94 patients underwent early surgery and 6 patients were excluded. Patients’ characteristics of both groups are depicted in table 1. No differences were seen between the groups, although preoperative bilirubin was 176 μmol/L in patients with an FCSEMS vs 154 μmol/L in patients who received a plastic stent (p=0.04, Mann–Whitney U). Papillotomy was performed in 53% of patients in the FCSEMS group and in 42% of patients in the plastic stent group. All SEMS were 10 mm in diameter, and most stents were 6 cm long. There were three stents of 4 cm and one of 8 cm.
Patients’ characteristics and diagnosis reported in the FCSEMS cohort and the plastic stent cohort in the preoperative drainage versus early surgery RCT
PBD with FCSEMS was performed successfully after the first attempt in 43 patients (88%), in 3 patients cannulation of the biliary duct was not achieved, a second ERCP was performed successfully using an FCSEMS (n=2) and 1 patient received percutaneous transhepatic drainage. In the remaining three patients, inadequate drainage despite the FCSEMS in situ was resolved by placement of an extra plastic stent due to occlusion of the FCSEMS in two patients; in the third patient, no stent occlusion was seen and follow-up was performed. Time to surgery was 5.3 weeks and did not differ compared with patients in the plastic stent group, 5.2 weeks. After PBD, surgical exploration was performed in all but one patient who declined surgery. Eight patients who underwent PBD with FCSEMS underwent palliative bypass (17%), the remaining 40 patients underwent resection. Resection was performed with the FCSEMS in situ. No perioperative problems were encountered due to the FCSEMS placement. Resection rate was higher compared with patients in the plastic stent group, 82% vs 56% (p=0.004).
FCSEMS versus plastic stent
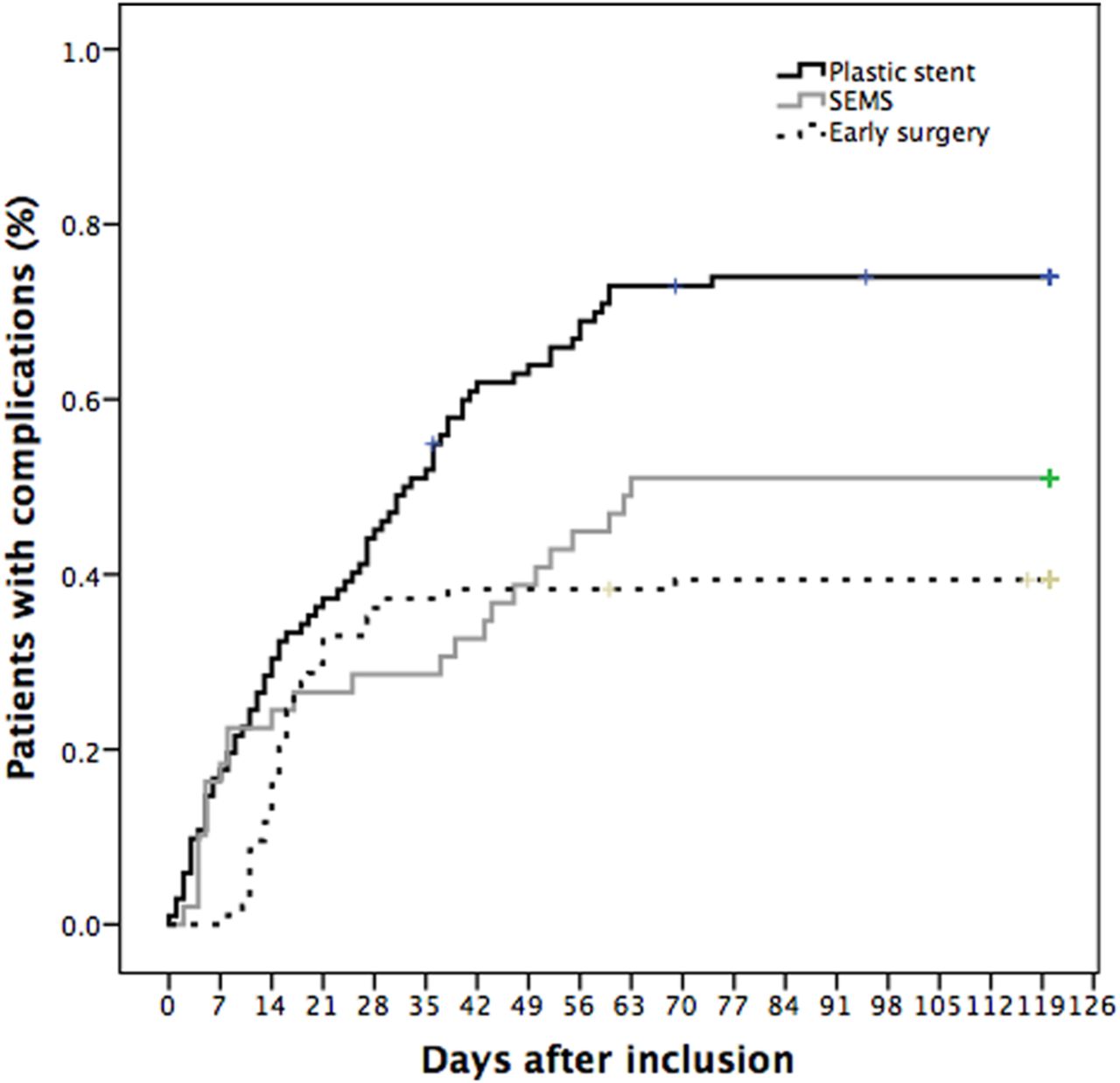
Data on primary and secondary outcomes were available in all patients. PBD-related complications occurred in 12 patients in the FCSEMS group (24%) compared with 47 patients in the plastic stent group (46%), with a relative risk of 1.9 (95% CI 1.1 to 3.2, p=0.011). After adjustment for age, gender, body mass index, bilirubin level and pathology, the odds of PBD-related complications in the plastic stent group compared with the FCSEMS group was 3.5 (95% CI 1.4 to 8.8, p=0.009). Bilirubin was no independent predictor for PBD-related complication (OR 0.99, 95% CI 0.9 to 1.1, p=0.395). Furthermore, patients were divided into two subgroups: higher and lower than the median bilirubin (median=167 mmol/L). No difference in complications was seen between both groups. The proportion of patients with PBD-related complications is illustrated in figure 1. Stent-related complications were reported in 3 patients (stent occlusion and subsequent papillotomy (n=1), stent occlusion and subsequent exchange (n=1), stent dysfunction and exchange (n=1)) in the FCSEMS group (6%) compared with 31 patients in the plastic stent group (30%). PBD complications and complications related to surgery are depicted in table 2. Post-ERCP pancreatitis occurred in nine patients after FCSEMS placement (18%), eight cases of mild and one severe pancreatitis. No differences were found between surgical complications in the FCSEMS and plastic stent group, that is, 40% vs 47%. In the FCSEMS group, time to surgery in patients with PBD-related complications was 4 days longer compared with patients without complications; in the plastic stent group, there was a 3-day difference (median).
Preoperative and postoperative complications reported in the FCSEMS cohort and the plastic stent cohort in the preoperative drainage versus early surgery RCT

Preoperative biliary drainage (PBD) complications from date of inclusion up to surgery in patients suffering from jaundice with resectable periampullary or pancreatic cancer undergoing biliary drainage prior to surgery. SEMS, self-expandable metal stent.
The secondary outcomes after PBD and surgery are shown in table 3. Overall complications including PBD and surgical complications were lower in the FCSEMS group compared with the plastic stent group (p=0.006). Non-protocol complications, preoperative and postoperative readmissions, and mortality did not differ significantly. However, mortality due to any cause within 120 days after inclusion was 6% in the FCSEMS group and 15% in the plastic stent group (p=0.128). Hospital stay, including readmissions, was shorter in the FCSEMS group, 12 vs 16 days. Data on pathology findings perineural invasion and vasoinvasive growth were not available for all patients.
Secondary outcomes reported in the FCSEMS cohort and the plastic stent and early surgery cohort in the preoperative drainage versus early surgery RCT
FCSEMS versus plastic stent versus early surgery
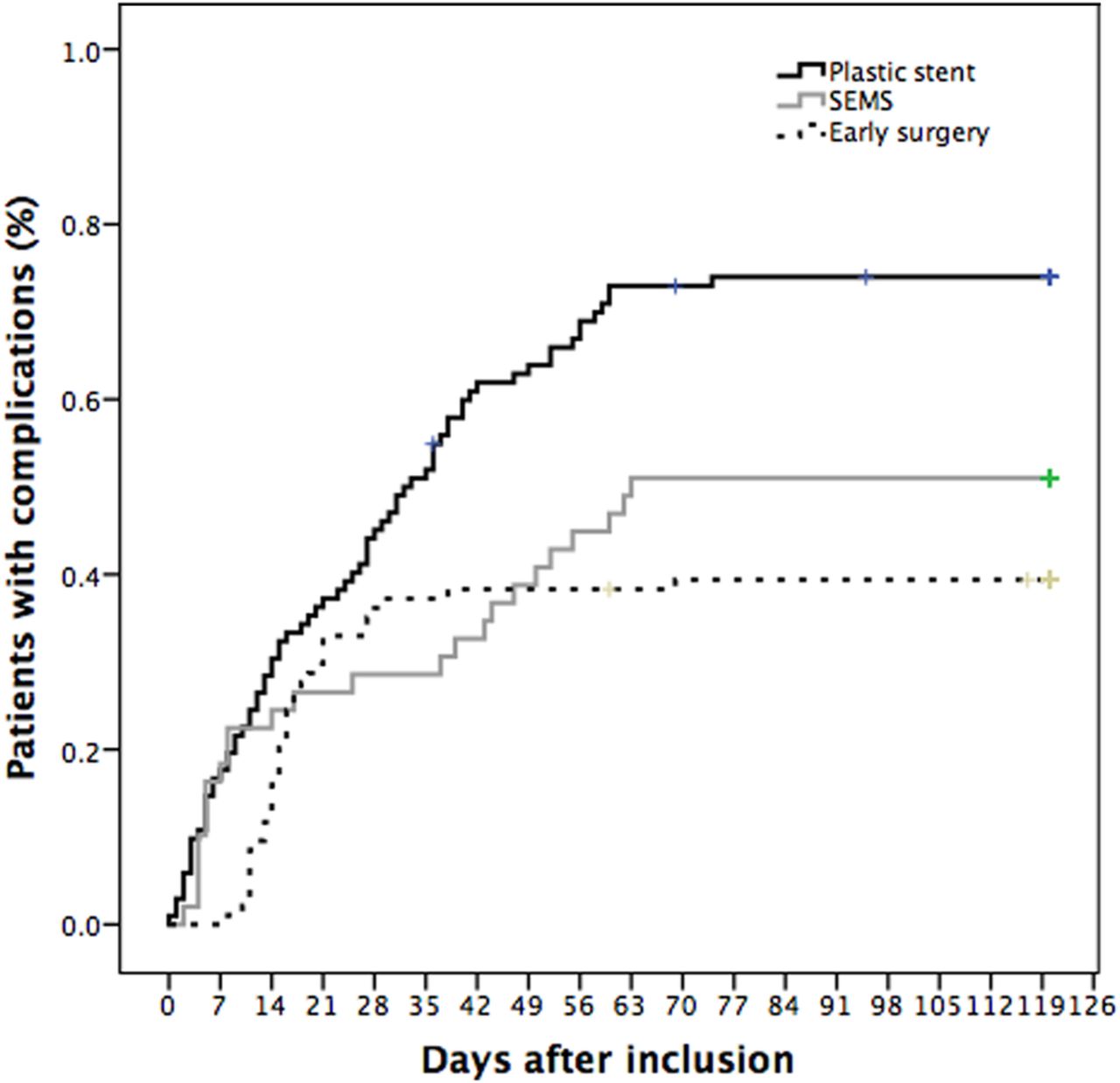
To demonstrate the possible outcome when comparing the FCSEMS cohort with the early surgery cohort in the preoperative drainage versus early surgery RCT, the early surgery group was added in table 3. Overall complication rate was highest in patients who had undergone PBD with plastic stent (74%) compared with 51% and 39% in the FCSEMS group and early surgery group. The proportion of patients with overall complications, related to PBD and surgery, in the FCSEMS, plastic stent and early surgery groups is illustrated in figure 2.
{kind=link}
{kind=link}
Overall complications (preoperative biliary drainage and surgery related) reported in the fully covered self-expandable metal stent (SEMS) cohort and the plastic stent and early surgery cohort in the preoperative drainage versus early surgery randomised controlled trial.
Discussion
This study compared the outcome after PBD with metal stents (FCSEMS) versus plastic stent in patients suffering from jaundice with a resectable pancreatic or periampullary tumour. FCSEMS were superior; PBD complications were reported in 25% compared with 46% of patients who received a plastic stent. Stent-related complications were observed in 6% vs 30%, respectively. The risks of both PBD and stent-related complications were lower in patients who received an FCSEMS. Overall complication rates were lower in the FCSEMS group compared with the plastic stent group owing to the low rate of PBD-related complications. No differences in surgical complications were seen between the FCSEMS and plastic stent groups. PBD with FCSEMS was performed successfully in 43 patients (88%) at the first attempt, and all patients were adequately drained after the first or a second attempt. No perioperative problems were encountered due to placement of the FCSEMS.
Despite its prospective and multicentre design, the present study has limitations. According to the post hoc power analysis, a significant difference from 46% of PBD-related complications in the plastic stent group would be detected if the percentage in the metal stent group was ≤21.5%. Our study showed a 24.5% complication rate in the metal stent group, higher than the calculated 21.5%. Therefore, the current study is insufficiently powered. Nevertheless, the clinical relevance of the observed significant reduction of complications from 46% in the plastic stent group to 24.5% (p=0.012) in the metal stent group is obvious. By performing a two-sided test with an α of 0.05, we accept a chance of 5% to detect a false positive effect concerning the primary hypothesis; PBD-related complication rate is lower in the metal stent group compared with the plastic stent group. Besides the primary outcome, particular complications were also tested to inform the reader.
The FCSEMS cohort was not part of the original RCT, newly included and the control group: patients receiving a plastic stent, is a historical control group. This for one seems to be reflected in the resection and bypass rates as more patients underwent resection in the FCSEMS cohort at which time a better selected surgical approach was used through the use of better imaging, multidisciplinary meetings and the availability of more defined criteria in pancreatic surgery. This might also explain the higher 120-day mortality rate in the plastic stent group, together with the recent centralisation of pancreatic surgery in the Netherlands, which is known to lead to lower mortality rates.26 Note that no adverse effects of the use of FCSEMS were seen on resection rates. Furthermore, inclusion varied between the participating hospitals possibly due to the heterogeneity of the patient population and hospital structure such as volume. In general, cohorts undergoing PBD first or early surgery are very heterogeneous; the indication for drainage or no drainage differs enormously, that is, jaundice yes or no, level of bilirubin, referral centre and type of diagnosis. Fifty per cent of patients seen in the hospital, which included most patients in the present study, had already received a stent at the referring hospital. Adjusting for confounding by indication is difficult, inclusion criteria were set and a logistic regression analysis was performed to adjust for known variables that could influence the outcome.27
Post-stent placement pancreatitis occurred more frequently in the FCSEMS group, although eight out of nine patients suffered from mild pancreatitis. This has been described before; expansion of covered and uncovered metal stents may cause post-ERCP pancreatitis due to compression of the pancreatic duct orifice.28 A (pre-cut) papillotomy relieves the initial compression of the duct orifice when performed during ERCP. No differences were observed between the FCSEMS group (53%) and the plastic stent group (58%). Despite a higher rate of post-ERCP pancreatitis, differences in time to surgery between patients with and without PBD-related complications were similar in the FCSEMS and plastic stent groups.
The superiority of biliary drainage with FCSEMS is evident in this study. This was already established for metal stents in patients with unresectable periampullary cancer. Two randomised trials comparing metal versus plastic stents for palliation in patients with malignant biliary obstructions showed a longer patency, lower number of reinterventions and decreased overall treatment costs when using a metal stent.29 ,30 In a systematic review by Moss et al11 on the use of metal versus plastic stents in the palliative setting, it was concluded that SEMS are the devices of preferred choice. Several studies are also available on PBD with SEMS in resectable patients and have reported good results.12–18 However, studies were often small and retrospective reporting on a non-consecutive cohort of patients without comparison with a plastic stent. Furthermore, the type of SEMS used can influence the interpretation of the available study results. A systematic review published in 2011 containing 11 studies comparing covered versus uncovered SEMS in patients suffering from jaundice with unresectable disease reported a longer duration of patency of covered stents, which was defined as time to stent occlusion, and similar stent dysfunction rates.24 Two other meta-analyses did not find a benefit of covered over uncovered SEMS, although analysing fewer studies compared with the abovementioned review, the same studies were included in both analyses.31 ,32 A clear preference cannot be given.
This study design was chosen given the high rate of PBD plastic stent-related complication compared with early surgery in our previous multicentre RCT and recently reported good outcomes with FCSEMS in a palliative setting. Performing a new RCT comparing FCSEMS followed by surgery with early surgery, with identical inclusion criteria as the previous trial, would withhold one group of selected patients from the current preferred treatment, that is, early surgery. The present study has established the applicability of SEMS in the preoperative setting. Potential benefits of PBD compared with early surgery in selected patients need to be determined with new RCTs, particularly using other inclusion criteria (bilirubin level). There is no evidence that resectability rates and survival of the stent group compared with the early surgery group are different according to the RCT follow-up study.33 Additional clinical trials are needed to determine whether a shorter period of drainage might result in similar success rates but lower complication rates and whether subgroups of patients can be identified who will benefit from the drainage-first approach, such as those with contraindications for early surgery, those who suffer from severe jaundice, cholangitis, and patients who need nutritious support. Furthermore, the percentage of patients that will undergo neoadjuvant treatment is rising worldwide. Lastly, there will be a group of patients who required PBD due to logistical reasons such as waiting lists for surgery.12 ,34–36
Other ongoing studies in Sweden (NCT00501176) and the USA (NCT01191814 and NCT01038713) are randomising between plastic and metal stents. Although the current treatment of choice for most patients suffering from jaundice with resectable pancreatic head cancer is early surgery without PBD, it is not likely that all centres will be able to fully implement this regimen.7 ,37Therefore, PBD is still performed in a selection of resectable patients.3 ,6 ,19
This study strongly supports the use of FCSEMS instead of plastic stents in patients in whom PBD is indicated. Early surgery is the treatment of choice in patients suffering from jaundice, but no definitive conclusions can be drawn on the results of PBD with FCSEMS compared with early surgery.
Acknowledgments
The authors would like to thank S. van Dieren for her assistance with the statistical analyses.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors JAMGT was responsible for the implementation of the study, analysis of data, drafting and revising the manuscript as first author. JEvH, PF, TMvG, EAJR, ORCB and DJG were responsible for the conception of the design, this design was then elaborated and approved after several meetings by all other authors; JAMGT, RT, FJGMK, EvdH, IHJTdH, FPV, IQM, YCAK, DB, MJB, EJS, NAvdG and MGHB. All authors were responsible for conducting the study, including patients and acquisition of data, and interpretation of this data after analysis. After the initial manuscript was drafted, all authors revised the manuscript critically and approved the final version. All authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Competing interests None declared.
Ethics approval The local medical ethics committees of all participating hospitals approved the study design. This study was conducted according to the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.