Article Text

Abstract
Ulcerative colitis and Crohn’s disease are the principal forms of inflammatory bowel disease. Both represent chronic inflammation of the gastrointestinal tract, which displays heterogeneity in inflammatory and symptomatic burden between patients and within individuals over time. Optimal management relies on understanding and tailoring evidence-based interventions by clinicians in partnership with patients. This guideline for management of inflammatory bowel disease in adults over 16 years of age was developed by Stakeholders representing UK physicians (British Society of Gastroenterology), surgeons (Association of Coloproctology of Great Britain and Ireland), specialist nurses (Royal College of Nursing), paediatricians (British Society of Paediatric Gastroenterology, Hepatology and Nutrition), dietitians (British Dietetic Association), radiologists (British Society of Gastrointestinal and Abdominal Radiology), general practitioners (Primary Care Society for Gastroenterology) and patients (Crohn’s and Colitis UK). A systematic review of 88 247 publications and a Delphi consensus process involving 81 multidisciplinary clinicians and patients was undertaken to develop 168 evidence- and expert opinion-based recommendations for pharmacological, non-pharmacological and surgical interventions, as well as optimal service delivery in the management of both ulcerative colitis and Crohn’s disease. Comprehensive up-to-date guidance is provided regarding indications for, initiation and monitoring of immunosuppressive therapies, nutrition interventions, pre-, peri- and postoperative management, as well as structure and function of the multidisciplinary team and integration between primary and secondary care. Twenty research priorities to inform future clinical management are presented, alongside objective measurement of priority importance, determined by 2379 electronic survey responses from individuals living with ulcerative colitis and Crohn’s disease, including patients, their families and friends.
- Ulcerative colitis, UC
- colitis
- Crohn’s disease, CD
- ileitis
- granuloma
- fistula
- stricture
- perianal
- inflammatory bowel disease, IBD
- pouch
- pouchitis
- guideline
- classification
- diagnosis
- monitoring
- endoscopy
- endoscopic
- colonoscopy
- sigmoidoscopy
- ultrasound
- magnetic resonance, MR
- computerised tomography, CT
- biomarker
- calprotectin
- management
- therapy
- surgery
- colectomy
- adult
- adolescent
- suppository
- enema
- 5-aminosalicylate
- 5-ASA
- mesalazine
- corticosteroid
- budesonide
- prednisolone
- hydrocortisone
- methylprednisolone
- thiopurine
- azathioprine
- mercaptopurine
- ciclosporin
- cyclosporine
- anti-TNF
- infliximab
- adalimumab
- integrin
- vedolizumab
- ustekinumab
- JAK
- janus kinase inhibator
- tofacitinib
- therapeutic drug monitoring
- anti-drug antibodies
- nutrition
- diet
- vitamin D
- anaemia
- antibiotics
- tuberculosis, TB
- cytomegalovirus
- CMV
- clostridium difficile
- cancer
- chemoprevention
- surveillance
- pregnancy
- fetus
- breastfeeding
- probiotic
- antibiotic
- faecal microbial transplant
- vaccine
- vaccination
- multidisciplinary team, MDT
- adherence
- self-management
- telephone clinic
- virtual clinic
- primary stress
- care
- shared care
- fatigue
- stress
- psychology
- psychotherapy
- cognitive behavioural therapy, CBT
- smoking
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Ulcerative colitis, UC
- colitis
- Crohn’s disease, CD
- ileitis
- granuloma
- fistula
- stricture
- perianal
- inflammatory bowel disease, IBD
- pouch
- pouchitis
- guideline
- classification
- diagnosis
- monitoring
- endoscopy
- endoscopic
- colonoscopy
- sigmoidoscopy
- ultrasound
- magnetic resonance, MR
- computerised tomography, CT
- biomarker
- calprotectin
- management
- therapy
- surgery
- colectomy
- adult
- adolescent
- suppository
- enema
- 5-aminosalicylate
- 5-ASA
- mesalazine
- corticosteroid
- budesonide
- prednisolone
- hydrocortisone
- methylprednisolone
- thiopurine
- azathioprine
- mercaptopurine
- ciclosporin
- cyclosporine
- anti-TNF
- infliximab
- adalimumab
- integrin
- vedolizumab
- ustekinumab
- JAK
- janus kinase inhibator
- tofacitinib
- therapeutic drug monitoring
- anti-drug antibodies
- nutrition
- diet
- vitamin D
- anaemia
- antibiotics
- tuberculosis, TB
- cytomegalovirus
- CMV
- clostridium difficile
- cancer
- chemoprevention
- surveillance
- pregnancy
- fetus
- breastfeeding
- probiotic
- antibiotic
- faecal microbial transplant
- vaccine
- vaccination
- multidisciplinary team, MDT
- adherence
- self-management
- telephone clinic
- virtual clinic
- primary stress
- care
- shared care
- fatigue
- stress
- psychology
- psychotherapy
- cognitive behavioural therapy, CBT
- smoking
1 Introduction
In the past decade there have been major advances in investigations, pharmacological, non-pharmacological and surgical interventions for both ulcerative colitis (UC) and Crohn’s disease. In light of this, the British Society of Gastroenterology (BSG) Clinical Services and Standards Committee (CSSC) commissioned a new guideline for the management of inflammatory bowel disease (IBD) in adults. This was to replace the 2011 iteration of IBD guidelines from the Society.1 The aim of this document is to provide high-quality disease management guidance for healthcare professionals managing IBD, to ensure that investigation, treatment and monitoring decisions are based on the best available evidence, and to promote and improve best accepted practice. Where appropriate the guidelines refer to relevant National Institute for Health and Care Excellence (NICE) documents, with attention drawn to how this guidance can be incorporated into the UK National Health Service (NHS) infrastructure and funding pathways.
2 Methodology
The guideline is of relevance to adults aged 16 years and over and was developed according to Grading of Recommendations Assessment, Development, and Evaluation (GRADE) methodology,2 in accordance with the principles of the AGREE II tool,3 and in compliance with the BSG Guidelines Advice Document.4 The completed document was formally peer reviewed by the BSG CSSC and BSG Council prior to submission for publication. The guideline writing process was supported by regular consultation from Professor Cathy Bennett (Systematic Research Ltd and Royal College of Surgeons in Ireland (RCSI)) and used a bespoke online platform developed by Dr Stuart Gittens (ECD Solutions: https://www.guideline.pub/bsg-ibd/) to develop clinical questions structured by Population, Intervention, Comparator and Outcome (PICO) or Population, Exposure, Outcome (PEO) development, to assimilate evidence and to facilitate voting of draft statements and recommendations using a modified eDelphi process.
After commissioning of the guideline by the BSG CSSC, a Guideline Development Group (GDG) was convened by the Chair of the IBD Section Committee of the BSG (ABH). A GDG Lead (CAL) and conflicts of interest Chair (TI) were appointed. Key Stakeholders from the following groups were represented: British Society of Gastroenterology (BSG), Association of Coloproctology of Great Britain and Ireland (ACPGBI), Royal College of Nursing (RCN), British Society of Paediatric Gastroenterology, Hepatology and Nutrition (BSPGHAN), British Dietetic Association (BDA), British Society of Gastrointestinal and Abdominal Radiology (BSGAR), and the Primary Care Society for Gastroenterology (PCSG). Patient representation was provided by Crohn’s and Colitis UK.
Members of the BSG IBD Section Committee were invited to take part in the GDG along with external clinicians with relevant experience. The GDG and all conflicts of interest for 12 months preceding GDG formation were vetted and approved by the BSG CSSC.
Clinical priorities to be covered by the guideline were set by the GDG including:
Definitions, clinical features and diagnosis
Investigations including imaging
Treatment of active UC including surgery and acute severe UC (ASUC)
Pouchitis management
Treatment of active Crohn’s disease (ileal, ileocolonic, colonic, jejunal, upper GI, perianal)
Maintenance treatment of Crohn’s disease
Surgery for Crohn’s disease (including non-perianal fistulising disease)
Common considerations for drug groups to include mesalazines, corticosteroids, thiopurines, methotrexate, ciclosporin, anti-TNF, vedolizumab, ustekinumab, tofacitinib and antibiotics
Therapeutic monitoring including drug levels and drug toxicity/immunogenicity, and pre-treatment infection screening and vaccination
Non-drug therapies including leucocyte apheresis and stem cell transplantation
Nutrition and dietary therapy
Lifestyle factors including smoking
Pain and fatigue
Psychological aspects
Service delivery
Primary care management of IBD
Where substantial up-to-date guidance existed on special circumstances—for example, pregnancy, osteoporosis, iron deficiency, immunosuppression in the context of prior malignancy or histology—extensive systematic review would not be performed but summary data would be presented to encourage best practice with referencing to signpost other guidance. Guidance for surgical technique in IBD would not be extensively covered due to a concurrent guideline development process in this area led by the ACPGBI.5 Health economics and costs of drugs would not be assessed as part of the guideline, although cost would be mentioned as an important consideration when there is a choice of treatments.
A clinical framework was then designed to visually map and group patient management decisions and influencing clinical factors, including disease location and severity. Sub-categorisations were made to identify aspects pertinent to pharmacological and non-pharmacological intervention, nutrition, imaging, surgery, primary care and service delivery. Four working groups were formed (led by NAK, TR, PH and PJS alongside CAL and ABH) to draft and develop a list of key thematic and sub-thematic clinical questions grouped into sections defined by the clinical framework that face IBD clinicians in everyday healthcare practice. These clinical questions were circulated to all stakeholder groups for review by members outside the GDG to ensure all relevant areas of clinical practice were covered. Following stakeholder review, the list was further developed producing 54 thematic questions with 360 associated clinical questions grouped around these themes (see online supplementary appendix 1).
Supplemental material
Next, the clinical questions were further revised, refined and combined with the thematic questions in order to design the systematic review. Keyword tables derived from these questions and formulated according to PICO or PEO structure were generated on the online platform, and structured searches of electronic literature databases were performed. The literature searches were designed, run in electronic databases and exported to Endnote reference managing software, supported by information specialists at York Health Economics Consortium. Searches of the Medline and EMBASE databases were performed in March 2017 and updated in March 2018. No date or study design limits were incorporated into searches in order to return all available evidence, including conference proceedings (although conference proceeding returns were limited to 5 years preceding the date of search). The search strategy used is presented in online supplementary appendix 2. In this way, systematic literature searches and reviews were undertaken to identify and synthesise evidence to support the creation of statements with supporting narrative syntheses of evidence. A total of 87 959 references were returned after deduplication from these searches. Focused top-up searches using keywords were performed until June 2019 to ensure evidence was up to date at the time of submission for publication. GDG members were able to also propose papers or electronic documents (eg, NICE guidance) for inclusion in the literature databases throughout the guideline development process. In this manner an additional 288 entries were added to the reference library to make a total of 88 247. References were cross-searched both manually using keywords and Boolean operators, and using a bespoke programmatic algorithm (the latter cross-referencing content of abstract, title and keywords with contents of PEO and PICO tables), both facilitated by the online platform. Literature was assessed according to the pre-designed PEO and PICOs, and abstracts±full text assessed for relevance and quality. Evidence-based evaluative text and associated reference lists were developed along with draft statements and grouped/archived in a customised electronic database. Statements considered potential health benefits, side effects and risks of recommendations to patients, as well as cost and service implications. Full economic analyses were not undertaken.
Following statement revision by the GDG according to Delphi methodology, an ‘IBD guidelines eDelphi consensus group’ of 81 clinicians and patients was formed consisting of representatives invited from all stakeholder groups listed above, and all members of the GDG except CB and SG who did not vote. A modified eDelphi mechanism process, employing the online platform, was then used to produce an evidence-based consensus, following a NICE accredited methodology. This consisted of three main rounds of anonymous web-based voting, using a custom-built online voting platform scoring each using a 5-point scale with updated iterations of the statements and evaluative text based on feedback after each round.
Following two rounds of anonymised voting, statements conforming to PICO/PEO which achieved consensus of 80% agreement or higher were categorised according to the GRADE system for grading quality of evidence and strength of recommendations. Assessments were made independently by two members of the GDG (blinded to one another’s assessment) using a custom-built electronic database by NAK in REDCap6 (at https://surveys.exeteribd.org.uk/). All assessments were reviewed and where necessary moderated by CAL and ABH to determine agreement. To assess the quality of evidence for each statement, each member considered study type, risk of bias, inconsistency, indirectness, imprecision, publication bias, effect size, plausible confounding variables and dose–response gradient if applicable. The quality of evidence ranged from ‘high’ (further research is very unlikely to change confidence in the estimate of effect), ‘moderate’ (further research is likely to have an important impact on confidence in the estimate of effect and may change the estimate), ‘low’ (further research is very likely to have important impact on confidence in the estimate of effect and is likely to change the estimate), and ‘very low’ (any estimate of effect is very uncertain). The strength of recommendation was assessed based on considerations of desirable and undesirable anticipated effects, the certainty of the evidence of effects, any important uncertainty about or variability in how much people value the outcome, whether the balance of these effects favours the intervention or comparison, the acceptability of intervention to key stakeholders and feasibility of intervention implementation. The strength of each recommendation was then recorded as ‘strong’ (meaning that benefits clearly outweigh risks and burdens or vice versa) and conditional recommendations as ‘weak’ (where benefits, risks and burdens are conditional, closely balanced or uncertain).
Where statements did not conform to PICO/PEO (such as subjective interventions or where outcomes were multiple) and evidence was indirect or of low quality, recommendations to inform clinical practice were presented as Good Practice Recommendations and listed separately to GRADE recommendations, but still underwent consensus voting.
The GDG voted on all statements and Good Practice Recommendations, and other eDelphi participants voted on one of three subsets of statements and Good Practice Recommendations in order to ensure adequate numbers of responses were obtained for each, that expertise was equally distributed across subject areas and that surgeon members of the group voted on all surgical-related topics. The total number of respondents per statement and recommendation are presented in online supplementary table 3. Statements and recommendations not reaching 80% consensus agreement following three rounds of voting were removed and are presented in online supplementary appendix 3.
Conflict of interest
To ensure transparency and declaration of any potential bias, all the GDG members were asked to declare a minimum of 12 months competing financial and non-financial interests when they joined the group and during initial statement drafting. All members of the GDG and IBD guidelines eDelphi consensus group also declared conflicts of interest before each of the three rounds of Delphi consensus voting. This is in keeping with the NICE approved processes. The final submitted conflicts of interest for each member is shown in online supplementary table 2. eDelphi participants were asked to abstain from voting where they either did not have sufficient knowledge to vote on a particular statement or where they identified themselves as having a conflict which precluded voting. The number of abstentions in the final round of voting is presented in online supplementary table 3.
Areas of unmet research priority identified by systematic review
Following systematic review, the original 414 clinical questions defined by the group, evaluative descriptions for each statement and the results of consensus voting were reviewed to determine where evidence was insufficient to provide recommendations for practice, or where further research was desirable to define and support best clinical practice. From this, 20 areas of research priority with associated questions were determined and described for a healthcare professional readership. General audience versions of these questions were then written and readability assessed by the Flesch Reading Ease and Flesch-Kincaid Grade Level (see online supplementary table 4). The importance to patients, their relatives, partners, parents, friends and carers of these 20 research priority themes was determined by two electronic surveys conducted by the UK patient charity Crohn’s and Colitis UK during December 2018 and January 2019 using the general audience versions and asking survey respondents to score each priority on a Likert scale of 1–9 (1=not important and 9=very important). Survey 1 was promoted by social media and Survey 2 through a combination of social media and direct email to respondents to Survey 1 who agreed to be contacted for future survey.
Revisions of the guideline
We suggest that every 2 years a formal assessment of the following should take place:
Research objectives identified by the guidelines should be reviewed for evidence of additional studies, contributing to resolving the objective
Review of new evidence that may change former recommendations
Identification of any error in the guidelines after publication
Exploration of any evidence of inequality in access to services between different social groups that can be addressed through guideline recommendations
Review of any new technology or drugs or legislation, that will change former recommendations
We suggest the guidelines should be fully updated after 5 years. All materials are archived using the online system at https://www.guideline.pub/bsg-ibd/.
Note on drug nomenclature
In this document we have adopted the following descriptors: ‘Immunosuppressive drugs’: corticosteroids, thiopurines, methotrexate, calcineurin inhibitors, janus kinase inhibitors and all biologic drugs where the mode of action is immunosuppressive; ‘Immunomodulators’: thiopurines and methotrexate; ‘biologics’: monoclonal antibody drugs.
3 Ulcerative colitis
3.1 Diagnosis
Ulcerative colitis (UC) is a chronic inflammatory disease characterised by mucosal inflammation starting distally in the rectum, with continuous extension proximally for a variable distance, often with an abrupt demarcation between inflamed and non-inflamed mucosa. Typically, patients with UC experience periods of relapse and remission. Up to 90% will have one or more relapses after the first attack, and early relapse or active disease in the first 2 years is associated with a worse disease course subsequently.7 8
Statement 1. Where ulcerative colitis is diagnosed by sigmoidoscopy, we recommend a full ileocolonoscopy to delineate disease extent, severity of inflammation and to exclude Crohn’s disease (GRADE: strong recommendation, very low-quality evidence. Agreement: 100%).
In patients presenting with suspected UC, stool cultures and Clostridium difficile toxin assay should always be performed to rule out infective causes. While UC is often initially diagnosed at flexible (or rigid) sigmoidoscopy, it is important to confirm the diagnosis, extent and severity of disease by means of full ileocolonoscopy, usually within the first year, as this can more definitively confirm the diagnosis of UC versus Crohn’s disease and give information that may help to predict future disease course, including potential and risk stratification for dysplasia,9 and thus will influence treatment choices. For histological assessment at least two biopsy specimens should be taken from five sites throughout the examined bowel, including the ileum and rectum, during the initial endoscopic evaluation.1
Rectal sparing in UC has been described in up to >3% of patients,10 but more frequently patchy inflammation of the rectum may be seen in those who have been given empirical topical therapy.11 12 The presence of a ‘caecal patch’, isolated peri-appendiceal inflammation and backwash ileitis can occur in UC, but if the histology and clinical pattern are not otherwise typical of UC, then small bowel evaluation is required to exclude Crohn’s disease (see Section 4.1.3.1: Crohn’s disease, Cross-sectional imaging: CT, MR and small bowel ultrasound). Backwash ileitis has been reported in up to 20% of patients with extensive colitis.13
3.1.1 Histology
No histological feature is diagnostic of UC, but the combination of basal plasmacytosis, diffuse crypt atrophy and distortion, villous surface irregularity and mucus depletion are suggestive of a diagnosis of UC in the correct clinical context.14 Uneven distribution of inflammation within the colon or within biopsies can occur in patients with long-standing disease, or after treatment.
3.1.2 UC versus Crohn’s disease
In 5–15% of IBD patients, endoscopic and histological assessments cannot distinguish between Crohn’s colitis and UC, and these patients are labelled as IBD-unclassified (IBD-U), or if features are still indeterminate after colectomy histology is assessed, described as indeterminate colitis.15–17 IBD-U is more common in children than adults.18 In a small proportion of UC patients their diagnosis is later changed to IBD-U or Crohn’s disease.19–21
3.2 Phenotypic classification
The Montreal classification22 in adults and Paris classification23 in children (table 1) are useful in ascribing phenotypes to patients both for treatment and to assist with service delivery and research.24 Children developing IBD generally have more extensive disease than adults.25 Establishing the extent of the inflammation in a patient with UC is important for prognosis as the likelihood of colectomy is dependent on disease extent. A systematic review showed that the 10 year colectomy rate is 19% for those with extensive colitis, 8% with left-sided colitis and 5% with proctitis; and male gender, young age and elevated inflammatory markers at diagnosis also increase the likelihood of colectomy.26 Backwash ileitis is also associated with more aggressive disease, and with primary sclerosing cholangitis.13 Those with extensive colitis also have the highest risk of developing colorectal cancer.27 28
Montreal and Paris classification in UC
Disease extent can change after diagnosis.29 Up to half with proctitis or proctosigmoiditis will develop more extensive disease.8 26 30 Of patients with proctitis initially, 10% will ultimately have extensive colitis.31 However, over time the extent of inflammation can also regress, and classification should always remain as the maximal extent.29 Endoscopic appearance may significantly underestimate the true extent (particularly in quiescent UC), and this should be confirmed by mapping biopsies.
3.3 Clinical and endoscopic disease activity
Definitions in relation to disease activity are shown in box 1. The Mayo Score for UC is widely used in clinical trials and may be applied to clinical practice as a composite clinical and endoscopic tool (table 2).32 The score of 0–12 includes a measure of stool frequency, rectal bleeding, a physician’s global assessment and a measure of mucosal inflammation at endoscopy. The partial Mayo score uses the non-invasive components of the full score and correlates well to patient perceptions of response to therapy.33
Mayo score for ulcerative colitis32
Definitions in IBD management
Steroid dependency: inability to wean systemic steroids below 10 mg prednisolone within 3 months without recurrent active disease, or symptomatic relapse of IBD within 3 months of stopping steroids.1279
Steroid refractory: inability to induce symptomatic remission with systemic steroids.1279
Mucosal healing: typically, this refers to absence of macroscopic mucosal inflammation or ulceration, although precise definitions between studies vary. While usually defined endoscopically, more recently there has also been interest in ‘histological healing’.56
Treat to target: the goal being more than symptomatic remission with the intention of reducing risk of future relapse or complications (eg, ileal strictures or colon cancer) resulting from uncontrolled but asymptomatic inflammation.56 360 Future studies are required to define targets, the practicality of achieving targets and to examine the balance of benefit versus risk and cost.
Therapeutic drug monitoring (TDM): measurement of drug (±anti-drug antibody) levels to assess compliance, drug metabolism and immunogenicity with a view to guide dose adjustments or switch off therapy (eg, where patients are relapsing despite therapeutic levels, or have developed high titre anti-drug antibodies with low levels).
Patient related outcome (PRO): a report directly from patients about how they feel or function in relation to their IBD and its therapy without interpretation by healthcare professionals. Provides an indication of the outcome of an intervention, or quality of care.1280
Patient reported outcome measure (PROM): a tool or instrument used to measure PROs.1280
There is wide variation in interpretation of disease activity endoscopically.34 The Ulcerative Colitis Endoscopic Index of Severity (UCEIS) has been developed to improve reliability (table 3).35 36 The Modified Mayo Endoscopic Score is another simple measure of endoscopic activity that correlates well with clinical and biological activity (table 4).37 Although both have been extensively validated, inter-observer variation remains a significant limitation for these visual scores.38 39
Ulcerative Colitis Endoscopic Index of Severity (UCEIS)35
Modified Mayo Endoscopic Score37
Symptomatic and endoscopic scores may be limited by their ability to quantify accurately the impact of disease on quality of life, including fatigue and psychosocial function, or if complex the indices may be difficult to apply to clinical practice.40 41 An increasing emphasis on patient reported outcomes measures (PROMs: standardised questionnaires filled out by patients without clinician involvement) in clinical trials may translate to routine clinical practice (box 1).42
3.4 Treatment targets
Statement 2. We suggest that symptomatic remission combined with mucosal healing should be the target of medical therapy in ulcerative colitis (GRADE: weak recommendation, very low-quality evidence. Agreement: 95.7%).
The ultimate target of medical therapy is a contentious issue as there is no fully agreed or validated definition of remission, although many parameters have been suggested both clinically and endoscopically.43–45 Using mucosal healing as a treatment target is contentious because of the implications for clinical practice, with the need for more endoscopic assessment and likely escalation of therapy in asymptomatic patients.46 In an Australian retrospective study, 61% of 246 patients were in clinical remission, but only 35% were in both clinical and endoscopic remission (Mayo endoscopic subscore ≤1), and only 16% of the 246 patients were also in histological remission.47 Using the Mayo endoscopic subscore, there is no consensus on the value of achieving a score of 0 rather than 1, with documented differences in future disease course between the two.46 There is lack of clear evidence about the importance of histological remission as well as endoscopic remission.48 49 Histological remission has now become an end-point for some new drug trials in UC, but there remains lack of agreement about the definition, and the evidence of long-term benefit is only from observational studies.44 48 50–54 There is, however, growing evidence that the presence of endoscopic and histological inflammation is predictive of future flares, lack of sustained remission, need for corticosteroids and colectomy.44 48 50–54 There is likewise evidence of the benefits of mucosal healing in reducing future risk of colorectal carcinoma55 (see Section 5.13: Chemoprevention and colorectal cancer surveillance). There is a growing consensus therefore that the target for UC should be clinical and/or patient-reported remission (defined as absence of rectal bleeding and return to normal bowel habit) combined with endoscopic remission (Mayo endoscopic subscore of ≤1).56 More evidence is needed of the implications for a more aggressive approach to achieving mucosal healing, including the acceptability to patients of increased medication with potential toxicity (often despite lack of clinical symptoms). A widely agreed definition is needed for both endoscopic healing and histological healing that can be used in clinical practice, and more evidence is also needed of the role of faecal calprotectin or other biomarkers as non-invasive surrogates for mucosal healing. Longer-term prospective studies of mucosal healing will be needed to provide evidence of the risks and benefits of this approach.
3.5 Initial treatment of active UC with 5-ASA
Statement 3. We recommend that mild to moderate ulcerative colitis should be managed with oral 5-ASA 2–3 g/day (GRADE: strong recommendation, high-quality evidence). We recommend the addition of 5-ASA enemas, rather than oral treatment alone (GRADE: strong recommendation, high-quality evidence. Agreement: 95.6%).
Statement 4. We suggest that ulcerative colitis patients flaring on 5-ASA therapy should receive dose escalation to 4–4.8 g/day orally alongside 5-ASA enemas (GRADE: weak recommendation, low-quality evidence. Agreement: 82.2%).
Oral 5-ASA (5-aminosalicylic acid) is the standard therapy for mild to moderately active UC. Meta-analyses support the efficacy of oral 5-ASA for induction therapy for mild to moderately active UC.57 58 Once daily dosing is as effective as divided doses.59 Doses ≥2 g/day are more effective than dosages <2 g/day for remission (RR 0.91; 95% CI 0.85 to 0.98).60 The majority of patients with mild to moderate UC will respond to 2–3 g 5-ASA (depending on formulation used) and higher doses can be used in those with more severe symptoms or those not responding initially.
3.5.1 5-ASA dose
The ASCEND trials investigated the dose–response effect of 5-ASA (Asacol) for the induction of response in UC. ASCEND I randomised 301 patients with mild-moderately active UC to 2.4 g or 4.8 g of mesalazine.61 At week 6, a similar proportion of patients experienced improvement in either group (51% vs 56%, p=NS). When results were stratified according to disease severity, patients with moderate disease had better response to 4.8 g/day, but there was no significant difference in dose–response in those with mildly active disease. ASCEND II confirmed that patients with moderately active UC had a better response to 4.8 g/day than 2.4 g/day (72% vs 59%, p=0.036).62 In the ASCEND III trial, 772 patients with moderately active UC were randomised to receive 2.4 g/day or 4.8 g/day mesalazine.63 Despite the large numbers in the study, there was no difference in the primary end-point of treatment success (complete clinical remission or partial response). There was a small but significant difference in remission, with 43% of patients on 4.8 g/day versus 35% of those on 2.4 g/day achieving remission at 6 weeks. Subgroup analysis showed that patients who had received steroid, oral 5-ASA and rectal therapies were more likely to respond to the higher dose.63 4.8 g/day 5-ASA is associated with more rapid symptom resolution than 2.4 g/day,64 and higher rates of mucosal healing at 3 and 6 weeks.65 Similarly, the 5-ASA MMX trials also showed that 4.8 g/day was more effective than 2.4 g/day in the subpopulation with prior exposure to 5-ASA, and in those who had an incomplete response to 8 weeks of 5-ASA MMX at 2.4 g/day.66
A post-hoc analysis of the ASCEND I and II data also showed that there was greater mucosal healing in the 4.8 g/day group compared with 2.4 g/day.65 There is also evidence of the effect of escalating doses of 5-ASA from the DEAR trial.67 In this study patients with quiescent UC but with a raised faecal calprotectin >50 µg/g had their current 5-ASA dose increased (from 1.2 g (or nil) to 2.4 g, or from 2.4 g to 4.8 g/day). Compared with a control group there was a significant increase in patients remaining in clinical remission, and with a faecal calprotectin <50 µg/g at 6 weeks. Oral 5-ASA is no more effective than oral sulphasalazine,59 but may be better tolerated (RR for an adverse event 0.48, 95% CI 0.36 to 0.63).57
Following commencement of 5-ASA, 10–30% of patients are in symptomatic remission at week 2, 30–45% by week 4 and 35–50% by week 8.68–71 High-dose 5-ASA should not be used routinely, but patients with symptoms that are failing to settle should have their dose increased.
3.5.2 Oral and enema 5-ASA
All UC patients (including those with extensive disease) should be offered a combination of oral and enema 5-ASA, and those with incomplete response to oral 5-ASA should have topical therapy added. The combination of oral and topical 5-ASA therapy is superior to monotherapy even in patients with pancolitis.72 73 A meta-analysis of four studies in active UC confirmed a relative risk of no remission of 0.65 (95% CI 0.47 to 0.91) for combined oral and topical therapy over oral 5-ASA alone for induction of remission.74 A small study in 18 UC patients with frequent relapses on standard dose oral 5-ASA showed the benefits of high-dose 5-ASA combined with 5-ASA enemas.75 Despite the evident benefits of enema therapy, the practical difficulty patients have in administering and retaining enemas remains a major obstacle, and support and education in this area is much needed.
3.5.3 Nephrotoxicity
Statement 5. We recommend that ulcerative colitis patients treated with 5-ASA should be monitored for the development of nephrotoxicity, with baseline renal function, repeated after 2–3 months, and then annually (GRADE: strong recommendation, very low-quality evidence. Agreement: 90.9%).
5-ASA therapy may be associated with renal complications.76 77 It is important to obtain baseline renal function, as renal disease may also be a primary complication of IBD itself. Renal manifestations of IBD include nephrolithiasis, urinary obstruction, fistulisation, glomerular disease, protein-losing nephropathy, secondary amyloidosis and renal failure.76 78 Nephrotic syndrome due to minimal-change nephropathy has been reported in a patient taking sulfasalazine, resolving with drug withdrawal and high-dose oral corticosteroids.79 Allergic reactions to sulfasalazine have recurred on challenge 5-ASA.80 Tubulointerstitial nephritis is a rare idiosyncratic reaction to 5-ASA therapy.
A UK study evaluated 151 patients with renal impairment associated with 5-ASA use.81 The temporal association with the drug, improvement on 5-ASA withdrawal (in 30% of the cases) and the recurrent renal damage on re-challenge in five patients was consistent with a true relationship, and a suggestive genetic association in the HLA region (p=1×10–7) was identified. Permanent renal replacement therapy was required in 15 patients. The median time on 5-ASA before renal impairment was 3 years (95% CI 2.3 to 3.7), and regular monitoring of renal function was uncommon. The frequency of 5-ASA nephrotoxicity has been estimated at 1 in 4000 patient years.82 83 Given the unpredictable nature of this occurrence, it is suggested that patients on long-term 5-ASA therapy should have renal function checked, including eGFR before starting, after 2–3 months, and then annually long-term, although there are no data to support a particular surveillance interval. Those with impaired renal function should be monitored more closely.
3.6 Corticosteroids in mild to moderate UC
Statement 6. We recommend that patients with mild to moderate ulcerative colitis in whom 5-ASA induction therapy fails or is not tolerated should be treated with oral prednisolone (GRADE: strong recommendation, high-quality evidence). We recommend that topically-acting oral corticosteroids such as budesonide MMX (GRADE: strong recommendation, moderate-quality evidence) and we suggest that beclomethasone dipropionate (GRADE: weak recommendation, moderate-quality evidence) can be used as alternative treatments for those wishing to avoid systemic corticosteroids (Agreement: 93.2%).
Prednisolone is superior to 5-ASA for induction of remission in UC,84 85 but has significant side effects and should be reserved for patients with failure of response or who are intolerant to oral and/or rectal 5-ASA (see Section 3.7:on Corticosteroids in moderate to severe UC).
3.6.1 Budesonide MMX
Randomised controlled trials have shown that oral budesonide MMX 9 mg daily is significantly more effective than placebo and can induce remission in mild to moderate UC, being as effective as 5-ASA.86–88 The CORE I and CORE II studies compared oral budesonide MMX 9 mg/day and 6 mg/day with placebo in patients with mild to moderate left-sided and extensive UC.87 Additional control groups were included (Asacol 2.4 g/day (CORE I) and Entocort EC 9 mg (CORE II)), but the studies were not powered to demonstrate differences between budesonide MMX and these controls. In a pooled analysis of both trials, the week 8 combined clinical and endoscopic remission rates were 17.7% for budesonide MMX 9 mg versus 6.2% for placebo (p=0.0002). A Cochrane systematic review concluded that the quality of evidence was moderate, and benefit was not demonstrated clearly for extensive UC but was significant for those with left-sided disease.89 Endoscopic healing rates were 27.6% versus 17.1% (p=0.009) for budesonide MMX and placebo, respectively.90 The 6 mg dose was not significantly better than placebo. Another placebo-controlled trial of budesonide MMX in mild to moderately active UC showed significant benefit in clinical, endoscopic and histological remission.91 Although no adequately powered comparative trials between budesonide MMX and conventional corticosteroids have been conducted to date, budesonide MMX may be considered as an alternative to conventional corticosteroids in patients with mild-moderate UC and failure of response to 5-ASA therapy.92
Budesonide has a lower rate of systemic adverse effects than conventional corticosteroids (33% vs 55%), and is not associated with adrenal suppression or a significant reduction in bone mineral density.93 94 Ileal-release budesonide does not induce remission in mild-moderately active UC and was in fact inferior to placebo and 5-ASA in two studies and a systematic review.89 93 95
3.6.2 Beclomethasone dipropionate
Oral beclomethasone dipropionate is a second-generation corticosteroid and may also be an alternative to conventional corticosteroids. In a randomised controlled trial in 282 patients, oral beclomethasone dipropionate 5 mg daily for 4 weeks, then alternate weekly for a further 4 weeks was shown to be non-inferior to prednisolone in efficacy, but there was also no difference in the co-primary end-point of steroid-related adverse events and reduction in morning cortisol below 150 nmol/L.96 In patients with active left-sided or extensive UC, oral beclomethasone dipropionate 5 mg/day has been demonstrated as equivalent to 2.4 g 5-ASA,97 and has been shown as more effective when added to 5-ASA compared with 5-ASA alone.98
Although more expensive, topically-acting oral corticosteroids are an alternative to prednisolone in UC patients with mild to moderate disease and 5-ASA failure.
3.7 Corticosteroids in moderate to severe UC
Statement 7. We recommend that moderate to severe ulcerative colitis should be treated with oral corticosteroids such as prednisolone 40 mg daily weaning over 6–8 weeks (GRADE: strong recommendation, high-quality evidence. Agreement: 100%).
Oral corticosteroids are effective for the induction of remission in patients with moderate to severe ulcerative colitis refractory to sulfasalazine or 5-ASA, and in patients who have responded to initial treatment with intravenous corticosteroids following hospitalisation for acute severe disease.84 85
In a meta-analysis of five randomised controlled trials, corticosteroids were superior to placebo for induction of remission in UC (RR of no remission, 0.65; 95% CI 0.45 to 0.93).99 Although the optimal dose and regimen for systemic corticosteroids in UC is uncertain, the current 40 mg dose recommendation is based on Baron’s studies where 40 mg was more effective than 20 mg/day.100 There is no evidence of benefit with doses higher than 40–60 mg/day,99 and doses above 40 mg may be associated with increased adverse effects.100 Approximately 50% of patients experience short-term corticosteroid-related adverse events such as acne, oedema, sleep and mood disturbance, glucose intolerance and dyspepsia.99 100 Single daily dosing is as effective as split-dosing and causes less adrenal suppression.101 The dose should be tapered over 6–8 weeks.
3.7.1 Failure of oral corticosteroids
There is variation in the definition of severe ulcerative colitis. The Mayo score or Disease Activity Index32 does not include systemic symptoms (fever, anaemia or abnormal inflammatory markers), whereas the Truelove and Witts criteria for severe disease102 specify one or more of these. Patients with systemic symptoms of fever, severe pain, significant anaemia, or those who are generally unwell and not tolerating their symptoms should be admitted for inpatient management (see Section 3.12:on Acute severe ulcerative colitis). Prolonging treatment with high-dose oral corticosteroids has a diminishing chance of achieving remission, and of those who do respond, there will be many who become corticosteroid-dependent (22% at 1 year in a study from the pre-biologic era103). There is however increasing risk of infective, metabolic and surgical complications for deteriorating patients who may require emergency admission and colectomy.104 105 There is no evidence from a meta-regression analysis that doses above 60 mg of methylprednisolone reduce colectomy rates in severe UC.106 Although there are few data on the time-course of response to oral corticosteroids, a study comparing oral prednisolone with prednisolone metasulphobenzoate showed that improvements in clinical and endoscopic disease activity may be seen within 2 weeks of treatment with oral prednisolone 40 mg/day,107 so patients not responding after 2 weeks should be considered for treatment escalation to biologics or admission to hospital, depending on how systemically unwell they are.
3.8 5-ASA maintenance therapy for UC
Statement 8. We recommend that oral 5-ASA should be the standard maintenance medical therapy in ulcerative colitis (GRADE: strong recommendation, high-quality evidence). We recommend that the choice of formulation should consider patient preference, likely adherence and cost. Once daily dosing is effective (GRADE: strong recommendation, high-quality evidence) and may improve adherence (Agreement: 100%).
Maintenance 5-ASA therapy is advocated to decrease the risk and frequency of flares. The most recent Cochrane analysis showed a trend towards greater efficacy with higher doses (2 g or more).108 Rectal 5-ASA is also an effective maintenance therapy for distal ulcerative colitis.109 110 There are randomised controlled trials evaluating once daily dosing with all the major 5-ASA formulations, and systematic reviews confirm that once daily dosing is as effective as divided dosing regimens.111–114 In community surveys, 5-ASA adherence is a major problem and some studies suggest that simplified dosing regimens are associated with better adherence.115 Therefore, once daily dosing should be considered as a standard dosing regimen for all 5-ASA use.
In an evaluation of data from Cochrane analyses there were no differences between the various 5-ASA formulations in terms of efficacy,116 confirmed in the most recent Cochrane analysis.108 There is little to choose between the different formulations of 5-ASA in terms of efficacy, and the best drug should be selected taking into account patient preference for formulation (for instance granules or tablets, tablet size and number required daily), in order to maximise treatment adherence117 and considering cost.
3.9 Treatment options for UC patients after 5-ASA failure
Statement 9. We recommend that ulcerative colitis patients on maintenance therapy with high-dose mesalazine, who required two or more courses of corticosteroids in the past year, or who become corticosteroid-dependent or refractory, require treatment escalation with thiopurine (GRADE: strong recommendation, moderate-quality evidence), anti-TNF therapy (GRADE: strong recommendation, high-quality evidence), vedolizumab (GRADE: strong recommendation, high-quality evidence) or tofacitinib (GRADE: strong recommendation, high-quality evidence). The choice of drug should be determined by clinical factors, patient choice, cost, likely adherence and local infusion capacity (Agreement: 96.6%).
3.9.1 Thiopurines
While studies vary in quality, meta-analyses consistently report a benefit of thiopurines over placebo for the maintenance of steroid-induced remission in UC but not for induction of remission. Meta-analysis of three randomised controlled thiopurine maintenance studies favours thiopurines over placebo (RR 0.6, 95% CI 0.37 to 0.95).118 In a further meta-analysis, OR was 2.59 (95% CI 1.26 to 5.3), absolute risk reduction was 23% and the number-needed-to-treat (NNT) to prevent one recurrence was five.119 A recent Cochrane review included 232 patients from four maintenance studies of azathioprine versus placebo and showed a benefit of azathioprine over placebo (44% vs 65% failure, respectively, RR 0.68, 95% CI 0.54 to 0.86).120 The side effects of thiopurines, both short- and long-term, should be considered (see Section 5.2.2on Drug management: thiopurines) in choice of therapy, and also in decisions about duration of therapy, particularly in older patients (see Section 5.2.7.1 Stopping thiopurines).
3.9.2 Infliximab
In the ACT1 and ACT2 clinical trials, UC patients with active disease despite corticosteroids and/or thiopurines (and/or 5-ASA for ACT2 only) were treated with 5 or 10 mg/kg infliximab or placebo at weeks 0, 2 and 6, and followed to week 54 (ACT1) or week 30 (ACT2). Clinical response at week 8 was similar in both active doses, and pooled data from both trials were 67% for 5 mg/kg versus 33% for placebo.121 At week 30 combined clinical remission rates were 30% for 5 mg/kg (13% for placebo), with very similar remission rates sustained to week 54 in ACT1. Corticosteroid-free remission rates were 22% for 5 mg/kg at week 30, sustained to week 54 in ACT1. In the UC SUCCESS study, patients in whom corticosteroid therapy had failed and who were receiving infliximab and azathioprine combination therapy (40%) had significantly higher remission rates at week 16, compared with infliximab alone (22%).122 10% of these patients had previously received immunomodulators, but not anti-TNF therapy. Cohort studies also show benefit of using infliximab for patients with corticosteroid-dependent UC, with steroid-free remission rates of 47% at 1 year, 77% colectomy-free at median 41.5 months, and better outcomes for those on combination therapy with thiopurines, and also in those who were thiopurine-naïve initially.123 124 Real-life experience of infliximab treatment in UC patients where conventional therapy had failed showed primary response rates vary from 67% (in a study from Leuven, starting infliximab prior to 2006 and including patients recruited to the ACT1 study),125 to 78% in a French multicentre study of patients treated from 2000 to 2009.126
3.9.3 Adalimumab
The ULTRA1 and ULTRA2 clinical trials127 128 showed that adalimumab 160 mg at week 0, 80 mg at week 2, followed by 40 mg fortnightly achieved remission at week 8 in 19% (placebo 9%) in ULTRA1 and 21% (placebo 11%) in the ULTRA2 study in patients naïve to anti-TNF therapy. The ULTRA2 maintenance study showed clinical remission rates at week 52 of 22% (12% placebo) in the anti-TNF naïve subgroup. Corticosteroid-free remission at week 52 in the same subgroup was 14% (placebo 6%). In the open-label extension study (ULTRA3), 25% remained in clinical remission on fortnightly or weekly adalimumab at 4 years after initial enrolment.129 Real-world data from the USA on the use of infliximab and adalimumab in UC patients naïve to anti-TNF therapy suggests comparable efficacy in the treatment of moderate to severe disease.130 131
3.9.4 Golimumab
The PURSUIT SC trial was an induction trial of golimumab, which included a dose-finding phase.132 1064 patients with UC that had failed to respond to either 5-ASA, oral corticosteroids, azathioprine or mercaptopurine, or who were steroid-dependent, were enrolled. All patients were anti-TNF naïve. 42.8% were receiving steroids at baseline, and a third were on thiopurines. Clinical response was achieved at week 6 in 51.0% on 200 mg/100 mg, 54.9% at 400 mg/200 mg, both significantly better (p<0.0001) versus placebo response rate of 30.3%. Clinical remission at week 6 was 17.8% (200 mg/100 mg), 17.9% 400 mg/200 mg, p<0.0001 versus placebo (6.4%). Both clinical response and remission at week 6, correlated with drug levels. Real-world observational studies corroborate with PURSUIT study observations.133
Network meta-analyses comparing the different anti-TNF agents in UC present conflicting data on the relative efficacy of infliximab, adalimumab and golimumab.134–137
3.9.5 Vedolizumab
In the GEMINI I clinical trial of vedolizumab in active UC, patients were enrolled to a randomised cohort. 225 patients received intravenous vedolizumab 300 mg at day 1 and 15, 149 patients received placebo and 521 patients were randomised to open-label vedolizumab in order to fulfil sample size requirements for the continuation maintenance study.138 139 Of the anti-TNF naïve patients in the randomised induction phase, clinical response at 6 weeks was seen in 26.3% of 76 patients on placebo versus 53.1% of 130 patients on vedolizumab, an estimated 26.4% difference (95% CI 12.4% to 40.4%). Clinical remission at 6 weeks was seen in 6.6% on placebo and 23.1% on vedolizumab, an estimated difference of 15.5% (95% CI 5.1% to 25.9%). Of the randomised responders who entered the maintenance phase (including those from the open-label induction cohort) and who had been anti-TNF naïve at entry, the durable clinical response rate (response at both weeks 6 and 52) was 26.6% for the 79 patients on placebo compared with 60.7% for the 145 patients given vedolizumab (either 4-weekly or 8-weekly). The estimated difference from placebo was 34.3% (95% CI 20.7% to 47.8%). The clinical remission rate at week 52 for the placebo group was 19.0%, and 46.9% for the combined vedolizumab group, an estimated difference from placebo of 28.0% (95% CI 14.9% to 41.1%). There were no clinically important differences in safety between the vedolizumab and placebo groups during the maintenance study.139
A recently published retrospective study from the VICTORY consortium analysed safety and efficacy data from 321 UC patients receiving vedolizumab therapy (71% of whom had previously been treated with anti-TNF therapy).140 Primary effectiveness outcomes were cumulative rates of clinical remission (defined as resolution of all UC-related symptoms on physician’s global assessment), endoscopic remission (defined as a Mayo endoscopic subscore of 0), corticosteroid-free remission and deep remission (clinical remission and endoscopic remission). In recognition of potential attrition bias, variability in follow-up and impact of right censoring, imputation analyses calculated 12 month rates as 20%, 17%, 15% and 14% respectively. On multivariable analyses, prior exposure to anti-TNF therapy was associated with a reduced probability of achieving clinical remission (HR 0.53, 95% CI 0.38 to 0.75) and endoscopic remission (HR 0.51, 95% CI 0.29 to 0.88).
Until recently there has been limited reporting of vedolizumab therapy outcomes for anti-TNF naïve patients with UC. However, a multicentre European retrospective study of 184 patients (50 Crohn’s disease and 134 UC patients) showed a greater efficacy than that reported in anti-TNF experienced patients with response, clinical remission and steroid-free remission rates at week 14 of 79.1%, 39.5% and 36.6%, respectively, in UC.141 The VARSITY trial has now been reported in abstract form and is the first head-to-head comparison of two biologic agents in IBD.142 Seven hundred and sixty-nine patients with moderately to severely active UC who had failed conventional therapies were randomised to intravenous vedolizumab 300 mg at weeks 0, 2 and 6 and then every 8 weeks, versus adalimumab subcutaneously 160 mg at week 0, 80 mg at week 2, and then 40 mg fortnightly, in a double-blind, double-dummy trial. Dose escalation was not permitted for either group. Recruitment of patients with previous anti-TNF therapy use was capped at 25% of the trial population. At 52 weeks, the primary end-point of clinical remission (a complete Mayo score ≤2 with no subscore >1) was achieved in 31.3% on vedolizumab versus 22.5% on adalimumab (p=0.006). Mucosal healing (Mayo endoscopic subscore ≤1) was 39.7% and 27.7%, respectively (p=0.0005). Corticosteroid-free remission rates (in those on steroids at baseline) at week 52 were not significantly different between the vedolizumab and adalimumab groups. Although no similar data are available for comparison with infliximab, these data provide support for vedolizumab as a first-line biologic option for UC failing conventional therapy.
3.9.6 Tofacitinib
A phase 2 dose-ranging induction study of the Janus kinase (JAK) inhibitor tofacitinib in patients with endoscopically confirmed active UC showed increased rates of clinical and endoscopic response and remission after 8 weeks of treatment that reached statistical significance for patients in the higher dosing arms of 10 mg and 15 mg oral twice daily.143 The OCTAVE-1 and OCTAVE-2 phase 3 induction studies confirmed the efficacy of a dose of 10 mg twice daily as induction therapy for active colitis.144 In these studies, the primary end-point of remission was defined clinically and endoscopically at week 8 by a total Mayo score ≤2, with no individual subscore >1 and a rectal bleeding subscore of 0. This was achieved by 18.5% and 16.6% of patients on active treatment in OCTAVE-1 and OCTAVE-2 versus 8.2% and 3.6% of patients on placebo (p=0.007 and p<0.001, respectively). For patients who had not previously received anti-TNF therapy, remission at 8 weeks on placebo and tofacitinib was 12.5% and 23.7% respectively (difference 11.2%; 95% CI 2.6% to 17.9%). Clinical responders to induction therapy (where response was defined as a decrease from baseline in the total Mayo score of ≥3 points and >30% with a rectal bleeding score decrease of at least one or a rectal bleeding subscore of 0 or 1) were eligible for enrolment in the maintenance OCTAVE-SUSTAIN trial. Of patients randomised to tofacitinib pooled from both trials, 57.6% (521/905) had a clinical response at week 8. This included both anti-TNF naïve and anti-TNF exposed patients. They were randomised 1:1:1 to oral tofacitinib 5 mg twice daily, 10 mg twice daily or placebo. After 1 year, remission was achieved in 34.3% in the tofacitinib 5 mg group, 40.6% in the tofacitinib 10 mg group and 11.1% in the placebo group (p<0.001 for both treatment arms vs placebo).
In the OCTAVE open-label follow-on study, patients who responded to induction therapy with 10 mg twice daily, but were then randomised to placebo in the OCTAVE-SUSTAIN study and then relapsed, were retreated with 10 mg twice daily open-label.145 Of these, 75.8% responded at month 2 and 67.5% at 1 year, showing that retreatment is effective after a break in therapy. The OCTAVE open-label study also showed that patients receiving 5 mg twice daily in the OCTAVE-SUSTAIN study who relapsed and were then treated with 10 mg twice daily open-label had a response rate of 58.6% at month 2 and 68.8% at 1 year.146
Although total adverse events did not appear to differ significantly between treatment and placebo groups, there was an increased risk of infections seen in tofacitinib treated patients during both induction and maintenance phases. In particular, herpes zoster occurred more often on active treatment, a finding consistent with prior experience of use of tofacitinib in patients with rheumatoid arthritis and psoriasis.147 148 Zoster vaccination should be considered before starting therapy in those aged over 70 years and those over 50 years considered at particularly high risk (such as recurrent shingles). As a live vaccination it must not be given for 3 months after stopping biologics, and tofacitinib should not be started for 4 weeks after vaccination (see Section 5.2.1.3.2 Live vaccines). Recent data from an open-label study149 in rheumatoid arthritis patients (over 50 years with at least one cardiovascular risk factor), comparing tofacitinib 5 mg or 10 mg twice daily with TNF-inhibitor therapy, have shown a five-fold increase in pulmonary embolus for the group on 10 mg twice daily tofacitinib compared with TNF inhibitor therapy),150 and at present the European Medicines Agency safety committee advises that the high dose should not be used in patients at increased risk of pulmonary embolus (heart failure, malignancy, impending/recent surgery, inherited coagulation disorders, previous thromboembolism, combined contraceptive therapy or HRT).151 Further data are required on the risks for UC patients treated with JAK inhibitors.
No comparative data for tofacitinib with biologics are available, and NICE approval has been granted for the treatment of moderate to severely active UC where conventional treatments or biological agents have not been tolerated, or have failed.152 Tofacitinib has the advantages of oral administration and, as a small molecule, immunogenicity is not an issue. This has to be weighed against the side effect profiles and costs of different agents.
3.9.7 Ustekinumab
The UNIFI trial, recently presented in abstract form, investigated ustekinumab as induction and maintenance therapy in moderate to severely active UC in adults who had failed to respond or were intolerant to corticosteroids, immunomodulators, anti-TNF therapy (one or more) or vedolizumab.153 154 Patients were randomised 1:1:1 to receive a single IV dose of placebo, 130 mg ustekinumab, or approximately 6 mg/kg ustekinumab (weight-tiered dosing: patients weighing ≤55 kg received 260 mg; patients weighing >55 kg and ≤85 kg received 390 mg; and patients weighing >85 kg received 520 mg), as in the UNITI Crohn’s studies. At week 8, 961 patients were evaluated. The primary end-point was clinical remission at week 8 (defined as a Mayo score ≤2 points, with no individual subscore >1), and was achieved by 15.6% on 130 mg ustekinumab, 15.5% on the approximately 6 mg/kg dose and 5.3% on placebo (p<0.001).153 Endoscopic healing (defined as Mayo endoscopy subscore of 0 or 1) was 26.3%, 27% and 13.8% in the three groups, respectively (p<0.001). Clinical response (decrease from baseline Mayo score of ≥30% and ≥3 points, with either a decrease from baseline in the rectal bleeding subscore of ≥1 or a rectal bleeding subscore of 0 or 1) was 51.3%, 61.8% and 31.3% in the three groups, respectively (p<0.001). Both active treatment groups had a significant improvement in IBDQ, mucosal healing (endoscopic healing as defined above), and histological healing (defined as 0–<5% neutrophils in epithelium, no crypt destruction and no erosions, ulcerations or granulations) was 20.3%, 18.4% and 8.9% respectively at week 8. There was no difference in adverse events compared with placebo, with no malignancies, opportunistic infections or TB reported. In the maintenance continuation study, 523 patients with clinical response at week 8 were re-randomised to placebo, 8-weekly or 12-weekly dosing, with week 44 remission rates of 24%, 38.4% and 43.8%, respectively (p=0.002 for 8-weekly and p<0.001 for 12-weekly vs placebo).154 Effects were seen in both anti-TNF naïve and anti-TNF refractory patients, but numerical benefits of 8-weekly dosing (compared with 12-weekly) were restricted to the anti-TNF refractory population. The safety profile was consistent with that observed in Crohn’s disease.
At the time of writing, ustekinumab does not have licensing or NICE approval for its use in UC. It should be noted that (unlike the UNITI studies in Crohn’s disease and the GEMINI studies of vedolizumab in UC) the UNIFI study permitted inclusion of patients with failure of two classes of biologic (TNF inhibitors and vedolizumab) and results should be interpreted accordingly.
3.9.8 Methotrexate
Methotrexate has no role in the maintenance of remission in UC. A Cochrane review in 2015 of methotrexate use in comparison to placebo, 5-ASA, sulfasalazine and mercaptopurine does not support its use in maintenance of remission in UC.155 In a European double-blind randomised trial, 111 patients were allocated to 25 mg/week parenteral methotrexate versus placebo alongside prednisolone for a flare of UC.156 Methotrexate was not superior to placebo (31.7% vs 19.6% remission, p=0.15) for the primary end-point of steroid-free remission at week 16 (Mayo score ≤2 with no item >1 and complete withdrawal of steroids and no use of another immunosuppressant (IS), anti-TNF therapy or colectomy). Clinical remission at week 16 (Mayo score ≤2 with no item >1) was, however, significantly higher on methotrexate (41.7% vs 23.5% p=0.04). The MERIT study treated 179 patients with active UC with open-label methotrexate 25 mg SC weekly, plus a tapering prednisolone course for 12 weeks. At 16 weeks there was a 51% response rate, and 84 patients were randomised to continue 25 mg methotrexate SC or placebo. There was no difference in outcome at week 48, with 27% of those on methotrexate and 30% on placebo maintaining steroid-free clinical remission with no need for additional therapies.157
3.9.9 Choice of immunosuppressive or biological therapy
Patients with chronic active UC failing 5-ASA therapy have in the past been offered thiopurine therapy. As the range of alternatives grows and costs of biologics fall, there is strong justification for moving directly to other immunosuppressive drugs with less toxicity that may be easier to manage. Thiopurines still have a role as combination therapy and to reduce immunogenicity, but the therapeutic pyramid is changing rapidly.
Until the VARSITY study comparing vedolizumab with adalimumab,142 there had been no head-to-head studies comparing anti-TNF drugs, vedolizumab, tofacitinib and ustekinumab. Indirect means of comparison are much weaker and, at best, hypothesis-generating. Network meta-analyses have compared vedolizumab with anti-TNF drugs and show broadly similar benefits.158–160 In contrast, the VARSITY trial shows a significant benefit for vedolizumab compared with adalimumab 40 mg every other week.142 Two network meta-analyses that include tofacitinib, one in abstract form, show comparable efficacy to anti-TNF agents and vedolizumab.161 162 The choice of which immunosuppressive agent to use depends on a number of factors (box 2). Patients may prefer to receive oral or subcutaneous therapy rather than intravenous therapy, although the latter may be preferred for patients where non-adherence may be an issue. Tofacitinib as an oral agent, with no concerns about immunogenicity, is an attractive choice, but with little real-world experience as yet. Gut-selective therapy may be considered safer because of concerns about risk of malignancy or infection; at present there is little long-term comparative safety data between vedolizumab and anti-TNF therapy to support this, although the long-term trial extension safety profile over 9 years from the GEMINI trials is very reassuring.163 The presence of significant extraintestinal manifestations may also be a consideration. Other practical issues are shown in box 2.
Factors to consider in choosing a biologic, immunosuppressive or immunomodulator therapy
Route of administration (oral, subcutaneous, intramuscular, intravenous)
Speed of response to induction therapy (consider need for bridging therapy)
Potential immunogenicity and need for combination therapy
Side effects including cancer risk
Persistence (continuing drug without loss of response after initial improvement)
Availability of infusion facilities and therapeutic drug monitoring
Overall cost (including drug delivery and monitoring)
3.9.10 Therapeutic choice after anti-TNF failure
Infliximab and other anti-TNF drugs have been used in UC for many years, and it is therefore important to consider alternatives for patients failing these drugs and who need to switch ‘out of class’ (see Sections 5.2.4.5: Common Disease Considerations, Primary non-response to anti-TNF therapy and 5.2.4.6: Common Disease Considerations, Secondary loss of response to anti-TNF therapy). It is important to note that surgery should always be discussed as an option in patients failing a therapeutic agent, particularly as there is generally a reduction in response to each successive immunosuppressive or biologic drug.
3.9.10.1 Vedolizumab after anti-TNF therapy
Statement 10. We recommend that vedolizumab can be used in the induction and maintenance of remission of ulcerative colitis in patients where anti-TNF treatment has failed (GRADE: strong recommendation, high-quality evidence. Agreement: 97.7%).
In the GEMINI I study of vedolizumab in active UC, 895 patients were enrolled and randomised responders were re-randomised to maintenance therapy or placebo.138 367 patients (41%) had prior failure of anti-TNF therapy. Of these patients, clinical response at week 6 was 39% for vedolizumab versus 20.6% for placebo (difference 18.1%, 95% CI 2.8% to 33.5%). Of the randomised responders entering the maintenance phase who had prior anti-TNF failure, clinical remission at week 52 was 36.1% for vedolizumab (given either 8- or 4-weekly) versus 5.3% for placebo (difference 29.5%, 95% CI 12.8% to 46.1%). Vedolizumab is effective in patients with prior exposure to anti-TNF drugs, although benefits are larger in those with no prior exposure.139 Data on clinical efficacy and safety from prospectively followed cohorts on vedolizumab are now available. In a recently reported GETAID study, 294 patients with active IBD (121 with UC), with an inadequate or loss of response to conventional therapy or at least one anti-TNF agent, were treated with vedolizumab.164 Concomitant use of corticosteroids, thiopurines or methotrexate was permitted. Among patients with UC, 36% were in steroid-free clinical remission and 50% had clinical response at week 14. In a review of safety data from vedolizumab trials, prior anti-TNF therapy was a risk factor for serious infection in UC patients (HR 1.99, 95% CI 1.16 to 3.42; p=0.0122). Eighteen vedolizumab exposed patients (<1%) were diagnosed with a malignancy including non-melanoma skin cancer, malignant melanoma, colon cancer, breast cancer, renal, liver and lung cancer; nearly all patients (except one with renal cancer) having had prior exposure to thiopurines and/or anti-TNF agents, making attribution difficult.165
3.9.10.2 Tofacitinib after anti-TNF therapy
Statement 11. We recommend that tofacitinib can be used in the induction and maintenance of remission of ulcerative colitis in patients where anti-TNF treatment has failed (GRADE: strong recommendation, high-quality evidence. Agreement: 91.1%).
In pooled data from the OCTAVE 1 and 2 trials, 589 patients had previously failed anti-TNF and had a week 8 clinical remission rate of 0.8% on placebo versus 11.4% on tofacitinib 10 mg twice daily (difference 10.6%, 95% CI 7.3% to 13.9%).166 Mucosal healing at week 8 (Mayo endoscopic subscore of 0 or 1) in patients with prior anti-TNF exposure was 6.5% on placebo versus 22.2% on tofacitinib 10 mg twice daily (difference 15.7%, 95% CI 10.0% to 21.4%). In OCTAVE-SUSTAIN, week 52 remission data for placebo, tofacitinib 5 mg twice daily and 10 mg twice daily in patients with prior anti-TNF failure were 11.2%, 24.1% and 36.6%, respectively, for clinical remission and 12.4%, 30.1% and 39.8%, respectively, for mucosal healing.
3.10 Proctitis
3.10.1 5-ASA suppositories in proctitis
Statement 12. We recommend that mild or moderately active ulcerative proctitis should be treated with a 1 g 5-ASA suppository (GRADE: strong recommendation, high-quality evidence. Agreement: 100%).
When treating mild to moderate proctitis, first-line therapy should be 5-ASA suppositories. These medications achieve much higher mucosal concentrations of the drug and work faster and better than oral 5-ASA monotherapy in disease which is confined to the rectum.167 Higher response rates are achieved if topical therapies are combined with oral 5-ASA,168 thus patients not responding fully to suppositories should have early addition of oral therapy. Suppositories are preferred to enemas for proctitis as they deliver the drug specifically to the rectum (enemas tend to pool higher up in the sigmoid) and are also better tolerated/retained, as shown in a study comparing 5-ASA suppositories with hydrocortisone foam enemas.169 Topical 5-ASA is more effective than topical corticosteroid.170 A Cochrane review did not show a dose–response relationship for rectal therapy (although this review assessed treatment of distal colitis, which included both proctitis and left-sided colitis up to the splenic flexure).171 A further review evaluating mucosal healing showed a dose–response relationship for oral but not rectal 5-ASA (again evaluating proctitis along with distal colitis).172 Divided doses are less convenient for patients. A study comparing 1 g 5-ASA suppository daily versus 500 mg three times daily showed more convenience and similar efficacy (except for mucosal healing) for the once daily dose,173 and a further study showed no difference between 1 g daily and 500 mg twice daily.174 Administering this dose at bedtime is practical for most patients, allowing the suppository to be retained for the longest possible time.171
3.10.2 Maintenance therapy for proctitis
Many patients respond promptly to 5-ASA suppositories, and if they have infrequent flares, are happy to start suppositories when they begin to flare and not take regular maintenance therapy. This is quite safe as the colorectal cancer risk in proctitis is similar to the general population. For many, however, regular preventive treatment is needed, and 5-ASA suppositories are the most effective maintenance therapy for proctitis.109 175 In long-term treatment, however, this needs to be weighed against the importance of adherence, and some patients may choose not to use long-term rectal therapy and prefer oral therapy. It is worth noting that alternate night or every third night suppositories do not appear to reduce the rate of maintenance of remission substantially.170
3.10.3 Corticosteroid suppositories in proctitis
Statement 13. We suggest that patients with ulcerative proctitis who do not respond or are intolerant to 5-ASA suppositories and oral 5-ASA may be switched to corticosteroid suppositories (GRADE: weak recommendation, low-quality evidence. Agreement: 84.8%).
Steroid suppositories are also effective in proctitis but not as effective as 5-ASA and so their use should be confined to those who either do not tolerate or do not respond to 5-ASA.171 176 Oral 5-ASA should be continued if possible. For those not responding to 5-ASA, the addition of a prednisolone 5 mg suppository in the morning while continuing 5-ASA suppositories at bedtime is worth trying. A novel budesonide suppository was studied in a four-group, prospective, double-blind, double-dummy randomised trial to treat UC proctitis with budesonide 2 mg, budesonide 4 mg, 5-ASA 1 g, or budesonide 2 mg plus 5-ASA 1 g.177 The 8-week study conducted in Germany, Russia and the UK assessed a primary end-point of resolution of clinical symptoms for three consecutive days (score of 0 for rectal bleeding and stool frequency on modified UCDAI). Budesonide 4 mg was more effective than 2 mg, but no different from 5-ASA 1 g or the combination of budesonide 2 mg and 5-ASA 1 g.
3.10.4 Treatment options in refractory proctitis
Statement 14. We suggest that refractory ulcerative proctitis may require treatment with corticosteroids, immunomodulators and/or biological therapy (GRADE: weak recommendation, very low-quality evidence. Agreement: 95.5%).
A proctitis management flowchart is shown in figure 1. In severe or refractory proctitis, it is important to ensure that conventional therapy has been delivered appropriately (with assessment of adherence) and that the diagnosis is correct. Proximal constipation is common and may contribute to symptoms and poor response to therapy, as may co-existing irritable bowel syndrome. It is important to exclude other conditions that may be causing symptoms, including infection (lymphogranuloma venereum, Neisseria gonorrhoeae, herpes simplex virus, syphilis, Giardia duodenalis, amoebiasis), solitary rectal ulcer, psoriatic colitis, chemical colitis and rectal prolapse.178
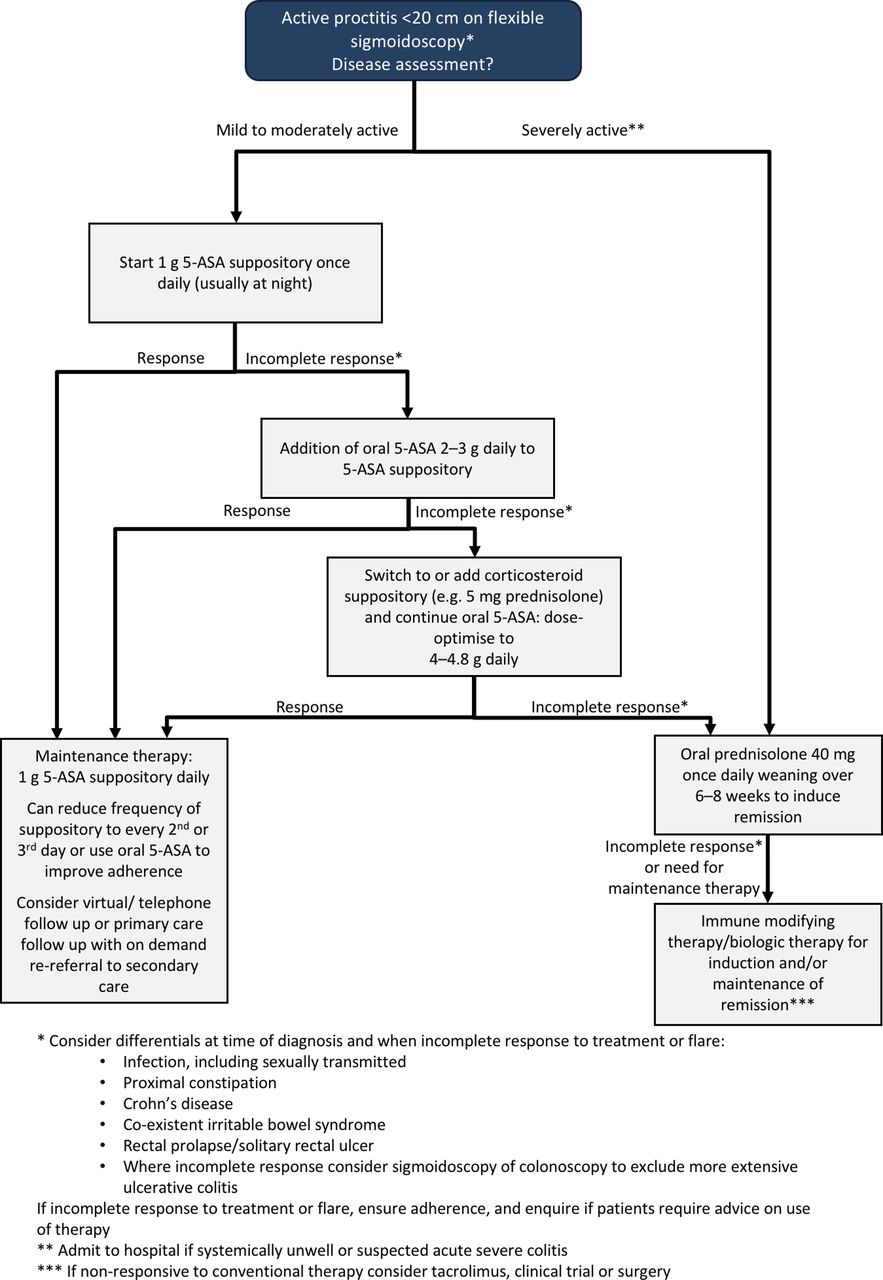
Management of proctitis.
If the diagnosis is correct and standard therapy has failed, then thiopurine therapy should be added,179 with escalation to biologics if no response.180–182 Many UC trials have excluded proctitis, but a case series of infliximab therapy for proctitis confirms good response.183 Patients with refractory proctitis have disabling symptoms but are often systemically well and are usually very reluctant to have proctocolectomy, so many other therapies have been assessed. There are many other treatments based on small trials or case series—for example, rectal tacrolimus (0.5 mg/mL, dose 3 mL twice daily)—although active absorption results in significant serum levels and close monitoring and dose adjustment are required to avoid toxicity.184
3.11 Stopping 5-ASA or thiopurine therapy
Evidence from many UC trials show that patients with a longer duration of remission have lower relapse rates, and duration of remission is an independent predictor, regardless of treatment received.185 186 Trials have also shown that age is a risk factor with relapse rates inversely proportional to age.185 187 A study of mesalazine maintenance therapy evaluated patients with UC in established clinical, endoscopic and histological remission (on the basis of sigmoidoscopy), and divided them into a short remission group (1–2 years) and prolonged remission (>2 years, with a median of 4 years). Patients were randomised to receive mesalazine 1.2 g daily or placebo. In the short remission group relapse rate at 1 year was 23% on mesalazine and 49% on placebo (p=0.035). In the prolonged remission group there was no significant difference whether on mesalazine (relapse in 18%) or placebo (26%). The prolonged remission group were also older and had longer duration of disease.188
As well as consideration of the relapse-preventing value of 5-ASA in prolonged remission, the other consideration is the potential colorectal cancer-preventing benefits. There are theoretical reasons why 5-ASA may have colorectal cancer preventive properties,189 but unclear whether 5-ASA has benefit independently, or whether the documented benefit relates to mucosal healing. Colorectal cancer risk is related to inflammation.55 190 Therefore, it is plausible that mucosal healing should be the main goal of colorectal cancer prevention, regardless of the treatment used.191 Patients should be advised that 5-ASA is a safe and effective long-term treatment, and should be advised that if they have documented prolonged clinical and endoscopic remission, there is no clear evidence whether continuing 5-ASA adds additional reduction in colorectal cancer risk, but if subsequent assessment after stopping 5-ASA shows mucosal inflammation, 5-ASA should be restarted.
Most of the published data on withdrawal of thiopurines evaluates UC patients in remission for 1–2 years only. In the only randomised controlled withdrawal trial of azathioprine, there was a relapse rate of nearly 60% at the end of the first year in those who discontinued the drug while in corticosteroid-free clinical remission (for a mean of 11–12 months) compared with 36% on continued azathioprine.185 Other cohort studies with marked heterogeneity in study design and follow-up have reported relapse rates ranging from 21% to 100% at 2 years.192 A prospective study in patients with UC stopping azathioprine after a minimum of 3 years of therapy in clinical, biological, and endoscopic remission showed a relapse rate of 37% after a mean follow-up of 55 months.193 The risks of relapse are likely to be much lower in patients with prolonged remission (5–10 years) and the benefits of continuing therapy are likely to be less than the risk of drug toxicity, including lymphoma. In the event of relapse there is a very high likelihood of regaining remission; 92% in one observational study.194 Relapse rates are lower in those continuing 5-ASA therapy,193 195 so all patients stopping thiopurines should be receiving 5-ASA if tolerated. In the absence of high-quality data, stopping thiopurines may be an option for those in long term (5–10 years or more) clinical, endoscopic and histological remission, after appropriate patient counselling. Periodic calprotectin monitoring may be a cost-effective method of monitoring ongoing mucosal healing after cessation.
3.12 Acute severe ulcerative colitis
Statement 15. We recommend that adult patients with acute severe ulcerative colitis (ASUC) (defined by the modified Truelove and Witts criteria as >6 bloody stools per day and systemic toxicity with at least one of: temperature >37.8°C, pulse >90 bpm, haemoglobin <105 g/L or C-reactive protein >30 mg/L) or adolescents with a Paediatric Ulcerative Colitis Activity Index (PUCAI) score of 65 or more should be admitted to hospital for assessment and intensive management (GRADE: strong recommendation, low-quality evidence. Agreement: 100%).
Between 15% and 25% of patients with UC will require hospitalisation for an acute severe flare of disease at some stage in the natural history of their disease, often as the index presentation.196 Acute severe ulcerative colitis (ASUC) is a potentially life-threatening condition, characterised by clinical and laboratory assessment using the modified Truelove and Witts criteria102 or, in the case of adolescent patients, the Paediatric UC activity index.197 In current practice C-reactive protein is measured far more than ESR, and has the advantage of a less non-specific increase with age.198 A retrospective UK study (1950–2007) showed that the colectomy rate during first admission with ASUC was 19%, but after several admissions rose to 38.2%.199 In the biologics era, the colectomy rate after admission for ASUC in the CONSTRUCT trial was 23% during the inpatient stay,200 and in another study was 19% at 2 years.201
Statement 16. We recommend that patients presenting with possible acute severe colitis should have urgent inpatient assessment and blood tests (FBC, CRP, U&E, LFTs and magnesium), stool culture, Clostridium difficile assay, radiological imaging (AXR or CT) and flexible sigmoidoscopy (GRADE: strong recommendation, very low-quality evidence. Agreement: 97.9%).
All patients admitted with ASUC should have baseline bloods (FBC, CRP, U&E, LFT and magnesium, stool culture and Clostridium difficile assay, radiological imaging (AXR or CT) and flexible sigmoidoscopy, with close monitoring after admission. MRI and ultrasound may have a role in determining the extent of colitis, but are less sensitive than CT in detecting perforation. The results of these tests will also assist in determining the prognosis for that admission (particularly to predict corticosteroid failure and the need for colectomy).196 202 Early flexible sigmoidoscopy is important to confirm diagnosis and obtain histology including evaluation for cytomegalovirus (CMV) (see Section 5.1.4cytomegalovirus infection in IBD) and prognosis. Stool culture and microscopy should be performed routinely, as soon as practicable, to exclude pathogenic bacteria including testing for C. difficile toxin. An accurate stool chart, recording frequency, consistency and the presence of blood should be kept, with patients instructed to keep this record if they are able to do so. As nearly half are likely to fail intravenous corticosteroids,200 consideration should be given to pre-biologics screening for all ASUC patients on admission.
3.12.1 Corticosteroid therapy for ASUC
Statement 17. We recommend that patients with ASUC should be treated with high-dose intravenous corticosteroids such as methylprednisolone 60 mg daily or hydrocortisone 100 mg 6-hourly (GRADE: strong recommendation, high-quality evidence) and should receive prophylactic low-molecular weight heparin (GRADE: strong recommendation, moderate-quality evidence. Agreement: 97.8%).
Intravenous corticosteroids such as hydrocortisone 100 mg four times daily or methylprednisolone 60 mg every 24 hours are the cornerstone of treatment of ASUC.106 203–205 Methylprednisolone has less mineralocorticoid effect than hydrocortisone at these doses and so causes significantly less hypokalaemia.206 There is no real advantage from giving higher doses and a bolus injection is as effective as a continuous infusion.207 Although a meta-regression analysis failed to show a relationship between dose and colectomy rate above the equivalent of 60 mg methylprednisolone,106 400 mg hydrocortisone is equivalent to 80 mg methylprednisolone. In children and adolescents, a dose of 1–1.5 mg/kg/day up to a maximum of 60 mg is recommended.208
In the landmark study by Truelove and Witts,102 oral cortisone 100 mg daily was given to 213 patients with acute flares of varying severity. Clinical remission was achieved in 41% of steroid treated patients versus 16% on placebo. In a subsequent study, 49 patients with severe UC were treated with intravenous prednisolone 21-phosphate and a clinical remission rate of 73% was noted 5 days after treatment.209 Definitions and terms differed widely in these studies compared with outcome measures in use today. A systematic review of 32 trials of steroid therapy for ASUC involving 1991 patients reported an overall response to steroids of 67%, with 29% (95% CI 28% to 31%) having colectomy. Mortality was 1% (n=22/1991; 95% CI 0.7% to 1.6%) and none of these outcomes changed between 1974 and 2006 (R2=0.07, p=0.8).106 In the CONSTRUCT cohort, after excluding those with infections or alternative diagnoses, response rate to intravenous steroids was 49%.200 Extending therapy beyond 7–10 days carries no additional benefit and increases toxicity.104 105 Patients should be assessed for a clinical and biochemical response after 3 days of intravenous steroid therapy to determine the need for salvage medical or surgical therapy.106 210
Risk of venous thromboembolism (VTE) is 2–3 fold higher compared with inpatients without IBD, so prophylactic subcutaneous low molecular weight heparin is important204 211 212 and does not precipitate or exacerbate colonic bleeding.213
Good Practice Recommendation 1. Corticosteroid treatment for patients with suspected ASUC should not be delayed pending results of stool cultures and Clostridium difficile assay (Agreement: 95.6%).
ASUC patients should have stool culture and Clostridium difficile toxin assay.214 215 C. difficile infection has been associated with a worse outcome in hospitalised IBD patients.216–218 If C. difficile is detected (or strongly suspected), treatment with corticosteroids should not be withheld, but additional treatment with oral vancomycin given219 (see Section 5.1.3: Common Disease Considerations, Clostridium difficile infection associated with IBD). Amoebiasis should be considered in those with recent travel to endemic areas, in whom consideration should be given to addition of metronidazole pending stool microscopy and culture.
3.12.2 Predictors of outcomes of ASUC
Most studies of factors predicting colectomy in ASUC look at patients treated with intravenous steroids±salvage therapy and do not specifically look at factors after ciclosporin or infliximab have been started. Low albumin is predictive of colectomy,220 221 with one study showing that albumin on day 3 of corticosteroid treatment was the only predictor of colectomy on multivariable analysis.222 A CRP/albumin ratio of 0.85 on day 3 of intravenous steroids also predicted colectomy with a sensitivity of 70%, specificity 76%.223 Flexible sigmoidoscopy performed with care is safe in ASUC and gives important information about disease severity.224 Severe endoscopic lesions (deep ulcers, extensive loss of mucosal layers, well-like ulcers or large erosions) have been associated with non-response to corticosteroids225 and colectomy.226 227 A study of 89 ASUC patients treated with intravenous corticosteroids and/or infliximab or ciclosporin used the UCEIS and showed that almost all patients with a UCEIS score of 7 or more on admission required rescue therapy,228 and another study shows UCEIS is predictive of need for rescue therapy and for surgery.229
3.12.3 Ciclosporin or infliximab rescue therapy for ASUC
Statement 18. We recommend that patients with ASUC failing to respond by day 3, as judged by a suitable scoring system, should be treated with rescue therapy in the form of intravenous infliximab or ciclosporin for patients who have not previously failed thiopurine therapy (GRADE: strong recommendation, high-quality evidence. Agreement: 97.8%).
Patients who do not respond to corticosteroid therapy after 3 days should be considered for second-line ‘rescue’ therapy or surgery. Early clinical risk stratification tools can be used to predict failure of medical therapy (table 5); those at high risk of failure should be offered rescue therapy after discussion with the colorectal surgeon (figure 2).
Indices predictive of failure of corticosteroid therapy for ASUC

Management of acute severe ulcerative colitis.
3.12.4 Ciclosporin in ASUC
The striking benefits of ciclosporin in ASUC were shown in a 1994 paper.230 A randomised controlled trial showed that 2 mg/kg intravenous ciclosporin was as effective as 4 mg/kg in ASUC, with response rates at day 8 of 83% and 82%, respectively with no difference in colectomy rates.231 Reviews have shown short-term colectomy rates in patients receiving intravenous ciclosporin vary from 26% to 47%.196 210 The initial ciclosporin dose is 2 mg/kg/day intravenously with a target trough ciclosporin concentration of 150–250 ng/mL.231 Responders should be converted to an oral dose twice the intravenous dose and administered in divided doses twice daily with a target trough concentration of 100–200 ng/mL.200 Oral ciclosporin should be continued for several months as bridging therapy,230–234 and long-term outcomes are much better if thiopurine maintenance therapy is given, rising from 40% to 66% in one study.235 Those requiring ciclosporin salvage therapy who have already failed thiopurine therapy have much worse outcomes.233 236
Large case series of ciclosporin therapy in UC have reported a significant toxicity profile, with serious infections in 5% of patients and mortality in 1–3%.233 237 238 Major adverse events related to ciclosporin therapy include nephrotoxicity (6.3%), seizures (3.6%), anaphylaxis (0.9%) and death (1.8%).238
3.12.5 Infliximab in ASUC
Infliximab is also effective in ASUC.220 239 240 Long-term follow-up data of the original Swedish trial239 which studied a single infusion of infliximab showed a significantly lower colectomy rate compared with controls (50% vs 76%; p=0.01) at 3 years, without use of maintenance infliximab.241 Contraindications to use include latent tuberculosis (TB), active sepsis, congestive heart failure and demyelination, and screening is required before starting treatment. Combination therapy using azathioprine with infliximab has a synergistic effect, with evidence of benefit in raising infliximab levels and reducing antibody formation against infliximab,242 even in patients who have previously failed monotherapy with thiopurines. Azathioprine or mercaptopurine should be started during hospitalisation and continued after discharge. Once patients have responded well to rescue therapy, corticosteroid doses should be tailed. Prophylaxis for Pneumocystis jirovecii should be given for those on 20 mg prednisolone or more (see Section 5.2.8.6: Common Disease Considerations, Prevention of Pneumocystis jirovecii infection).
3.12.6 Comparison of infliximab and ciclosporin in ASUC
Head-to-head comparisons between ciclosporin and infliximab have demonstrated equivalent efficacy. In the open label CySIF trial, 115 patients previously naïve to infliximab and ciclosporin, who had a Lichtiger score >10 points (range 0–21) and colitis refractory to at least 5 days of intravenous steroids, were randomised in a 1:1 ratio to receive intravenous ciclosporin (2 mg/kg per day for 1 week followed by oral drug until day 98) or infliximab (5 mg/kg on days 0, 14 and 42).243 In both groups, azathioprine was started at day 7 in patients with a clinical response. The primary end-point was treatment failure defined by absence of a clinical response at day 7, a relapse between day 7 and day 98, absence of steroid-free remission at day 98, a severe adverse event leading to treatment interruption, colectomy or death. There was no statistically significant difference between treatment failure in patients given ciclosporin (60%) and infliximab (54%). Nine (16%) patients in the ciclosporin group and 14 (25%) in the infliximab group had severe adverse events, which was also not statistically different. Similar mucosal healing rates (47% ciclosporin, 45% infliximab) and colectomy rates (17% ciclosporin, 21% infliximab) were achieved in both groups. There was no difference in colectomy-free survival at 1 and 5 years in patients treated with either ciclosporin or infliximab.244
The CONSTRUCT trial was an open-label pragmatic randomised trial in 270 patients, who were randomly allocated (1:1) to receive either infliximab (5 mg/kg intravenous infusion given over 2 hours at baseline and again at 2 weeks and 6 weeks after the first infusion) or ciclosporin (2 mg/kg per day by continuous infusion for up to 7 days followed by twice-daily tablets delivering 5.5 mg/kg per day for 12 weeks). The primary outcome was quality-adjusted survival; the area under the curve of scores from the Crohn’s and Ulcerative Colitis Questionnaire completed by participants at baseline, 3 months, and 6 months, then every 6 months from 1 year to 3 years.200 There was no statistically significant difference between the two groups for the primary end-point as well as the secondary end-point of colectomy rates, time to colectomy, serious adverse events or death. Colectomy rates were 29% for infliximab and 30% for ciclosporin at 3 months, and 35% and 45% respectively at 1 year, with no significant difference between the treatments.200 However, treatment with infliximab was associated with greater cost of treatment compared with ciclosporin.
A meta-analysis of infliximab and ciclosporin randomised controlled trials shows no difference in response up to 1 year.245 In the Spanish ENEIDA registry, where patients with steroid unresponsive ASUC were treated with ciclosporin (the majority of whom were given azathioprine maintenance therapy), the colectomy rate at 5 years was 25.4%. For those treated with infliximab, either continuing repeat infusions, combination therapy with azathioprine, or azathioprine only, the 5-year colectomy rate was similar at 26.2%.234
Mortality from infliximab trials is comparable to data on ciclosporin (0–2%).196 210 234 The most significant risk for both infliximab and ciclosporin relates to those on either of these drugs combined with high-dose corticosteroids who fail medical treatment and go on to colectomy with deteriorating physical condition (anaemia, hypoalbuminaemia and oedema) where surgical complications are a significant concern (see Section 3.12.9:Ulcerative Colitis, Surgery for acute severe UC).
Ciclosporin and infliximab are equally effective in ASUC. Infliximab, however, is simpler to use and is thus used much more widely now. Although infliximab was more expensive, use of biosimilars is bringing costs down.
3.12.7 Sequential therapy (infliximab and ciclosporin) in refractory ASUC
Sequential therapy with infliximab and ciclosporin can be associated with profound immunosuppression and potentially risks serious adverse events and infections and is not recommended,246 247 although a recent review suggested that the risks were not excessive (on the basis of low-quality data).248 In the ENEIDA registry sequential therapy was defined as treatment with the second agent (ciclosporin or infliximab) within 3 months after the steroid-refractory ASUC attack, and was used in 10% of those with long-term outcomes available.234 The median time between treatments was 24 days (95% CI 2.5 to 75.0), and showed comparable safety to use of one rescue therapy only. The greatest risk of this approach is delaying surgery in a patient whose physical condition is deteriorating.
3.12.8 Accelerated infliximab induction regimen in ASUC
Statement 19. We suggest that patients treated with infliximab for ASUC who have not responded sufficiently to a 5 mg/kg dose 3–5 days after first infusion should be treated with an accelerated induction regimen after colorectal surgical review to determine whether emergency colectomy is required (GRADE: weak recommendation, low-quality evidence. Agreement: 95.7%).
Recent studies have demonstrated an association between higher serum levels of anti-TNF and better outcomes.249 A post hoc analysis of ACT 1 and 2 clinical trials noted that patients in the lowest quartile of infliximab serum concentration were less likely to achieve clinical response, remission and mucosal healing, independent of randomised dose (5 mg/kg or 10 mg/kg).250
Various factors, including a high TNF burden in ASUC, proteolytic degradation of anti-TNF associated with increased drug clearance and faecal losses from increased gut permeability due to severe inflammation, support the need for dose optimisation of infliximab in the acute phase.251 In a recent study, serum and non-inflamed tissue anti-TNF drug levels were shown to be related, but serum and tissue drug levels were not associated in inflamed tissue.252 This suggests that high mucosal cytokine levels during inflammation act as a ‘sink’ for drug, and thus a higher serum level of the drug may be required to neutralise tissue TNF. In another study, a high baseline CRP (>50 mg/L) and a low serum albumin (<35 g/L), as surrogates for severe inflammation and extensive colitis, independently correlated with lower infliximab concentrations from week 0–6.253
There is further evidence of benefit with accelerated infliximab dosing in ASUC. Three doses of accelerated infliximab dosing at 5 mg/kg, administered over a median 24 days to steroid-refractory patients, demonstrated a colectomy rate of 6.7% compared with 40% in a retrospective cohort (standard 5 mg/kg induction at 0, 2 and 6 weeks).254 For those completing induction therapy, the colectomy rates during follow-up were similar (median follow-up of 2.4 years for standard dosing and 1.6 years for accelerated dosing regimen). A recent review suggested that dose intensification may benefit half of patients with ASUC treated with infliximab, with case control studies showing that 1–2 extra infusions in the first 3 weeks can dramatically reduce colectomy rates.251
Patients treated with infliximab who are not responding sufficiently to a 5 mg/kg dose after 3–5 days can be treated with an early repeat infusion, particularly in those with a low albumin (below 35 g/L). Some clinicians use an initial 10 mg/kg dose as salvage therapy but there is as yet insufficient data to demonstrate the value of this in comparison to a 5 mg/kg dose.255 Optimal timing and dose (5 mg/kg or 10 mg/kg) are as yet unclear. Accelerated dosing should only be given after colorectal surgical review, with agreement that colectomy is not required imminently (see figure 2). Further studies are required to evaluate the use of drug levels and biomarkers to determine personalised dosing for patients.
3.12.9 Colectomy for ASUC
Good Practice Recommendation 2. In acute severe ulcerative colitis, delay in surgery is associated with an increased risk of surgical complications, mandating early referral and direct involvement of specialist colorectal surgical and stoma care teams (Agreement: 100%).
Outcomes from ASUC were revolutionised by the use of corticosteroids and the introduction of timely surgery in those who had not responded. Mortality plummeted from 24% to <1% in the landmark studies.102 256 Despite rescue therapy, a significant number of patients still go to surgery in the acute situation. Although meta-analysis has not shown evidence that infliximab increases postoperative complications in UC,257 a recent series has shown that outcomes for surgery have been worse since the introduction of biologics.258 One possible explanation for this discrepancy would be that, in the case of ASUC, using biologics as rescue therapy after failure of corticosteroids creates a delay in surgery. Although thromboembolic complications are a significant risk,259 a recent study did not show a difference between those going to surgery after steroids only and those receiving steroids and ‘rescue therapy’ prior to colectomy. Both groups however had been inpatients for a long time before surgery (10 vs 12 days).260
Statement 20. We recommend that patients with ASUC who have not responded within 7 days of rescue therapy with infliximab or ciclosporin, or those with a deterioration or complications before that time (including toxic megacolon, severe haemorrhage or perforation) require subtotal colectomy and ileostomy, with preservation of the rectum (GRADE: strong recommendation, very low-quality evidence. Agreement: 97.4%).
Timely decision-making is therefore important in order to prevent delays or prolongation of medical therapy, as those failing medical therapy and undergoing colectomy have higher postoperative complication rates after delayed surgery.105 Prolonged admission prior to surgery was the only significant predictor of postoperative complications in another study.261 In a study from the USA, mortality in those who had colectomy within 3 days of admission was used as a comparator.262 For those with colectomy up to 6 days, the adjusted ORs for postoperative death was 2.12 (95% CI 1.13 to 3.97) and 2.89 (95% CI 1.41 to 5.91) for colectomy up to 11 days.
Multidisciplinary team involvement with gastroenterologist, colorectal surgeon, and stoma therapist enables better management.196 263 Surgical input at an early stage helps patients to understand that colectomy is an important treatment option and is not an outcome to be avoided at any cost. Prompt joint decision-making is essential to avoid unnecessary delays (figure 2).
3.13 Surgical management in UC
3.13.1 Emergency colectomy for UC
Surgery in ASUC is indicated when the disease is medically resistant, there are intolerable side effects of medication, or when there is life-threatening haemorrhage, toxic megacolon or perforation.264 Toxic megacolon is a devastating complication of severe colitis, characterised by radiographic distension of the colon often with fever, tachycardia, neutrophil leucocytosis and anaemia.
In this setting, the operation of choice is a subtotal colectomy and end ileostomy with long rectal stump.259 265 266 This could be performed laparoscopically or open according to local expertise, although a laparoscopic approach is likely to result in shorter length of stay and reduced risk of infectious complications.267–269
Care should be taken to avoid leakage from the rectosigmoid stump, either by formation of mucous fistula, locating the top of the remnant in the subcutaneous tissue of the abdominal wall, or closing the stump but leaving a transanal catheter in the initial postoperative period to prevent stump ’blow-out', with no clear evidence of the preferred technique.269 If the patient wishes to consider restoration of intestinal continuity with a proctectomy and ileoanal pouch, this should not be undertaken in the acute setting, given the significant risk of complications in a patient who is likely to be clinically unwell, hypoalbuminaemic and on immunosuppressive medication. Timing of pouch surgery should be an individualised decision with multidisciplinary input, with a minimum of 3 months and preferably 6 months from the initial subtotal colectomy in order that adhesions may be safely manageable and the patient allowed time to generally recover from the initial procedure. A population cohort study from Sweden showed that the median time to subsequent reconstructive surgery is almost 12 months.270 At the time of ileoanal pouch surgery, a temporary covering loop ileostomy will reduce the clinical anastomotic leak rate as well as the septic sequelae of a leak, but may be omitted in optimal circumstances.269 A subsequent anastomotic leak from a non-defunctioned ileal pouch-anal anastomosis would generally require defunctioning.
3.13.2 Outcomes after colectomy for UC
Statement 21. We suggest that surgical resection of the colon and rectum in ulcerative colitis should be offered to patients who have chronic active symptoms despite optimal medical therapy. Ileoanal pouch reconstruction or end ileostomy provide equivalently good quality of life, and are a matter of patient choice (GRADE: weak recommendation, very low-quality evidence. Agreement: 94.4%).
Proctocolectomy followed by ileal pouch anal anastomosis (IPAA) is well-established as a management option for UC. Multiple case series have demonstrated good outcomes in terms of quality of life, with a majority of patients indicating they would undertake the same procedure again.271–274 In one of the larger series, 95% of patients reported good or excellent functional and quality of life outcomes over up to 10 years of follow-up.273 A further study showed no deterioration in functional outcome over 10 years or more.275 Comparison with medical therapies are difficult since there are no published comparative data, and in the absence of randomisation there would be selection bias. Comparison of IPAA to end ileostomy suggests that both are associated with equivalent quality of life, and the decision should be a matter of patient choice after detailed explanation and counselling. Functional outcomes are just as good after laparoscopic-assisted pouch surgery.276
Statement 22. We suggest that pouch surgery should be performed in specialist high-volume referral centres (GRADE: weak recommendation, low-quality evidence. Agreement 97.4%).
Ileoanal pouch surgery is not currently a centralised service in the UK. However, data from the UK suggest that high-volume centres (more than 100 procedures between 1996 and 2008) had lower pouch failure rates.277 In this study, high-volume centres had a pouch failure rate of 5.2%, similar to the rate of 5.3% reported from the Cleveland Clinic (5.3%) in the USA.273 A further study showed that there is a significant learning curve for pouch surgery, with improving outcomes dependent on the number of procedures undertaken for both trainees and senior staff.278 Likewise, there is evidence that management of leaks after IPAA procedure improves with increasing experience, and results in better pouch salvage rates.279
3.13.3 Surgery in UC patients with primary sclerosing cholangitis
Good Practice Recommendation 3. Patients undergoing colectomy who have co-existent ulcerative colitis and primary sclerosing cholangitis should be advised that there is an increased risk of pouchitis, to inform decision-making regarding ileoanal pouch formation or permanent ileostomy (Agreement: 100%).
While the occurrence of complications following IPAA surgery in patients with co-existent UC and primary sclerosing cholangitis (PSC) is high, the risk of pouch failure is low. The most common short- and long-term complication is pouchitis, with acute, recurrent acute and chronic pouchitis all occurring frequently. The largest published series of 100 patients with co-existent UC and PSC with IPAA followed for a median of 5.9 years, reports 30-day complication rates of 39% and overall pouchitis rates of 64%.280 Pouch excision was only necessary in 3% of patients in this series. Other smaller series present similar data with high rates of pouchitis, although whether the rate is higher than in the non-PSC UC cohort is unclear, with data conflicting.281–283 For PSC patients with UC undergoing liver transplantation, graft outcomes are better for those who have an end ileostomy after colectomy compared with colectomy and IPAA.284 Graft loss was mainly associated with hepatic artery thrombosis and biliary strictures. The risk associated with IPAA is not dependent on the timing of colectomy in relation to the liver transplantation. Patients can be offered pouch formation if they have PSC as long as they understand the potential implications.
3.13.4 Fertility and delivery after restorative proctocolectomy
Good Practice Recommendation 4. For females requiring emergency subtotal colectomy and ileostomy, decisions regarding proctectomy and ileoanal pouch reconstruction should be discussed because of the potential for impaired fertility. Decisions should be personalised, including use of laparoscopic techniques and the option of delaying until after completion of the family (Agreement: 100%).
Any pelvic surgery incurs a risk to fertility. Whereas there is evidence that medical treatment of UC does not impair female fertility,285 a retrospective systematic review and meta-analysis of fertility rates 1 year after open IPAA surgery showed 63% infertility with a relative risk of 3.91 associated with the surgery,286 corroborating an earlier meta-analysis showing an infertility rate of 15% for medically-treated UC and 48% after IPAA.287 Time to conception is longer post-surgery, with a more frequent necessity of in vitro fertilisation and higher incidence of caesarean section.288 It is likely that Fallopian tube scarring in relation to the procedure is the cause of infertility.286 In selected female patients without proctitis, subtotal colectomy with ileorectal anastomosis (IRA) may be preferable as this does not impair fertility,289 although this procedure is not suitable for all and the long-term risk of rectal malignancy remains following IRA. There is evidence that pelvic scarring is much reduced when IPAA is performed laparoscopically.290 Consistent with this, time to first spontaneous pregnancy following IPAA is shorter in those undergoing laparoscopic surgery in comparison to open procedures.291 In a retrospective questionnaire-based study comparing fertility in 15 women following laparoscopic IPAA to that in a control group having appendectomy, infertility was demonstrated in 27% which was no different to the control group,292 suggesting that laparoscopic restorative proctocolectomy may be the preferred option for female patients of reproductive age.
3.14 Pouches and pouchitis
3.14.1 Assessment of new symptoms after IPAA
Good Practice Recommendation 5. Patients with ongoing symptoms after pouch surgery should have pelvic MRI scan, stool culture and Clostridium difficile assay. Pouchoscopy should be performed to assess the pouch, the pre-pouch ileum and the mucosa at the anal transition zone (Agreement: 100%).
Up to 50% of patients will develop pouchitis at some time after IPAA (as many as 40% in the first year). Typical symptoms of pouchitis include increased bowel frequency, urgency, nocturnal seepage or incontinence, pelvic discomfort and abdominal cramps (table 6).293 Diagnosis is based on the presence of symptoms in conjunction with endoscopic appearance and histology to rule out other conditions. Patients who develop symptoms may not have pouchitis: post-surgical complications should be considered particularly within the first year after surgery.294 This can be due to fistula development, pelvic sepsis and anatomical problems related to pouch construction (for instance, long cuffs with flutter valve effects or mechanical causes of poor pouch emptying). A study in 68 patients with antibiotic-dependent or refractory primary idiopathic pouchitis, who had had both pouchoscopy and pelvic MRI, showed that 38% had chronic peri-pouch sepsis. Those with sepsis more often had inflammation in the upper pouch only, and although some had a collection that could be drained radiologically, outcomes were poor with most remaining on long-term antibiotics and nearly a third having a defunctioning stoma or pouch excision.293 In patients with chronic pouchitis 20%–30% have secondary causes for their symptoms, which include CMV infection, Candida, Clostridium difficile, 295 ischaemia, autoimmune disorder, or damage from radiotherapy, chemotherapy or non-steroidal anti-inflammatory drugs.180 296 A proportion may have Crohn’s disease, with reported frequency ranging from 3.6%–13%.297
Pouchitis Disease Activity Index1284
Endoscopy is the main tool in the diagnosis and differential diagnosis of pouchitis. The most commonly used clinical scores for pouchitis evaluation are the Pouchitis Disease Activity Index (based on symptoms, endoscopy and histology (table 6) and the simpler Modified Pouchitis Disease Activity Index (symptoms and endoscopy only).298 299 In both, endoscopy is key. Pouchoscopy may be best carried out using a gastroscope in view of the flexibility and smaller calibre of this compared with a colonoscope, and a digital examination adds valuable information. At the time of pouchoscopy it is important to assess the pre-pouch ileum as well as the pouch itself, the rectal cuff and anal transition zone (to look for cuffitis). Morphological changes of oedema, loss of vascular pattern, erythema, haemorrhage, erosions/ulceration should be looked for. Ulcers in the afferent loop may indicate Crohn’s disease or use of NSAIDs. Inflammation in one half of the pouch with sharp demarcation along the suture line may suggest ischaemia. Staple-line ulcers with normal pouch mucosa elsewhere are common and do not suggest pouchitis.296 300 Other investigations include pelvic MRI to rule out collections, fistulae or anatomical abnormalities; stool cultures and C. difficile toxin and celiac serology.
3.14.2 Treatment of acute pouchitis
Statement 23. We recommend that a 2 week course of ciprofloxacin or metronidazole is the first-line treatment of acute pouchitis (GRADE: strong recommendation, low-quality evidence). We suggest that ciprofloxacin is better tolerated and may be more effective than metronidazole (GRADE: weak recommendation, low-quality evidence. Agreement: 97.2%).
Antibiotic therapy is the standard treatment for acute pouchitis,301 with observational data demonstrating 96% of patients have a symptomatic response to antibiotics.302 There is very little evidence comparing different antibiotics. However, one small study of 16 patients demonstrated that ciprofloxacin was superior to metronidazole in the treatment of acute pouchitis.303 Ciprofloxacin is better tolerated with fewer adverse effects than metronidazole and may therefore be considered first line treatment for acute pouchitis.304
There is one trial of probiotics in primary prevention of pouchitis. Forty patients were randomised to a specific probiotic mixture containing eight bacterial strains, or placebo.305 Ten percent of the probiotic treated arm developed pouchitis in a year compared with 40% of the placebo-treated group. An uncontrolled retrospective study reported primary prophylaxis with sulphasalazine 2 g. At a median 68 months, pouchitis occurred in 15% on sulphasalazine, compared with 64.5% not given the drug.306
There are more studies examining secondary prevention of pouchitis. Two trials show benefit for a probiotic mixture of eight bacterial strains given after a 1 month course of antibiotics for patients with chronic relapsing pouchitis.307 308 An open-label study of a probiotic mixture in 28 patients without symptoms, (36% had previous pouchitis but none had symptoms at study entry) designed to evaluate immunological changes in the pouch, showed progressive improvement in PDAI scores over 1 year, and expansion of mucosal regulatory T cells, compared with patients on no treatment.309 A small study of Lactobacillus rhamnosus GG over 3 months (in patients with previous pouchitis, and with endoscopic pouch inflammation, but no symptoms) showed no benefit.310 Overall trial quality in these studies was low, and further trials would be helpful to clarify management.304 311 Probiotic therapy can be recommended for prevention of relapsing pouchitis, but there is insufficient evidence to recommend primary prophylactic probiotics after pouch surgery, or even whether this should be given to those at higher risk of pouchitis, such as those with pre-operative extra-intestinal manifestations, primary sclerosing cholangitis or high titres of p-ANCA.312 313 Recent studies have shown that alterations in pre-colectomy bacterial microbiota are predictive of subsequent pouchitis, with increases in Ruminococcus gnavus, Bacteroides vulgatus, Clostridium perfringens, and absence of Lachnospiraceae genera (Blautia and Roseburia) and this may inform future treatment strategies.314 A small open-label study of faecal microbial transplantation (FMT), (single treatment via nasogastric tube) in 10 patients with chronic pouchitis did not show obvious clinical benefit.315
FMT can be used to treat Clostridium difficile infection in the context of ulcerative colitis when first line antibiotics are ineffective.316 There is currently no place for FMT in the management of IBD unless complicated by C. difficile infection outside of the clinical trial setting.
Anti-diarrhoeal drugs are often used by patients with IPAA to reduce bowel frequency. There is no evidence of benefit in pouchitis treatment although they are often continued. More evidence is required to support this common practice.
3.14.3 Treatment of chronic pouchitis
Statement 24. We suggest that chronic pouchitis may be treated with a combination of antibiotics (ciprofloxacin, metronidazole, tinidazole, rifaximin), oral budesonide or oral beclomethasone (GRADE: weak recommendation, very low-quality evidence. Agreement: 85.7%).
Chronic pouchitis or chronic refractory pouchitis is defined as occurring when patients with pouchitis remain symptomatic despite 4 weeks’ treatment with antibiotics. Patients who fail to respond to 2 weeks of an antibiotic, or relapse rapidly after stopping, can be treated with a combination of antibiotics for 4 weeks. Ciprofloxacin plus rifaximin and ciprofloxacin plus tinidazole have been shown to be effective in randomised controlled trials.301 Oral budesonide 9 mg and oral beclomethasone dipropionate 10 mg daily given for 8 weeks have also been shown to be effective,317 318 and if symptoms worsen on stopping, biologics should be considered rather than continuing long-term steroids. Some antibiotic-dependent patients may require long-term rotating antibiotic therapy, and coliform sensitivity testing may help to choose appropriate agents.319 Patients with pre-pouch ileitis (occurring in 6% of patients with pouchitis) represent a high-risk group for chronic refractory pouchitis and should be considered for early escalation to immunomodulatory therapy.320
3.14.4 Treatment with biologics in chronic refractory pouchitis
Statement 25. Chronic refractory pouchitis not responding to antibiotics or locally-acting corticosteroids should be reassessed to consider other factors, and if excluded, we suggest that patients may be offered biologics (GRADE: weak recommendation, low-quality evidence. Agreement: 90.9%).
Patients developing chronic treatment-refractory pouchitis should be re-evaluated to exclude other causes (see above). A recent systematic review with meta-analysis of the literature regarding the use of anti-TNF therapy for patients with chronic refractory pouchitis has shown moderate to good benefit in eight case series for infliximab and adalimumab therapy with a pooled remission rate of 53%.301 A preliminary report of a small double-blind randomised trial of adalimumab for chronic refractory pouchitis showed that six patients on adalimumab all improved, with only two of seven on placebo improving. The study was too small for statistical significance.321 A series of 20 patients with chronic antibiotic-dependent, or refractory pouchitis showed benefit with vedolizumab therapy. Assessed at 14 weeks, PDAI and Oresland scores improved with 17/19 patients able to stop antibiotic therapy.322 A small open-label study of 10 patients using tacrolimus enemas (0.08 mg/kg) showed response in nine, and remission in seven.323
3.14.5 Follow-up of pouch patients
Good Practice Recommendation 6. Ileoanal pouch patients should have long-term specialist follow-up where there is sufficient expertise to deal with complications, and collect long-term outcome data. Rapid access for diagnosis and treatment of suspected pouchitis should be available (Agreement: 100%).
Ulcerative colitis patients who have undergone ileoanal pouch anastomosis represent a small group of patients, who have undergone a specialised procedure with a 5%–10% chance of long-term failure and significant risk of complications,324 of which pouchitis is the most frequent. A pouch clinic enhances patient satisfaction,325 and facilitates data collection for audit and research purposes. Participation in a national pouch registry is invaluable for this purpose.326
3.14.6 Pouch surveillance
Statement 26. Restorative proctocolectomy with an IPAA does not completely abolish the risk of neoplasia. We suggest that patients with high-risk factors may be offered surveillance pouchoscopy although it is unclear how frequently this should be performed. Low-risk patients do not require surveillance (GRADE: weak recommendation, very low-quality evidence. Agreement: 94.4%)
The risk of neoplasia in pouches is extremely small, with a risk of cancer less than 0.02% at 20 years.327 328 Cancer may arise following pouch surgery within the rectal cuff, within the pouch itself or arise from the skin (squamous cell carcinoma).329 Risk of pouch-associated neoplasia is elevated in patients with a diagnosis of IBD-associated cancer,330 family history of colorectal cancer, type C ileal changes (severe pouchitis rapidly after pouch formation, with moderate to severe villous atrophy), long retained rectal cuff, and primary sclerosing cholangitis.331 Although controversial, annual pouchoscopy is recommended by most commentators for these high-risk patient groups.332 333 The indications for pouch surveillance in the asymptomatic population without the above risk factors is uncertain,328 although abnormal endoscopic findings are not uncommon.334 335 A decision in this low-risk group to either perform no surveillance unless symptomatic, or 5-yearly, should be discussed with the patient, and documented. Examinations should be performed by an experienced endoscopist.
4 Crohn’s disease
4.1 Diagnosis, classification and assessment
Crohn’s disease is a complex chronic inflammatory gastrointestinal condition with variable age of onset, disease location and behaviour. There is no single unifying definition of Crohn’s disease and a combination of investigative modalities is often needed to confirm the diagnosis. The most widely accepted framework for making a diagnosis dates back nearly 30 years.336 Factors include an appropriate clinical history and examination, ileocolonoscopy, small bowel imaging, blood tests and histology. Mucosal biopsies from endoscopic procedures or surgical resection specimens show focal or patchy (rather than diffuse) inflammation and/or crypt distortion. Discontinuous segments of disease (‘skip lesions’), ileal involvement and granulomatous inflammation are more suggestive of Crohn’s disease, as is a tendency for inflammation to be worse in the proximal colon.14
Distinguishing between Crohn’s disease and UC can sometimes be complicated; partially-treated UC can demonstrate patches of inflammation, backwash ileitis occurs in UC, and granulomas only occur in about half of Crohn’s disease patients. Cryptolytic granulomas can occur in UC, diverticular inflammation and all forms of colitis and are very non-specific. Pathologists find it easier to distinguish between IBD and non-IBD than they do to separate Crohn’s from UC, and the diagnosis is helped greatly by discussion at a multidisciplinary team meeting with clinicians and pathologist present.14 Studies have shown about 3% of UC patients will be reclassified as Crohn’s colitis, and conversely a small number (0.6–3%) will be reclassified to UC after an initial diagnosis of Crohn’s disease.19 21 There is a separate cohort who can be neither assigned as Crohn’s disease or UC, so are labelled as IBD unclassified.
4.1.1 Phenotypic classification
The Montreal classification29 is widely used to classify the key phenotypic features of patients with Crohn’s disease.22 In order to capture the change in disease location and behaviour over time, and growth failure in the paediatric IBD phenotype, the Paris classification was developed as a modification of Montreal (table 7).23 337 338 Using these classification systems in clinical practice is useful to ensure appropriate decision-making regarding surgery, medical treatment and surveillance. Montreal and Paris define disease extent according to endoscopic or macroscopic features. With an increasing emphasis on mucosal healing as a therapeutic target, it is important to note that histological evidence of inflammation may be more extensive than macroscopic features. This has been shown in paediatric studies, where inclusion of histological inflammation increases those classified with ileal involvement from 49% to 71.3%, those classified with Paris L3 disease increases by 10%, those with Paris L3+L4a by 24% and those with Paris L4 disease by 27%.339–341 A further approach to classifying disease relates to defining early disease: there is evidence that early treatment with biologics is more effective and an international consensus has proposed a Paris Definition for Early Crohn’s Disease, defined as disease duration of 18 months or less after diagnosis without previous exposure to immunomodulators and/or biologics.337
Montreal and Paris classification in Crohn’s disease
4.1.2 Clinical and endoscopic disease activity
The Crohn’s disease activity index (CDAI)342 has in the past been used in clinical trials,343 but it has a number of limitations, including the parameters used to define remission (CDAI <150), and contemporary trial design no longer favours use of CDAI.344 In clinical practice, CDAI is cumbersome to calculate, requires diary data from patients, is weighted towards diarrhoea (which is often caused by factors other than inflammation), is not usable in patients with stomas and is not validated for use after surgery. In contrast, the Harvey Bradshaw Index (HBI) is both simple to calculate and measure, and less susceptible to confounding factors relying on clinical parameters only, yet is heavily weighted by diarrhoea.345 An HBI score ≤4 is often used to define clinical remission. There is also value in monitoring patient-reported outcome measures (PROMs), reflecting the overall impact of disease on the individual.346 The IBD-Control PROM is an easy to use, reliable 8-item measure which correlates well with other quality of life measures347 and should be used to monitor patients’ perspective of their disease. It should be noted that neither HBI nor PROMs measures correlate well with objective markers of inflammation in Crohn’s disease,348 as subjective factors including psychological status impact significantly on patient-reported well-being. These measures are thus complementary to objective measures of disease activity obtained at endoscopy, imaging and surrogate measures including faecal calprotectin. More objective measures of disease impact including the Lemann index349 and endoscopic inflammation scores are more useful as treatment targets in clinical trials,350 and may drive therapeutic decision-making in clinical practice.
There are a number of endoscopic scoring systems which are used regularly in clinical trials351 352 although the two most commonly used are the Crohn’s Disease Endoscopic Index of Severity (CDEIS)353 and the Simplified Endoscopic activity Score for Crohn’s disease (SES-CD; table 8).354 While the CDEIS is complex to calculate, the SES-CD is a simple, reproducible and reliable endoscopic score.355 356 Both are used to assess for complete mucosal healing as an end-point in clinical trials. Although not used extensively in routine clinical practice, the SES-CD does systematise recording of features in each segment of the colon. Validated MRI activity scores are increasingly used as adjunct end-points in clinical trials.357 358 The Rutgeerts score (table 9) is used specifically to assess recurrent disease in the neo-terminal ileum after surgery.359
Simple Endoscopic Score for Crohn’s disease (SES-CD)354
Endoscopic evaluation of postoperative Crohn’s disease recurrence at ileocolic anastomosis: Rutgeerts score359
In clinical practice there is evidence that treatment escalation and de-escalation driven by objective markers of inflammation that are surrogates for endoscopy (CRP, faecal calprotectin), as well as clinical variables, can result in improved endoscopic and quality of life outcomes, at least in the short term.360 361 (The CALM trial is discussed further in the Section on Use of faecal calprotectin to inform therapy changes 5.5.1.2). It seems likely that this will translate into long-term benefit, but as yet there is no widely agreed treatment target in Crohn’s disease. As safer and more powerful therapies become available, it may be appropriate and feasible to use targets based on these objective measures in routine practice, in addition to clinical symptoms, to ensure effective control of the disease on a long-term basis. The choice of surrogate measure (such as faecal calprotectin), endoscopy, cross-sectional imaging or combinations of these at intervals may differ between patients, depending on their disease distribution, severity and their personal preference.
4.1.3 Diagnostic tests
Good Practice Recommendation 7. Suspected Crohn’s disease should be investigated with ileocolonoscopy including segmental colonic and ileal biopsies (to look for microscopic disease); and with imaging to assess location and extent of small bowel disease (Agreement: 97.8%).
Ileocolonoscopy with biopsy is established as the first-line investigation for suspected Crohn’s disease. Ileoscopy with biopsy histology is superior in establishing the diagnosis of mild ileal Crohn’s disease, however, intubation of the terminal ileum may not always be possible, and up to 20% of patients have isolated proximal small bowel disease beyond the reach of even complete ileocolonoscopy. For example, out of a cohort of 150 Crohn’s disease patients, 36 had active small bowel disease diagnosed using CT enterography following a normal ileocolonoscopy.362 Ileoscopy and radiological imaging are complementary in diagnosis of ileal Crohn’s disease.363 364 Dedicated small bowel imaging should be performed to complement ileocolonoscopy in all patients with suspected Crohn’s disease and those with an unclassified colitis at ileocolonoscopy. Mucosal biopsy specimens are essential for a complete macroscopic and microscopic assessment of the colon and distal ileum.9 365
Statement 27. We suggest that adult patients with Crohn’s disease do not routinely require upper gastrointestinal endoscopy as part of the diagnostic evaluation unless they have upper gastrointestinal symptoms (GRADE: weak recommendation, very low-quality evidence. Agreement: 91.1%).
Crohn’s disease in the upper gastrointestinal tract has a prevalence up to 13% in some studies,366 and 16% in a more recent study of 119 patients.367 When found, it is usually accompanied by ileal or colonic disease.368 It has been suggested that upper GI endoscopy can help to differentiate between UC and Crohn’s disease in patients with an unclassified colitis. Changes of focal gastritis occur, however, in UC as well as Crohn’s disease,369 and so gastroscopy may not be helpful. If there is vomiting, dyspepsia or other upper GI symptoms then upper GI endoscopy is indicated, but not routinely in adults with suspected or proven Crohn’s disease.
4.1.3.1 Cross-sectional imaging: CT, MR and small bowel ultrasound
Statement 28. We suggest that cross-sectional imaging, specifically MRI, CT and ultrasound, have largely replaced conventional barium fluoroscopic and nuclear medicine techniques and have the advantage of evaluating both luminal and extraluminal disease. Emphasis should be placed on MR enterography and ultrasound as they do not expose patients to ionising radiation (GRADE: weak recommendation, moderate-quality evidence. Agreement: 97.9%).
Luminal barium fluoroscopic techniques have been the mainstay of radiological imaging for many years and have reasonable diagnostic accuracy for Crohn’s disease.370 They have largely been replaced by cross-sectional imaging techniques which also provide information about the bowel wall and extra-enteric soft tissues, and thereby can better classify disease phenotype and behaviour. It is necessary to distend the bowel prior to CT or MRI using intraluminal contrast agents,371 with little data supporting invasive enteroclysis techniques over standard enterography,372 which is better tolerated by patients. Ultrasound can be performed without or with bowel distension using oral contrast agents. Several meta-analyses show no consistent difference in accuracy for Crohn’s disease diagnosis between CT enterography (CTE), MR enterography (MRE) or small bowel ultrasound (SBUS),373–377 with sensitivity and specificity in the region of 85–95%. However, a recent UK multicentre trial of 284 newly diagnosed or suspected relapse Crohn’s disease patients showed that MRE had greater sensitivity for small bowel disease extent (presence and location) compared with SBUS (80% vs 70% respectively).378 MRE also had greater specificity than SBUS (95% vs 81% respectively), although SBUS had superior sensitivity to MRE for colonic disease presence in newly diagnosed patients (67% vs 47% respectively). Diagnostic accuracy for abscess, fistulae and stenosis is also largely equivalent between techniques.376
4.1.3.2 Detection of active disease
Accuracy for detecting patients with active disease is generally reported to be over 85%,376 379 although the data supporting SBUS is currently less consistent than for MRE and CT enterography380 and multicentre trial data suggest MRE is significantly more sensitive than SBUS for detecting active small bowel disease (96% vs 90% respectively).378 Radiological signs of disease activity include increases in bowel wall thickness and vascularity, contrast enhancement, T2 and diffusion weighted imaging signal (for MRE), and identification of ulceration and acute extraluminal complications.376 Validated and reproducible disease activity scores have been developed for MRE.358 381 Intravenous contrast-enhanced small bowel ultrasound shows promise382 but there is as yet insufficient data to recommend first-line use.
4.1.3.3 Investigation of strictures
Statement 29. We suggest that, while there is no clear evidence of diagnostic superiority for one cross-sectional imaging modality over another for stricture diagnosis, emphasis should be placed on techniques that do not expose patients to ionising radiation. For colonic or anastomotic strictures, endoscopy and biopsy should be performed to assess and exclude cancer, provided the stricture is accessible and endoscopy deemed safe (GRADE: weak recommendation, very low-quality evidence. Agreement: 100%).
Data supporting the use of imaging to quantify fibrosis are limited383 and the topic is under active investigation, with novel MRI magnetisation transfer sequences,384 delayed contrast enhancement,385 contrast enhanced ultrasound386 and ultrasound elastography387 all showing promise. Ultrasound detection of strictures may be improved by oral contrast.377
Compared with an age-matched population, Crohn’s disease patients have a 2–3-fold increased incidence of colorectal cancer, while the risk of small bowel malignancy is increased between 18 and 27 times.388 389 Up to 3.5% of Crohn’s disease strictures may be complicated by dysplasia or malignancy390 so endoscopic biopsy of accessible strictures should be performed to achieve a pathological diagnosis.
4.1.3.4 Radiation exposure
Diagnostic imaging, particularly CT scanning, can expose Crohn’s disease patients to doses of ionising radiation which may significantly increase their lifetime risk of cancer.391–393 This risk is particularly important for children and young people.394 Crohn’s disease patients have more than twice the radiation exposure compared with UC patients.395 A study of 409 patients from a tertiary hospital showed that 15.5% had a cumulative exposure dose in excess of 75 mSv392 (this dose is considered to increase the risk of cancer mortality by 7.3%). Factors associated with excessive diagnostic radiation exposure included age under 17 at diagnosis, upper gastrointestinal disease location, penetrating disease, need for intravenous corticosteroids and more than one Crohn’s disease surgical operation. Although significant dose reductions are now possible with emerging CT image reconstruction techniques,396 397 MRE and small bowel ultrasound are generally preferred over CT to limit patient exposure to ionising radiation.
4.1.3.5 Capsule endoscopy
Statement 30. We suggest that capsule endoscopy has greater sensitivity for mucosal small bowel Crohn’s disease than radiological imaging techniques and can generally be performed where inflammatory small bowel disease is still suspected despite normal or equivocal cross-sectional imaging. Minor changes found at capsule endoscopy may be insufficient in isolation to diagnose Crohn’s disease, particularly with recent NSAID use (GRADE: weak recommendation, moderate-quality evidence. Agreement 90.9%).
Capsule endoscopy provides high resolution endoluminal images of the small bowel, is less invasive than conventional endoscopic techniques and is usually well tolerated by patients.398 Although recent randomised trial data suggest a clear fluid preparation may be sufficient, marginally outperforming active bowel preparation,399 patients are commonly given bowel preparation.400 A recent European expert technical review assessing available meta-analysis data recommends the use of PEG bowel preparation to improve visualisation, but notes inconclusive evidence on the impact of preparation on completion rates and diagnostic yield.401 The same technical review also recommends use of an anti-foaming agent prior to capsule ingestion to improve visualisation.401
Evaluating diagnostic accuracy of capsule endoscopy is hampered by a lack of reference standard and many studies instead report the ‘diagnostic yield’. In this regard, meta-analysis data suggest the diagnostic yield of capsule endoscopy in suspected Crohn’s disease is significantly greater than barium fluoroscopy (52% vs 16%), CT enterography (68% vs 21%) and ileocolonoscopy (47% vs 25%).381 In established Crohn’s disease it was significantly greater than push enteroscopy (66% vs 9%), barium fluoroscopy (71% vs 36%) and CT enterography (71% vs 39%).402 Data suggest capsule endoscopy is superior to MRE at detecting small bowel inflammation in Crohn’s disease, particularly for proximal or superficial small bowel lesions,370 although a recent meta-analysis did not find any statistically significant difference in diagnostic yield between MRE and capsule endoscopy.370
The utility of diagnostic yield as a surrogate for diagnostic accuracy has been criticised403 with specificity for capsule endoscopy reported as 53% in one study, using a consensus reference standard paradigm.404 Minor mucosal abnormalities found at capsule endoscopy can be seen in normal individuals, particularly those who have been using NSAIDs,398 405 and while validated diagnostic criteria for capsule endoscopy diagnosis of Crohn’s disease are in development, they are not currently in widespread clinical use.398 405
Use of capsule endoscopy should therefore be restricted to those with a high clinical suspicion of Crohn’s disease (suggestive clinical picture and raised faecal calprotectin) and abstinence from NSAID ingestion for at least 1 month,405 where cross-sectional imaging has been normal or equivocal.
Statement 31. The risk of capsule retention is low in suspected Crohn’s disease patients without symptoms suggestive of stricture. However, when obstructive symptoms are present, or in known stricturing Crohn’s disease where capsule endoscopy is indicated, we suggest that patency capsule should precede capsule endoscopy (GRADE: weak recommendation, low-quality evidence. Agreement: 93.5%).
The size and rigidity of capsules used for capsule endoscopy mean they can be retained within the small bowel, usually in stricturing disease. The risk of capsule retention is lower in patients with suspected Crohn’s disease than in those with established disease. In a 2017 meta-analysis the risk of capsule retention in suspected Crohn’s disease (nine studies, 968 patients) was 3.6% (95% CI 1.7% to 8.6%), although there was considerable heterogeneity between included studies.406 In established Crohn’s disease (11 studies, 558 patients), the risk of capsule retention was 8.2% (95% CI 6% to 11%).406 Retention after successful patency capsule passage or exclusion of strictures by cross-sectional imaging was 2.7% (95% CI 1.1 to 6.4). Comparative data regarding cross-sectional imaging and patency capsule is limited.401 When capsule endoscopy is indicated in patients with known stricturing Crohn’s disease or those with suspected strictures, including patients presenting with abdominal pain or distention, nausea or vomiting, or a history of small bowel resection, abdominal/pelvic radiation exposure or chronic NSAID use, the use of preceding patency capsule is suggested.401 405 407
4.1.3.6 Balloon-assisted enteroscopy
Device-assisted endoscopy such as balloon-assisted enteroscopy can visualise the small bowel mucosa beyond the reach of ileocolonoscopy, allowing tissue biopsy for histological assessment. The diagnostic yield may be similar to capsule endoscopy, with a recent systematic review reporting a yield of 63.4% (95% CI 42% to 82.3%) in known or suspected Crohn’s disease,408 with likely greater sensitivity than MRE.409 The procedures are however costly, invasive, requiring deep sedation or general anaesthesia, and not without risk. A recent meta-analysis410 reported a perforation rate of 0.15% (95% CI 0.05% to 0.45%) for diagnostic balloon-assisted enteroscopy, and an overall major complication rate (including perforation and bleeding) of 0.72% (95% CI 0.56% to 0.90%) has been reported.408 Given the high diagnostic accuracy of alternative less invasive tests, notably cross-sectional imaging and capsule endoscopy, diagnostic device-assisted techniques should be reserved for patients with high clinical suspicion of Crohn’s disease despite negative ileocolonoscopy, who have suspicious but not diagnostic cross-sectional imaging or capsule endoscopy, particularly if findings would alter therapeutic strategy, or in patients where a firm histological diagnosis would alter management.405 Device-assisted enteroscopy does have a role in established Crohn’s disease where therapeutic intervention, such as stricture dilatation, is needed.411
4.2 Induction of remission in mild to moderate disease ileocolonic disease
4.2.1 Budesonide in ileocaecal Crohn’s disease
Statement 32. We recommend that mild to moderate ileocaecal Crohn’s disease can be treated with ileal-release budesonide 9 mg once daily for 8 weeks to induce remission (GRADE: strong recommendation, high-quality evidence. Agreement: 100%).
In a randomised double-blind trial, ileal-release budesonide 9 mg once daily for 8 weeks was as effective as prednisolone (40 mg daily tapering to 5 mg at 8 weeks) at inducing remission in patients with mild-to-moderate ileocaecal Crohn’s disease with treatment efficacy (CDAI score <150) of 51% on budesonide at 8 weeks compared with 52.5% for prednisolone,412 and significantly fewer side effects. Multiple meta-analyses have also demonstrated the efficacy of budesonide 9 mg/day over placebo in inducing remission.413–415 A once-daily 9 mg dose is as effective as 3 mg three times daily.416 In the context of more severe disease (CDAI >300) budesonide is inferior to prednisolone (RR 0.52, 95% CI 0.28 to 0.95).414 When remission has been achieved, budesonide should be tapered over 1–2 weeks.
4.2.2 Corticosteroids in colonic Crohn’s disease
Statement 33. We recommend that active Crohn’s colitis can be treated with an 8-week course of systemic corticosteroids to induce remission (GRADE: strong recommendation, high-quality evidence. Agreement: 100%).
In mild, moderate and severe colonic Crohn’s disease, systemic corticosteroids such as prednisolone are effective in inducing remission.417–419 A starting dose of 40 mg tapering by 5 mg weekly is often used, but should be tailored to disease severity and patient tolerance. Ileal-release budesonide does have benefit in Crohn’s disease affecting the proximal colon,412 but there is no evidence of benefit in more distal colonic inflammation. There are no trials of colonic-release budesonide-MMX in Crohn’s disease at present.
4.2.3 Nutritional therapy
Statement 34. We suggest that Exclusive Enteral Nutrition (EEN) may be used to induce remission in mild to moderate Crohn’s disease patients where avoidance of corticosteroid is desired, and in those who are motivated to adhere strictly to EEN for up to 8 weeks (GRADE: weak recommendation, very low-quality evidence. Agreement: 86.4%).
Statement 35. We recommend that polymeric feeds are as effective as elemental or semi-elemental feeds in treatment of Crohn’s disease, and improve adherence (GRADE: strong recommendation, very low-quality evidence. Agreement: 86.7%).
4.2.3.1 Exclusive Enteral Nutrition (EEN)
Meta-analysis has shown that EEN is as effective as corticosteroids at inducing remission in 73% of paediatric patients on an intention to treat basis420 but not in adults.421 In paediatrics, it is considered the primary treatment option to induce disease remission,420 and has added value in that it not only improves nutritional status but also benefits growth. In adults, although studies have been small and underpowered, there does seem to be a consistent message that, where tolerated, EEN can be effective at inducing remission422–425 even in the presence of complications.426 There is increasing evidence that EEN can alter the microbiome, with differences in those who have a long-term response.427
Tips on the use of EEN are shown in box 3. In practice, EEN is not frequently used in adult populations. This is reportedly due to a lack of high-quality evidence for its use428 and limited access to dietetic expertise within an IBD multidisciplinary team (MDT).429 Where avoidance of corticosteroids is considered appropriate and patients are motivated to try dietary alternatives, EEN should be considered with appropriate dietetic support.421 429 430
Practical guide for Exclusive Enteral Nutrition (EEN) to induce remission in Crohn’s disease
Counsel patients on the risks and benefits of all available treatment options including EEN.
EEN is provided as a prescribed liquid diet excluding all food and drink except still water. Some units allow limited optional intake beyond this, but there is little evidence supporting what foods or drinks can be added without impacting efficacy. Permit Crusha flavouring (now sugar-free), Fox’s Glacier Mints, sugar-containing 7-Up and black coffee.
Whole protein, peptide or elemental diets are equally efficacious but whole protein feeds are more palatable and are more likely to be tolerated.
EEN is nutritionally complete with all relevant micronutrients and trace elements.
Limited palatability and tolerance are often reasons for failure, so encouragement from the whole MDT is important for success. This is best achieved with a formalised MDT pathway for EEN management and specific points of contact to assess progress.
A starter regimen, increasing the prescribed daily volume gradually over a few days while reducing food intake, is important to build up tolerance and prevent the risk of refeeding, especially in patients where dietary intake has been suboptimal beforehand or weight loss has been significant.
Bloods for refeeding syndrome include urea and electrolytes (for potassium), phosphate and magnesium, and should be monitored daily while calorie intake is increased to maximum in at-risk patients.
A standard target regimen should be based on requirements for energy: 25–30 kcal/kg/day and protein: 1 g/kg/day. Non-standard regimens may be used where refeeding syndrome is a risk (with lower calories), or where catch-up nutrition is required.
Once the target regimen is met, EEN should be continued for 6–8 weeks to induce mucosal healing.
Once EEN is established, the vast majority of patients can continue with their usual daily activities.
Most adult patients can tolerate EEN orally, however nasogastric feeding may be required if target volumes cannot be met orally or where feed tolerance is limited with boluses.
Regular monitoring via email or telephone will help to maintain adherence.
MDT, Multidisciplinary team.
Ten days of EEN can achieve symptomatic relief; however mucosal healing takes longer, up to 8 weeks.431–433 Further research is needed to identify the optimum duration, but 4–6 weeks of EEN is considered the minimum.429 434
EEN given as elemental diets are not palatable, therefore polymeric (whole protein) and semi-elemental (peptide) based feeds were created to overcome this barrier and have been shown to be as effective as elemental diets.435 EEN can be taken orally in the majority of patients, however the nasogastric route can be considered as an alternative where appropriate.436 A Cochrane review showed no difference in outcomes between elemental and non-elemental feeds, but evidence quality was very low.421
4.2.3.2 Elimination diets
There is much interest in elimination diets being used to induce or maintain disease remission. Following a course of EEN, patients can be unsure what foods to add back into their diet first. A low fat, low fibre, exclusion (LOFFLEX) diet was developed to provide a dietary intervention for 2–4 weeks based on a small number of foods unlikely to trigger symptoms (an exclusion diet) followed by gradual food reintroduction with a new food every few days. The LOFFLEX diet has been shown to maintain disease remission in 56% of patients at 2 years,437 but is not used widely. Another study in paediatrics used a 3-day rapid food reintroduction diet compared with a 5-week food reintroduction plan and showed similar relapse rates of almost 50% of patients at 12 months indicating that food can be reintroduced more quickly than traditionally thought.438 A variety of other diets have been proposed in this context, but they lack the backing of high-quality evidence.428 The recently reported Crohn’s disease treatment with eating (CD-TREAT) study explored the possibility of replicating EEN with solid foods.439 Both EEN and the experimental diet achieved similar microbiome effects in healthy volunteers and rats, as well as improved HLA-B27 rat ileitis histopathology scores. In addition, the same paper reported a non-blinded study of five children with relapsing Crohn’s disease in which the experimental diet achieved 3/5 remission and 4/5 response by weighted paediatric CDAI.439 This is an area that requires further investigation before it can be considered a standard therapy.
4.2.4 Antibiotic therapy
Trials of antibiotic therapy in Crohn’s disease have studied a wide range of antimicrobial agents. While a meta-analysis demonstrated efficacy for these pooled trials over placebo (RR for continued disease activity 0.85 (95% CI 0.73 to 0.99), p=0.03),440 there was such heterogeneity in the agents and dosing regimens used that it makes it difficult to draw meaningful conclusions.
The risk of adverse effects, particularly with prolonged or repeated courses, should also be taken into consideration. In this regard, rifaximin (a non-absorbed oral antibiotic), in an extended-intestinal release formulation has been shown in a large dose-ranging study to be effective, although at a higher dose than usually employed (800 mg BD). However, there was no dose-response, with numerical but not statistical difference to placebo for the 400 mg BD and 1200 mg BD dose.441 442 Rifaximin is unlicensed for this indication.
In a blinded randomised trial in 73 patients with paediatric Crohn’s disease, azithromycin 75 mg/kg 5 days per week for 4 weeks, then metronidazole 20 mg/kg/day for another 4 weeks, compared with metronidazole only for 8 weeks, showed a remission rate of 66% for azithromycin/metronidazole and 39% for metronidazole (p=0.025), although response rates were similar. In 12 patients failing metronidazole, 83% achieved remission on open-label azithromycin.443 There is continuing research interest in antibiotic therapy in Crohn’s disease treatment, but at present antibiotics should only be used in patients with disease complicated by infection (abscesses, bacterial overgrowth, Clostridium difficile) or perianal fistulising disease. Overall the efficacy for antibiotics as induction therapy in mild-moderate Crohn’s disease remains unproven.
The role of Mycobacterium avium subspecies paratuberculosis (MAP) has been debated for many years. A randomised placebo-controlled trial of 2 years therapy with clarithromycin, rifabutin and clofazimine in 213 patients with active Crohn’s disease, with a further year of follow-up, showed early benefit of antibiotics, but overall there was no significant difference in relapse rate during follow-up.444 There was debate about the dosage and formulation chosen, and the study design (with withdrawal of non-responders at week 16). A further phase 3 trial using higher doses was reported in October 2018.445 A total of 331 patients with moderate to severely active Crohn’s disease were randomised to RHB-104 (clarithromycin 95 mg, rifabutin 45 mg and clofazimine 10 mg) five capsules twice daily or placebo for 52 weeks, in addition to their pre-study therapy. At week 26, remission was achieved in 37% versus 23% on placebo (p=0.007), and durable remission (from week 16 to 52) was achieved in 18% versus 9% on placebo (p=0.019). No data are available on endoscopic healing or on persistence of benefit after stopping treatment.
4.2.5 Surgery in localised ileocaecal Crohn’s disease
Statement 36. We suggest that laparoscopic resection should be considered in localised ileocaecal Crohn’s disease for those failing or relapsing after initial medical therapy, or in those preferring surgery to continuation of drug therapy (GRADE: weak recommendation, moderate-quality evidence. Agreement: 93.5%).
The LIR!C study compared laparoscopic ileocaecal resection (n=73) to infliximab (n=70) for patients with terminal ileal disease in whom conventional therapy had failed.446 Across a number of comparators there was equivalence between the two approaches, suggesting that resection is a reasonable alternative to medical therapy in this scenario. The LIR!C trial excluded those who had previous resection, a small bowel segment longer than 40 cm, abscesses or where surgery was deemed likely due to pre-stenotic dilatation. During the median follow-up period of 4 years (range 2–6), approximately a third of patients (n=26, 39%) in the infliximab group required surgery while a quarter of patients in the surgery group (n=19, 26%) required infliximab. Taken together, these data suggest resection is a cost-effective intervention based on the cost of originator infliximab.447 Present day medical costs should be lower with the widespread availability of biosimilar infliximab.
4.3 Initial treatment of moderate to severe ileocolonic Crohn’s disease
4.3.1 Corticosteroids
Statement 37. We recommend that moderate to severely active uncomplicated luminal Crohn’s disease should be treated initially with systemic corticosteroids (GRADE: strong recommendation, high-quality evidence), but we suggest that those with extensive disease or other poor prognostic features should be considered for early introduction of biological therapy (GRADE: weak recommendation, moderate-quality evidence. Agreement: 86.7%).
Systemic corticosteroids are still an effective initial therapy for moderate to severely active Crohn’s disease,418 419 regardless of disease location, but every effort should be made to limit exposure.448 For less severe symptoms in those with ileocaecal disease location, ileal-release budesonide may be tried initially, but if ineffective, prednisolone may be required. For teenagers, particularly where growth has not completed, and for patients with diabetes or steroid intolerance, alternatives can be considered, including EEN.
4.3.2 Early use of biological therapy
In patients with an aggressive disease course or ‘high-risk’ poor prognostic factors, the early introduction of biologics may be considered. High-risk features include: complex (stricturing or penetrating) disease at presentation; perianal fistulising disease; age under 40 years at diagnosis; and need for steroids to control the index flare.449 450 The predictive power of these features is limited. There is great interest in biomarkers that identify a Crohn’s disease subgroup at high risk of an aggressive disease course. A gene expression signature from peripheral CD8 T cells in active untreated IBD has been identified,451 and is now being tested using a whole blood assay in randomised controlled trials of a ‘top-down’ versus accelerated ‘step-up’ therapy.
The decision to start biological therapy should also consider factors such as stage of life, work absence and availability of other treatment options. Discussion in a multidisciplinary team meeting can be helpful. As well as anti-TNF therapy, vedolizumab and ustekinumab can be considered as first-line biologics.
4.4 Maintenance treatment in ileocolonic Crohn’s disease
Statement 38. We recommend that systemic or locally acting corticosteroids should be avoided as maintenance therapy in Crohn’s disease due to toxicity and lack of efficacy (GRADE: strong recommendation, high-quality evidence. Agreement: 100%).
Irrespective of whether remission is induced surgically or medically, corticosteroids are not effective in maintaining remission in Crohn’s disease compared with placebo (see Section 5.2.8.1: Overuse of corticosteroids). Systematic reviews and pooled trial data show that budesonide does not reduce relapse rates over a 12-month period.452–454 One systematic review did show a modest reduction in CDAI scores, but this was outweighed by a significant increase in adverse events and adrenocortical suppression compared with the placebo groups.454
4.4.1 Immunomodulator therapy
Statement 39. We recommend that for patients with moderate to severe Crohn’s disease responding to prednisolone, early introduction of maintenance therapy with thiopurines (GRADE: strong recommendation, low-quality evidence) or methotrexate (GRADE: strong recommendation, moderate-quality evidence) should be considered to minimise risk of flare as prednisolone is withdrawn (Agreement: 93.3%).
Relapse of Crohn’s disease is common on corticosteroid withdrawal, particularly in moderate to severe disease, and early initiation of corticosteroid-sparing therapy is appropriate. Immunomodulators such as azathioprine, mercaptopurine or methotrexate are effective in the maintenance of remission of Crohn’s disease.
4.4.1.1 Thiopurine therapy
Statement 40. We recommend that azathioprine or mercaptopurine can be used as monotherapy in the maintenance of remission in Crohn’s disease (GRADE: strong recommendation, low-quality evidence. Agreement: 100%).
Thiopurines should not be used for induction of remission in active Crohn’s disease. Thiopurines are more effective than placebo in maintenance of remission in Crohn’s disease but the Cochrane analysis reports low quality evidence (NNT=9).455 A systematic review and network meta-analysis also showed the benefit of azathioprine/mercaptopurine compared with placebo in remission maintenance (OR 1.7 (95% CI 1.3 to 2.6)), although anti-TNF therapy was significantly more effective than thiopurines.456
4.4.1.2 Methotrexate
Statement 41. We suggest that methotrexate may be used for the maintenance of remission of Crohn’s disease, and the dose should be at least 15 mg weekly. Subcutaneous administration has better bioavailability than oral, particularly at higher doses (GRADE: weak recommendation, moderate-quality evidence. Agreement: 88.4%).
Methotrexate should not be used as monotherapy for induction of remission, but may be used in Crohn’s disease patients failing to respond to corticosteroids. The landmark trial evaluated intramuscular methotrexate 25 mg weekly given to patients with chronic active Crohn’s disease despite at least 3 months of prednisolone. It showed increased clinical remission rates compared with placebo at 16 weeks, with reduced prednisolone requirements.457 458
A follow-on study also showed efficacy of methotrexate as a maintenance therapy,459 a finding which has been confirmed in a recent Cochrane review.460 A network meta-analysis and systematic review showed the benefit of methotrexate with ORs of 2.4 (95% CI 1.1 to 4.8).456
In other disease areas there is convincing evidence of the superiority of parenteral administration of methotrexate over the oral route.461 462 As a result, a variety of studies have attempted to compare the efficacy of different routes of administration for methotrexate in Crohn’s disease. A retrospective cohort study of 118 patients showed benefit of methotrexate in both induction and maintenance treatment for Crohn’s disease, with steroid-free remission being achieved in 37.2% of patients, and maintained relapse-free in 63.6% for a median of 12 months.463 A multicentre retrospective study in 226 children showed numerical, but not statistical superiority of subcutaneous methotrexate over the oral route, with sustained corticosteroid-free remission in 32% for subcutaneous versus 26% for oral (OR 1.7, 95% CI 0.5 to 5.9).464 There was no difference in nausea or abnormal liver enzymes between the two routes of administration.
Oral methotrexate has reduced and extremely variable bioavailability (not corrected by use of folic acid) compared with parenteral administration, particularly at doses above 15 mg.465 466 Because bioavailability and pharmacokinetics are very similar for subcutaneous and intramuscular methotrexate, the subcutaneous route should be preferred to intramuscular as it is easier and less painful.467
Induction therapy should be given by the subcutaneous route. If patients prefer, this can be switched to oral during the maintenance phase, with the option to switch back to subcutaneous if effectiveness is lost. Whatever the route of administration, methotrexate should be given with folic acid to reduce gastrointestinal and liver toxicity, 5 mg weekly (traditionally 1–2 days after the methotrexate dose) or 1 mg daily.
4.4.2 Mesalazine
Statement 42. We recommend that mesalazine is not used for induction or maintenance of remission in Crohn’s disease (GRADE: strong recommendation, moderate-quality evidence. Agreement: 97.7%).
UK data from 1990 to 2010 show over half of patients with Crohn’s disease were prescribed 5-ASA,468 and Swiss data show it is more often given for Crohn’s colitis.469 A Cochrane systematic literature review showed that oral 5-ASA has no efficacy in maintaining clinical remission in Crohn’s disease,470 with similar negative findings in meta-analyses for induction or maintenance.413 414 471 472 A recent review of colonic Crohn’s disease473 showed that there was no benefit for 5-ASA in colonic Crohn’s disease, but two studies have shown possible benefit for sulphasalazine in remission induction.418 419 Thus, 5-ASAs are not recommended for induction or maintenance treatment of Crohn’s disease.
4.4.3 Biological therapy with anti-TNF drugs, vedolizumab or ustekinumab
Statement 43. We recommend that patients refractory to immunomodulator therapy despite dose optimisation should be considered for biological therapy. Choice between anti-TNF therapy, ustekinumab and vedolizumab should be made on an individual basis, considering patient preference, cost, likely adherence, safety data and speed of response to the drug (GRADE: strong recommendation, very low-quality evidence. Agreement: 95.7%).
4.4.3.1 Infliximab
Infliximab is a monoclonal antibody to tumour necrosis factor alpha (TNF) and was the first in class to be used in IBD, demonstrating definitive benefit in luminal Crohn’s disease in the ACCENT I study. 573 patients with active luminal disease received a single 5 mg/kg intravenous dose, and after assessment of response at week 2, were randomly assigned to infusions of placebo at weeks 2, 6 and then 8-weekly (group 1), or infliximab 5 mg/kg at the same time points, or 5 mg/kg at weeks 2 and 6, then 10 mg/kg 8-weekly. At week 2, 58% responded to the initial infusion, and of these responders: at week 30, 39% treated with 5 mg/kg maintenance and 45% on 10 mg/kg were in clinical remission, with similar remission rates observed at week 54.474 In routine clinical practice reported results are significantly better, with a large single-centre cohort of 614 Crohn’s disease patients (treated for luminal, perianal or extraintestinal manifestations) showing that 89.1% had clinical improvement after initial treatment and 63.4% showing sustained clinical benefit.475 This study included a significant proportion of patients receiving episodic therapy, whereas regular scheduled therapy is of proven superiority.476
4.4.3.1.1 Combination therapy of infliximab with an immunomodulator
Statement 44. We recommend that combination therapy of infliximab with a thiopurine should be used as it is more effective than monotherapy infliximab in induction and maintenance of remission in active Crohn’s disease (GRADE: strong recommendation, high-quality evidence. Agreement: 97.7%).
The SONIC study showed that combined infliximab and azathioprine was superior to infliximab in achieving clinical remission and mucosal healing.477 A network meta-analysis of published data shows that combination therapy was more effective than azathioprine monotherapy, as was adalimumab monotherapy.456 Similar benefits of combination therapy are seen in children.478 479 Addition of an immunosuppressant has also been shown to reduce the need for dose escalation of infliximab and also reduces the rate of drug switching.480
In the PANTS 3-year observational cohort of 1601 Crohn’s patients treated with infliximab or adalimumab, 751 patients were treated with infliximab.481 At week 54 the immunogenicity rates for Remicade and biosimilar infliximab (Inflectra/Remsima) were 26% and 28%, respectively. Immunomodulator use reduced the risk of immunogenicity in infliximab therapy (HR=0.37, p<0.0001).
Statement 45. We suggest that combination therapy of infliximab with methotrexate therapy may be used in Crohn’s disease to reduce immunogenicity (GRADE: weak recommendation, moderate-quality evidence. Agreement: 90.5%).
A study of patients who had recently started prednisolone treatment for active disease showed that combination therapy with infliximab and methotrexate was no more effective that infliximab monotherapy in maintaining remission up to 50 weeks, although equally safe.482 A recent Cochrane systematic literature review evaluating this460 and a further small open-label study483 reached the same conclusion. Immunogenicity to infliximab may, however, be reduced by the addition of methotrexate,480 suggesting that some clinical benefit might have been observed beyond the 1 year timeframe of the study. A paediatric registry study of 502 Crohn’s disease patients studied the impact of concomitant immunomodulator therapy on the duration of infliximab therapy.484 Concomitant methotrexate, taken for more than 6 months, increased likelihood of remaining on infliximab, both compared with non-use of immunomodulators and compared with thiopurine use. Due to the small number of girls given methotrexate, only boys were included in this analysis.
In order to maximise the benefit of infliximab therapy and reduce treatment failure, combination therapy with immunomodulator should always be preferred (with stronger evidence for azathioprine than methotrexate). For those intolerant to thiopurines and methotrexate, alternatives to infliximab should be used unless there are other compelling reasons (such as the presence of perianal disease).
4.4.3.2 Adalimumab
Adalimumab is a monoclonal antibody to TNF administered subcutaneously. The CLASSIC I study in moderate to severe Crohn’s disease naïve to anti-TNF therapy showed that the optimum dose for induction therapy was 160 mg followed by 80 mg at week 2, with remission (CDAI <150) achieved in 36% (p=0.001 against placebo) compared with 24% (80 mg/40 mg), 18% (40 mg/20 mg) and 12% on placebo.485 In the CHARM study of maintenance therapy, responders to induction therapy with 80 mg subcutaneously and 40 mg at 2 weeks were given placebo, 40 mg every 2 weeks or 40 mg weekly, with 12%, 36% and 41%, respectively, in clinical remission at week 56.486 The GAIN trial showed efficacy of adalimumab in patients with active Crohn’s disease and loss of response or intolerance to infliximab (secondary infliximab failures).487 Data from the EXTEND trial demonstrated adalimumab to be effective in inducing and maintaining endoscopic mucosal healing over the longer term,488 and with improved outcomes in those who achieved deep remission.489
The signal for the importance of combination therapy with an immunomodulator is not as strong in studies of adalimumab as it is for infliximab. A meta-analysis suggested that combination therapy with an immunomodulator was slightly better than adalimumab monotherapy for induction of remission, but remission rates at 1 year were no different, and there was no reduction in rates of dose escalation compared with monotherapy.490 Likewise, the DIAMOND trial comparing adalimumab monotherapy to combination therapy with azathioprine in 176 Japanese Crohn’s disease patients naïve to biologics and immunomodulators showed similar remission rates at weeks 26 and 52,491 and another study has shown efficacy of monotherapy with adalimumab in maintaining clinical remission for up to 4 years.492
A variety of studies on drug levels and immunogenicity have shown a difference between adalimumab monotherapy and combination treatment, with higher trough levels in patients on combination therapy with an immunomodulator,493 although clinical benefit was not shown. In the DIAMOND study there was a trend to higher trough drug levels and fewer antibodies against adalimumab with an improvement in endoscopic response at week 26, but not at 1 year.491 In another study higher trough levels were associated with endoscopic response and mucosal healing at 6 and 12 months.494 In the PANTS 3-year observational cohort of 1601 Crohn’s disease patients treated with infliximab or adalimumab, immunogenicity to adalimumab was present in 11% at 1 year and 23% at 3 years, and was associated with non-remission at week 5.481 Concomitant immunomodulator therapy reduced immunogenicity (HR 0.34, 95% CI 0.21 to 0.56, p=0.0001). Combination therapy was particularly beneficial in those patients with HLA-DQA1*05 who are more likely to develop antibodies against both adalimumab and infliximab.495 A study of UC and Crohn’s disease patients losing response to infliximab and adalimumab monotherapy showed anti-drug antibodies present in 61 (27%) of those on adalimumab. Of these, nine patients were given a thiopurine or methotrexate, with six responding with restored clinical response, improved drug levels and loss of antidrug antibodies.496 Although it has not been possible to demonstrate the clinical benefits of combination therapy for adalimumab in the way it has been for infliximab combination therapy, there is evidence that concomitant immunomodulator therapy reduces immunogenicity and increases trough levels, which may be clinically beneficial for longer-term adalimumab maintenance therapy.
4.4.3.3 Choice of anti-TNF agent in Crohn’s disease
There is little to choose between adalimumab and infliximab in efficacy in luminal Crohn’s disease, and practical considerations regarding mode and frequency of administration are the main factors as well as consideration of the relative need for combination therapy with an immunomodulator (see Section 5.2.4.1: Choice of anti-TNF agent). Certolizumab is not licensed for treatment of IBD in the UK and will not be discussed here.
4.4.3.4 Vedolizumab
Statement 46. We recommend that in Crohn’s disease, vedolizumab can be used in both anti-TNF naïve patients and in those where anti-TNF treatment fails. Choice of treatment in biologics-naïve patients should be individualised (GRADE for induction therapy: strong recommendation, moderate-quality evidence; GRADE for maintenance therapy: strong recommendation, high-quality evidence. Agreement: 95.5%).
Vedolizumab is a monoclonal antibody to the α4β7 integrin and blocks lymphocyte trafficking to the gut by blocking the binding of α4β7 to the mucosal addressin cell adhesion molecule-1 (MAdCAM-1). It has been demonstrated as effective in inducing remission in the GEMINI-2 trial.497 Of 967 patients entering the randomised induction (Cohort 1) and open-label induction (Cohort 2), 461 (47.7%) had a CDAI fall of 70 points and entered the randomised maintenance phase. Pooled data from the ITT population of the GEMINI-2 and the GEMINI-3 population (a 10-week induction study with dosing at weeks 0, 2 and 6) presents induction outcomes at weeks 6 and 10, split into 277 TNF-naïve and 490 TNF-failure patients.498 Response rates (CDAI fall of 100 points) were better at week 10 on vedolizumab, with TNF-naïve patients responding better (48.4% on vedolizumab vs 30.1% on placebo) compared with TNF-failure (39.7% on vedolizumab vs 22.5% on placebo). Remission rates at week 10 were also better for TNF-naïve patients (26.6% on vedolizumab vs 15.4% on placebo) compared with TNF-failure (21.8% on vedolizumab vs 11.0% on placebo). Among induction responders who were re-randomised to placebo or two different maintenance vedolizumab dosing strategies, at week 52 clinical remission was achieved in 39% of patients receiving 8-weekly infusions and 36.4% of patients receiving 4-weekly infusions compared with 21.6% of patients in the placebo group.
A systematic review has also demonstrated that vedolizumab was superior to placebo in induction and maintenance of remission in IBD and has an acceptable safety profile over the short term.499 Vedolizumab responders also appear to have persistence of benefit, with long-term follow-up data from the GEMINI-2 study showing that, of responders at week 6 for whom data were available, 83% were in remission after 2 years and 89% after 3 years.500 Observational studies have shown consistent findings—for example, a Scottish retrospective study of 153 patients had 1 year steroid-free remission of 28.6%.501 The Swedish SWIBREG study reported 147 patients with active Crohn’s disease (86% of whom had previously failed anti-TNF therapy) showed 1 year clinical remission of 54%.502 Recently reported real-world data suggest that higher rates of response with vedolizumab are more likely in patients with Crohn’s disease of ≤2 years duration in comparison to those with later stage disease >2 years.503 This study did not identify an association of response to vedolizumab with disease duration in UC.
In case of slow response to vedolizumab, prednisolone treatment can be maintained initially, or other immunomodulator therapy used or continued for 6–8 weeks, but as yet there are few data to support this practice.
There are currently no head-to-head comparative trials published of anti-TNF therapy versus anti-integrin therapy. Due to heterogeneity in trial design and patient characteristics, results of network meta-analyses comparing different agents should be treated with some caution, and are no substitute for head-to-head comparisons.504 Using propensity score matching, 269 patients with active Crohn’s disease in the VICTORY consortium were matched 1:1 with anti-TNF treated patients. At 1 year remission was observed in vedolizumab and anti-TNF treated patients in 38% and 34% respectively, HR 1.27 (95% CI 0.91 to 1.27), steroid-free remission in 26% and 18%, HR 1.75 (95% CI 0.90 to 3.43), endoscopic healing in 50% and 41% respectively, HR 1.67 (95% CI 1.13 to 2.47).505 Side effects of vedolizumab are discussed in the Section 5.2.5 Drug management: vedolizumab and ustekinumab. In biologics-naïve patients, anti-TNF therapy is currently likely to be an initial biologic choice, but there are situations where vedolizumab may be preferred (such as where there is an advantage of gut-specific immunosuppression, or use in older patients where infection and malignancy are a concern), but there are few data to support a clear benefit of anti-integrin therapy in any particular subgroup in Crohn’s disease as yet.
4.4.3.5 Ustekinumab
Statement 47. We recommend that ustekinumab can be used in the induction and maintenance of remission of Crohn’s disease, both in anti-TNF naïve patients and in those where anti-TNF treatment fails. No direct comparison data are available with other biological therapies (GRADE: strong recommendation, high-quality evidence. Agreement: 97.7%).
Ustekinumab is an anti-IL12/23 p40 antibody and has been evaluated in the UNITI and IM-UNITI studies in patients with Crohn’s disease. UNITI-1 enrolled patients who had prior anti-TNF failure (primary or secondary loss of response or intolerance). Clinical response at week 8 was 37.8% in those receiving ustekinumab 6 mg/kg (p<0.001 vs placebo), 33.5% with 130 mg (p=0.001 vs placebo) and 20.2% with placebo.506 UNITI-2 enrolled patients who had no previous failure with anti-TNF drugs (mostly anti-TNF naïve, but a small number with previous successful use of anti-TNF therapy). Clinical response at week 8 was 57.9% for 6 mg/kg, 47.4% for 130 mg and 32.1% for placebo (p<0.001 vs both doses). Responders from both studies at week 8 were randomised to the IM-UNITI maintenance arm. Of these randomised responders, 53.1% treated with 90 mg subcutaneously every 8 weeks (p=0.005 vs placebo), 48.8% given 90 mg subcutaneously 12-weekly (p=0.04 vs placebo) and 35.9% on placebo were in remission at 44 weeks. In total, 45% of those randomised to IM-UNITI were anti-TNF refractory. Of these, 41.1% were in remission at week 44 on ustekinumab 90 mg subcutaneously 8-weekly compared with 26.2% on placebo (p=0.10).
Efficacy has been demonstrated in a retrospective observational GETAID study of 122 Crohn’s disease patients refractory to anti-TNF drugs. 65% had clinical benefit within 3 months, and in 68% of these, benefit was maintained at 12 months.507 A growing real-world experience confirms the benefit of ustekinumab.508–512 Side effects of ustekinumab are discussed in the Section 4.9.5: Vedolizumab and ustekinumab therapy.
4.4.3.6 Choice of biological therapy after anti-TNF failure
Statement 48. We suggest that, where a switch from anti-TNF therapy to a different drug class is required in Crohn’s disease, the choice to use vedolizumab or ustekinumab may be made on an individual basis. Factors to be included in the decision-making process should include patient preference, cost, likely adherence, safety data and speed of response to the drug. The potential for surgery as an alternative to further drug therapy should also be considered (GRADE: weak recommendation, very low-quality evidence. Agreement: 97.8%).
To date there are no head-to-head studies comparing ustekinumab and vedolizumab in patients with IBD who have failed anti-TNF therapy, but indirect comparisons suggest no difference in efficacy in this relatively treatment-refractory group.513
A consistent theme across multiple clinical trials in Crohn’s disease is that response rates are generally lower in patients with a longer disease duration,514 515 or who have proven refractory to other therapies.506 Given the reduced likelihood of response to therapies in patients who have medically refractory but surgically tractable disease (eg, limited ileocaecal inflammation), surgical approaches should be actively considered to restore quality of life and reduce the risk of complications resulting either from prolonged uncontrolled inflammation or from the use of multiple drug therapies often interspersed with multiple courses of corticosteroid therapy.
4.4.3.7 Corticosteroid use and infection risk while on anti-TNF therapy
Statement 49. Patients with Crohn’s disease treated with a biological therapy in optimal dose who remain corticosteroid-dependent (particularly if on triple immunosuppression with immunomodulator therapy) are at significant risk of opportunistic infections. We recommend that alternative medical treatments or surgery should be explored (GRADE: strong recommendation, moderate-quality evidence. Agreement: 97.8%).
The observational Crohn’s Therapy, Resource, Evaluation, and Assessment Tool registry (TREAT) was established to compare infliximab safety with conventional non-biological therapy.516 Conventional immunomodulator therapies and anti-TNF therapies were associated with an increased risk of infection, including serious and opportunistic infections. Nonetheless the greatest risk of infection, and with it an associated increase in mortality, was seen in patients on corticosteroid therapy (see Section 5.2.1.2: Common Disease Considerations, Infection risk in patients on anti-TNF therapy). Requirement for continuous corticosteroid therapy or repeated short courses in patients on biologics suggests that treatment may be failing, and consideration should be given to switching to an alternative (see Section 5.2.4.6: Common Disease Considerations, Secondary loss of response to anti-TNF therapy) or considering other options, including surgery.
4.4.4 Haematopoietic stem cell transplantation
Despite the increasing range of drugs available, there are still a number of Crohn’s disease patients with severe resistant disease or in whom surgical resection is not appropriate (usually due to extensive disease or incipient short bowel syndrome). For this group of patients, autologous haematopoietic stem cell transplantation (HSTC) has been used. The ASTIC study, an RCT of autologous HSTC published in 2015, set a high bar for its primary end point (of sustained therapy-free clinical, endoscopic and radiological remission at 1 year) and failed to achieve it.517 One of the 23 patients undergoing HSTC died and serious adverse events (particularly infection) were common, especially in individuals with perianal Crohn’s disease. Nonetheless in this treatment-refractory population there were, among the component parts of the composite primary outcome, suggestions of benefit in some patients and further trial data are needed.518
4.4.5 Leucocyte apheresis
Statement 50. We recommend that leucocyte apheresis is not used for active Crohn’s disease due to lack of efficacy (GRADE: strong recommendation, high-quality evidence. Agreement: 100%).
Although a number of uncontrolled studies have suggested possible efficacy of leucocyte apheresis in IBD, a randomised, double-blind controlled trial in 235 patients with moderate to severely active Crohn’s disease showed no benefit of granulocyte/monocyte apheresis over sham apheresis.519
4.5 Proximal jejunal or extensive small bowel disease
Statement 51. Patients with jejunal or extensive small bowel disease have a worse prognosis. We suggest that they may be considered for early use of biological therapy, and should have nutritional assessment and support (GRADE: weak recommendation, very low-quality evidence. Agreement: 100%).
Crohn’s disease proximal to the terminal ileum (L4) occurs in 16% of Crohn’s disease patients, and of these about half will have jejunal involvement.520 Patients with jejunal involvement are more likely to have stricturing disease, and to require repeated surgery, compared with those who have oesophageal, gastric and/or duodenal disease or those with no disease above the terminal ileum.520 In a study of capsule endoscopy, patients with jejunal lesions (in addition to disease elsewhere) were more likely to have relapses over the next 2 years.521 In patients having small bowel surgery, those with jejunal disease have a higher recurrence rate, compared with those with ileocaecal disease.522 As a consequence of poorer prognosis, patients with jejunal or extensive small bowel disease should be considered for early introduction of biological therapy.
4.6 Upper gastrointestinal Crohn’s disease
Statement 52. We suggest that mild gastroduodenal Crohn’s disease may be treated with proton pump inhibitors. We suggest that moderate or severe disease may also require treatment with corticosteroids, and other immunosuppressive or biological therapies as for Crohn’s disease elsewhere in the gut (GRADE: weak recommendation, very low-quality evidence. Agreement: 92.7%).
Statement 53. We suggest that mild oesophageal Crohn’s disease may be treated with proton pump inhibitors. Nutritional assessment and support is essential. A short course of corticosteroids may be required if symptoms worsen, but early anti-TNF therapy should be considered for ongoing moderate to severe disease. Oesophageal dilatation should be used for strictures, and surgery is a last resort for disease refractory to all medical therapy (GRADE: weak recommendation, very low-quality evidence. Agreement: 97.6%).
A multidisciplinary international expert panel (European Panel on the Appropriateness of Crohn’s Disease Therapy, EPACT II) published guidance on the management of special situations in Crohn’s disease in 2009, including upper gastrointestinal disease.523 No discrimination was made between oesophageal, gastric or duodenal disease, and limited evidence was provided in support of recommendations. However, the group split guidance into patients with stenosis and those without, with recommendation that Helicobacter pylori be sought and eradicated in all.
In the absence of stenosis, proton pump inhibitors (PPI) were recommended as first-line therapy, with steroids second-line, and thiopurines and infliximab as third-line. Adalimumab was deemed of uncertain benefit. 5-ASA, certolizumab, surgery and natalizumab were deemed inappropriate.
In the presence of stenosis, balloon dilatation was recommended as first-line therapy, with PPI second-line, and steroids/thiopurines/surgery as third-line. Infliximab was deemed of uncertain benefit.
Nutritional support is often needed, and may be best delivered by gastrostomy tube for severe or stricturing disease. Exclusive enteral nutrition is beneficial, especially in children. In isolated oesophageal disease, alternative diagnoses should be considered, including gastro-oesophageal reflux disease, sarcoidosis, tuberculosis, disseminated fungal disease, Behçet’s disease and malignancy.524
4.6.1 Orofacial granulomatosis
Statement 54. We suggest that patients presenting with features of orofacial granulomatosis (OFG) and gastrointestinal symptoms, raised inflammatory markers or raised faecal calprotectin should have the gastrointestinal tract investigated for inflammation (GRADE: weak recommendation, very low-quality evidence. Agreement: 100%).
Orofacial granulomatosis (OFG) is a rare disease with similar microscopic appearances to intestinal Crohn’s disease. Granulomatous inflammation is found in about two-thirds of biopsies in OFG but is not needed for a diagnosis.525 The precise relationship between OFG and Crohn’s disease remains uncertain, with oral Crohn’s disease and OFG terminology often overlapping.
Gastroenterologists have been reported to miss around half of oral lesions compatible with oral Crohn’s disease when compared with dentist examination.526
The threshold for luminal assessment should probably be lower in younger patients, where positive findings are more likely. Sarcoidosis, tuberculosis and chronic infection (particularly dental-associated infection) should be considered in the differential diagnosis. Patients should be referred for assessment to an oral medicine clinic.
The current evidence for OFG management relates to case series only. Topical steroids and tacrolimus are often used, but with limited evidence. An 8-week cinnamon and benzoate-free diet was reported in 25 patients with OFG as first-line therapy with 72% responding, but with flares on further consumption of previously eliminated cinnamon/benzoate-containing foods.527 The mechanism of this effect remains unclear and the long-term continuation of such a diet is challenging. Six weeks of exclusive enteral nutrition (EEN) with Elemental 028 has been used successfully to treat 19 of 22 children with OFG, with 10/10 of isolated OFG cases and 10/12 cases with OFG and Crohn’s disease responding.528 Objective criteria for improvement were not reported in this study. Such a diet would naturally eliminate cinnamon and benzoate, so may be overly-exclusive in some patients who might have responded to a more targeted elimination.
In a retrospective cohort of 22 non-Crohn’s disease OFG patients treated with intralesional triamcinolone injection, 63.6% of patients had no disease recurrence after a single course of injections.529 The mean disease-free period after therapy was 28.9 months (95% CI 28.7 to 29.1). Response to azathioprine in OFG was significantly greater in those with Crohn’s-associated disease.530 A small case series of 14 OFG patients, half with Crohn’s disease, treated with infliximab suggested 71% short-term response, but only 33% were still responding at 2 years.531 Two patients with loss of response subsequently responded to adalimumab.
It would seem pragmatic to treat systemic Crohn’s disease with standard therapies in the presence of OFG and to add dietary, topical or intralesional approaches if there is no response. Conversely, systemic treatment of isolated OFG should be conserved for disease unresponsive to more limited approaches.
4.7 Stricturing disease
For guidance on imaging see the Section 4.1.3.3 Crohn’s disease, Diagnostic tests, Investigation of strictures.
4.7.1 Medical therapy for strictures
Good Practice Recommendation 8. Patients with stricturing small bowel Crohn’s disease should have joint medical and surgical assessment to optimise medical therapy and plan requirement for surgical resection or strictureplasty (Agreement: 100%).
The CREOLE study evaluated 97 Crohn’s disease patients with symptomatic small bowel strictures and assessed response to adalimumab treatment. Treatment was successful at week 24 in 64% of patients, and a prognostic score at baseline was constructed. This included clinical features (use of immunosuppressive drugs at baseline, obstructive symptoms, severity and duration, and MRE features (length of stricture <12 cm, an intermediate proximal small bowel dilatation (18–29 mm), marked enhancement on delayed T1-weighted sequence and absence of fistula). A higher score was associated with greater likelihood of response to therapy. The authors emphasised the complexity of assessing inflammation and stricturing, which nearly always occur together, and the value of both clinical and MRI features in deciding the value of using drug therapy rather than surgery for small bowel strictures.532
Small bowel bacterial overgrowth is common in small bowel Crohn’s disease,533 particularly in areas above strictures, and responds to broad-spectrum antibiotics534 535 (for further detail see the Section on 4.10.1.2.2 Post-surgical management of Crohn’s disease: Small intestinal bacterial overgrowth). For nutritional advice for patients with strictures see box 8.
4.7.2 Surgical therapy for strictures
Rates of surgery for Crohn’s disease appear to be declining.536 537 Patient selection and outcomes in stricturing disease can be optimised by careful assessment of fibrotic burden538 as well as due consideration of alternatives including endoscopic therapy,539–542 and decisions are best taken with joint input from all MDT members. As discussed above, a prognostic score based on MRE features and clinical factors can help in predicting the likely response to anti-TNF therapy. A moderate degree of dilatation proximal to the stricture is associated with greater likelihood of response than either massive dilatation or, rather surprisingly, no dilatation. Having more marked obstructive symptoms, but with a shorter duration, is also associated with success of anti-TNF therapy.532
4.7.3 Strictureplasty
Statement 55. We recommend that strictureplasty is an alternative to resection in patients with small bowel Crohn’s disease strictures shorter than 10 cm, and is useful where there are multiple strictures or a need to preserve gut length. Longer strictures can be treated using non-standard strictureplasty techniques (GRADE: strong recommendation, very low-quality evidence. Agreement: 97.3%).
Strictureplasty, a technique for surgical treatment of small bowel strictures without loss of bowel length, is indicated with single or multiple strictures, impending short gut or previous extensive small bowel resection. The presence of fistulae, fistula-associated abscesses or possible carcinoma are contraindications. The presence of active inflammation at the stricture site does not prevent successful strictureplasty.543 Strictureplasty is not associated with increased recurrence or re-operation rates.544–546 In fact, there is evidence re-operation rates may be lower at strictureplasty than resection sites,547 although a meta-analysis of seven studies (688 patients) from 2006 showed a non-significant trend to lower risk of complications if strictureplasty alone was performed, but a non-significant trend to increased recurrence after strictureplasty and significantly longer recurrence-free survival for those having a bowel resection.548 The conventional Heineke–Mikulicz strictureplasty is generally used for strictures up to 10 cm length, with intermediate length (10–25 cm) using a modified technique such as the Finney procedure and an enteroenterostomy (Michelassi procedure) for longer strictures.538 549 The newer techniques are generally as safe and effective as the conventional strictureplasty.550
Good Practice Recommendation 9. If there are multiple strictures close to each other in a segment of bowel and there is adequate remaining healthy bowel, a single resection may be preferable to multiple strictureplasties (Agreement: 100%).
If multiple small bowel strictures can be dealt with by a single resection in a patient with adequate bowel length elsewhere, then this is preferable to avoid a complex multiple strictureplasty procedure, but such decisions have to be individualised, considering the patient’s condition at the time of surgery (corticosteroid and immunosuppressive drug use, serum albumin, anaemia, nutritional status), potential for postoperative complications from complex surgery and the risk of future malabsorption and malnutrition due to short gut.538 550 551
4.7.4 Endoscopic therapy for strictures
Statement 56. We suggest that balloon dilatation is an appropriate treatment for ileocolonic anastomotic strictures less than 4 cm in length, without sharp angulation and with non-penetrating disease, although the majority will require repeated dilatation. Endoscopically accessible ileal strictures are also amenable to balloon dilation, but complication rates and recurrence rates are higher (GRADE: weak recommendation, low-quality evidence. Agreement: 94.4%).
Endoscopic balloon dilatation may prevent or delay the need for surgical resection or strictureplasty for Crohn’s disease-related intestinal strictures, including anastomotic strictures. A key concern is the long-term outcome, in particular the need for surgical resection. A systematic review identifying 24 published studies reported outcomes from 1163 patients, with overall surgical intervention rates over a median follow-up period of 15–70 months of 27%.541 Surgical intervention rates were higher after dilatation of primary strictures, but this did not reach statistical significance. Stricture length <4 cm was associated with a significant reduction in the need for surgical intervention. However, in a different systematic review of largely the same primary papers, 25 studies with data on 1089 undergoing a total of 2664 dilatations estimated the cumulative rate for surgery after 5 years of follow-up as 75%, leading the authors to suggest caution around use of the technique.542 However, this figure may overestimate the ultimate requirement of surgery as 5-year follow-up data were only available in 455 patients, who may have remained in follow-up due to a more complicated disease course. The authors did not find any association between stricture subtype and outcomes.
A small study has shown benefit of intralesional injection of corticosteroids at the time of balloon dilatation of Crohn’s disease strictures,552 but further studies have not shown benefit.553 554
4.8 Non-perianal fistulising Crohn’s disease and abscesses
4.8.1 Intra-abdominal abscesses
Statement 57. We suggest that intra-abdominal abscesses complicating Crohn’s disease may be treated initially with intravenous antibiotics and where possible radiological drainage. Surgical drainage may be required but immediate resection should be avoided (GRADE: weak recommendation, very low-quality evidence. Agreement: 91.9%).
4.8.2 Medical therapy
In the first instance, patient optimisation is required when localised perforation in Crohn’s disease has led to abscess formation. Surgical intervention is mandatory within the context of free peritonitis and highly likely to be required at some stage in the setting of localised abscess formation. Ideally, surgery takes place following treatment of sepsis and treatment of nutritional deficiencies. Exclusive enteral nutrition can be an effective means of controlling intestinal inflammation without use of corticosteroids.
Good Practice Recommendation 10. Following treatment of an abdominal abscess in the setting of non-perianal fistulising Crohn’s disease, joint medical and surgical discussion is required, but interval surgical resection is not always necessary (Agreement: 100%).
Some observers suggest that surgery may be avoided by percutaneous radiological drainage of abscesses and then resumption of medical therapy.555 The largest case series to date of 51 patients identified retrospectively from review of medical charts from a single centre over a 10-year period has shown that patients undergoing surgical resection were significantly less likely to develop abscess recurrence than those treated with antibiotics alone or percutaneous drainage over a mean follow-up of 3.75 years (12% vs 56%).556 Nevertheless, non-surgical approaches were successful in preventing subsequent surgery in almost half of the patients treated medically. An almost identical proportion of patients avoided surgery over long-term follow-up in a different series of 32 patients managed with percutaneous drainage for perforating Crohn’s disease.557 This strategy, if successful in treating sepsis, is likely to lead to lower morbidity and potentially lower stoma rates.
4.8.3 Enterovaginal and enterovesical fistulae
Statement 58. We recommend that enterovaginal and enterovesical fistulae should be managed jointly with medical control of inflammation and surgical resection (GRADE: strong recommendation, very low-quality evidence. Agreement: 100%).
Data on the management of non-perianal fistulae, especially from randomised trials, are limited. There are even more limited data on the outcomes of patients treated for specifically entero-gynaecological or enterovesical fistula. Although these fistulae are rare, they are a serious problem to patients with Crohn’s disease. A systematic literature review showed that response to medical therapy (fistula closure) was complete in 38.3% of rectovaginal fistulae and 65.9% of enterovesical fistulae.558 For enterovesical fistulae, risk factors for the need for surgical intervention include sigmoid origin and other complications of Crohn’s disease including small bowel obstruction, abscess formation, other fistulation, ureteric obstruction or urinary tract infection.559 These authors suggest that enterovesical fistulae should be treated medically initially, with surgery reserved for those with bowel obstruction or abscess formation, non-responders or recurrence after medical therapy. In a series of 47 patients with genital fistulae, antibiotics had no lasting benefit, thiopurines resulted in 13% complete and 24% partial response, and anti TNF-alpha therapy gave 17% complete and 30% partial response. Surgery was undertaken in a third of patients, but only 22% had complete response after a first operation and 39% after reintervention. Overall, fistula closure was only achieved in a third of patients.560
These studies highlight that there is still very limited evidence on which to base specific management guidance, but medical therapy alone or in combination with surgery would appear to offer benefit to some patients in the management of enterovaginal and enterovesical fistulae. Patients should be discussed in multidisciplinary meetings and treatment individualised, considering patients’ symptoms and situation.
4.8.4 Enteroenteric fistulae
Enteroenteric fistulae are often asymptomatic and expert consensus guidelines have recognised that these do not always require surgery.561
4.8.5 Enterocutaneous fistulae
Statement 59. We suggest that low volume enterocutaneous fistulae may be controlled with immunomodulator and biological therapy. High-volume fistulae usually require surgery to achieve symptom control (GRADE: weak recommendation, very low-quality evidence. Agreement: 100%).
Enterocutaneous fistulae usually communicate with segments of active Crohn’s inflammation, often in the context of other complications including intra-abdominal abscess and luminal strictures, or with surgical anastomoses (as a manifestation of the poor healing which characterises Crohn’s disease). Historically, enterocutaneous fistulae were treated surgically but, with the advent of anti-TNF therapy, conservative approaches can be deployed and may lead to definitive fistula closure in some patients. There are no prospective trial data to guide therapy. Both the fistulae and any associated complications will need to be managed together. For example, in the context of a high output fistula with nutritional deficiency and luminal stricture, a patient will require a period of nutritional and biochemical optimisation, control of sepsis and drainage of collections before definitive surgical management.562 563
There is little formal evidence on the role of immunosuppressive therapy. If a fistula is associated with active inflammation then medical therapy is worthwhile, but it is unlikely to help a postoperative fistula.564 A retrospective series of 48 patients with enterocutaneous fistula from GETAID included 21 postoperative fistulae (within 30 days of surgery, most but not all of which were intestinal resections).565 One third had multiple tracts and one quarter had high output. In addition to managing the associated complications, patients were treated with anti-TNF therapy. One third had fistula healing, half of whom relapsed over a median follow-up of 3 years. One third of patients developed an intra-abdominal abscess while on anti-TNF therapy. Surgery was required in 54% of patients overall. Complexity (multiple tracts) and associated stenosis were associated with reduced rates of healing with anti-TNF therapy and increased need for surgery. Increasing complexity of the fistula is associated with adverse outcomes including mortality.566 All patients with enterocutaneous fistulae should be managed by a multidisciplinary team.
4.8.6 Anti-TNF therapy for non-perianal fistulae
Statement 60. We suggest that anti-TNF therapy may be used to control inflammation or maintain remission in the setting of non-perianal fistulising Crohn’s disease (GRADE: weak recommendation, low-quality evidence. Agreement: 94.6%).
Statement 61. We recommend that anti-TNF therapy should only be started after abscesses have been treated with antibiotics and, where possible, drainage (GRADE: strong recommendation, very low-quality evidence. Agreement: 94.9%).
Higher quality evidence is available for infliximab relative to adalimumab for the use of anti-TNF therapy in the setting of non-perianal fistulising Crohn’s disease. The ACCENT II trial included 25 women with a total of 27 draining rectovaginal fistulae at baseline.567 Closure at week 14 after open label infliximab induction therapy was achieved for 45% of fistulae. Randomisation to infliximab during maintenance therapy was associated with a longer duration of fistula closure compared with placebo therapy (median 46 weeks vs 33 weeks). Outcomes for patients in ACCENT II with enterocutaneous fistulae have not been reported separately, but these patients represented less than 10% of the total cohort. Adalimumab has never been subjected to a randomised control trial of efficacy in fistulising Crohn’s disease.
4.9 Perianal Crohn’s disease
4.9.1 Assessment of perianal disease
Good Practice Recommendation 11. Multidisciplinary decision-making should be the standard of care for patients with perianal Crohn’s disease (Agreement: 97.4%).
Multidisciplinary team working in perianal Crohn’s disease is widely regarded as best practice according to expert consensus.561
Statement 62. We recommend that pelvic MRI is used as an important adjunct to clinical assessment and examination under anaesthesia (by an experienced surgeon) in evaluation of fistulising perianal Crohn’s disease. Depending on local availability and expertise, endoanal ultrasound may also be used (GRADE: strong recommendation, high-quality evidence. Agreement: 100%).
Pelvic MRI has a well-recognised role in defining the anatomy of perianal fistulae as an adjunct to examination under anaesthesia (EUA). Initial reports of sensitivity compared with EUA suggested rates of 85–89%.568–570 MRI may also pick up a significant burden of non-fistulising perianal disease that would otherwise be missed clinically.570 571 Endoanal ultrasound has also shown high sensitivity, although use is limited in patients with anal or other luminal stenoses.569 570 Interpretation of fistula imaging (MRI or endoanal ultrasound) is dependent on operator expertise.
An experienced colorectal surgeon should perform EUA to assess perianal disease and identify the anatomy of the fistula tracts, as specialist expertise and knowledge are likely to improve identification of all tracts.569 572 573 In a comparison with endoscopic ultrasound and MRI, an experienced operator correctly classified 91% of patients’ perianal fistulae at EUA (95% CI 75% to 98%).569 However, a combination of two tests from MRI, endoanal ultrasound and EUA is recommended to give the optimal assessment.574 Specifically, unless directed by the results of MRI or endoanal ultrasound, then small abscesses or collections may be missed, particularly if there is significant induration or a supralevator collection.574 EUA is more sensitive than MRI in assessment of anal ulceration or anal canal stenosis.571
Statement 63. We recommend that examination under anaesthesia should include an assessment of the rectal mucosa as the presence of proctitis is associated with lower rates of fistula healing in perianal Crohn’s disease (GRADE: strong recommendation, high-quality evidence. Agreement: 100%).
Assessment of rectal mucosa at the time of EUA is important.572 575 Largely observational data, but with a large effect size, from the pre-biologics era show that outcomes are worse for perianal fistulising disease associated with rectal inflammation. A study from St Mark’s of perianal fistulising Crohn’s disease patients diagnosed in 1993–4 showed that 29% of those with rectal involvement had proctectomy compared with 4% of those with no rectal involvement.576
4.9.2 Seton insertion
Statement 64. We recommend that setons should be placed to prevent re-accumulation of perianal sepsis in fistulising Crohn’s disease (GRADE: strong recommendation, moderate-quality evidence). The optimal timing of seton removal is uncertain (Agreement: 97.1%).
EUA permits drainage of abscesses and placement of setons, with evidence that placing setons prior to starting anti-TNF therapy improves rates of healing and reduces recurrence rates.577–579 A recent meta-analysis confirmed the benefits of combined surgical and medical therapy in improving healing and makes recurrent abscess less likely.580 The exception to routine insertion of setons would be patients with rectovaginal fistulae in the absence of an abscess or collection. In this situation, setons may make faecal discharge per vagina worse.
Evidence for the timing of seton removal is unclear. Early studies removed setons at or shortly after the second infliximab infusion.567 577 579 More recent studies suggest later removal, either after completing infliximab induction therapy581 or after at least five infusions.582 Setons need to be removed to permit complete healing of fistula tracks, but if active inflammation is ongoing, then seton removal may result in recurrent abscess. The optimal timing and assessment method remain unclear, and some patients may require long-term setons to avoid or delay proctectomy. Further trials are needed to better understand the optimal management of perianal fistulae in Crohn’s disease.583 584
4.9.3 Anti-TNF therapy post-surgery for complex perianal fistulae
Statement 65. We recommend that infliximab is used as the first-line biological therapy for complex perianal fistulae, and should be started as soon as adequate drainage of sepsis is achieved (GRADE: strong recommendation, high-quality evidence. Agreement: 100%).
4.9.3.1 Infliximab for perianal fistulising disease
Higher level evidence is available for infliximab relative to adalimumab for complex perianal fistulae following initial surgical management, such as draining abscesses and seton placement. Use of infliximab has been shown to be effective for the closure of perianal fistulae. In a study of 94 patients with Crohn’s disease and abdominal or perianal fistulae, induction therapy with 5 mg/kg or 10 mg/kg was associated with complete fistula closure rates of 55% and 38% compared with 13% placebo.585 In the subsequent ACCENT II trial, this induction response was confirmed in an open-label phase, with fistula closure in 69% of patients at 14 weeks. Subsequent randomisation to infliximab was associated with a significantly longer median time to loss of response compared with patients randomised to placebo (>40 weeks vs 14 weeks), with 36% of patients completing this maintenance phase showing a complete absence of draining fistulae after 54 weeks of infliximab treatment compared with 19% of placebo patients (p=0.009).567
Higher infliximab doses may be beneficial for perianal fistulising disease, with target levels >10 µg/mL associated with better response.586
4.9.3.2 Adalimumab for perianal fistulising disease
Fistula closure or improvement has not been the primary outcome of any prospective randomised trials of adalimumab. The CHARM trial showed increased efficacy compared with placebo for closure of abdominal or perianal fistulae as a secondary end-point, but outcomes for fistula subtypes have not been reported. At baseline there were 117 patients with draining fistulae. All patients received open-label induction therapy with adalimumab and were then randomised to maintenance therapy with adalimumab or placebo. Complete fistula closure at week 56 was seen in 33% of subjects on adalimumab versus 13% on placebo (p=0.016).486 Of all those with healed fistulae at week 56 (including those on placebo), 90% (28/31) maintained healing after a year of open-label adalimumab.587
A randomised controlled trial in which 76 patients with active perianal fistulising disease received open-label therapy with 24 weeks adalimumab in combination with either ciprofloxacin 500 mg BD for 12 weeks or placebo found that, after 12 weeks, the primary end-point of 50% reduction in draining fistulae was achieved in 71% in the combination adalimumab/ciprofloxacin group against 47% in the adalimumab/placebo group (p=0.047).588 However, by week 24 (ie, 12 weeks after cessation of antibiotic therapy) the difference between the two groups was no longer significant. This suggests the addition of an antibiotic may speed healing but not affect the final outcome. Further evidence is required before this can be recommended as routine practice.
4.9.4 Combined surgical treatment with anti-TNF therapy
None of these studies included initial surgical interventions for the management of fistula tracts. No randomised controlled trial has compared these treatments directly or attempted to evaluate the additional benefit of combination therapy compared with treatment with either surgery or anti-TNF alone. Nevertheless, comparison between these approaches has been the subject of several retrospective studies which have recently been systematically reviewed. Although significant heterogeneity between individual studies limits interpretation, there is a consistent trend towards improved outcomes with combined surgical and anti-TNF treatment.580 583 Careful preparation of the fistula track with curettage to destroy all epithelial tissue and ligation of the internal opening as standard treatment in both active and control arms of one trial of mesenchymal stem cells achieved a ‘placebo’ (surgical preparation only with no active medical treatment) success rate of 34% at week 24.589 It is highly likely that multiple treatment modalities will be needed to control perianal fistulae in Crohn’s disease.590
4.9.5 Vedolizumab and ustekinumab therapy
Post hoc analysis of 57 patients with fistulae (site not specified) in the GEMINI 2 study showed higher rates of closure of draining fistulae at 1 year: 41.2% on 8- weekly vedolizumab (p=0.03 vs placebo) and 22.7% on 4- weekly vedolizumab (not significant vs placebo).497
Data for outcomes for those patients with fistulae at baseline in the CERTIFI phase 2o and UNITI phase 3 studies of ustekinumab have been reported in abstract form, showing a non-significant trend towards improved fistula healing in patients randomised to ustekinumab compared with placebo.591 Additional data suggesting healing with ustekinumab come from relatively small case series of TNF refractory patients.507 508 592 Further controlled trial data are needed to confirm the role of ustekinumab in perianal fistula healing.
4.9.6 Surgical treatment of fistulae
Good Practice Recommendation 12. Surgical options for perianal Crohn’s disease fistulae (advancement flap, LIFT, infill procedures) should only be offered in selected patients after counselling as long-term results are poor, particularly for those with complex disease and ongoing disease activity. (Agreement: 97.1%).
In a survey of British surgeons, commonly performed definitive procedures in the context of perianal Crohn’s disease were removal of draining seton only (70.7%), fistulotomy (57.1%), and less commonly advancement flap (38.9%), fistula plug (36.4%) and the ligation of intersphincteric track (LIFT) procedure (31.8%).593 The reported efficacy of curative surgical options within the context of perianal Crohn’s disease is variable. Advancement flaps and the LIFT technique are effective in selective patients with perianal Crohn’s disease, with healing observed in two-thirds of patients at 1 year in a small prospective study.594 There is, however, progressive failure over time, related to both treatment failure and recurrent disease.595 Video-assisted anal fistula treatment (VAAFT) combined with advancement flap has been reported in complex fistulising Crohn’s disease with an 82% success rate at 9 months.596 Systematic review has demonstrated fistula plugs may be effective in 55% of Crohn’s disease-related fistulae,597 although variation in reported success is wide. A prospective randomised control trial of fibrin glue in 36 patients with Crohn’s disease perianal fistulae showed effective therapy in 38% after 8 weeks.598 In comparison, just 16% of those under observation only after removal of seton achieved remission (p=0.04). The benefit was greater in patients with simple fistulae. Administration of expanded adipose-derived stem cells in addition to fibrin glue appears more effective than fibrin glue alone.599 The long-term efficacy of fibrin glue, collagen plugs and paste is not clear.
4.9.7 Allogeneic adipose-derived stem cell therapy for perianal fistulae
Expanded allogeneic adipose-derived stem cells are simple to administer and safe.600 In a recent phase III study, 212 patients with treatment-refractory complex perianal fistulising Crohn’s disease were randomly assigned to a single intralesional injection of 120 million Cx601 cells (darvadstrocel) or placebo.589 Both active and control groups had an initial EUA with curettage of fistula tracts, and insertion of setons if needed, followed at least 2 weeks later by a further EUA with ligation of the internal fistula opening and injection of the trial treatment into the tissue adjacent to all fistula tracts. Week 24 complete remission rate was 50% for active treatment versus 34% for placebo (p=0.024). The high placebo response rate likely reflects the extensive surgical interventions received by the placebo group including curettage of the fistula tract and closure of the internal opening. Of note, failure of anti-TNF therapy was not a requirement for study entry, but rather patients had to have failed at least one of antibiotics, immunomodulator therapy or anti-TNF therapy. In fact, 79% of patients in this trial had been on an anti-TNF in the previous 6 months and 61% were on anti-TNF therapy at the point of randomisation. One-year outcome data demonstrate combined remission (closure of all treated external openings that were draining at baseline, and absence of collections >2 cm on MRI) of 56.3% in the darvadstrocel group, versus 35.6% in the placebo group (p=0.021). Clinical remission at 1 year was 59.2% and 41.6% respectively (p=0.013).601 Other groups have reported promising data with alternative preparations of allogenic stem cells, reviewed recently.602 Given the complexity of appropriate patient selection, management of luminal disease, surgical technique, selection of adjunct therapies and choice of stem cell preparation, patients offered these therapies should be closely monitored as part of a clinical trial or registry.
4.9.8 Defunctioning stoma formation
Statement 66. We recommend that faecal stream diversion can be used in patients with severe perianal Crohn’s disease refractory to medical therapy. Patients should be counselled that rates of subsequent successful reversal are low and proctectomy may ultimately be required (GRADE: strong recommendation, low-quality evidence. Agreement: 100%).
Creation of a defunctioning stoma has long been recognised to offer rapid improvement of perianal Crohn’s disease, even in complex cases. The mechanism likely relates to diversion of the faecal stream, which of itself seems to contain factors that promote rectal inflammation.603 Evidence is limited to expert opinion, supported by several case series.604–607 Although many of these series originate from a pre-biologics era, more recent data suggest that rates of successful stoma reversal after ileostomy for complex perianal Crohn’s disease are low.608 609 A systematic review showed that faecal diversion improves symptoms in approximately two-thirds of patients, but bowel restoration is only successful in 17%.610 Rates of successful reversal may be particularly low in those with rectal involvement.610 It should be noted that, after initial improvement, recurrence of inflammation can occur in the pelvis and defunctioned segment of bowel, and may present non-specifically with weight loss, raised inflammatory markers and fevers. For severe refractory disease, proctectomy is an effective treatment, but considered by expert consensus to be a last resort.607
4.10 Post-surgical management of Crohn’s disease
4.10.1 Disease recurrence following ileocolonic resection
In a study of factors predictive of recurrent disease after ileocaecal resection there was a symptomatic recurrence rate of 20% at 1 year and 47% at 5 years. There was a rapid development of endoscopic lesions in the neoterminal ileum (73% at 1 year).359 Risk factors for disease recurrence are discussed in the section below on medical prophylaxis (see Section 4.10.3: Reassessment and medical prophylaxis following ileocolonic resection).
4.10.1.1 Investigation for symptomatic recurrence following ileocolonic resection
Statement 67. We suggest that, in the event of symptomatic recurrence following ileocolonic resection for Crohn’s disease, an assessment of mucosal inflammation may be performed with ileocolonoscopy. Faecal calprotectin and/or cross-sectional imaging may be used if ileocolonoscopy is not possible or acceptable, but may not be sensitive enough to detect localised inflammation (GRADE: weak recommendation, low-quality evidence. Agreement: 97.4%).
After resection for Crohn’s disease of all inflamed tissue, the cumulative rate of symptomatic recurrence at 3 years is approximately 50%.359 Patients presenting with new symptoms of pain or diarrhoea after resection should be evaluated to confirm whether recurrent disease is the cause, as the differential diagnosis includes bile salt malabsorption and irritable bowel syndrome. Although ileocolonoscopy is the gold standard assessment to determine postoperative recurrence, there are times when it is not appropriate or technically possible and cross-sectional imaging may be needed. There is good agreement between assessment by MR enteroclysis and endoscopy: mean observer agreement was seen in 77.8% (kappa 0.67) in the diagnosis of postoperative recurrence.611 In experienced hands, small bowel ultrasound is predictive of endoscopic findings,612–614 with good correlation to the Rutgeerts score.615 While CT has also been shown to be effective in identifying postoperative recurrence,616 617 it should be avoided where possible to limit radiation exposure.
Faecal calprotectin and lactoferrin in postoperative Crohn’s disease patients correlate well with clinical disease activity as measured by the Harvey Bradshaw Index, whereas the correlation with C-reactive protein was weaker.618 There was, however, low sensitivity and specificity of the stool tests, particularly in those with mild or moderate clinical symptoms. In addition, this study did not show that faecal calprotectin was predictive of endoscopic (rather than clinical) recurrence. In the POCER trial, faecal calprotectin correlated with endoscopic recurrence, with a level >100 µg/g stool indicating endoscopic recurrence with a sensitivity of 89% and negative predictive value of 91%.619 A further multicentre observational cohort study of 86 asymptomatic Crohn’s disease patients following ileocaecal resection also identified a cut-off of faecal calprotectin of 100 µg/g as best to discriminate between endoscopic recurrence versus remission.620 In this study the sensitivity, specificity, negative predictive value, positive predictive value and overall accuracy at 100 µg/g were 95%, 54%, 69%, 93% and 77%, respectively. The TOPPIC trial also showed association of faecal calprotectin with clinical recurrence.621 TOPPIC also demonstrated the power of faecal calprotectin as a time-dependent variable, in that a 100 µg/g rise in calprotectin led to an 18% increase in the HR for clinical recurrence. It is suggested therefore that the use of faecal calprotectin is most helpful when there is a comparison value for the same patient when in known remission. A rise in the background level in the context of clinical symptoms should trigger further investigation and treatment.
4.10.1.2 Non-inflammatory causes of diarrhoea after ileocolonic resection
Good Practice Recommendation 13. Patients with recurrent symptoms following resection for Crohn’s disease, who have no evidence of active inflammation, should have consideration of other diagnoses including bile salt malabsorption, bacterial overgrowth, functional bowel disorders, adhesions, fibrostenotic or anastomotic strictures (Agreement: 97.3%).
Gastrointestinal symptoms in patients with previous surgery for Crohn’s disease are not necessarily related to recurrent inflammation. Conversely, minor anastomotic Crohn’s disease recurrence is often asymptomatic. Other diagnoses should be considered.
4.10.1.2.1 Bile salt malabsorption
Statement 68. We recommend that, following ileal resection, Crohn’s disease patients with diarrhoea suggestive of bile acid malabsorption should be given a therapeutic trial of a bile acid sequestrant such as colestyramine or colesevelam (GRADE: strong recommendation, moderate-quality evidence). A SeHCAT study can be considered for failed response to therapy or if the diagnosis is unclear (Agreement: 97.2%).
Bile acid diarrhoea due to malabsorption is common following ileal resection, occurring in more than 80% of patients.622–625 A therapeutic trial of bile acid sequestrants is therefore appropriate, particularly if faecal calprotectin is not significantly raised. A 75Se-HCAT (SeHCAT) scan should only be requested when there is uncertainty, as it is often abnormal after ileal resection or with ileal inflammation, and an abnormal scan does not prove that symptoms are due to bile salt malabsorption. Colestyramine is effective623 626 but may be unpalatable, and other agents such as colestipol or colesevelam, which are more expensive, can be used as alternatives for those who do not tolerate it.622 Bile acid sequestrants need to be stopped during the SeHCAT test. Loperamide can also be used.627 There is increasing interest in bile acid malabsorption as a cause of functional diarrhoea.628 Serum markers of bile acid diarrhoea, such as reduced fibroblast growth factor-19 levels629 630 and raised 7-alpha-hydroxycholestenone (C4),631 are not yet widely available; both tests will be abnormal in ileal resection, and also with ileal inflammation.
4.10.1.2.2 Small intestinal bacterial overgrowth
Small intestinal bacterial overgrowth occurs more commonly after Crohn’s disease resection,533 and can mimic Crohn’s disease in causing symptoms of bloating, diarrhoea, nausea or vomiting, weight loss or malnutrition.632 The prevalence in one study was 30% using a lactulose breath test, measuring hydrogen and methane.633 Bacterial overgrowth is more common if there are blind loops, dysmotility, diverticulae or strictures. The gold standard test for small intestinal bacterial overgrowth is jejunal aspirate with quantitative culture for aerobic and anaerobic organisms. This test is invasive and usually not available. Glucose or lactose hydrogen breath tests are more often used. Measurement of methane as well as hydrogen is recommended to increase sensitivity, but there is a lack of standardisation and poor sensitivity and specificity for these tests.634 Empirical treatment is recommended if the diagnosis is likely, with broad-spectrum antibiotics such as metronidazole, ciprofloxacin534 or rifaximin.635 Recurrent courses of treatment may be required.
4.10.1.2.3 Other causes of recurrent symptoms following ileocolonic surgery
Other co-existing conditions that can cause diagnostic confusion include irritable bowel syndrome,636 coeliac disease and short gut syndrome in those with extensive small bowel resection. Lymphoma and malignancy must also be considered. Postoperative complications should also be considered, including anastomotic strictures, collections and port-site hernia (after laparoscopic surgery).
4.10.2 Smoking cessation following surgery
Statement 69. We recommend that all patients smoking after intestinal resection for Crohn’s disease should be actively encouraged to stop (GRADE: strong recommendation, moderate-quality evidence. Agreement: 100%).
The best described environmental factor affecting the outcome of IBD is cigarette smoking, which has a negative impact on the clinical course of Crohn’s disease. It has been shown that cigarette smokers have quicker and more severe postoperative relapse in Crohn’s disease.621 637 Thus, all efforts should be made to help patients quit smoking after surgery by offering counselling, pharmacotherapy or nicotine replacement therapy (see Section 5.8.1: Smoking and Crohn’s disease).
4.10.3 Reassessment and medical prophylaxis following ileocolonic resection
Statement 70. We suggest that, following ileocolonic resection for Crohn’s disease, ileocolonoscopy may be performed at 6 months to assess the neoterminal ileum in order to consider treatment escalation if mucosal inflammation (Rutgeerts i2 or above) (GRADE: weak recommendation, low-quality evidence). If the anastomosis is not within reach of endoscopic examination, then cross-sectional imaging with MR enterogram may be performed (Agreement: 89.2%).
Statement 71. We suggest that Crohn’s disease patients with significant risk factors for disease recurrence following ileocolonic resection (particularly smoking) or with recurrent disease at 6 months post-surgery colonoscopy may be started on thiopurines (GRADE: weak recommendation, low-quality evidence) or anti-TNF therapy (GRADE: weak recommendation, low-quality evidence. Agreement: 94.4%).
Statement 72. We recommend that mesalazine should not be given to prevent recurrence after ileocolonic Crohn’s disease resection (GRADE: strong recommendation, moderate-quality evidence. Agreement: 97.2%).
A summary flowchart of postoperative medical prophylaxis following ileocolonic resection for Crohn’s disease is shown in figure 3.

Medical prophylaxis after ileocolonic resection for Crohn’s disease.
4.10.3.1 Risk factors for disease recurrence after ileocolonic resection
Surgery for the majority of patients with Crohn’s disease is not curative, with high rates of disease recurrence by 1 year.638 Endoscopic recurrence predicts future clinical relapse.359 639 By 6 months, endoscopic recurrence is apparent in between 39% and 84% of patients.640–642 A meta-analysis of the placebo groups of postoperative maintenance trials showed an endoscopic recurrence rate of 58% (95% CI 51% to 65%) at a median 1 year after surgery.643
Clinical factors predictive of symptomatic recurrence in the Rutgeerts study were preoperative disease activity, indication for surgery (fistulae and abscess being associated with more recurrence than strictures) and number of previous resections.359 Severity of recurrent mucosal lesions in the neoterminal ileum at colonoscopy after resection was the main predictor of subsequent symptomatic recurrence on multivariable analysis. Preoperative disease activity was the main clinical predictive factor. Smoking was not evaluated in this study but is the most important risk factor, with meta-analysis showing an increased risk of endoscopic recurrence by 2.5-fold and clinical recurrence 2-fold.637 Other risk factors for postoperative recurrence include prior resection, penetrating disease, perianal disease, extensive bowel disease (>50 cm), granulomas in the resection specimen and myenteric plexitis in the proximal resection margin.643–646
4.10.3.2 Evidence of benefit from medical prophylaxis to prevent postoperative recurrence
Postoperative prevention trials have been challenging in this area as clinical recurrence is less common than endoscopic recurrence, and commonly used end-points for clinical relapse such as the CDAI score are not validated in the postoperative setting. It has been much easier to demonstrate reduction in endoscopic recurrence rates, and endoscopic lesion severity does correlate with clinical recurrence risk.359 647
4.10.3.2.1 Thiopurine therapy
For those who are not able to stop smoking, the TOPPIC trial provided evidence that thiopurines may improve their chance of maintaining remission after surgery. This study did not, however, confirm a wider role for thiopurines in the postoperative context, with no overall difference in either clinical or endoscopic recurrence at 3 years (although a post-hoc analysis showed that complete endoscopic healing (Rutgeerts score i0) was more likely in the mercaptopurine group).621 A Cochrane review of previous trials showed low quality evidence for benefit of thiopurines in comparison to placebo.648
4.10.3.2.2 Anti-TNF therapy
Early studies had shown benefit for infliximab in preventing postoperative recurrence, but in general it has been easier to demonstrate prevention of endoscopic recurrence at 1 year649 650 or 2 years,651 as clinical relapse rates in these studies were lower and differences non-significant. The Yoshida650 study had follow-up at 3 years and there was a significantly higher remission rate of 93.3% on infliximab compared with 56.3% on no treatment. A study by Sorrentino et al 652 evaluated those who remained in clinical and endoscopic remission on infliximab at 2 years post-surgery, at which time the treatment was stopped. Ten of the 12 patients had endoscopic relapse at 4 months and all achieved healing on retreatment with lower doses of infliximab (3 mg/kg 8-weekly). A large double-blind placebo-controlled trial of postoperative infliximab in 297 patients did not demonstrate significant reduction in clinical relapse at 76 weeks (12.9% on infliximab) compared with placebo (20%), but did show reduction in endoscopic recurrence (30.6% vs 60%). Clinical relapse rates were low despite patients having to have a risk factor for recurrence (previous surgery, resection for penetrating disease, recent perianal fistulae or current smoking).653 For patients given anti-TNF prophylaxis postoperatively, the use of multiple anti-TNF drugs in the past makes relapse much more likely.654 A randomised three-arm study compared postoperative adalimumab against azathioprine and 5-ASA with a 2-year follow-up. There was significantly reduced endoscopic recurrence for those on adalimumab (adalimumab 6.3%, azathioprine 64.7%, 5-ASA 83.3%) and significantly reduced clinical recurrence (12.5%, 64.7% and 50%, respectively).655
4.10.3.2.3 Postoperative colonoscopy at 6 months
The POCER trial was a pragmatic randomised trial that compared an active care model using endoscopic assessment at 6 months postoperatively with standard care (no colonoscopy at 6 months).640 All patients entering the trial received metronidazole for 3 months postoperatively, and those at high risk of recurrence received thiopurines (or adalimumab if intolerant). In the active care group, treatment was stepped up if 6-month endoscopic recurrence was documented: to thiopurine, fortnightly adalimumab with thiopurine, or weekly adalimumab. At 18 months endoscopic recurrence was 49% in the active group versus 67% in the standard care group (p=0.03) and clinical recurrence was 27% and 40%, respectively (p=0.08).
4.10.3.2.4 Antibiotic therapy
Antibiotic therapy can maintain remission for at least 3 months after surgery.656 657 Metronidazole is the most widely used,658 but is poorly tolerated (23% dropped out during the 3 months trial treatment on metronidazole 20 mg/kg daily), and causes neuropathic complications which relate to total dose and generally prohibit longer use. Ornidazole is also effective but still limited by significant side effects (32% dropped out during the 1 year trial treatment).659 In a small pilot study, ciprofloxacin did not show much benefit over placebo.660 In view of its gut specificity and reduced side effect profile, there is interest in using rifaximin in this context. There is a study of rifaximin for maintenance therapy over 3 months after medically-induced remission,661 but trials are awaited in the postoperative setting.
4.10.3.2.5 Other treatment
Evidence regarding 5-ASA is conflicting, with small studies showing no significant benefit. Meta-analysis has shown a modest reduction in clinical recurrence and severe endoscopic recurrence,662 but less effectiveness than other therapies.663 Likewise, steroids have significant toxicity and are ineffective in maintaining postoperative remission.656 As yet there are not enough data to specifically recommend vedolizumab or ustekinumab in this context.
5 Common disease considerations
5.1 Infectious diseases and IBD: differential and concurrent diagnoses
5.1.1 Tuberculosis
Statement 73. We recommend that the differential diagnosis of tuberculosis should be considered in patients with suspected ileocaecal Crohn ’s disease, particularly in patients born in or who have lived for extended periods in endemic areas or have other risk factors for infection (GRADE: strong recommendation, very low-quality evidence. Agreement: 97.8%).
Differentiating between intestinal tuberculosis (TB) and Crohn’s disease may be challenging in those who have lived in endemic areas as clinical features may be similar. Features suggestive of a diagnosis of intestinal TB include night sweats, concomitant pulmonary tuberculosis, positive tuberculin skin test, antibodies to TB, abdominal lymphadenopathy, ascites, transverse ulcers and a patulous ileocecal valve.664–666 Haematochesia, involvement of the sigmoid colon, skip lesions and aphthous ulceration are more common in Crohn’s disease, whereas weight loss may be predictive of TB.665 Extraintestinal manifestations are more commonly associated with Crohn’s disease.666 A recent study from South Korea used 40 Crohn’s patients and 40 with intestinal TB to develop a predictive model using colonoscopic, laboratory and radiological criteria. Features suggesting Crohn’s at colonoscopy were anorectal lesions, longitudinal ulcers, aphthous ulcers and cobblestoning. Colonoscopic features suggesting TB were fewer than four segments of colon involved, patulous ileocaecal valve, transverse ulcers and scars or post-inflammatory polyps. Positive ASCA serology and proximal small bowel disease suggested Crohn’s, and a positive quantiferon gold test and typical pulmonary lesions suggested TB. A score derived from these features was able to make an accurate diagnosis in 96.3% of patients.667 TB PCR performed on intestinal biopsies may be helpful for discrimination between the diseases.668
5.1.2 Enteric infections associated with IBD
Statement 74. We recommend that all patients presenting with acute flares of colitis should have stool cultures for entero-invasive bacterial infections and stool Clostridium difficile assay (GRADE: strong recommendation, low-quality evidence). Microscopy and culture for amoebic or Shigella dysentery should be performed in patients with relevant travel history (Agreement: 93.5%).
The risk of enteric infections is higher in IBD than controls.669 A UK study showed that 10.5% of IBD relapses were associated with enteric infection (half were Clostridium difficile).670 A more recent retrospective study in over 9000 Mayo Clinic IBD patients from whom stools were collected showed a low rate of bacterial infection of less than 3% by culture and PCR (excluding C. difficile infections), with no adverse impact on disease course (higher proportions of stool positive patients remained in remission over the next year compared with those with a non-infective disease flare or C. difficile infection).671 A recent USA study using a multiplex PCR for gastrointestinal pathogens reported that 18.1% and 16.1% of samples from Crohn’s disease and UC patients respectively were positive. Crohn’s disease patients were more likely to have norovirus and Campylobacter, while UC patients were more likely to have bacterial infections, particularly Campylobacter, Plesiomonas and Escherichia coli (compared with non-IBD samples).672 The sensitivity of the molecular test used, the breadth of pick-up of the panel covered and the likelihood of false-positive infections because of asymptomatic carriage all warrant consideration when assessing the literature in this area. Nevertheless, a comprehensive infection screen considering clues from the history, and local infectious epidemiology, is an essential component of evaluating IBD disease flares.
5.1.3 Clostridium difficile infection associated with IBD
Statement 75. We suggest that Clostridium difficile infection in acute severe ulcerative colitis is associated with significantly increased risk of colectomy and should be treated with oral vancomycin (GRADE: weak recommendation, low-quality evidence. Agreement: 93.2%).
Clostridium difficile infection is more common in IBD than non-IBD populations, and in contrast to non-IBD populations, is less associated with PPI and antibiotic therapy.673 674 C. difficile can also be a cause of chronic pouchitis.675
A Canadian population-based case-controlled study of 278 UC patients hospitalised due to a flare of colitis and tested for C. difficile infection identified 6.1% were positive. These patients had an increased risk of colectomy (adjusted OR 3.39) and preoperative C. difficile infection was associated with a higher risk of postoperative infectious complications (OR 4.76).218 Observational studies have shown approximately 20% of IBD patients with C. difficile infection require colectomy.214 676 Outcomes in hospitalised IBD patients with C. difficile infection are worse with higher colectomy rates and higher mortality.215–218 677 678 A systematic review and meta-analysis showed that the 3-month colectomy risk was not increased by C. difficile infection (OR 1.35; 95% CI 0.68 to 2.67) either in IBD or non-IBD populations, but the colectomy risk after 1 year or more was higher for IBD overall (OR 2.23; 95% CI 1.18 to 4.21) and UC specifically (OR 2.96; 95% CI 1.19 to 7.34).679
In non-IBD populations vancomycin is equally as effective as metronidazole for mild C. difficile, but has superior efficacy in severe disease.680 As such, Public Health England recommend vancomycin therapy in severe infection, as do others.219 681 It is not necessary to withhold corticosteroid treatment for acute severe colitis in this situation, and a decision regarding continuation of immunomodulator therapy should be taken on an individual basis (including the surgical team in the discussion).196 681 It is prudent not to escalate therapy or introduce rescue therapy with infliximab or calcineurin inhibitors in ASUC associated with C. difficile infection, as there is little or no data on safety in this situation.
5.1.4 Cytomegalovirus infection in IBD
Statement 76. We suggest that patients with moderate to severe colitis, particularly those with corticosteroid-refractory disease, should have colonic biopsies to look for cytomegalovirus disease by H&E staining, and preferably also immunohistochemistry or quantitative tissue PCR (GRADE: weak recommendation, low-quality evidence. Agreement: 93.3%).
Cytomegalovirus (CMV) in IBD can be diagnosed by the presence of typical CMV inclusions on H&E stain, immunohistochemistry and/or tissue PCR. A recent systematic review suggested that blood-based testing and histology lack sensitivity to predict reactivation of CMV in the colon and so immunohistochemistry or tissue PCR remain essential in the detection of CMV IBD.682 In a retrospective case control study from the Mayo Clinic, the risk of CMV disease was independently associated with refractory disease, treatment with immunomodulators and age over 30 years.683 Other studies show an association of CMV with corticosteroid use, corticosteroid-refractory UC and leukopaenia.684–687 CMV viraemia and blood PCR have poor sensitivity for diagnosis of CMV colitis, though specificity is high.688 Immunohistochemistry or quantitative PCR can be used to detect CMV on mucosal tissue, and may allow detection of CMV in patients who do not have inclusion bodies on H&E staining.689–692 A recent systematic review has identified wide heterogeneity of the definitions of CMV infection and CMV intestinal disease.693 Due to this heterogeneity, the prevalence of CMV intestinal disease in IBD varies from 2% to 38%. Tissue PCR has a sensitivity of 65% to 100% and a specificity of 40% to 100% whilst immunohistochemistry had a sensitivity of 93% and a specificity of 92% to 100%. These are the preferred methods of diagnosis.
5.1.4.1 Treatment of CMV in IBD
Statement 77. We suggest that CMV reactivation in the colonic mucosa of patients hospitalised with an exacerbation of ulcerative colitis or Crohn’s colitis may be treated by intravenous ganciclovir 5 mg/kg twice daily while continuing conventional therapy with corticosteroids or rescue medication with infliximab or ciclosporin (GRADE: strong recommendation, very low-quality evidence). In rare cases with systemic disease (meningo-encephalitis, pneumonitis, hepatitis or oesophagitis), all immunosuppressive therapy should be stopped while CMV is treated (GRADE: weak recommendation, very low-quality evidence). (Agreement: 88.4%).
Reactivation of CMV infection detected by serology is common in IBD patients receiving immunosuppression.694 Low-level reactivation may disappear without antiviral therapy. Small observational studies show benefit for treating colonic CMV disease in UC patients, particularly those who are steroid-refractory.695 696 Hospitalised patients with refractory UC, associated with CMV disease, treated with ganciclovir and requiring treatment with infliximab or ciclosporin did not have a worse outcome compared with those receiving ganciclovir only.697 Antiviral therapy in patients with a high density of CMV inclusions (biopsy specimens with five or more inclusions) reduces the need for surgery in the following year.698 Despite the lack of controlled trial data, a recent review concluded that there was sufficient evidence to support antiviral therapy in patients with moderate to severe colitis, particularly those resistant to steroids and colonic CMV reactivation by H&E staining with immunohistochemistry and/or CMV tissue PCR.699 The treatment recommended by ECCO is intravenous ganciclovir (5 mg/kg twice daily) for 3–5 days, then oral valganciclovir (900 mg twice daily) for 2–3 weeks, but virology/microbiology advice should be taken regarding route and duration of therapy.700 Systemic CMV reactivation causing meningoencephalitis, pneumonitis, oesophagitis or hepatitis carry a poor prognosis and require prompt antiviral therapy and cessation of all immunosuppressive therapy.700
5.2 Immunosuppressive therapy
Good Practice Recommendation 14. All IBD patients to be initiated on immunosuppressive therapy should receive written information regarding the benefits, risks, side effects and monitoring of treatment (Agreement: 97.9%).
It is important that all patients receive written information prior to starting treatment, in addition to counselling regarding the risks of treatment and how these are minimised by monitoring. Patients have differing perceptions regarding treatment and this can significantly influence drug adherence.701 No study has addressed the impact of specific patient information, but a recent survey of IBD patients showed that patients access a wide variety of information sources about IBD and its treatment.702 Of these, information from the IBD team and written patient information material were the most widely used, and the most trusted by patients. Information can be provided by IBD teams in written form or by sign posting to official patient support websites that provide high-quality drug information for patients.
5.2.1 Prevention of infection related to IBD and immunosuppressive therapy
If evidence of active HBV, latent or active TB, HCV or HIV infection, seek specialist input prior to commencing immune modifying therapy.
Statement 78. We suggest that blood tests for thiopurine methyltransferase status and screen for HBV, HCV and HIV (and VZV if no history of chicken pox, shingles or varicella vaccination) may be arranged once diagnosis is confirmed for all Crohn’s disease and moderate to severe ulcerative colitis patients (GRADE: weak recommendation, very low-quality evidence. Agreement: 88.9%).
Statement 79. We recommend that IBD patients commencing immunomodulators or biologics treatment should undergo screening for HBV, HCV and HIV (and VZV if no history of chicken pox, shingles or varicella vaccination), unless screened already at time of diagnosis (GRADE: strong recommendation, very low-quality evidence. Agreement: 88.9%).
All IBD patients should be screened at diagnosis for infection risk, as there is both an increased risk of infection as a result of the disease and a high likelihood of requiring immunosuppressive drug therapy (box 4). Patients without a clear history of chickenpox, shingles or receipt of two doses of varicella vaccine should be tested for varicella zoster virus (VZV) IgG. All patients with IBD should be screened for hepatitis B and C, and HIV. The prevalence of hepatitis B and C viral infection in IBD was similar to the general population in 315 patients from France (hepatitis B virus 2.54%, hepatitis C virus 0.95%).703 A Dutch study showed that rates of screening for hepatitis B remain suboptimal at 36–49%.704 Opportunistic testing for HIV should be done at the same time, as the condition is treatable and has public health implications. A panel of viral screening at diagnosis makes it more likely that patients can receive appropriate vaccinations with less delay to receiving immunomodulator therapy, which is now used in at least half of patients at some stage in their disease course. For the same reason, checking thiopurine methyltransferase (TPMT) status early reduces delays in starting thiopurines.
Infection and pretreatment checklist at diagnosis and prior to immunomodulator or biological therapy
History of specific infections: HSV (oral, genital), VZV (chicken pox, shingles), tuberculosis.
Immunisation status: BCG, diphtheria, tetanus, pertussis, Haemophilus influenzae type B, polio, meningococcus, measles, mumps, rubella, pneumococcus, HPV, rotavirus, influenza, VZV/shingles.1285
Prior exposure to TB: household contacts, prolonged stay or origin from endemic area.
TB screening: patients considered for anti-TNF therapy should be screened for tuberculosis using a combination of clinical risk stratification, chest x-ray and interferon-gamma release assays.
TPMT: check in all patients considered for thiopurine therapy.
Serology: HBV, HCV, HIV and VZV (in patients without clear history of prior infection or prior vaccine).
5.2.1.1 Epstein Barr Virus
There is increasing interest in Epstein Barr virus (EBV) infection in IBD patients because of the risk of severe complications, including haemophagocytic syndrome and post-mononucleosis type lymphomas after primary infection and haemophagocytic syndrome and post-transplant type lymphoma during latent infection. A Spanish tertiary care centre studied 1483 patients aged over 17 years between 2006 and 2016.705 They assessed EBV seroprevalence and seroconversion and documented those who developed complications while on azathioprine. EBV had a role in tumour development in three out of five patients on azathioprine, but only one (in a 66-year-old man) occurred during a primary infection. The authors conclude that the risk of haemophagocytic syndrome and lymphoma on thiopurine therapy is not restricted to young males. This is confirmed in a USA paediatric IBD follow-up cohort, where 3/5 patients with haemophagocytic syndrome (all on thiopurines) were female. There was no association with use of infliximab or methotrexate (although numbers on methotrexate were much smaller).706 It remains unclear whether screening for EBV status should be done routinely in adults.707 In paediatric patients who are particularly at risk from primary EBV infection, there may be more justification for screening in order to avoid thiopurine use in those who are seronegative. Routine EBV testing prior to thiopurine therapy remains controversial.
5.2.1.2 Infection risk in patients on anti-TNF therapy
Meta-analysis of clinical trial data of 4135 patients receiving anti-TNF therapy as part of randomised clinical trials found a 0.9% incidence of opportunistic infection.708 This represented a two-fold increased risk of infections including TB, herpes simplex, oral or oesophageal candidiasis, herpes zoster, CMV, EBV and Nocardia in IBD patients (RR 2.05; 95% CI 1.10 to 3.85). The relative risk for TB was 2.52 (95% CI 0.62 to 10.21). Pooled analysis of 2266 patients receiving adalimumab as part of clinical trials found that higher disease activity was associated with an increased risk of opportunistic infection, with a 31% (HR 1.31; 95% CI 1.04 to 1.64) increase accompanying every 100 point rise in CDAI.709 IBD patients over 50 years of age receiving immunosuppression are at highest risk of opportunistic infection.710 711
For patients starting biologics or immunosuppressive drugs, the viral screen (as recommended at diagnosis, see box 4) should be performed if not done initially, or if new risk factors have arisen since that time.
5.2.1.2.1 Tuberculosis
Statement 80. We recommend that prior to commencing anti-TNF therapy, IBD patients should be screened for tuberculosis (TB) using a combination of clinical risk stratification, chest x-ray and interferon-gamma release assays (IGRAs) (GRADE: strong recommendation, low-quality evidence. Agreement: 97.8%).
Screening for active or latent TB is essential prior to starting anti-TNF or other biologic therapy. A Dutch study suggested that screening rates for TB in IBD patients are high at 90–97%, with 3% latent prevalence.704 Tuberculin skin test is likely to have false-negative results due to immunosuppressive therapy, so interferon gamma release assays (IGRA) should be used. A high rate of anergy to skin-based antigen tests was shown by immunising 82 consecutive IBD patients against tuberculin (TST) or control antigens.712 In this study no TST result was positive, but 71% of patients failed to respond to any antigen. Importantly, 83% of patients on steroid or immunomodulator therapy were anergic versus 43% not on these therapies (p<0.002). A retrospective study of TB screening in 340 patients in the USA with 512 Quantiferon TB Gold (QFT-G) IGRA tests reported 1.5% positivity, 2.7% indeterminate and 95.8% negativity.713 Only one case of tuberculosis reactivation occurred in 17 months of follow-up (0.3%). This patient had an indeterminate test and was on immunosuppressive therapy prior to testing. No significant difference was seen in positivity rates between those on immunosuppressive therapy and those not. Only moderate concordance was seen between TST and QFT-G in this study (kappa=0.4152, p=0.0041). IGRA tests were evaluated in 125 adult patients with IBD in London, 90 of whom were anti-TNF naïve, with 35 on established anti-TNF therapy.714 109 (87%) were BCG vaccinated. 98% IGRA tests were negative, 1% indeterminate and 2% positive. This method of screening was deemed cost-effective in comparison to the 2005 British Thoracic Society guideline.715 No subsequent cases of TB were reported with a median follow-up of 24 months. A Korean study examined newly developed TB cases in IBD patients on established anti-TNF therapy.716 They described 25 cases in total (84% pulmonary, 16% extrapulmonary), of whom 76% developed TB within 5 years of commencing anti-TNF despite previous negative screening for latent infection, and 12% developed reactivation of latent infection after 3 months of chemoprophylaxis. Primary infection with TB on anti-TNF agents is therefore a significant risk, particularly in higher incidence areas, irrespective of baseline screening.
It has been proposed that extensive screening for TB using chest x-ray and IGRA compared with chest x-ray and TST is only cost-effective if latent prevalence is >12% or false positivity rate of TST is >20%.717 In low prevalence areas, patients should have a risk assessment questionnaire and chest x-ray, with IGRA test if at increased risk.
5.2.1.2.2 Strongyloides stercoralis
Statement 81. We suggest that IBD patients who have travelled for long periods or lived in endemic areas may be at increased risk of parasitic infections, and may have Strongyloides serology, and eosinophil count checked prior to commencing anti-TNF therapy (GRADE: weak recommendation, very low-quality evidence. Agreement: 90.9%).
Strongyloides stercoralis is an intestinal parasitic infection affecting tens of millions of people globally. It has been estimated the infection may be present in up to 10–40% of the population in tropical and subtropical countries, rising to 60% in the poorest socioeconomic communities where environmental conditions favour spread of infection.718 Patients with HIV/AIDS have twice the risk of infection compared with non-HIV populations (OR 2.17; 95% CI 1.18 to 4.01). Immunocompromised patients, particularly those on systemic steroids, are at risk of potentially fatal hyperinfection syndrome, characterised by increased parasite burden leading to GI bleeding, pneumonia, sepsis or meningitis.719 Blood eosinophilia is a common finding in patients with S. stercoralis infection though is not present in all patients.720 S. stercoralis serology is unreliable in immunocompromised individuals. Treatment is with ivermectin or albendazole.
Risks and management of other opportunistic infections are well-covered in the ECCO guidance.700
5.2.1.3 Vaccination
Statement 82. We recommend that a vaccination history should be obtained and vaccinations updated for all patients with Crohn’s disease, those with moderate to severe ulcerative colitis at diagnosis, and prior to commencing immunomodulator or biologics in all patients. Live vaccinations may be given at least 4 weeks before starting and at a minimum of 3 months after stopping, but not while receiving immunosuppressive therapy (GRADE: strong recommendation, very low-quality evidence. Agreement: 93%).
Statement 83. We recommend that IBD patients receiving immunomodulators or biologics should receive influenza vaccination each autumn, and pneumococcal vaccination with a booster after 5 years (GRADE: strong recommendation, very low-quality evidence. Agreement: 95.5%).
A vaccination history should be taken both at diagnosis and prior to starting immunosuppressive therapy (see box 4). General advice regarding vaccination is given in box 5.
General considerations regarding vaccination
Live vaccines are contraindicated if your patient is on immunosuppression or with significant protein calorie malnutrition: live vaccines include BCG, attenuated (oral) influenza vaccine, measles, mumps and rubella (MMR), polio, rotavirus, oral typhoid Ty21a, varicella zoster, yellow fever. Immunosuppressive therapies include: glucocorticoids (prednisolone ≥20 mg/day or equivalent for 2 weeks or more), thiopurines, methotrexate, biological therapy and tofacitinib.
Shingles vaccination (current UK age recommendation is at age 70 years or up to the age of 79 years if not given at age 70 years) may be administered to those on low-level immunosuppression (defined as ≤20 mg prednisolone/day for >14 days, either alone or in combination with low-dose non-biological oral immunomodulators (methotrexate ≤25 mg/week, azathioprine ≤3 mg/kg/day or mercaptopurine ≤1.5 mg/kg/day).735
Immunomodulators should be withheld for 4 weeks after live vaccine administration.
Live vaccines should be avoided for at least 3 months after discontinuing treatment with immunosuppressive therapies above.
Infants exposed to biologics in utero should not receive live vaccines for 6 months after birth.
IBD patients on immunosuppressant therapy should receive pneumococcal vaccine and annual influenza vaccination (prior to starting treatment if possible) with a single pneumococcal booster at 5 years.
5.2.1.3.1 Non-live vaccines
IBD patients have a greater risk of contracting influenza than non-IBD populations (incidence rate ratio 1.58; 95% CI 1.49 to 1.68) and are more likely to require admission to hospital.721 Annual influenza vaccination is recommended for all immunosuppressed patients,1 700 722 although vaccine efficacy may be reduced, particularly in those on anti-TNF therapy.723 It should be remembered that the nasal influenza vaccine contains live virus and so should be avoided, with the injection favoured instead.
Assessment of hepatitis B serology and vaccination in all seronegative patients at diagnosis is recommended in ECCO guidelines, although the value of this in low prevalence countries has been questioned, and in the UK it may be more appropriate to offer this to high-risk groups on the basis of lifestyle, occupation or other factors.724 Efficacy of vaccination may be impaired in active IBD725 and in those on immunosuppressive drugs.726 727 After hepatitis B vaccination, anti-HBs response should be measured as higher doses may be required. Accelerated double-dose vaccination in IBD has been shown to improve response, with double-dose Engerix-B vaccine at 0, 1 and 2 months.728
Pneumococcal vaccination is also affected by immunosuppression and should ideally be administered at least 2 weeks before starting immunomodulators. Three pneumococcal vaccines are licensed in the UK: pneumococcal polysaccharide vaccine (PPV23, containing polysaccharide from 23 capsular types of pneumococcus) and two variants of pneumococcal conjugate vaccine (PCV13 and PCV10, containing polysaccharide from 13 and 10 capsular types of pneumococcus).729 The current recommendation for adults on immunosuppression is a single dose of PCV13 followed by PPV23 at least 2 months later; however, we recommend reviewing the Green Book for further detail. Booster pneumococcal vaccination with PPV23 is recommended after 5 years in patients who are asplenic, who have reduced splenic function or chronic renal disease. It seems reasonable to give boosters to patients on long-term immunomodulator therapy also, although there is little evidence in this group.
5.2.1.3.2 Live vaccines
Following live vaccination, the UK Department of Health currently recommends allowing 4 weeks for the immune response to be established prior to commencing immunosuppressive or biologics therapy.730 Live vaccination should be avoided during biologics therapy and for a minimum of 3 months after stopping.731–733 The evidence base for the 3-month period is poor, and while drug blood levels will be minimal by this time, it is unclear whether alterations to white cell populations may have more persistent subtle effects on immunity. The USA Centre for Disease Prevention and Control states in their IDSA guidelines that zoster live vaccination can be considered for patients aged 60 or over while on treatment with low-level immunosuppression (defined as prednisolone doses <20 mg, methotrexate weekly dose ≤0.4 mg/kg, azathioprine ≤3 mg/kg/day or mercaptopurine ≤1.5 mg/kg/day).734 In the UK the age recommendation for zoster vaccine is at age 70 or up to the age of 79 if not given at age 70, and the Green Book also advises that shingles vaccination may be administered to those on low-level immunosuppression (defined as ≤20 mg prednisolone/day for >14 days, either alone or in combination with low-dose non-biological oral immunomodulators (methotrexate ≤25 mg/week, azathioprine ≤3 mg/kg/day or mercaptopurine ≤1.5 mg/kg/day)).735
The UK Department of Health Green Book vaccination guide Chapter 6730 also suggests that all live vaccines can be considered for those on low-dose immunosuppression as defined above, including low-dose immunosuppressive drugs in combination with prednisolone up to 20 mg. There is evidence from a small controlled study that the use of zoster vaccine in IBD patients on low-level immunosuppression does not result in adverse effects, although antibody titres were somewhat lower than those in vaccinated IBD patients not taking immunosuppressive drugs.736 Live vaccination must not be given to those taking biologics, and should only be undertaken for those on low-level immunosuppression after careful consideration of the risks and benefits in conjunction with the patient.
The Green Book advises that live vaccination should be delayed until 6 months of age in children exposed in utero to biologics.730
5.2.2 Drug management: thiopurines
A checklist of considerations when commencing thiopurines is shown in box 6, and table 10 gives a guide on interpretation of thiopurine metabolites during dose optimisation. Practical management of thiopurine side effects is described in box 7.
Use and interpretation of thiopurine metabolites
Initiation of thiopurines
Before starting:
All patients should receive verbal and written information about their medication
Baseline FBC, U&E and LFT measurement
If available test NUDT15 genotype
Screen for HCV, HBV, HIV, refer if positive, consider HBV vaccination if naïve
Check VZV immunity and vaccinate if low
Vaccinate for influenza and pneumococcal vaccine
Check cervical screening up to date
Check TPMT and start at target dose once result available. Normal TPMT: 2 mg/kg azathioprine or 1 mg/kg mercaptopurine. Low: 1 mg/kg azathioprine or 0.5 mg/kg mercaptopurine. Very low: avoid thiopurine
Monitoring:
FBC, U&E and LFT at least at weeks 2, 4, 8, and 12, and then at least 3-monthly
Managing side effects of thiopurines
Pancreatitis:
Do not give AZA or MP again, even at low dose. High chance of recurrence
Nausea and vomiting:
Try switching from AZA to MP; or continue drug with split dosing
If recurs then consider low dose (25–33% of standard dose) AZA or MP+allopurinol 100 mg
Flu-like symptoms:
Unlikely to resolve on switching from AZA to MP; some evidence for AZA/MP+allopurinol 100 mg
If convincing early hypersensitivity reaction, there is high risk of recurrence and so consider switch to alternative class of drug
Newly abnormal LFTs:
Stop and check thiopurine metabolites
Withhold until LFTs abnormality resolves
If not resolving, investigate as usual
Once resolved, re-challenge with low dose AZA/MP+allopurinol 100 mg. This is particularly likely to work if the original metabolites showed hypermethylation (High MeMP levels)
Myelotoxicity:
Check thiopurine metabolites and alter dosage according to table 10
Monitor white cell counts closely
If total white cells <3.5×109/L or neutrophils <2×109/L, withhold thiopurine until counts correct above this level
If neutrophils <1 ×109/L, patients should be warned to present for antibiotics±GCSF if febrile
If TGN high, then restart at lower dose once abnormality has resolved and monitor haematology and thiopurine metabolites carefully
If MeMP high then consider restarting low-dose thiopurine with allopurinol 100 mg
If TGN low or normal then likely to reoccur. Advise to stop thiopurine in this circumstance
AZA, azathioprine; MP, mercaptopurine; AZA/MP, azathioprine or mercaptopurine; GCSF, granulocyte colony stimulating factor; MeMP, methylmercaptopurine nucleotides; TGN, 6-thioguanine nucleotides.
5.2.2.1 Thiopurine methyltransferase and NUDT15
Statement 84. We recommend that all IBD patients considered for thiopurine therapy should have assessment of thiopurine methyltransferase (TPMT) status (GRADE: strong recommendation, moderate-quality evidence. Agreement: 100%).
20–30% of IBD patients stop thiopurine treatment because of side effects. While overall, thiopurine methyltransferase (TPMT) activity does not predict adverse effects, the subset of patients with low TPMT activity are at increased risk of discontinuing thiopurines due to adverse effects. In a prospective study of TPMT-directed versus standard therapy, patients with TPMT variants fared significantly better if dosed according to TPMT status (2.6% haematological adverse effects in TPMT-directed therapy versus 22.9% in undirected group, RR 0.11, 95% CI 0.01 to 0.85).737 In a prospective evaluation of TPMT activity in 207 patients with IBD commenced on azathioprine, patients with heterozygous TPMT deficiency were much more likely to withdraw due to adverse effects compared with those with wildtype TPMT status (79% vs 35%, p<0.001).738 There is evidence that TPMT measurement in all patients starting thiopurine therapy is cost-effective.739 740
Statement 85. We recommend that thiopurines should be avoided in patients with low TPMT activity. The dose of thiopurine should be reduced to 50% in those with intermediate thiopurine activity. Daily dosage should also be reduced in patients with significant renal impairment (GRADE: strong recommendation, moderate-quality evidence. Agreement: 100%).
The usual dose of azathioprine is 2–2.5 mg/kg daily and for mercaptopurine 1–1.25 mg/kg daily for patients with normal TPMT activity (box 6). There is a very high risk of thiopurine-induced myelosuppression in patients with absent TPMT activity (homozygous or compound heterozygous TPMT deficiency). While very low dose (5% of usual target) has been proposed, a thiopurine should generally be avoided in this group. In those with heterozygous TPMT deficiency, however, 50% of standard thiopurine dose is associated with improved tolerance.737
Genetic variation in NUDT15 has now also been described in association with myelosuppression. This was originally described in East Asians741 but has now also been described in IBD patients of European ancestry.742 Recent CPIC guidelines recommend NUDT15 testing, particularly for Asian patients, with consideration of dose reduction or thiopurine avoidance.742
5.2.2.2 Starting dose for thiopurines
Azathioprine and mercaptopurine should be started at the full dose. There is no evidence that starting at low doses and then gradually increasing up to target improves safety or tolerance, and low-dose initiation may cause significant delay in achieving the correct target dose.743
5.2.2.3 Renal excretion of thiopurines
Thiopurine metabolites are renally excreted. Thiopurines should be used with caution in renal impairment with 75% of usual dose given if creatinine clearance is 10–50 mL/min, and 50% of usual dose if <10 mL/min.744
5.2.2.4 Cervical neoplasia and thiopurines
Statement 86. We recommend that women with IBD commencing thiopurine therapy should be advised to participate in a national cervical screening programme (GRADE: strong recommendation, very low-quality evidence. Agreement: 95.7%).
A number of large studies have found an increased risk of cervical dysplasia among women with IBD compared with controls.745 This risk is mainly confined to those on oral immunosuppressive therapy, including corticosteroids, and those who smoke.746–749 A meta-analysis gives an overall modest increase in risk, with an OR of 1.34 (95% CI 1.23 to 1.46) for IBD patients on immunosuppression.750 As a consequence, all women should be encouraged to participate in national cervical cancer screening programmes; in the UK this is currently 3-yearly from age 25–49 and 5-yearly from age 50–64 years.
5.2.2.5 Drug monitoring for thiopurines
Statement 87. Thiopurine metabolites (TGN and MeMP) can be used to optimise drug dosing. We suggest that metabolite monitoring may be used for those with inadequate response to therapy or toxicity, but should not be a substitute for routine monitoring blood tests (GRADE: weak recommendation, low-quality evidence. Agreement: 92.9%).
Measurement of the thiopurine metabolites (thioguanine nucleotides (TGN) and methylmercaptopurine (MeMP)) offers a benefit over standard haematological and biochemical monitoring by detecting non-adherence to therapy, inadequate dosing or an unnecessarily high dose of thiopurine,751 752 as shown in table 10. Furthermore, detection of a skewed metabolism towards excessive thiopurine methylation determines a group of patients at risk of poor response and hepatotoxicity.
Although one study has suggested cost-effectiveness of metabolite monitoring in improving sustained response to thiopurines,753 it is unclear whether routine measurement in all patients on thiopurines is beneficial, owing to wide variation in levels (as much as fivefold intra-patient variation in one study754). Although TGN levels of 230–400 pmol/8×108 erythrocytes have been associated with better response and MeMP levels >5000 pmol/8×108 erythrocytes with more liver toxicity,755 appropriate thresholds are unclear and small prospective studies have not shown clinical benefit.756–758 In patients on combination therapy with infliximab and thiopurines, a lower target level of TGN of 125 pmol/8×108 RBCs may be adequate to achieve therapeutic levels of infliximab,759 with a further study suggesting a target level of >105 pmol/8×108 RBCs.760
5.2.2.6 Low-dose thiopurines with allopurinol
Statement 88. We suggest that low-dose thiopurines (25–33% of usual dose) used in combination with allopurinol 100 mg may be considered in patients with thiopurine hepatotoxicity, nausea or flu-like symptoms, or those who are hypermethylators (GRADE: weak recommendation, low-quality evidence. Agreement: 81.4%).
Individuals whose methylation pathways predominate (hypermethylators) create less TGN and more methylated metabolites (MeMP). They therefore have lower thiopurine efficacy and a higher risk of side effects, particularly hepatotoxicity.761 This pattern of metabolism can be picked up as early as 4 weeks after starting the drug (ie, long before therapeutic effect is anticipated) and circumvented by switching to a low-dose thiopurine (25–33% of usual dose) with allopurinol 100 mg co-prescription regimen, avoiding toxicity and increasing efficacy. Allopurinol achieves this optimisation of thiopurines by reducing methylation and increasing levels of the target metabolite, TGN.762 763 The accepted ratio of MeMP to TGN at which a switch is indicated is MeMP:TGN ≥11.764 One randomised study comparing low-dose thiopurine with allopurinol with thiopurine monotherapy showed a higher proportion of patients were able to avoid steroid or biologic on combination treatment: 69.6% vs 34.7%, RR 2.1 (95% CI 1.07 to 4.11).765 Withdrawal rates due to adverse events on combination therapy were 30.4% versus 47.8% in those receiving monotherapy (RR 1.47, 95% CI 0.76 to 2.85). Other uncontrolled series show consistently that adverse effects experienced on monotherapy can frequently be circumvented by low-dose thiopurine with allopurinol,766–769 and clinical responses improved.766 770–772
5.2.2.7 Thiopurine toxicity
Statement 89. We recommend that IBD patients initiating thiopurine or methotrexate therapy should have baseline FBC, U&E and LFT measurement, with monitoring of these bloods at least at weeks 2, 4, 8 and 12, and then at least 3-monthly with monitoring for side effects (GRADE: strong recommendation, low-quality evidence. Agreement: 100%).
TPMT testing will only predict a proportion of early haematological toxicity on thiopurines,737 773 and no current pretreatment test will rule out future biochemical toxicity on a thiopurine. Hence, early intensive monitoring for haematological and biochemical toxicity is recommended in all patients with blood tests for full blood count, renal and liver biochemistry at 2, 4, 8 and 12 weeks of therapy,774 with ongoing 12-weekly blood monitoring as toxicity can occur at any stage during therapy.774 775 Bloods should be repeated 2 weeks after all dose increases. In a Spanish nationwide database study of nearly 4000 patients, the cumulative incidence of thiopurine side effects was 26%. Nausea was seen in 8%, hepatotoxicity in 4%, myelotoxicity in 4% and pancreatitis in 4% (pancreatitis occurring more often in Crohn’s than UC, and more likely if also taking prednisolone).776 While a genetic predictor of thiopurine-induced pancreatitis has recently been discovered (the HLA-DQA1*02:01-HLA-DRB1*07:01 haplotype), routine screening is not considered cost-effective at present.777
In patients with side effects to azathioprine, potential strategies include split dosing, a switch to mercaptopurine778 and use of low-dose thiopurine/allopurinol (as detailed in Section on Low-dose thiopurines with allopurinol 5.2.2.6). The success of such strategies varies between type of adverse reaction, and more details are provided in box 7.
5.2.3 Drug use: methotrexate
Gastrointestinal and liver toxicity of methotrexate is reduced by administration of folic acid, either 1 mg daily or 5 mg weekly, traditionally taken 1 or 2 days after the methotrexate dose.779 780 Methotrexate has comparable safety to thiopurines.781 782 Risk of cirrhosis is much lower than previously thought and routine liver biopsy after prolonged use is not necessary. Abnormalities of liver function can be transitory; in one study of 87 IBD patients (with a cumulative methotrexate dose of 1813 mg) this occurred in 24% of patients treated, but many normalised without stopping methotrexate and only 5% had to stop the drug.783 In this study 17 liver biopsies were performed, none showing advanced liver fibrosis or cirrhosis. Another study of 518 patients on methotrexate for inflammatory disease (24% with Crohn’s) assessed liver fibrosis by transient elastography.784 Six percent (31 patients) had FibroScan results suggesting severe liver fibrosis (4% of the Crohn’s disease patients). Only 13 went on to liver biopsy, with just under half having severe fibrosis confirmed histologically. On multivariable analysis, BMI >28 kg/m2 and alcohol intake >14 drinks per week were independent predictors of FibroScan values >7.9 kPa. Patients with these additional risk factors should be screened using transient elastography. For all patients, methotrexate should be stopped if transaminases exceed twice the upper limit of normal. Pulmonary toxicity in the form of acute interstitial pneumonitis presents with dyspnoea, dry cough and fever, and is rare. Most cases are reversible on withdrawal of methotrexate.781 All patients commencing methotrexate should have a baseline chest x-ray.
5.2.3.1 Methotrexate and pregnancy
Statement 90. We recommend that, due to teratogenic and embryotoxic effects of methotrexate, prior to conception women should discontinue methotrexate for 6 months (GRADE: strong recommendation, low-quality evidence). If patients become pregnant on methotrexate then the drug should be discontinued and high dose folic acid (15 mg daily) provided for at least 6 weeks. We suggest that men taking methotrexate may not need to discontinue treatment prior to conception (GRADE: weak recommendation, low-quality evidence. Agreement: 92.7%).
Methotrexate is teratogenic and should not be given to women of childbearing age without detailed discussion and agreement about the importance of assured contraception during therapy, and for 6 months after stopping the drug. If there are concerns about reliability of adherence to effective contraception, then alternative therapy should be used. Information on 63 pregnancy outcomes of women exposed to low-dose methotrexate in the first trimester reported that 30% underwent termination of pregnancy, and of the remaining women, 25% had miscarriage and 12% of those going to term had a baby with congenital abnormality (including one child with multiple skeletal abnormalities).785
There is no firm evidence to support the recommendation that men should discontinue methotrexate pre-conception. Two cohort studies of men receiving the drug for rheumatoid arthritis are reassuring regarding risk of preterm birth and fetal malformation. In a study of men with immunosuppressive and biological drug therapy for rheumatic diseases (of whom 100 were taking methotrexate), there was no evidence of an increase in adverse pregnancy outcomes.786 A further study of 113 pregnancies where the male partner had taken low-dose methotrexate for rheumatological disorders also showed no increase in risk.787 A Danish nationwide cohort study showed no adverse birth outcomes in children born to 193 men taking methotrexate.788
5.2.4 Drug management: anti-TNF including biosimilars
5.2.4.1 Choice of anti-TNF agent
Data regarding differences in efficacy between available anti-TNF drugs are not available from direct head-to-head trials. Existing trial data are difficult to compare indirectly owing to differences in study design and patient populations. Nevertheless, several systematic reviews and meta-analyses have reported minimal or inconsistent efficacy differences in Crohn’s disease, with possible superiority of infliximab compared with other anti-TNF agents in the induction phase of treatment of UC.161 789–791 No significant differences in safety profile have been reported,792 although the increased immunogenicity of infliximab potentially increases the need for co-prescription of an immunomodulator, with resulting effects on safety.
A retrospective study using USA Medicare data showed no difference between adalimumab and infliximab treatment for Crohn’s disease in the proportion of patients continuing treatment at 6 months, nor in rates of surgery or hospitalisation.793 In a retrospective study of 3205 biologic-naïve patients with Crohn’s disease from a USA national administrative claims database, those who received infliximab had a small but significantly lower risk of Crohn’s disease-related hospitalisation, surgery or need for steroids compared with those started on adalimumab (adjusted HRs of 0.8 (95% CI 0.66 to 0.98), 0.76 (95% CI 0.58 to 0.99) and 0.85 (95% CI 0.75 to 0.96), respectively). The study used propensity scores to match the cases as there were significant differences at baseline between the groups.794
In a nationwide Danish IBD registry-based propensity score-matched cohort study, when used as a first anti-TNF in Crohn’s disease, adalimumab-treated patients had a higher rate of all-cause hospitalisations (HR 1.84, 95% CI 1.18 to 2.85), a trend towards higher UC-related hospitalisation and a higher rate of serious infection requiring hospitalisation (HR 5.11, 95% CI 1.20 to 21.80) relative to infliximab. The risk of abdominal surgery was not different between the two treatment groups.795 In the prospective randomised SWITCH trial 47% of Crohn’s disease patients in remission on standard dose infliximab who were switched to adalimumab 40 mg every other week either required dose escalation or switch back to infliximab to maintain remission.796 Combination infliximab plus azathioprine and adalimumab also seemed to be more effective than certolizumab in inducing remission in a recent network meta-analysis (OR 3.1 (95% CI 1.4 to 7.7) and 2.1 (95% CI 1.0 to 4.6) respectively), although both appeared equivalent in maintaining remission (and both were superior to thiopurine alone).456
In a Swiss study, patients offered a choice between treatments stated that ease of use was the most important consideration with a majority favouring adalimumab, but also cited time required for treatment, time interval between doses, evidence of efficacy and fear of injections as reasons for expressing preference.797 A Korean study cited the presence of a doctor as the reason why a majority favoured infliximab.798 Relative costs and infusion unit availability issues/access should also be considered (see box 2).
5.2.4.2 Biosimilar anti-TNF drugs
Statement 91. We recommend that biosimilar infliximab may be used for IBD patients starting treatment (GRADE: strong recommendation, low-quality evidence). We recommend that patients already on originator infliximab can be switched to biosimilar infliximab if in stable response or remission (GRADE: strong recommendation, moderate-quality evidence. Agreement: 97.7%).
The introduction of biosimilar medicines has introduced competition into the market for biological medicines with significant cost reductions. Biosimilar medicines are approved for use in the EU by the European Medicines Agency on the basis of high similarity of structure, purity and biological activity to the originator biological medicine, with clinical evidence of comparable safety and efficacy for at least one therapeutic indication.799 Based on all the scientific data (comparability studies in quality, non-clinical and clinical areas), extrapolation to other indications (where the drug is believed to have a similar mechanism of action) can then be made for the biosimilar. The European Medicines Agency does not regulate interchangeability, switching or substitution, which is the remit of national bodies. It is recommended that biosimilars are prescribed by brand name to ensure full traceability and accountability. Patients should be fully informed about the biological medicine they are using, particularly if there is a change to a biosimilar from the originator molecule. Automatic substitution is inappropriate, as all changes should be made with the full agreement and supervision of the prescribing physician.800 Extrapolation by indication is likely to be required for biosimilar use in IBD (comparative trials for regulatory purpose have not, to date, been performed in IBD) and should be evaluated by regulators on a case-by-case basis. Switching from originator biological medicine to biosimilar should also remain a clinical decision to be made by the physician and patient on an individual basis supported by the scientific evidence and by national recommendation.801 Currently, scientific evidence is lacking for reverse switching (back from biosimilar to originator), multiple switching and cross-switching.802 The effect on safety, efficacy and immunogenicity is not known and these practices should be avoided unless there is a specific need identified by the treating physician for an individual patient.
Biosimilar infliximab is already in use in IBD, and there is evidence available to support its safety and effectiveness. The NOR-SWITCH investigators studied 482 patients with Crohn’s disease, UC, spondyloarthritis, rheumatoid arthritis, psoriatic arthritis or plaque psoriasis who were randomised to continue originator infliximab or switch to CT-P13 biosimilar infliximab.803 Switching to biosimilar infliximab was non-inferior over 52 weeks with 26% experiencing disease worsening with continuation of originator infliximab versus 30% of those switched to CT-P13. A potential limitation of this study was a selected 15% non-inferiority margin. NOR-SWITCH was not powered to examine non-inferiority in individual disease groups, though the CI was close to inferiority for CT-P13 in Crohn’s disease. Excluding patients who had detectable anti-drug antibodies (ADAs) at baseline, the incidence of ADAs was 7% for infliximab originator and 8% for CT-P13, with no significant difference in immunogenicity. Two single-centre observational studies of switching from Remicade to CT-P13 in Crohn’s disease and UC have also shown good short-term outcomes.804 805 Cohort studies of switching to biosimilar infliximab for psoriasis, ankylosing spondylitis and rheumatoid arthritis have all confirmed comparable efficacy and tolerability following switching.806–809
Biosimilar versions of adalimumab became available in the UK in late 2018. Comparative clinical effectiveness and safety trials against originator adalimumab have been conducted in rheumatoid arthritis and psoriasis. Principles as discussed above should be used in decision-making about the use of all biosimilar adalimumab drugs in IBD. Post-marketing surveillance and outcomes data collected in national registries are essential to look for safety evidence, including immunogenicity, with biosimilar medicines.
5.2.4.3 Assessment after anti-TNF induction therapy
Good Practice Recommendation 15. All IBD patients should be reviewed 2–4 weeks after completing loading doses of anti-TNF therapy to assess response and optimise maintenance dosing based on clinical response and measures such as serum drug and anti-drug antibody concentrations, blood inflammatory markers, faecal biomarkers or endoscopy (Agreement: 82.5%).
Clinical response to anti-TNF agents is seen early in Crohn’s disease and UC. Non-responders to induction therapy seem to have little benefit from sustained treatment, as shown in the ACCENT and CHARM studies.476 486 A clinical assessment should be made 2–4 weeks after loading doses have been given. For those who have responded, dose optimisation is recommended. If a response is unclear, then measurement of biomarkers, serum C-reactive protein and faecal calprotectin, or comparison of disease activity scores or PROMs with baseline values, may be helpful. For those with complete lack of response, treatment should be discontinued and alternatives considered (choosing a different class of therapy). Further data are needed on the use of drug level monitoring during induction to guide therapy. Much of the data on drug levels after induction is at a later time point, such as 14 weeks after starting infliximab in the TAILORIX study (see below).810 Observational data in UC show that higher infliximab drug levels at weeks 2 and 6 during induction therapy are associated with early mucosal healing, but there are no prospective studies using drug levels at these early time points to guide dose adjustment.811
5.2.4.4 Drug levels of infliximab and adalimumab
Trough concentrations during and following induction therapy have been shown to correlate with response to therapy for both infliximab and adalimumab.812 In an analysis of infliximab data from the ACT 1 and ACT 2 UC studies, serum levels at week 8 correlated with clinical response, remission and mucosal healing.250 This is confirmed in many studies, also showing that undetectable serum levels are often associated with anti-drug antibodies and worse clinical outcomes.813–815 The randomised TAILORIX trial assessed use of drug levels in 122 luminal Crohn’s disease patients starting infliximab with an immunomodulator, and did not show benefit for treatment intensification starting at week 14 based on regular clinical assessment combined with drug levels and biomarker measurement when compared with clinical assessment only.810 The TAXIT study recruited IBD patients on stable maintenance infliximab therapy to evaluate trough infliximab levels to guide dosing.816 In the initial phase, all had their dose optimised with a target level of 3–7 µg/mL. Patients with low trough levels had their dose increased. For Crohn’s disease patients there was a corresponding increase in clinical remission. Patients with high trough levels had their dose reduced. Overall this optimisation strategy was shown to be cost-effective. Patients were then randomised to dosing over the following year based on clinical features alone or based on trough levels. There was no difference in remission between the two groups, but there was a lower rate of flare in those randomised to the trough level-based dosing.
As discussed in the Section 4.9.3.1: Infliximab for perianal fistulising disease, higher levels may be required for patients with perianal fistulae.586 Drug levels vary according to the assay used, and consensus has not yet been achieved on the optimal therapeutic ranges. A flow chart for the use of anti-TNF therapeutic drug monitoring is presented in figure 4.

Anti-TNF therapeutic drug monitoring.
5.2.4.5 Primary non-response to anti-TNF therapy
Statement 92. We suggest that treatment options for failure of initial anti-TNF therapy (increase dose, shorten dosage interval, switch to alternative anti-TNF, or switch to different drug class) may be informed by the clinical context and by measurement of serum drug and anti-drug antibody concentrations (GRADE: weak recommendation, low-quality evidence. Agreement: 97.7%).
Treatment failure to anti-TNF therapy should be divided into primary non-response (failure to respond to induction therapy) and secondary loss of response. For patients with primary non-response to one anti-TNF, the likelihood that they will respond to a second is small but is dependent on the clinical context. Switching to a drug that acts through a different mechanism is more likely to be successful. Measuring drug and antibody levels may have a role, with recent evidence suggesting that drug levels in primary non-responders are often lower than in responders,817 and antibody formation can be a significant factor within a few weeks of treatment initiation.
5.2.4.6 Secondary loss of response to anti-TNF therapy
Statement 93. We suggest that patients with secondary loss of response to anti-TNF therapy may have serum drug and anti-drug antibody concentrations measured to inform appropriate changes in treatment (GRADE: weak recommendation, moderate-quality evidence. Agreement: 97.6%).
Secondary loss of response to anti-TNF therapy can occur as a consequence of immune-mediated neutralising antibodies to the drug (although there are likely to be other mechanisms including non-neutralising, drug-clearing antibodies or non-immune-mediated mechanisms). Measurements of drug and antibody levels are helpful in guiding next steps.818 A retrospective analysis of 247 IBD patients with 330 loss of response events (188 to infliximab and 142 to adalimumab) showed that, following loss of response, trough concentration measurements and anti-drug antibodies could inform the likely outcome of interventions. Patients with either adequate drug concentrations (adalimumab >4.5 µg/mL or infliximab >3.8 µg/mL) or positive anti-drug antibodies (adalimumab >4 µg/mL equivalent or infliximab >9 µg/mL equivalent) did better by switching to an alternative anti-TNF or an alternative class of drug, whereas patients with low drug concentration and negative antibodies improved with dose increase.819 A decision analytic model in Crohn’s patients losing responsiveness to infliximab showed that a testing strategy was likely to be cost-effective compared with empiric changes in treatment.820 In a prospective study of IBD patients with secondary loss of response to infliximab, all of whom had a dose increase, mucosal healing occurred in half of patients and was associated with a rise in trough levels.821 In patients losing response to infliximab and manifesting with ‘end of dose’ recurrence of Crohn’s symptoms, drug levels and anti-drug antibody levels should be checked and consideration given to starting concomitant immunomodulator therapy where this is not already being used. To increase the drug levels of infliximab by shortening the infusion interval to 6 weeks may be as effective as shortening to 4 weeks or giving a 10 mg/kg dose.822 Once remission has been recaptured over a period of 3–4 months, it may be possible to reduce the dose or stretch the intervals back out again without losing response. In a further retrospective study in 168 Crohn’s patients losing response, 112 patients were treated with 10 mg/kg 8-weekly and 56 with 5 mg/kg at 4-week intervals. Sustained response was achieved in 50% who received double dose and 39% of those with interval shortening, OR 1.5 (95% CI 0.8 to 2.9).823 Doubling the dose is generally more convenient and cost-effective than interval shortening.
A significant proportion of patients have detectable drug levels and a low titre of anti-drug antibodies. Management in this situation is not clear as antibodies may be transient824 and, as shown in a post-hoc analysis of the TAXIT trial,825 infliximab dose escalation can facilitate an adequate trough drug level and can result in clinical response despite the presence of anti-drug antibodies. Starting the patient on immunomodulator therapy (if they are not already on this) can abolish the antibody response and restore efficacy, particularly if combined with an increase in anti-TNF dose.826
The presence of low drug levels in the presence of high titre antibodies (and perhaps even low titre antibodies in the context of adalimumab) mandates a switch, ideally within class to an alternative anti-TNF therapy, particularly if the patient has previously shown themselves to be anti-TNF responsive over a prolonged period. Of note, individuals who form antibodies to one biological therapy may be more prone to forming them to a second.827 In this context, having a low threshold for combining the second biologic with immunomodulator therapy is logical to reduce the risk of future antibody-mediated loss of response.
Many of the published studies on switching from originator to biosimilar infliximab have measured drug and anti-drug antibody concentrations before switching.803 828 This may identify patients with low drug levels and/or antibodies, who probably should not switch, with a more appropriate action either to withdraw therapy (if in deep remission) or switch to a different drug class.
5.2.4.7 Annual review of patients on biologics therapy
Good Practice Recommendation 16. IBD patients receiving immunomodulators or biologics should have an annual review of treatment, including consideration of response and treatment continuation, optimisation or cessation (Agreement: 97.7%).
National Institute for Health and Care Excellence (NICE) technology appraisals for biological therapies in IBD (infliximab, adalimumab, golimumab, vedolizumab and ustekinumab) recommend annual review.137 829–832 Although there is little evidence to support this, it is sensible to assess the safety and efficacy of long-term treatment with both immunosuppressive and biological drug therapy. Patients may be having their treatment in infusion facilities or at home, and a formal clinical review is necessary to ensure that changing circumstances, adverse effects of treatment, long-term clinical remission or other factors do not make it more appropriate to withdraw treatment or substitute alternative therapy.816
5.2.5 Drug management: vedolizumab and ustekinumab
Statement 94. We suggest that pretreatment screening and blood monitoring of therapy on vedolizumab and ustekinumab should at present follow recommendations for anti-TNF drugs due to insufficient long-term safety data at this time to recommend an alternative algorithm (GRADE: weak recommendation, very low-quality evidence. Agreement: 95.3%).
Vedolizumab and ustekinumab are contraindicated in patients with active TB, sepsis or opportunistic infections, including gut infections such as Clostridium difficile. Pretreatment screening should be undertaken as for anti-TNF treatment. Latent TB should be treated prior to commencing either drug. Patients should be up to date with vaccination prior to starting treatment where possible. Non-live vaccines may be administered during either drug treatment, but not live vaccines. Both drugs should be stopped if severe infection develops.
5.2.5.1 Vedolizumab
Close monitoring for evidence of progressive multifocal leucoencephalopathy (PML) in patients treated with vedolizumab has shown no cause for concern. However, patients should be monitored for and advised to report any neurological symptoms that develop because of the rare occurrence of PML in patients treated with other integrin receptor antagonists in conjunction with systemic immunosuppressive drugs.
Integrated long-term safety data (May 2009 to June 2013) showed that serious C. difficile infections, sepsis or TB occurred in 0.6% of patients and there were no cases of PML.165 833 Other studies show no increase in infection risk.834–836 A meta-analysis of 49 studies of biologics with safety data in IBD did show that there is an increase in risk of opportunistic infections that is no different between anti-TNF and anti-integrin agents. Long-term safety data for vedolizumab over 9 years are reassuring.163 The same study showed very small numbers of malignancies.837 An advantage of the gut-specific immunosuppression of vedolizumab, however, is that it does not alter the immune response to parenterally administered antigens, although it does affect the response to orally administered vaccines.838 There is still uncertainty about the mechanism of action of vedolizumab, with recent data showing that modulation of innate immunity contributes to its therapeutic efficacy.839 Subanalysis and data from the GEMINI studies have shown that the frequency of infusion related reaction (IRR) with vedolizumab is around 5%.840
5.2.5.2 Ustekinumab
Ustekinumab, through inhibition of IL-12 and IL-23, inhibits key molecules in cellular immunity. Although there are no head-to-head data with anti-TNF therapy, safety appears to be very good. Data from dermatological studies (where the drug has been NICE-approved for treatment of psoriasis since 2009) are also reassuring. Analyses of psoriasis registry data show that anti-TNF therapies are associated with a greater risk of serious infection (1.9–2.9/100 patient-years) compared with ustekinumab (0.93/100 patient-years),841although at a lower dose of ustekinumab than used in Crohn’s disease. A further safety review in psoriatic arthritis treatment concluded that the most common events were respiratory tract infections, nasopharyngitis, headache and injection site reactions.842 In 167 Crohn’s patients failing anti-TNF therapy, treated with ustekinumab, a very similar side effect profile occurred, with no malignancy, TB or deaths attributed to the drug. It was noted that 11.4% developed arthralgia,512 but arthralgia was not noted to be more common on active treatment than placebo in the IM-UNITI maintenance trial. Adverse events associated with infusions in the UNITI and IM-UNITI trials occurred in 3.4% of patients.506
5.2.5.3 Extraintestinal manifestations (EIM) of IBD and vedolizumab therapy
There has been interest in the impact of vedolizumab on patients with extraintestinal manifestations (EIMs). The OBSERVIBD GETAID cohort followed 294 patients treated with vedolizumab (173 Crohn’s disease, 121 UC) of whom 49 (16.7%) had EIMs at baseline (47 arthropathy, four skin, and two both joints and skin). At week 54, 44.7% had complete remission of their arthropathy and 75% of their skin EIMs. On multivariable analysis, remission of arthropathy was associated with clinical remission of their luminal disease and with recent onset of arthropathy. However, during follow-up 13.8% developed de novo arthropathy and 4.8% paradoxical skin inflammation.843
5.2.6 Cancer and treatment with biologics
Biologics in the treatment of IBD are not completely contraindicated in patients with prior malignancy, and decisions should be individualised. A delay of at least 2 years after successful cancer eradication is appropriate, and this should be extended to 5 years for those cancers with a high risk of late metastatic spread (including breast, malignant melanoma and renal cell carcinoma).844 Data from the New York Crohn’s and Colitis Organisation for 333 IBD patients with a history of cancer followed up for 5 years did not show any differences in the rate of cancer-free survival between patients treated with anti-TNF therapy, immunomodulators, anti-TNF/thiopurine combination therapy or no immunosuppression.845 Evidence related to malignancy in relation to IBD and its treatment is reviewed in recent ECCO guidance.846
5.2.7 Withdrawal of immunosuppression for patients in sustained remission
5.2.7.1 Stopping thiopurines
Statement 95. We suggest that IBD patients in prolonged remission on thiopurines, and who have mucosal healing, may stop the drug after discussion of risks and benefits and considering patient preference. Reintroduction if relapse occurs is usually successful (GRADE: weak recommendation, low-quality evidence. Agreement: 95.3%).
A recent systematic review summarised the published data on thiopurine withdrawal in patients in clinical remission.192 Relapse rates were higher among patients randomised to withdrawal, and at 12 months ranged from 16.5% to 53% in Crohn’s disease and from 11% to 77% in UC. Fewer studies reported longer term rates: at 5 years ranging from 63% to 85% in Crohn’s disease and 43% to 65% in UC. Two studies reported on the rate of success at reintroducing thiopurines in Crohn’s disease, with rates of 74%194 and 96%,847 with only a single study reporting this outcome in UC with successful reintroduction in 92% of cases.194 The risk of relapse should be weighed against the emerging risks of longer term thiopurine therapy, including infections and cancer. In particular, the absolute risk increase of lymphoma rises markedly with increasing age.848
5.2.7.2 Stopping anti-TNF therapy
Statement 96. We suggest that anti-TNF therapy may be withdrawn in patients with prolonged corticosteroid-free remission and mucosal healing. Retreatment in the event of relapse is usually successful, but there is insufficient evidence about which clinical factors predict relapse after withdrawal and decisions should be individualised (GRADE: weak recommendation, very low-quality evidence. Agreement: 93.2%).
From studies assessing outcomes of stopping therapy after at least 12 months of anti-TNF therapy, the estimated relapse rate at 1 year was 39% for Crohn’s and 35% for UC/IBD-U.849 The estimated relapse rates at 2 years were 54% for Crohn’s disease and 42% for UC/IBD-U. Among patients relapsing and retreated with anti-TNF, the estimated chances of success were 88% for Crohn’s disease and 76% for UC/IBD-U. Various models to predict chance of relapse have been proposed.192 The clinical factors associated with relapse, however, vary between studies.850 Younger age, smoking, longer disease duration, fistulising perianal Crohn’s disease, anaemia, raised CRP and raised faecal calprotectin are linked with increased risk of relapse. Mucosal healing (and in some studies low serum drug levels) are associated with a lower risk of relapse. Patients receiving escalated dosages of anti-TNFs or for the indication of postoperative recurrence in Crohn’s disease had a >75% risk of relapse on drug withdrawal. Persistent abnormalities on MRE in Crohn’s disease patients in endoscopic remission also makes relapse more likely.851 Decisions regarding withdrawal should be taken in the context of the individual patient, their disease history and the consequences of relapse.852 Patient profiles favouring treatment withdrawal include: older patients without previous complications, surgery and with no evidence of active inflammation, those with comorbidities increasing their infection risk, those with undetectable trough drug levels and other practical reasons mitigating against continuing injections or infusions.853 There is no safe minimum period of corticosteroid-free remission, but at least 1–2 years seems reasonable. The concept of cyclical biologics use (stopping when deep remission is established and restarting in the event of pre-clinical relapse) has been introduced, but there is no evidence as yet that this is safe or cost-effective.853 All the published data so far come from prospective and retrospective cohort studies such as the STORI study.854 Data on outcomes after withdrawal of newer biologics are awaited.
5.2.7.3 Monitoring following immunosuppressive and biological therapy withdrawal
Statement 97. We suggest that patients in whom anti-TNF therapy is withdrawn should be observed for evidence of relapse. Monitoring of faecal calprotectin may be helpful in this context as levels may rise before clinical relapse occurs (GRADE: weak recommendation, low-quality evidence. Agreement: 97.9%).
As with stopping thiopurines, faecal calprotectin rises prior to clinical relapse.855 856 A study of serial faecal calprotectin, C-reactive protein, full blood count and protein electrophoresis at 3-month intervals after stopping azathioprine showed that calprotectin was the only predictor of clinical relapse in both Crohn’s disease and UC.857 Serial measurement of faecal calprotectin offers a potential opportunity to escalate therapy prior to the development of symptoms, although prospective evidence to validate increasing therapy in this context is lacking. It should not be measured routinely in all patients, but targeted to those where there are significant anxiety or concerns related to stopping anti-TNF therapy.
5.2.8 Drug management: corticosteroids
5.2.8.1 Overuse of corticosteroids
Statement 98. We recommend that prolonged corticosteroid therapy is harmful and should be minimised by specialist intervention and involvement with the multidisciplinary team to explore other treatment options (GRADE: strong recommendation, moderate-quality evidence. Agreement: 97.8%).
Corticosteroids are effective agents at inducing clinical remission, but do not have a role in preventing relapse.99 858 Steroid dependency is generally defined as an inability to wean below 10 mg of prednisolone or 3 mg of budesonide within 3 months of starting, or disease flare within 3 months of stopping steroids; steroid refractory disease is active disease despite taking up to 1 mg/kg/day of prednisolone for 4 weeks. Steroid excess is considered to be two or more courses of steroid over 1 year. A recent audit found that 14.9% of IBD patients had steroid dependency or excess in the UK, more commonly in UC than Crohn’s disease.448 Prolonged steroid use (often defined as continuous therapy for more than 3 months) is associated with numerous side effects including increased infection risk, osteoporosis, suppression of the hypothalamic-pituitary-adrenal axis, diabetes, weight gain and cardiovascular disease. There is evidence of increased mortality in IBD patients on long-term steroids, with a study in USA Medicare and Medicaid patients showing that prolonged steroid use (more than 3000 mg prednisolone equivalent in 1 year) carries greater mortality (significant for Crohn’s, non-significant for UC) compared with patients starting anti-TNF therapy,859 with data from the TREAT registry also showing that prednisolone use was an independent risk factor for mortality.516 In an audit excessive steroid use was avoidable in nearly half of patients,448 was more likely to be avoided if patients attended a dedicated IBD clinic, and if there was a local multidisciplinary IBD team. Steroid use in the previous year is an important disutility included in the ICHOM dataset,346 and documenting assessment of alternative therapies and discussion with the patient is important for all patients on long-term steroids.
5.2.8.2 Corticosteroid-related bone disease
Good Practice Recommendation 17. Risk factors for osteoporosis in IBD include prolonged corticosteroid use, but general risk factors should also be screened for and corrected, including malnutrition, inflammation, smoking and lack of weight-bearing exercise (Agreement: 100%).
Approximately 35–40% of patients with IBD suffer from osteopenia and 15% from osteoporosis, and both Crohn’s disease and UC patients have increased risk.860–862 Risk factors include uncontrolled inflammation, malabsorption (particularly in Crohn’s disease), weight loss, prolonged or high-dose oral steroid use or lack of physical activity.863–866
5.2.8.3 Calcium and vitamin D supplementation
Statement 99. We recommend that all patients receiving a course of corticosteroids for a disease flare should receive an intake of 800–1000 mg/day calcium and 800 IU/day vitamin D (GRADE: strong recommendation, very low-quality evidence). This can be achieved by administration of oral calcium and vitamin D supplements while on corticosteroids, or vitamin D only if dietary calcium intake is adequate. Lifestyle modification advice including regular physical exercise and smoking cessation should also be provided (Agreement: 90.9%).
For patients who have to receive corticosteroids, other factors should be addressed that have a negative impact on bone mineral density. This includes advice to stop smoking, reduce excess alcohol intake and partake in regular muscle-building and weight-bearing exercise such as weight training or running.860 Vitamin D deficiency is common, and occurs in more than half of patients with UC and Crohn’s disease in the UK and northern Europe.867 868 In older people, there is evidence from a systematic review that vitamin D supplementation with daily dose of 700–800 IU reduces the risk of hip and non-vertebral fractures.869 A study of patients with Crohn’s disease showed that treating their active disease, and supplementing vitamin D with 800 IU and 500–1000 mg calcium daily, resulted in a small increase in bone density over the next 4 years.870 Steroids reduce calcium absorption from the gut and increase urinary losses, leading to secondary hyperparathyroidism which results in bone resorption. A Cochrane review of five trials confirmed that calcium and vitamin D supplementation for all patients treated with steroids prevented bone loss from the lumbar spine and forearm.871 Calcium supplementation may increase cardiovascular risk (particularly if not accompanied by vitamin D supplementation). A Swedish long-term cohort study showed that a total (dietary and supplements) calcium intake greater than 1400 mg daily was associated with increased all-cause mortality (HR 1.4; 95% CI 1.17 to 1.67).872 Calcium supplements should not be given without vitamin D, and treatment with calcium and vitamin D should not therefore continue long term unless dietary calcium intake is less than 800 mg daily. An online calcium calculator can be used to estimate dietary calcium intake (http://www.cgem.ed.ac.uk/research/rheumatological/calcium-calculator/). Vitamin D should be measured and supplemented if deficient, with a high loading dose followed by maintenance.
Statement 100. We recommend that patients starting corticosteroids should be assessed for risk of osteoporosis. Those at high risk should be started on bisphosphonate therapy at the onset of corticosteroid therapy (GRADE: strong recommendation, high-quality evidence), after ensuring adequate calcium intake and supplementing vitamin D (Agreement: 90.7%).
Reduction in bone mineral density and fracture risk are worsened by oral corticosteroid use, and the greatest bone loss occurs in the first 6 months of treatment.873 874 Before starting oral steroids, patients should have their fracture risk assessed as shown in figure 5. For patients aged over 40, the Fracture Risk Assessment Tool (FRAX) can be used to assess the 10 year probability of a major osteoporotic fracture (http://www.shef.ac.uk/FRAX/). Patients with a high FRAX score (score ≥20% major fracture and ≥3% hip fracture), those aged under 40 with risk factors or those receiving prolonged (more than 3 months) or repeated courses of oral corticosteroids should have their bone mineral density assessed by bone densitometry.861 875 Note that FRAX does not discriminate past versus current corticosteroid use, nor does it stratify risk according to doses beyond 7.5 mg, and risk should be adjusted accordingly.876 877 Patients on long-term steroids should have a repeat bone densitometry at 1 year, and if stable, repeated at 2–3-year intervals, but if declining, repeated annually. Women and men aged 70 or more, with past fragility fracture, taking high-dose steroids (7.5 mg or more prednisolone-equivalent), or at high risk based on FRAX score, should be considered for bone-protective therapy at the start of steroid treatment.878 Alendronate or risedronate should be used, unless contra-indicated or not tolerated, in which case intravenous zoledronate or teriparatide should be given. For women of childbearing age requiring bone-protective therapy, if they are taking effective contraception (or not sexually active), oral bisphosphonates are the first-line therapy followed by teriparatide if oral bisphosphonates cannot be used.878 Denusomab and high-dose intravenous bisphosphonates should not be used in this situation due to lack of data on the risk of fetal harm should an unplanned pregnancy occur. There is a lack of safety data on use of denosumab with immunosuppressive therapy, and on all osteoporosis therapies during pregnancy, other than calcium and vitamin D.878

Osteoporosis prevention and management in IBD.
Bisphosphonate or denosumab therapy are associated with the rare adverse effects of osteonecrosis of the jaw or atypical femoral fractures. Current UK guidance for the prevention and treatment of osteoporosis recommends dental examination with preventative dentistry in those with dental disease or other risk factors (eg, use of corticosteroids or smoking).877 These guidelines also encourage patients to maintain good oral hygiene and regular check-ups with reporting of new oral symptoms (eg, dental mobility, pain or swelling) while on therapy.877 Treatment review is recommended to consider stopping bisphosphonate after 5 years (after 3 years for zolendronate) unless patients are aged over 70, have previous hip/vertebral fracture, sustain a fracture during treatment or are continuing ≥7.5 mg prednisolone, in which case treatment may be continued.877 If treatment is discontinued fracture risk should be assessed after a new fracture, or if no new fracture should be assessed after 18 months to 3 years.877
5.2.8.4 Corticosteroid-related adrenal suppression
Good Practice Recommendation 18. Patients receiving prolonged courses of corticosteroids are at risk of adrenal suppression and should have a tapering course if stopping. They should be warned about possible steroid withdrawal syndrome, including non-specific symptoms such as weakness, nausea and arthralgia (Agreement: 97.8%).
Corticosteroid withdrawal syndrome can present with weakness, fatigue, loss of appetite, weight loss, nausea and vomiting, diarrhoea and abdominal pain, and so can mimic the underlying disease. It is under-recognised, occurring in about half of patients tested immediately after withdrawal of medium- or high-dose prednisolone used for long periods.879 Symptoms may be mild, with decompensation only when exposed to stressful situations, or can be severe. Stimulation tests (such as the ACTH test or short synacthen test) are abnormal in 46–100% immediately after stopping, but still abnormal in 26–49% after 1 week, and in a few patients remain abnormal 6–22 months later.880 Neither previous prednisolone dose nor duration are good predictors of the problem, which will occur with rectal-administered as well as oral steroids, and can occur after as little as 4 weeks of treatment. Steroid tapering does not completely prevent its occurrence. There is no optimal test to confirm adrenal suppression in this situation. Steroid dose and duration should be minimised where possible, with slow taper, and awareness when suggestive symptoms occur. Slow tapering of budesonide is not required as there is little or no suppression of the HPA axis.
5.2.8.5 Other metabolic complications of corticosteroids
Good Practice Recommendation 19. Patients on prolonged corticosteroids should have blood pressure, glycaemic control and serum potassium monitored. They should receive vaccinations as for those on immunomodulatory therapy (Agreement: 82.6%).
Before starting oral corticosteroid therapy for 3 months or longer or repeating oral steroids within 6 months of a previous course, record height, weight, blood pressure, full blood count, fasting plasma glucose or HbA1c and lipids. Blood pressure and BMI should be measured at every clinic visit. For patients with dyslipidaemia or a raised cardiovascular risk at initiation, repeat a lipid profile 1 month after initiation and then every 3–6 months. Monitor fasting glucose or HbA1c every 3 months. An annual examination by an ophthalmologist is required for patients with symptoms of cataracts, a personal or family history of open angle glaucoma, diabetes mellitus, high myopia or connective tissue disease (particularly rheumatoid arthritis). Mood disturbance such as depression or sleep disturbance should be questioned at every clinic visit. Steroids may exacerbate the potassium-lowering effects of thiazide or loop diuretics, and potassium should be monitored.875 Avascular necrosis of the femoral head is a serious complication of prolonged steroid use, and if hip pain develops should be considered, and if suspected urgent MRI is recommended along with cessation of steroids. Patients on long-term steroids should be vaccinated as for those on immunosuppressive therapy (see Section 5.2.1.3: Common Disease Considerations, Immunosuppressive therapy, Vaccination).
5.2.8.6 Prevention of Pneumocystis jirovecii infection
Statement 101. We suggest that adult IBD patients on triple immunosuppression and using more than 20 mg prednisolone may be offered prophylactic antibiotics for Pneumocystis jirovecii (co-trimoxazole oral 960 mg three times weekly or 480 mg daily) (GRADE: weak recommendation, very low-quality evidence. Agreement: 85.7%).
Prophylaxis for Pneumocystis jirovecii using co-trimoxazole has been shown to reduce incidence by 91% in a meta-analysis of studies in transplant recipients and haematological malignancy.881 In the Spanish registry ENEIDA study of 571 patients treated with rescue therapy, two developed P. jirovecii pneumonia (PJP) and one died. Both had received double immunosuppression (corticosteroids and azathioprine) and had not received prophylaxis, which was given to all receiving triple immunosuppression. The risk relates as much to use of corticosteroids as to other immunosuppressive drugs.234 A study from the USA showed a low incidence of PJP in IBD patients despite low use of prophylaxis. There were three cases identified among 937 patients with 6066 patient-years follow-up with wide confidence intervals around the risk related to each class of immunosuppressant.882 Overall risk is low. PJP prophylaxis should perhaps be restricted to those on triple therapy taking ≥20 mg prednisolone, particularly those with other risk factors (age, frailty, comorbidity). The optimal dose regimen is unclear, but in adults co-trimoxazole 960 mg three times per week or 480 mg daily are widely used. Stevens–Johnson syndrome is a rare but devastating complication of co-trimoxazole and should be discussed with patients when offering co-trimoxazole therapy.
5.3 Diet and IBD
Good Practice Recommendation 20. IBD patients should be encouraged to eat a varied diet that meets their energy, macro- and micronutrient requirements. All who are at risk of malnutrition should have dietitian or nutrition team review, and where nutritional requirements cannot be met, supplementation with enteral or parenteral nutrition are indicated (Agreement: 100%).
Dietary patterns and food consumption vary hugely across the world and the diet is very different in countries with a high prevalence of IBD compared with countries with a low prevalence. From epidemiological evidence, when people migrate from a country with a low prevalence of IBD to a country with a high prevalence they are at increased risk of developing IBD, thus incriminating environmental changes. Dietary components that have been associated with an increase in the risk of or relapse of IBD include cereals, dietary fibre, sugar, fat, fruit, vegetables and protein.883–887 However, no one dietary component is consistently blamed. Thus, until strong scientific evidence supports a defined diet, patients with IBD should be advised to eat a varied diet to meet their energy and nutrient requirements, including dietary fibre. The diet (box 8) should be based on local healthy eating guidelines and include a wide variety of fruit and vegetables, cereals, grains, nuts and seeds, protein-rich foods with a moderation/reduction of high fat, particularly animal fat, high sugar and processed (cured, salted or smoked) meats. Patients with stricturing Crohn’s disease may need to alter their intake of dietary fibre and fibrous foods for symptomatic management of strictures and may need supplementation with enteral or parenteral nutrition to achieve their energy and nutritional requirements.424 436 Management of short gut or intestinal failure due to Crohn’s disease is covered well elsewhere.888
Practical dietary advice in IBD
In general:
Some dietary components (ie, cereals, dietary fibre, sugar, fat, fruit, vegetables and protein) have been associated with IBD; however, a relapse or ongoing symptoms cannot be attributed to one dietary component
Non-evidence based self-directed exclusion diets are to be discouraged as they can lead to limited diet quality and nutrient deficiency
All IBD patients should be advised to eat a varied diet to meet energy and nutrient requirements, including dietary fibre. The diet should be based on local healthy eating guidelines and include a wide variety of fruit and vegetables, cereals, grains, nuts and seeds, protein-rich foods with a moderation/reduction of high fat, particularly animal fat, high sugar and processed meats
Patients with stricturing Crohn’s disease: consider limiting dietary fibre and fibrous foods. Supplementation with enteral or parenteral nutrition may be required to achieve energy and nutritional requirements
Patients with functional bowel symptoms (in remission/mildly active disease): consider giving dietary advice as for irritable bowel syndrome (eg, low FODMAP diet)
Diet with an ileostomy*
Initial dietary advice: small frequent, nutrient dense meals/snacks and oral nutritional supplements where necessary
Sodium: to prevent dehydration, sprinkle extra salt onto meals; add 0.5−1 teaspoon per day
Potassium: increase intake if serum potassium is low (potassium-rich foods suitable for an ileostomy include bananas, potatoes and potato crisps, spinach, fish, poultry, lean red meat, sweet potato, avocado)
Fibre: a high fibre intake can increase loose stools, flatulence and bloating
Thickening output: bananas, pasta, rice, white bread, mashed potato, marshmallows or jelly
Fluids: avoid chronic dehydration and advise 2–2.5 litres of fluids per day, more during hot weather or exercise. Check urinary sodium to detect dehydration. Be cautious with high intakes of hypotonic (eg, tea, water) and hypertonic (eg, fruit juice) drinks as these can increase stoma output and increase dehydration. Encourage isotonic drinks (eg, Dioralyte, sports drinks) and if ileostomy output exceeds one litre per day recommend oral rehydration solution: 1 litre tap water with six level teaspoons glucose, one level teaspoon salt, half teaspoon sodium bicarbonate or sodium citrate with or without flavouring
1–2 tablets (2–4 mg) loperamide half hr before meals.
Avoid stoma blockages: recommend chewing food thoroughly and advise caution with fruit and vegetable skins, sweetcorn and celery and avoid nuts (smooth nut butters are fine).
Vitamin B12 monitoring.
An ileostomy pathway based on patient education for monitoring fluid balance post discharge reduces readmission rates for dehydration.1287
*Ileostomy diet advice does not apply to patients with short gut, jejunostomy or high-output ileostomy.
5.3.1 Nutritional assessment and monitoring
Good Practice Recommendation 21. Patients with IBD should have an assessment of their general nutritional status and screening for evidence of recent weight loss and/or assessment of malnutrition risk at each clinic appointment and on hospital admissions (Agreement: 95.7%).
Malnutrition is common in IBD and comprises undernutrition and overnutrition. Up to 85% of patients with IBD have undernutrition.889 Unintentional weight loss and low BMI are common in patients with newly diagnosed IBD and during disease relapse. The causes are multifactorial and include suboptimal nutritional intake, alterations in energy/nutrient requirements and metabolism, malabsorption, excessive gastrointestinal losses and medication. Overnutrition occurs in 15–40% of patients with IBD and may in part be due to improved management of IBD and the obesity epidemic.890 891 Thus, nutritional assessment in patients with IBD is crucial to identify and appropriately manage patients with or at risk of malnutrition.
There are limited data on the frequency of routine nutritional assessment in IBD, although inpatients seem to be much more frequently assessed892 than outpatients.436 893
Standard nutritional assessments should assess BMI, recent unintentional weight loss and the nature of disease. However, deficits in body composition, muscle strength and serum micronutrients are common in IBD, and BMI alone cannot detect these. An increase in fat mass and decrease in fat-free mass are often reported and increased intra-abdominal fat (visceral fat) is linked to increased cardiovascular risk, increased surgical complications and hospitalisation.890 A more detailed assessment of nutritional status should also include measurements of body composition (waist circumference (a proxy for visceral adiposity894), tricep skinfold thickness, mid arm muscle circumference), muscle (hand-grip) strength and micronutrient status (dietary intake and serum measurements).895
5.3.2 Blood tests for specific nutritional deficiencies
Statement 102. We recommend that IBD patients who are malnourished or at risk of malnutrition should have relevant screening blood tests to assess for macronutrient and micronutrient deficiencies. This may include measurement of iron stores, vitamin B12, folate, vitamins A, C, D and E, potassium, calcium, magnesium, phosphate, zinc and selenium (GRADE: strong recommendation, very low-quality evidence. Agreement: 93.6%).
Measurement of macronutrient and micronutrient status in IBD is important for ongoing monitoring in patients who have or are at risk of malnutrition; however, interpretation of results can be challenging. Some micronutrients are influenced by disease activity so serum levels should consider C-reactive protein (CRP) when interpreting these micronutrients. A reliable clinical interpretation can be made only if the CRP is <20 mg/L (plasma zinc), <10 mg/L (plasma selenium, vitamin A and vitamin D) or <5 mg/L (vitamin B6 and vitamin C).896 Magnesium deficiency has been reported to occur in 13–88% of patients with IBD,897 but serum magnesium is not an accurate measurement of magnesium status because less than 1% of magnesium stores are in the blood. The remainder is in bone, soft tissue and muscle.898 Magnesium deficiency in IBD is likely to be caused by increased gastrointestinal losses. Symptoms of magnesium deficiency include abdominal cramps, impaired healing, fatigue and bone pain. Magnesium supplementation can be given orally or intravenously, although oral supplementation can worsen diarrhoea. Up to a third of patients with IBD fail to meet the recommended dietary intake for calcium and calcium supplementation should be considered alongside vitamin D supplementation (see Section 5.2.8.3: Common Disease Considerations, Calcium and vitamin D supplementation). Plasma potassium levels should be monitored and supplemented as required. There are existing ECCO guidelines for monitoring and management of iron, vitamin B12 and folate deficiency.899 General advice about iron replacement is shown in box 9.
Iron deficiency anaemia in IBD
A third of patients with active IBD have iron deficiency anaemia
Anaemia causes fatigue, affects quality of life and delays recovery
As systemic inflammation inhibits absorption of iron, iron tablets should not be used in those with active disease and, in patients with inactive disease, no more than 100 mg elemental iron should be taken daily899
Ferritin levels up to 100 µg/L in the presence of inflammation may still reflect iron deficiency.899 Measurement of transferrin saturation may therefore be helpful
Consider other causes of anaemia (eg, folate deficiency, B12 deficiency or bone marrow depression) in patients with IBD
Intravenous iron should be used first line in patients intolerant of oral iron who have active IBD and moderate to severe anaemia (Hb <100 g/L), or those who need erythropoietin899
Iron absorption may be improved by once daily or alternate daily oral dosing1288
5.3.3 Vitamin D
Statement 103. We suggest that vitamin D levels should be measured and deficiency corrected in Crohn’s disease and ulcerative colitis (GRADE: weak recommendation, very low-quality evidence. Agreement: 86.7%).
In a multicultural UK IBD cohort, the prevalence of vitamin D deficiency (<50 nmol/L) was 66% in Crohn’s disease and 69% in UC, and severe vitamin D deficiency was 27% in Crohn’s disease and 36% in UC.867 Median vitamin D levels were lower in black and Asian ethnic groups relative to white subjects, and IBD-related surgery was associated with vitamin D deficiency in the Crohn’s disease group (OR 2.9). A recent Norwegian study reported the prevalence of vitamin D deficiency (25-OH-D concentrations <50 nmol/L) to be 53% in Crohn’s disease and 44% in UC.868 Vitamin D levels in IBD patients are lower than in the general population.900 901 Latitude did not influence the association between IBD and vitamin D.901
In Crohn’s disease patients, vitamin D concentrations were inversely associated with disease activity measured by the Harvey Bradshaw index, and in UC vitamin D deficiency was associated with elevated calprotectin >100 mg/kg. Vitamin D deficiency is associated with low bone mineral density.902 Vitamin D is important in some immune-mediated diseases although its role in IBD inflammation is not fully elucidated.903 Retrospective studies have shown an association between higher levels of vitamin D and remission rates,904 and durability of response to anti-TNF therapy.905 906 It is unclear whether this association is due to confounding by increased disease activity associated with lower vitamin D (although controlled for in these studies).
Limited data exist on the impact of vitamin D supplementation on clinical disease course in IBD. A small double-blind randomised controlled trial of 108 patients with Crohn’s disease treated with 1200 IU daily of oral vitamin D3 or placebo for 1 year just failed to reach significance with 13% in the intervention group versus 29% in the placebo group experiencing a clinical relapse (p=0.06).907 Small uncontrolled studies show that high-dose vitamin D improves clinical indices in Crohn’s disease.908 909 Vitamin D status should be routinely measured in IBD and deficiency should be corrected using oral supplementation, with evidence that this reduces risk of bone disease; but as yet the impact of vitamin D on inflammation in IBD and its impact on disease course, and the optimal vitamin D level as a goal of treatment is poorly understood.
5.3.4 Dietary treatment of functional symptoms in IBD
Statement 104. We suggest that a low FODMAP diet may be used to treat functional bowel symptoms in IBD patients (GRADE: weak recommendation, low-quality evidence. Agreement: 84.4%).
At least a third of patients with inactive IBD have coexisting functional bowel symptoms (eg, abdominal pain, bloating, increased flatulence, diarrhoea and/or constipation) and these symptoms may be mistaken for active IBD.910 Objective markers of disease activity (histological and inflammatory markers (eg, faecal calprotectin, CRP)) alongside clinical symptom assessment help to distinguish between functional bowel symptoms and active IBD. Identification of functional bowel symptoms in inactive IBD is important to avoid unnecessary and potentially harmful treatment strategies. In contrast, active disease should be excluded before establishing that symptoms are functional in nature. From a dietary perspective, identification of dietary triggers is useful but it is often difficult due to diet complexity and a delay in symptom generation following food ingestion. Many patients with IBD alter their diet in an effort to control their symptoms, whether during periods of active disease or during remission.911 Indeed, these self-induced dietary restrictions may be detrimental to patients’ nutritional status, therefore supervision by a dietitian may be required. A diet low in fermentable oligosaccharide, disaccharide, monosaccharide and polyols (FODMAP) has become a recognised successful management strategy for functional bowel disorders like IBS. In IBD, 56% of patients who had previously received low FODMAP dietary advice reported overall symptom improvement.912 Furthermore, in a dietary re-challenge study, FODMAPs (specifically fructans) increased functional bowel symptoms in patients with quiescent IBD.913 In a prospective study of a low FODMAP diet in 88 IBD patients, 78% of patients reported satisfactory relief from their functional bowel symptoms at follow-up compared with only 16% at baseline.914 Mechanisms by which food-related functional symptoms in IBD develop, and which dietary interventions are effective and safe for the management of functional symptoms in inactive IBD, remain unclear.
5.4 Preoperative optimisation
Statement 105. We recommend that IBD patients should have assessment and optimisation of their physical condition prior to elective surgery. This should include appropriate imaging to determine disease extent and complications; radiological drainage of abscesses and treatment of sepsis; correction of anaemia; treatment of malnutrition and physical mobilisation (GRADE: strong recommendation, very low-quality evidence. Agreement: 97.3%).
Despite improvements in medical therapy, the rate of surgery in Crohn’s disease after 5–10 years ranges from approximately 20%–30%.536 915 Postoperative complications are also more common in patients undergoing IBD surgery than operations for other conditions due to the active inflammation, emergency setting, complications and drug treatment.916
5.4.1 Preoperative nutritional status
Statement 106. We recommend that prior to surgery all IBD patients should have their nutritional status assessed and if at risk of malnutrition should receive nutritional support (oral nutritional supplements or enteral or parenteral nutrition if required) (GRADE: strong recommendation, very low-quality evidence. Agreement: 97.3%).
Statement 107. We suggest that patients with penetrating or stricturing Crohn’s disease, or those who are malnourished, may benefit from exclusive or partial enteral nutrition for at least 6 weeks preoperatively (GRADE: weak recommendation, very low-quality evidence. Agreement: 97.2%).
Malnutrition and nutrient deficiencies are common in IBD.917 918 Severe malnutrition (BMI <18.5 kg/m2 and recent weight loss >10% body weight) is associated with a higher risk of postoperative complications, particularly intra-abdominal sepsis919 and increased mortality.920 Poor preoperative nutritional status has been identified as an independent risk factor for postoperative intra-abdominal septic complications (OR 6.23, 95% CI 1.75 to 22.52) in multivariate analysis.921 Thus, all IBD patients undergoing surgery should be assessed for risk of malnutrition. Elective surgery should ideally be postponed until malnutrition is treated. However, in an emergency situation this may not be feasible, and should be considered in the nature of operation undertaken to minimise risk of complications.
5.4.1.1 Evidence for preoperative nutritional support
There are few prospective studies of preoperative nutrition and no prospective randomised trials with a non-nutrition control group. A meta-analysis of pre-surgical nutritional support in gastrointestinal surgery patients found that the provision of 500–1000 kcal of an immune enhancing oral nutritional supplement plus usual food significantly reduced post-surgical complications.922 A more recent systematic review of preoperative nutrition in Crohn’s disease included 14 original studies, but only five prospective studies including one randomised trial.923 Five studies showed significantly reduced complications and infectious episodes in patients receiving preoperative nutritional therapy. Significant heterogeneity was reported between studies in terms of the nutritional supplement used and timing of nutrition. There is sufficient evidence to propose delaying surgery when possible to allow a multimodal approach to management including nutrition, steroid weaning and management of any abscesses.
The European Society of Parenteral and Enteral Nutrition (ESPEN) recommends preoperative nutritional support for 7–10 days in patients who are undergoing major gastrointestinal surgery and are mildly malnourished.924 A longer duration is recommended for severely malnourished patients even if it delays surgery.924 If oral nutritional supplements are not tolerated, then enteral nutrition should be considered and parenteral nutrition should only be used when nutritional targets cannot be delivered by the enteral route.436 924
5.4.2 Preoperative serum albumin
Hypoalbuminaemia (albumin <30 g/L), as a reflection of significant inflammation or secondary to malabsorption, is frequently associated with severe malnutrition although is not in itself a marker of nutritional status.919 This level of hypoalbuminaemia is associated with a higher risk of postoperative intra-abdominal sepsis.925 The evidence to support the use of intravenous albumin is weak919 925 and correction of hypoalbuminaemia hinges on treatment of underlying sepsis and control of inflammation. Nutritional support alone is very unlikely to restore low albumin levels to normal while sepsis and uncontrolled inflammation persist, but feeding is an important supportive measure.926 927
5.4.3 Preoperative anaemia
Preoperative anaemia (Hb <130 g/L in men and <120 g/L in women) increases the risk of postoperative intra-abdominal sepsis, correction of which is associated with improvement in outcomes including risk of intestinal obstruction and haemorrhage, anastomotic leak, postoperative perforation, pulmonary oedema and septic complications such as pneumonia and wound infection.925 928 Perioperative red cell transfusion in patients undergoing ileocaecal resection has been shown to be associated with an increased risk of postoperative complications including an anastomotic leak, ileus, intra-abdominal abscess, wound dehiscence and thrombotic events.929 Anaemia should be recognised and treated early, preferably with oral or intravenous iron and other haematinics as needed, and avoiding blood transfusion where possible.
5.4.4 Preoperative corticosteroids
Statement 108. We recommend that prior to elective surgery for Crohn’s disease or ulcerative colitis, corticosteroids should be stopped or dose minimised wherever possible to reduce risk of postoperative complications (GRADE: strong recommendation, low-quality evidence. Agreement: 94.6%).
Patients undergoing IBD surgery while on corticosteroids have an increased risk of postoperative infectious complications and anastomotic leaks.930–932 There is some evidence that risks are greater for those taking high-dose steroids (40 mg prednisolone or more).932 933 A comparison of prednisolone doses greater than 20 mg versus 20 mg or less did not show a significant difference in risk of infections.931 Use of more than ≥15 mg oral corticosteroid in UC patients within 30 days of IPAA surgery, or more than ≥20 mg in the setting of proctocolectomy, is associated with increased risk of complications.934 935 IBD patients having elective surgery should have their corticosteroids stopped if possible, or brought to as low a dose that can be managed without deterioration.
Statement 109. We recommend that IBD patients who have been on oral corticosteroids for more than 4 weeks prior to surgery should receive an equivalent intravenous dose of hydrocortisone while nil by mouth in the perioperative period (GRADE: strong recommendation, moderate-quality evidence. Agreement: 100%).
Patients who are on corticosteroids at the time of their IBD surgery should be given intravenous hydrocortisone in equivalent dosage until they can resume oral prednisolone.930 Prednisolone 5 mg is equivalent to hydrocortisone 20 mg or methylprednisolone 4 mg. There is no value increasing steroid dosage to cover stress in the perioperative period, as shown in a randomised trial in IBD surgery936 and case series.937 Anaesthetists will generally give a single steroid dose prior to induction (such as dexamethasone 4 mg intravenous or intramuscular) for those taking more than 5 mg prednisolone.938 Patients who are on physiological corticosteroid replacement because of disorders of the hypothalamic pituitary axis (such as oral hydrocortisone 20 mg mane, 10 mg nocte) should receive supplementary doses in the perioperative period.939 For patients who have had complete resection of active disease, it is important to avoid inappropriate prolongation of steroids after surgery, and there is virtue in standardised steroid-taper protocols in the postoperative period, dependent on the dose and duration of steroids preoperatively (table 11).
Postoperative prednisolone tapering
5.4.5 Preoperative thiopurines
With one exception,940 the literature on the use of immunosuppressive therapy (thiopurines and methotrexate) leading up to surgery does not describe an association with an increased risk of postoperative complications.932 933 941
5.4.6 Preoperative anti-TNF therapy
The risk of surgical complications for Crohn’s patients taking anti-TNF therapy during the perioperative period has been assessed in many small observational studies. The majority of systematic reviews and meta-analyses conclude that there is a small increase in risk of infectious complications,257 932 942–945 although one systematic review found no difference.946 This risk is less than that for corticosteroid use,947 and anti-TNF therapy alone does not justify the formation of a diverting stoma. Operative risk should be based on other risk factors including presence of fistulae, abscess, low albumin, anaemia and corticosteroid use in addition to anti-TNF therapy.930 There is evidence in Crohn’s disease that risk is related to anti-TNF drug levels.948 If clinically appropriate, cessation should be 6–8 weeks before surgery for infliximab and 4 weeks for adalimumab, but evidence to support this is lacking. If necessary, treatment should be restarted soon after the patient is well enough to be discharged from hospital. For UC, compared with Crohn’s disease there are fewer data on which to assess risk of anti-TNF therapy and studies have methodological limitations, but two meta-analyses conclude that the postoperative risk is not increased overall.944 949 Anti-TNF therapy for Crohn’s patients should therefore be discontinued where possible prior to elective surgery. If not appropriate to stop, then timing of injections should be arranged to have as long a gap as possible prior to the operation. Stopping anti-TNF therapy prior to UC surgery is less critical.
Statement 110. We recommend that patients with ulcerative colitis should not be considered for pouch surgery while taking corticosteroids (GRADE: strong recommendation, very low-quality evidence. Agreement: 94.1%).
In patients having proctocolectomy, corticosteroids are associated with an increased risk of impaired wound healing and need for re-operation.935 There is no evidence of increased complication risk for patients taking immunomodulators (mercaptopurine, ciclosporin) who have ileoanal pouch surgery950 or IBD surgery generally.941 A two-stage IPAA procedure carries more risk than a three-stage procedure if patients are on anti-TNF therapy.951 Pouch surgery is complex with inherent risks, and it is prudent to conduct a controlled withdrawal of both corticosteroids and anti-TNF as part of a staged approach to pouch formation, which should always be done in an elective setting.
5.4.7 Summary of recommendations for operative optimisation
In elective surgery IBD patients should have their physical condition assessed and optimised prior to surgery. This should include assessment of comorbidities; imaging or endoscopy to document disease extent; drainage of abscesses and treatment of sepsis; assessment and correction of nutritional deficiencies; and stopping corticosteroids and biologics where possible. All IBD patients undergoing surgery should follow an enhanced recovery (ERAS) protocol.436 924 A checklist is shown in box 10.
IBD operative checklist
Before admission:
Notify physicians of planned admission date if elective surgery or notify of emergency admission
Optimise nutrition in weeks prior to elective surgery
Smoking cessation education and support including from general practitioner and community support services
Stoma nurse counselling (where relevant) and appropriate psychological support including peer support
Agree and implement plan regarding medical therapy: minimisation of steroid use; dose optimisation of immunomodulators and biologics prior to and after surgery
Postoperative during inpatient stay:
Dietary assessment and nutritional plan
Tail prednisolone as per table 11.
Consider medical prophylaxis
5.5 Faecal calprotectin
5.5.1 Faecal calprotectin in the differential diagnosis of IBD versus IBS
Statement 111. We recommend that, for patients aged 16–40 presenting in primary care with chronic diarrhoea and symptoms that may be consistent with either IBD or IBS, faecal calprotectin is a useful screening tool with a high negative predictive value. If significantly elevated, patients should have an infective cause excluded and be referred for further investigation (GRADE: strong recommendation, moderate-quality evidence. Agreement: 97.9%).
Faecal calprotectin is a sensitive and specific marker of intestinal inflammation and is a useful non-invasive method to investigate patients with chronic gastrointestinal symptoms in low-risk groups for malignancy, when infection and coeliac disease have been excluded as the cause and symptoms are suspected to be either due to IBD or IBS (figure 6). A normal level has a very high negative predictive value for IBD.952–954 By contrast, the positive predictive value of levels above the assay reference level (normal defined as <50 µg/g stool) is low, and it is recommended that a higher threshold is used to trigger colonoscopy, which improves the positive predictive value with little reduction in the negative predictive value.955 956 Due to the variety of calprotectin assays in commercial use, the exact cut-off prompting colonoscopy should be determined locally, but it is generally between 100 and 250 µg/g stool and should be monitored to ensure appropriate specificity and sensitivity. Used in this way, faecal calprotectin can be used as a cost-effective measure957 to prevent unnecessary colonoscopy in those where IBD is extremely unlikely.958

Use of faecal calprotectin in primary care.
Faecal calprotectin is generally raised in patients with bloody diarrhoea and patients with this presenting feature will need flexible sigmoidoscopy regardless of the calprotectin result. In acute diarrhoea due to infection, calprotectin is also likely to be raised and will not discriminate between IBD and gastroenteritis, thus stool culture and/or flexible sigmoidoscopy or colonoscopy are the appropriate diagnostic investigations. While there is limited evidence to support routine repeat testing, an evaluation of the York Faecal Calprotectin Care Pathway found that, in 243 patients with a faecal calprotectin ≥100 µg/g after a median of 18 (IQR 14–29) days, repeat testing identified a reduction in 53% of patients, either to <100 µg/g or, if initially >250 µg/g, into the 100–250 µg/g range.959
Faecal calprotectin is not sensitive enough in the exclusion of advanced colorectal adenoma or colorectal carcinoma,960 961 and so in patients with rectal bleeding and abdominal pain, change in bowel habit, weight loss, or iron-deficiency anaemia, cancer pathway referral should be strongly considered962 and calprotectin is not appropriate. In primary care, symptoms of change in bowel habit with rectal bleeding and abnormal haematology in patients under 50 years are strongly predictive of IBD or colorectal cancer, but generally do not discriminate between the two.963 IBD is significantly more common in younger age groups, so referral will generally be to medical gastroenterologists. However, if there are reasons to suspect malignancy, patients should be referred via a suspected cancer pathway, although both need rapid colonoscopy (figure 6).962
5.5.1.1 Faecal calprotectin in the assessment of disease activity in known IBD
Statement 112. We suggest that, in IBD patients where it is unclear if symptoms are due to ongoing inflammation or other non-inflammatory causes (such as bile acid malabsorption, functional bowel disorder or short bowel), faecal calprotectin measurement may be used to provide evidence of mucosal inflammation (GRADE: weak recommendation, low-quality evidence. Agreement: 97.8%).
Faecal calprotectin is a useful surrogate marker of inflammatory activity in IBD.964 It correlates well with endoscopic inflammation in UC965 and in Crohn’s disease.966 If it is unclear whether new symptoms represent a relapse or other causes, particularly in Crohn’s disease, then calprotectin is useful to confirm active inflammation and can be a non-invasive alternative to flexible sigmoidoscopy or colonoscopy and cross-sectional imaging. If relapsing disease is clinically obvious, then measurement is not necessary.
A recent meta-analysis including data for 2822 IBD patients and 298 controls found that a calprotectin cut-off of 50 µg/g had the best sensitivity (90.6%) to detect endoscopically active disease, with specificity performing best (78.2%) at levels >100 µg/g.967 A separate meta-analysis has shown that a threshold of 250 µg/g provides better specificity of 82% than thresholds of 100 µg/g and 50 µg/g (specificity of 66% and 60%, respectively) in differentiating active IBD from remission.968 However, a faecal calprotectin of 250 µg/g had a relatively lower sensitivity of 80% compared with a sensitivity of 84% and 92% at cut-offs of 100 µg/g and 50 µg/g, respectively.
5.5.1.2 Use of faecal calprotectin to inform therapy changes
Statement 113. We suggest that faecal calprotectin is a validated biomarker for endoscopic and histological disease activity. It may therefore be a useful non-invasive parameter to inform decisions on treatment escalation or de-escalation (GRADE: weak recommendation, moderate-quality evidence. Agreement: 100%).
There is increasing evidence of the benefits of mucosal healing in reducing future relapse rate.50 52 969 970 Meta-analyses have shown that faecal calprotectin can discriminate between active and inactive IBD, although accuracy is greater for UC than Crohn’s disease.968 971 Studies in UC patients in clinical remission show that calprotectin correlates with endoscopic inflammation,972 and for those with both clinical and endoscopic remission, correlates with histological inflammation.973 A further study showed that calprotectin levels were a better predictor of relapse over the next year than the presence of histological inflammation.974
The information about mucosal inflammation provided by faecal calprotectin levels is a practical means to target increases in drug dosage, and studies are now starting to investigate the value this has in improving long-term outcomes. In UC, patients with clinically inactive disease but raised calprotectin can have levels reduced to those associated with lower risk of relapse by increases in dose.67 In Crohn’s disease the open-label randomised CALM study has shown that calprotectin levels below 250 µg/g stool, CDAI <150, CRP <5 mg/L and no prednisolone can be used as a target, with dose escalation of adalimumab and azathioprine at intervals until these levels are reached.360 At 1 year the ‘treat to target’ group achieved the primary end-point of a colonoscopic CDEIS score <4 without deep ulcers in 45.9%, with only 30.3% of the control group achieving this (p=0.010). Calprotectin may also be useful in predicting the likelihood of future relapse in order to decide who can withdraw therapies. In the STORI study, patients stopping anti-TNF with mucosal healing and a calprotectin ≥300 µg/g had a relapse rate of 30%, but those with both mucosal healing and a lower calprotectin had a relapse rate of between 10% and 20%.854 975 Serial measurement over time can give a more accurate prediction of the likelihood of relapse.976
5.5.2 Collection of faecal calprotectin samples
There remain practical issues around the use of faecal calprotectin. These include variability between different assays, variability in levels in different stool samples from one patient during 1 day, lack of stability for samples kept at room temperature for more than a few days, and variation in calprotectin levels related to the interval between stools being passed.977 978 It is therefore recommended that the first stool passed in the morning is routinely used for sampling, and that this is stored for no more than 3 days at room temperature before analysis.
5.6 Lower GI endoscopy in IBD patients
5.6.1 Flexible sigmoidoscopy and colonoscopy in acute colitis
In the 1970s and 1980s it was recommended that colonoscopy be avoided in severe colitis because of the risk of toxic megacolon or perforation,979–981 or be limited to a flexible sigmoidoscopy without bowel preparation.982 Colonoscopy equipment and technique has changed radically since then, and more recent data suggest that it can be performed safely and provide useful information in acute severe colitis.983 Endoscopic assessment with a limited unprepared sigmoidoscopy and biopsies with minimal air insufflation can be performed safely by an experienced endoscopist.224 In a study of colonoscopy in IBD, complications were no more likely in severe colitis than less active disease, nor did tolerance of the procedure relate to disease activity.984 Retroflexion in the rectum is not recommended in the presence of active colitis due to risk of perforation. In acute severe colitis the inflamed area of rectum and colon are generally free of stool, so it is reasonable to avoid bowel preparation.
5.6.2 Bowel preparation for colonoscopy
High-quality preparation is desirable to allow optimal colonic mucosal visualisation and to facilitate chromo-endoscopy. There are limited studies examining the effectiveness of bowel cleansing in IBD. A prospective observational study in 429 IBD patients showed poorer bowel cleansing quality in comparison to patients attending for investigation of abdominal pain.985 In a study of 100 IBD patients with age- and sex-matched controls, disease activity was not associated with poorer quality bowel preparation according to the Boston Bowel Preparation Scale.986 However, questionnaire assessment during bowel preparation demonstrated that a higher visceral sensitivity index, anxiety and a higher Harvey Bradshaw index was associated with increased abdominal pain and nausea, which in turn led to greater anxiety immediately prior to colonoscopy.986 IBD patients also experience high embarrassment and burden from the bowel cleansing process, and are more likely to find colonoscopy painful.987 Patients may experience an increase in abdominal symptoms suggestive of a flare within 1 month following colonoscopy,983 but no definite correlation to bowel preparation has been reported. As aphthous ulceration has been associated with use of sodium phosphate,988 PEG-based bowel cleansing agents are commonly used in IBD. Low-volume regimens are better tolerated and bowel cleansing is non-inferior to high-volume PEG regimens.989
5.7 Drug treatment adherence
Statement 114. We recommend that IBD patients should be routinely asked about medication adherence because non-adherence is common and results in worse outcomes. Risk factors include young age, psychological distress, patient beliefs and discordance between patient and health professional GRADE: strong recommendation, moderate-quality evidence. Agreement: 100%).
There is no gold standard definition of treatment non-adherence, but patient self-reporting is simple and reasonably accurate.990 Non-adherence is common, occurring in at least a third of IBD patients,991 most frequently for those on 5-ASA drugs.992 Although lower rates are reported with immunosuppressive drug use,993 994 even patients on infliximab have non-adherence rates of 17% and for adalimumab this could be as high as 29%.995
The impact of non-adherence is significant, with increased relapse rates996 and generally worse clinical outcomes.997
Studies have identified numerous factors associated with IBD medication non-adherence. Although there is some heterogeneity across studies, the factors that are most consistently associated with non-adherence include psychological distress, patient beliefs (particularly about the efficacy of the drug or necessity of taking it) and discordance between the health professional and patient.991 995 998 999 Practical barriers to adherence (eg, cost, complex treatment regimens, inconvenience, busy lifestyle, forgetfulness) constitute a major issue for adherence, although patient perception greatly affects what is perceived as a barrier.998
5.7.1 Strategies to improve adherence
Statement 115. We recommend that IBD patients at risk of non-adherence should be offered a variety of means to improve adherence, such as regimen simplification, reminder aids and additional support and education (GRADE: strong recommendation, low-quality evidence. Agreement: 97.8%).
There are few intervention studies evaluating methods of improving non-adherence in IBD. One study evaluated education sessions1000 with a non-significant improvement in adherence. Trials using multicomponent intervention1001 1002 are more successful in improving adherence, with techniques combining education sessions with practical aids. These include regimen simplification, medication reminder charts, weekly or daily electronic pill-box organisers with alarms, or mobile phone alarms.1003 Web-based interventions are also valuable including education about disease and how to manage flares, monitoring using a traffic-light system and access to advice from a health professional by email or phone.1004 Although psychological factors are a significant influence on adherence,1005 there are no intervention studies to date.
5.8 Smoking
All IBD patients should be asked about cigarette smoking. Those who smoke should be advised of the widespread harm to health, and should be advised to stop. They should be offered referral to a smoking cessation service, where they should be offered behavioural therapy (eg, cognitive behavioural therapy) in combination with pharmacotherapy (nicotine replacement, bupropion or varenicline).1006 Bupropion and varenicline should not be given to those under 18 and pregnant women should be advised about risks and benefits of nicotine replacement therapy. Without support, there is a less than 10% likelihood of long-term abstinence in smokers attempting to stop, but these interventions increase success rates substantially.1007 1008
5.8.1 Smoking and Crohn’s disease
Statement 116. We recommend that smokers with Crohn’s disease should be encouraged to stop, as smokers have a higher risk of disease flare, a higher incidence of surgery and a higher risk of postoperative recurrent disease (GRADE: strong recommendation, low-quality evidence. Agreement: 100%).
Cigarette smoking is more common in patients diagnosed with Crohn’s disease.1009 The increase in smoking is more pronounced in those diagnosed at an older age, with one USA study showing a prevalence of smoking of 47% in those diagnosed over age 40 compared with 27% in the background population.1010 Continued smoking results in a worse disease course compared with those who quit or never smokers,1009 1011 a higher risk of surgery and worse outcomes after surgery. A meta-analysis showed a 2.5-fold increase in risk of repeat surgery and a twofold increased risk of clinical recurrence.637 It is of note that smoking makes surgical complications more common after colorectal surgery for any indication.1012 1013 Passive smoking1014 and light smoking (less than 10 per day) are just as bad as heavy smoking.1015 The adverse effects of smoking are more pronounced in women than in men with Crohn’s disease.1016
Efforts to help Crohn’s disease patients quit smoking are therefore important, with evidence that setting up a smoking cessation service is cost-effective with costs paid for by reduced disease management costs.1017 Despite this, there is poor awareness among patients of the benefits of quitting1018 1019 and measures to help patients quit are underused.1020 Benefits of quitting accrue at any stage in the course of Crohn’s disease.1021 When active measures are employed, significant numbers can be helped to stop. The TABACROHN study showed 31% of 408 patients quit initially, with 23% still abstinent after 18 months follow-up.1022
5.8.2 Smoking and UC
Statement 117. Ulcerative colitis patients who continue to smoke cigarettes should be encouraged to stop. There is an increased risk of flare after stopping, and patients should be made aware of this. We suggest that they are informed that an increase in medication may be required to control their disease (GRADE: weak recommendation, very low-quality evidence. Agreement: 95.7%).
UC is more common in non-smokers and is more likely to arise in those who have recently quit smoking.1011 1023 The highest risk period for disease onset is in the first 2–5 years after stopping.1024 Ex-smokers present later in life than never-smokers.1025 1026 UC patients who smoke have reduced colectomy rates, less primary sclerosing cholangitis and less back-wash ileitis than never-smokers.1014 The same study showed higher cigarette consumption was associated with less extensive disease and reduced need for therapy. UC patients who quit smoking have a significantly worse disease course than those who continue, with more corticosteroid and azathioprine use and increased hospitalisation rates.1014 1027 Interestingly, a large study showed that smoking does not reduce the risk of pouchitis after ileal pouch-anal anastomosis for UC, neither smoking at the time of operation nor later.1028 Ex-smokers with refractory UC who resumed smoking (mean 8.6 cigarettes daily) subsequently had high rates of corticosteroid-free remission.1029 In spite of the benefits of smoking in UC, every effort should be made to encourage patients to stop. For patients who do plan to stop, a plan to mitigate the risk of worsening disease by an increase in their treatment should be discussed. Trials of transdermal nicotine therapy in the 1990s showed at best modest benefit in active UC,1030 1031 but maintenance trials were negative,1032 and small trials of enema therapy were shown to be associated with inability to retain the enema in 30%, and side effects of nausea, light-headedness and tremor.1033 There are no trials of nicotine gum use in UC, but case reports show effectiveness in ex-smokers with refractory UC.1034 1035 Electronic cigarettes are now widely used as a cigarette substitute and, by means of a small vaporiser, provide a similar experience to smoking, with nicotine and taste and throat sensations akin to tobacco smoke. There is very little evidence of the effect of e-cigarettes on UC, although a case report surprisingly shows no benefit despite comparable amounts of nicotine.1036 The use of nicotine gum to control UC should only be recommended in refractory disease and as an alternative to resumption of smoking, with full discussion of its addictive nature.
5.9 Psychology and stress
Statement 118. We suggest that in patients with IBD, psychological therapies including cognitive behavioural therapy, hypnotherapy and mindfulness meditation may be offered to interested patients, particularly those with psychological symptoms, as an adjunctive therapy to improve symptom control and quality of life (GRADE: weak recommendation, very low-quality evidence. Agreement: 91.1%).
A study using the UK Health Improvement Network (THIN) showed that patients with depression had a significantly greater risk of developing Crohn’s disease (adjusted HR 2.11, 95% CI 1.65 to 2.70) and UC (adjusted HR 2.23, 95% CI 1.92 to 2.60).1037 In this study treatment with selective serotonin reuptake inhibitors (SSRI) and tricyclic antidepressants (TCA) were protective against Crohn’s disease, whereas mirtazapine, serotonin and norepinephrine reuptake inhibitors, SSRI, serotonin modulators and TCA were protective for UC.
5.9.1 Treatment of anxiety and depression in IBD
Anxiety and depression are common in IBD and are associated with poorer outcomes including the need for hospitalisation.1038–1040 A high proportion of patients with IBD have co-existent symptoms of IBS.1041 1042 Stress can promote a flare of IBD.1043 High quality studies of pharmacological intervention for anxiety or depression are limited and this is an area of research need. Reports of psychological intervention (psychotherapy, patient education and relaxation techniques) have demonstrated a reduction in healthcare utilisation with psychotherapy,1044 and relaxation techniques can reduce anxiety, pain and stress levels while improving quality of life and mood.1045 However, a Cochrane Systematic Review in 2011 revealed high levels of bias within studies and no benefit in health-related quality of life, emotional status or disease remission in adults, with limited benefit noted in adolescents.1046 Conflicting outcomes have been published from studies of small patient numbers regarding the impact of cognitive behavioural therapy on psychological symptoms in IBD.1047–1050 Limited studies on the therapeutic benefit of mindfulness suggest it may be a useful adjunct to pharmacological therapy to improve psychological symptoms in IBD, improve quality of life and to facilitate coping with symptoms during a disease flare.1051–1053 Gut directed hypnotherapy has an established evidence base in IBS, and though it may be useful in symptomatic control in IBD and delay flares in UC, further research is necessary in this area.1054 1055
5.10 Pain and fatigue in IBD
Good Practice Recommendation 22. Patients with IBD and pain should be investigated for stricturing disease, abscesses or uncontrolled inflammation. In the absence of an obvious cause of pain, other factors should be considered including adhesions, visceral hypersensitivity, functional bowel disorder or dysmotility, depression and/or anxiety, sleep disturbance, stress and psychosocial factors (Agreement: 95.7%).
Pain is a common symptom in IBD and may be present in patients with and without evidence of clinical disease activity.1056 1057 Pain in IBD adversely affects quality of life.1058–1060 It is more common in females and in those experiencing stress, anxiety and depression.1061 1062 In Crohn’s disease, pain is more common in smokers and those receiving steroids and antidepressants1063 and narcotics.1064 When inflammation, stricturing disease, abscesses, uncontrolled inflammation or adhesional causes of pain have been excluded, other factors should be considered. In addition to psychosocial factors, causes of pain may include co-existing irritable bowel syndrome,910 1065 1066 visceral hypersensitivity (which may be mediated by microscopic inflammation, including the presence of mast cells),1067 1068 fibromyalgia1069 and bacterial overgrowth.632
5.10.1 Psychological therapy for unexplained pain in IBD
Statement 119. We suggest that psychological interventions may be useful for IBD patients with pain where no physical cause can be found, and may be discussed and offered as adjunctive therapy (GRADE: weak recommendation, very low-quality evidence. Agreement: 93.5%).
Psychological interventions, especially cognitive behavioural therapy, may have a positive impact on depression and improve quality of life in IBD.1070 Due to overlap between diagnoses of IBD and IBS with visceral hypersensitivity, psychological interventions for pain in these conditions may also be efficacious in IBD patients. Relaxation training may improve chronic pain in UC.1045 1071
5.10.2 Opioid medication use in IBD
Good Practice Recommendation 23. Long-term opioid use is associated with poor outcomes in IBD and should be discouraged. Investigation for causes of pain, use of alternative non-opioid drugs and psychological support should be considered (Agreement: 100%).
Opioid medications have analgesic and anti-motility properties. They are more likely to be prescribed to IBD patients than to matched controls.1072 Risk factors for use include female gender, multiple surgeries, severity of pain, higher clinical disease activity, a history of depression or anxiety and polypharmacy, particularly with neuropsychiatric drugs.1073 1074 Patients with sustained poor quality of life have a higher risk of subsequent opioid use and a decreased time to first opioid prescription.1075 Use of narcotics correlates with corticosteroid use in IBD.1076 A Canadian point prevalence study showed that opioid prescribing was highest in the first month following IBD diagnosis where 11% of patients received this class of drug.1077 Prescription was more common in females and in Crohn’s disease relative to UC. Patients with IBD were more likely to become heavy opioid users (defined as a dose exceeding 50 mg of morphine or equivalent per day for at least 30 consecutive days) than age-matched controls. Use of narcotics in both Crohn’s disease and UC is associated with increased prevalence of depressive symptoms,1078 a higher risk of serious infection in IBD516 and increased mortality.516 1077 Historical studies show an association of opioid prescription with development of toxic megacolon in fulminant colitis.1079 1080
5.10.3 Fatigue in IBD
Good Practice Recommendation 24. IBD patients should be asked about symptoms of fatigue, as it is common and often not reported. Fatigue does not necessarily correlate with disease activity and can result in significantly worse quality of life (Agreement: 89.1%).
Fatigue is an increasingly recognised symptom affecting patients with IBD and many other chronic inflammatory disorders. Research into IBD-related fatigue has increased in recent years.1081 IBD patients describe a spectrum of symptoms including tiredness, lethargy and lack of energy that do not subside with rest.1082 Due to a lack of understanding regarding the aetiology and complexity of individual experience of fatigue, many healthcare professionals identify the symptom as of importance but describe difficulty understanding or conceptualising fatigue, thus struggle to assess the severity of fatigue and describe frustration at not being able to adequately improve the symptom for patients.1082 Approximately 50% of patients with IBD report fatigue at the time of diagnosis,1083 and in cohort studies the prevalence of fatigue is between 40% and 72% of IBD patients.1084–1088 Fatigue is associated with poor health-related quality of life,1089 and related factors include poor sleep quality and mental illness.1084 Disability and depression associated with fatigue is equally prevalent between UC and Crohn’s disease.1089 Patients describe a negative impact on social and emotional well-being and a limiting effect on the ability to gain employment.1090 Studies identify active disease or history of surgical resection in Crohn’s disease as a predictor of fatigue.1089 1091 However, fatigue remains very common in patients with inactive disease with a prevalence around 30–50%.1084 1086–1088 1091–1093
5.10.3.1 Investigations and treatment in IBD patients with fatigue
Good Practice Recommendation 25. IBD patients experiencing fatigue should be investigated for subclinical disease activity and other potentially modifiable factors considered such as sleep pattern, medication side effects, anaemia, iron deficiency, electrolyte disturbance, thyroid dysfunction, vitamin D and B12 deficiency and psychological symptoms (Agreement: 93.5%).
A questionnaire study of 631 patients in Europe, North America and Asia Pacific showed that daily fatigue was reported by 53% of IBD patients with anaemia.1094 Anaemia in IBD can be multifactorial including poor oral intake, malabsorption, chronic blood loss or due to chronic inflammation. Vitamin B12 and iron therapy are easily administered treatments that may correct anaemia in IBD patients. A Canadian population-based study found iron deficiency in the absence of anaemia did not contribute to fatigue.1095 However, a recent European study identified iron deficiency as a risk factor for fatigue (OR 2.5, 95% CI 1.2 to 5.1).1096 Muscle fatigue has been associated with low serum vitamin D and magnesium.1097 Other contributing factors should also be considered including pain, sleep disturbance, alcohol misuse and emotional stress. Medications should be reviewed for those that may contribute to fatigue. Corticosteroids have been demonstrated as a determinant of fatigue,1085 although this may be a reflection of disease severity as opposed to a medication side effect. Avoidance of steroids and cessation of immunomodulatory therapy in Crohn’s disease were predictors of improved physical and cognitive fatigue, respectively, in a longitudinal study.1084 Recent data have demonstrated higher circulating frequencies of memory T-cells in fatigued patients with IBD.1098 Whole blood stimulation demonstrated higher production of the Th1 cytokines TNF-alpha and IFN-gamma. Anti-TNF therapy with either infliximab or adalimumab has been shown to reduce the symptoms of fatigue.1099–1101
5.10.3.2 Non-pharmacological therapy for fatigue in IBD
Statement 120. We suggest that IBD patients with disabling fatigue in whom no correctable metabolic deficiency or active disease is found, or where fatigue persists despite addressing these factors, may be directed to non-pharmacological therapies. Patients may be interested in supportive psychotherapy, stress management or graded exercise (GRADE: weak recommendation, low-quality evidence. Agreement: 89.1%).
A randomised controlled trial of solution-focused therapy for fatigue in quiescent IBD for 3 months showed a reduction in fatigue for up to 3 months following completion of therapy.1102 However, the effect was lost by 6 months post therapy. A further randomised controlled trial of 45 Crohn’s disease patients compared professionally-led stress management versus self-directed self-management versus conventional therapy. After eight sessions, a non- significant trend to reduced tiredness was observed.1103 A longitudinal study has shown a positive effect of regular exercise on physical fatigue in IBD.1084
5.11 IBD-associated arthropathy
Statement 121. We recommend that the mainstay of symptom relief for IBD-associated arthropathy which is related to IBD activity should be through control of intestinal inflammation, physiotherapy and simple analgesia (GRADE: strong recommendation, very low-quality evidence. Agreement: 100%).
Statement 122. We recommend that for IBD-related arthropathy which is not related to IBD activity, rheumatology referral, physiotherapy and simple analgesia should be offered (GRADE: strong recommendation, very low-quality evidence. Agreement: 93.6%).
Statement 123. We suggest that short-term use of NSAIDs is safe if IBD is in remission, but long-term use or use in active disease carries more risk of worsening IBD symptoms. There is no high-quality evidence that COX-2 inhibitors are safer than non-selective agents (GRADE: weak recommendation, very low-quality evidence. Agreement: 81.4%).
5.11.1 Treatment of type 1 arthropathy
The natural history and clinical features of IBD-related arthropathies are described in the 2016 ECCO guidelines on extraintestinal manifestations of IBDe.1104 In patients with type one peripheral arthropathy, (joint pain with swelling or effusion, often asymmetric, affecting less than five joints, mainly weight-bearing lower limb joints)1105, inflammation is usually associated with flares of IBD, and responds well to treatment of the underlying disease. Local injection of corticosteroids may be required if symptoms don’t resolve rapidly. A small proportion will go on to have more persistent problems, which may require sulfasalazine, methotrexate, or anti-TNF therapy.
5.11.2 Treatment of type two arthropathy
Type two arthropathy (more than five joints, symmetrical distribution and mainly upper limbs) is usually independent of gut inflammation, and symptoms are more persistent. Referral to a rheumatologist is helpful for consideration of immunomodulator or biological therapy, and it is important to discriminate between the other causes of joint pain which can include non-specific arthralgia, osteonecrosis, lupus-like syndrome in relation to anti-TNF therapy, and corticosteroid withdrawal arthralgia. Azathioprine-related arthralgia usually occurs early in treatment and resolves rapidly on stopping the drug. The axial spondyloarthropathy has a much more disabling long-term course, and early diagnosis is vital, but can be very delayed.1106 Low back pain in young people (under 45 years), for more than 3 months that is improved with exercise and not relieved by rest, pain that is worse in the latter part of the night, and morning stiffness lasting more than 30 min, should trigger investigation with MRI scanning (sagittal images of cervicothoracic and thoracolumbar regions with T1 and STIR images, and coronal/oblique sacroiliac joints with T1 and STIR) and referral to a rheumatologist, as plain radiology of the spine and sacroiliac joints will miss most early disease. HLA-B27 is less often positive in IBD-associated axial arthropathy. Specialist assessment and physiotherapy can prevent long-term disability,1107 and initial treatment is with NSAIDs, early progression to treatment with anti-TNF agents often being necessary, as sulfasalazine and methotrexate are not effective.1108 1109 Simple analgesia is preferable to NSAIDs, but NSAIDs are more effective.
5.11.3 Safety of NSAID use in IBD
Data on non-selective NSAIDs is conflicting. A long-term study in over 600 IBD patients showed that low-dose NSAIDs were safe, but standard doses caused a rise in disease activity scores (particularly in Crohn’s colitis), but not relapse.1110 Short-term use is safe, particularly using low doses where the IBD is well-controlled, with a relapse risk of about 20%.1111 1112 A meta-analysis of seven studies of selective COX-2 inhibitors in IBD showed a risk of flare of 14% (95% CI 6.7 to 24.4) with no difference to placebo (relative risk 0.86, 95% CI 0.39 to 1.88)),1113 in keeping with a Cochrane analysis.1114 The risk of flare could be higher when given to patients with active IBD, as COX-2 is important in intestinal repair mechanisms.
5.12 Other IBD therapy
5.12.1 Probiotics, prebiotics and synbiotics in IBD
A systematic review assessed 21 studies in UC.1115 Nine were trials of induction therapy (seven using probiotics and one each prebiotic and synbiotics). The majority assessed the addition of the investigational treatment alongside standard therapy (mostly 5-ASA), with standard therapy alone being used in the control group. Study quality was variable, many being small trials, but overall the majority showed benefit, with statistical significance in 16 of the studies. The largest studies used a mixture containing eight probiotic organisms and overall there is evidence of benefit for this treatment in UC as an addition to standard therapy, with insufficient evidence to recommend other agents. A Cochrane review of probiotics in induction therapy published in 2007 (and so not including the largest studies reported in the systematic review) concluded that there was insufficient evidence to recommend probiotic therapy in induction of remission, but that it may improve symptoms in mild to moderate colitis.1116 The remaining trials evaluated maintenance therapy, some with remission induction followed by maintenance therapy. There was a modest benefit in a number of studies, and some showed equivalence to 5-ASA therapy. A variety of agents were used in these studies. Again, a Cochrane review in 2011 concluded that there is insufficient high quality evidence to show benefit in maintaining remission.1117 One study comparing a prebiotic, a probiotic and a synbiotic in UC using quality of life as an end-point concluded that synbiotic therapy was more effective than the other treatments.1118 In conclusion, probiotic therapy may have modest benefits in UC, but should not be routinely used. By contrast to UC, there is no evidence of any benefit in the current literature for these treatments in Crohn’s disease.1115
5.12.2 Faecal microbial transplantation
Statement 124. We suggest that faecal microbiota transplantation (FMT) shows some evidence of benefit in ulcerative colitis and should be used in the context of clinical trials until further high-quality evidence clarifies the potential for benefit and optimal administration protocol (GRADE: weak recommendation, moderate-quality evidence. Agreement: 93.3%).
To date there have been four randomised placebo-controlled trials of faecal microbiota transplantation (FMT) for the treatment of UC, with three meeting their primary end-point showing a significant improvement in remission compared with placebo.1119–1122 An open-label study showed that benefit is more evident in UC than Crohn’s disease.1123 The published trials vary greatly in route and frequency of FMT administration,1124 with evidence that improved microbial diversity can persist for 4–8 weeks,1119 1125 but does not persist after 1 year,1119 and growing evidence that colonic rather than nasoduodenal administration may be safer and more effective.1126 In spite of these encouraging data, FMT remains an investigational treatment for use only in clinical trials in IBD.1127
5.12.3 Complementary and alternative therapy for IBD
Complementary and alternative medicines (CAMs) include diverse medical and healthcare strategies which are considered to fall outside conventional treatment. Such interventions include herbal treatments, pre/probiotics, acupuncture and are often part of traditional Chinese medicine. There is evidence that 30–50% of patients with IBD use CAMs and this tends to be higher in women than men.1128 1129 While there is no evidence to recommend the routine use of CAMs, certain agents have shown early promising signals in pilot studies. Two promising candidates are curcumin, which is the active ingredient of turmeric (Curcuma longa)1130–1132 and fish oils, where there is good evidence of anti-inflammatory effects, but the largest and most rigorous trial (in Crohn’s disease) showed no benefit.1133 No recommendations can be made due to lack of sufficient high-quality evidence regarding efficacy and dose and larger studies are needed. Helminth therapy remains interesting despite the negative result of a randomised controlled trial in UC.1134 The results of a similar trial in Crohn’s disease remain to be reported. Anecdotal evidence supports the use of acupuncture although there are no controlled trials and, in this case, blinding is an obvious problem. Moderate exercise has shown no harm in IBD and a positive benefit in terms of bone health.1135
Further data are required to move promising CAMs into the category of conventional treatment.1136 Despite the absence of robust evidence supporting the use of CAMs in IBD, there is evidence that many patients use CAMs.1128 It is good practice to enquire about the use of CAMs as patients are often either reluctant to mention this, given the negative social and legal connotations associated with cannabis for example,1137 or may not realise that they are worth mentioning (eg, acupuncture, herbal supplements, exercise). It should be emphasised that they should continue conventional treatments of proven value even if they choose to use CAMs in addition.
5.12.3.1 Cannabis extracts
There is increasing interest in use of cannabidiol (CBD) in medicine. This does not have the psychotropic effects of the delta9-tetrahydrocannabionol (THC) component in cannabis. CBD can have beneficial effects in the gut including reduction in nausea, reduced gastric acid secretion, anti-inflammatory effects and reduction in intestinal motility. Cannabis use has been reported to improve IBD symptoms,1138 and many patients claim that it has beneficial effects.1139 A small double-blind randomised trial in 60 patients compared an oral CBD-rich botanical extract with placebo in mild-moderate active UC. At 10 weeks, the primary end-point of remission was achieved in 28% on CBD versus 26% on placebo (non-significant). The treatment caused side effects of dizziness and somnolence (likely due to the residual THC content of the botanical extract). There was some evidence of symptom improvement in the per protocol analysis.1140 A previous small randomised double-blind study in 21 Crohn’s disease patients compared smoking two marijuana cigarettes (containing 115 mg of THC) to a cannabis flower extract without THC over 8 weeks. The primary end-point of clinical remission was met in 45% on active treatment compared with 10% on placebo, but the difference was not significant.1141 Further adequately powered studies are needed, with rigorous blinding, and objective measures of inflammation as well as symptoms.
5.13 Chemoprevention and colorectal cancer surveillance
IBD is a widely accepted risk factor for the development of colorectal cancer (CRC). CRC accounts for one in six deaths in UC,1142 with median age younger than that of sporadic CRC.1143 There is a wealth of data from large national and international population-based studies demonstrating increased risk of CRC with UC, and CRC or small bowel neoplasia with Crohn’s disease.1144–1146 A case–control study of 68 cases and 136 controls showed that the severity of inflammation, both endoscopic and histological, determines the risk of colorectal neoplasia in UC.1147 This has been supported by a cohort study demonstrating that histological inflammation predisposes to advanced neoplasia.1148 Case–control studies have shown that the presence of post-inflammatory polyps, as a marker of previous severe inflammation, increase the risk of CRC in UC.28 1149 1150 However, a recently published retrospective multicentre cohort study including 462 patients with post-inflammatory polyps confirmed their association with greater severity and extent of colonic inflammation and colectomy risk but did not observe an association with colorectal neoplasia.1151 Finally, the age of onset at diagnosis and the influence therefore of the length of disease in individuals (as stratified by phenotypic classification systems) must be considered as important factors for surveillance, given the association between length of disease duration and the development of cancer.1144 1152
5.13.1 Surveillance ileocolonoscopy
Statement 125. We recommend that IBD patients with colonic disease should be offered ileocolonoscopy 8 years after symptom onset to screen for neoplasia, to determine disease extent and decide on the frequency of ongoing surveillance (GRADE: strong recommendation, very low-quality evidence. Agreement: 89.1%).
Long duration of disease increases the risk of developing IBD-associated CRC, with the risk starting to increase at about 10 years after diagnosis, by which time meta-analysis suggests the incidence is 2–3%.1143 1153 Later studies have shown the cumulative incidence to be 1% at 10 years, 3% at 20 years and 7% at 30 years.1154 This change over time may reflect the increased implementation of surveillance strategies, the introduction of drugs that control inflammation more effectively, or the changing approach to maintenance therapy or colectomy.1155 Current UK, European and USA endoscopy guidance suggests commencement of surveillance endoscopy for dysplasia in IBD should begin at between 6 and 10 years following diagnosis.1156–1158 A Cochrane review1159 evaluated three UC case–control studies1160–1162 and concluded there was evidence for surveillance resulting in earlier detection stage and better prognosis, with indirect evidence of cost-effectiveness. A study of 149 IBD-associated cancers (59 Crohn’s disease, 90 UC) showed that those with prior surveillance had greater 5-year survival and earlier tumour stage at detection.1163 A review of the St Mark’s programme showed surveillance may reduce the risk of advanced and interval colorectal cancer incidence.1164 Those with extensive disease carry the highest risk of colorectal cancer, whereas left-sided colitis patients have an intermediate risk and those with proctitis only have no increased risk.1165 Extent therefore should determine the appropriate surveillance interval. Patients with primary sclerosing cholangitis (PSC) should have annual surveillance colonoscopy from diagnosis.1166 For all other patients, surveillance should begin 8 years after diagnosis, or after the onset of symptoms if there was a significant delay before diagnosis. Surveillance technique, including use of chromoendoscopy, is set out in the SCENIC consensus guidelines,1167 and the surveillance interval after the initial surveillance should be determined according to degree of inflammation, extent, presence of post-inflammatory polyps or strictures, dysplasia, PSC or family history of colorectal cancer under the age of 50 years.1155 1156 Patients with proctitis and no evidence of proximal progression do not require ongoing surveillance colonoscopy. A summary adapted from the 2010 BSG and 2015 SCENIC guidance is presented in box 11.
Colonoscopy surveillance in patients with IBD to detect and manage dysplasia/neoplasia
Commencement of colonoscopy surveillance:
8 years after IBD symptom onset
From diagnosis if primary sclerosing cholangitis
Next surveillance interval (summary of 2010 BSG update guidance)*:1156
Lower risk: next surveillance in 5 years if extensive colitis with no active endoscopic or histological inflammation or left sided colitis or Crohn’s colitis affecting <50% of colon
Intermediate risk: next surveillance in 3 years if extensive colitis with mildly active endoscopic or histological inflammation or post-inflammatory polyps (often termed ‘pseudopolyps’) or family history of colorectal cancer in first degree relative aged ≥50 years
Higher risk: next surveillance in 1 year if extensive colitis with moderate/severely active endoscopic or histological inflammation or if stricture or dysplasia in last 5 years or primary sclerosing cholangitis (including post-orthotopic liver transplant) or family history of colorectal cancer in first degree relative aged <50 years
In determining next surveillance interval, consider patient preference, presence of multiple post-inflammatory polyps, age and comorbidity, accuracy and completeness of examination. If previous colectomy and ileostomy, or colectomy and ileorectal anastomosis: retained rectum should have surveillance examination. Retained rectum after surgery is more difficult to inspect and so proctectomy with/without pouch reconstruction should normally be considered.
Methods of detection*:
Surveillance should be performed where possible during disease remission, though may not be possible in some patients, and chronic active disease is a risk factor for dysplasia.
Statements published as part of 2015 SCENIC international consensus:1167
When performing surveillance with white-light colonoscopy, high definition is recommended rather than standard definition (strong recommendation, low-quality evidence)
When performing surveillance with standard-definition colonoscopy, chromoendoscopy is recommended rather than white-light colonoscopy (strong recommendation, moderate-quality evidence)
When performing surveillance with high-definition colonoscopy, chromoendoscopy is suggested rather than white-light colonoscopy (conditional recommendation, low-quality evidence)
When performing surveillance with standard-definition colonoscopy, narrow-band imaging is not suggested in place of white-light colonoscopy (conditional recommendation, low-quality evidence).
When performing surveillance with high-definition colonoscopy, narrow-band imaging is not suggested in place of white-light colonoscopy (conditional recommendation, moderate-quality evidence).
When performing surveillance with image-enhanced high-definition colonoscopy, narrow-band imaging is not suggested in place of chromoendoscopy (conditional recommendation, moderate-quality evidence).
Colonoscopically targeted biopsies are recommended over random colonic biopsies.1289 If taking random biopsies, 2–4 biopsies should be taken every 10 cm.1156
Management of dysplasia*:
Statements published as part of 2015 SCENIC international consensus:1167
After complete removal of endoscopically resectable polypoid dysplastic lesions, surveillance colonoscopy is recommended rather than colectomy (strong recommendation, very-low quality evidence).
After complete removal of endoscopically resectable non-polypoid dysplastic lesions, surveillance colonoscopy is suggested rather than colectomy (conditional recommendation, very-low quality evidence).
For patients with endoscopically invisible dysplasia (confirmed by a GI pathologist), referral is suggested to an endoscopist with expertise in IBD surveillance using chromoendoscopy with high-definition colonoscopy (conditional recommendation, very low-quality evidence).
If dysplastic lesions cannot be resected completely due to extent or multiplicity, referral to MDT for discussion regarding definitive management including surgical options should be arranged.
*Neither extensive systematic review nor consensus voting has been undertaken as part of the current guideline development process regarding subsequent surveillance intervals after initial surveillance colonoscopy, or methods to detect dysplasia. Instead a summary is adapted/reproduced from the 2010 BSG1156 and 2015 SCENIC1167 guidance.
5.13.2 IBD-related cancer chemoprevention with mesalazine
Statement 126. We recommend that patients with ulcerative colitis or IBD-U with left-sided or more extensive disease should be advised to take mesalazine in doses of at least 2 g daily to reduce risk of colorectal cancer (GRADE: strong recommendation, moderate-quality evidence. Agreement: 95.5%).
Although there is a lack of randomised prospective data regarding chemoprevention of CRC in IBD, a number of studies have shown a protective effect of 5-ASA on the risk of IBD-associated CRC. A systematic review suggests the drug has multiple biological effects that protect against neoplasia.1168 These include stabilisation of cell cycle regulation, scavenging of reactive oxygen or nitrogen species, inhibition of TNFα, NF-κB and TGFβ pathways, interference with Wnt/beta-catenin signalling and antimicrobial activity. A systematic review and meta-analysis of eight studies contained 867 cases of colorectal neoplasia and 143 of non-cancer dysplasia. Prescription of 5-ASA is associated with OR of 0.6 (95% CI 0.4 to 0.9, p=0.04) for development of CRC,1169 although the advantage was only seen in studies from referral centres, not population-based studies.
Two more recent meta-analyses have been published in 2017, confirming that 5-ASA reduces the risk of CRC in UC.1170 1171 Sulfasalazine was not protective. A dose-dependent protective effect was noted with 5-ASA with a minimum dose of 1.2 g1169 or 2 g.1171 It remains unclear whether the protective effect of 5-ASA simply represents more effective mucosal healing rather than a specific drug effect. In patients who are also taking immunosuppressive drug therapy there are no data to show that 5-ASA has additional benefits, whereas a recent retrospective study demonstrated that stopping 5-ASA in patients on anti-TNF therapy was not associated with a worse disease course.1172
5.13.3 IBD-related cancer chemoprevention with thiopurines
Statement 127. We suggest that thiopurines may reduce risk of colorectal cancer in patients with ulcerative colitis and IBD-U, but evidence for a chemopreventative role from methotrexate, calcineurin inhibitors, anti-TNF and anti-integrin agents is lacking at present and they cannot be currently recommended solely for chemoprevention against colorectal cancer (GRADE: weak recommendation, low-quality evidence. Agreement: 93%).
Inflammation may in part promote tumorigenesis,1173 so understanding the impact of immune-modifying therapy on cancer development is an important area of unmet clinical need. There are currently no randomised prospective data interrogating the effect of immunomodulatory agents (including thiopurines, methotrexate, calcineurin inhibitors, anti-TNF and anti-integrin agents) on the risk of IBD-associated CRC, and evidence is based on cohort studies.1165 1174 1175 A recent meta-analysis from 2017 of 24 studies including 76 999 patients concluded there was evidence of a protective role of thiopurines in high-grade dysplasia and CRC prevention in UC, but not Crohn’s disease.1176 Potential benefit in reducing colorectal cancer risk must be weighed against the very small increase in risk of lymphoma, particularly in older patients.
There are no randomised prospective data on the effect of folic acid or antioxidants (vitamin A, C, E, selenium and beta-carotene) on the risk of CRC in IBD. Red blood cell folate is reduced in IBD patients who develop CRC compared with those who do not.1177 Two case–control studies have shown a non-significant dose-dependent reduction in CRC with folic acid supplementation.1178 1179
5.14 Anti-TNF, vedolizumab, ustekinumab and tofacitinib therapy during pregnancy
5.14.1 Fetal and infant exposure to anti-TNF drugs
Statement 128. IBD patients receiving anti-TNF therapy should be counselled about the risks and benefits of continuing treatment throughout pregnancy. We suggest that, for patients with active disease or a high risk of relapse, it may be advisable to continue the drug throughout, while for those with inactive disease who wish to discontinue therapy it may be reasonable to stop at the start of the third trimester (GRADE: weak recommendation, very low-quality evidence. Agreement: 97.7%).
Active transfer of IgG from the maternal to fetal circulation occurs at the surface of the syncytiotrophoblast placental layer through the selective binding of the Fc gamma portion of the maternal IgG antibody to the fetal circulation.1180 Active transport of IgG starts at approximately week 13 of gestation progressing continually until delivery with a preferential transport of IgG1 followed by IgG4, IgG3 and then IgG2.1180 1181 Infliximab, adalimumab and golimumab are IgG1 monoclonal antibodies, whereas certolizumab is a Fab fragment of IgG1 (without the Fc portion of IgG1) and so there is significantly less transfer through the placenta. Infliximab levels were detectable for up to 7 months and adalimumab levels remained detectable for up to 11 weeks from birth.1181 The use of infliximab and adalimumab during pregnancy has been associated with fetal and cord blood levels of drug up to fourfold higher than in maternal blood.1181–1183 A recent study showed that median cord blood drug concentrations were more than the median maternal drug concentrations at the time of birth for infliximab and adalimumab, with a much longer time for drug clearance in infants with the mean time for drug clearance of 7.3 months for infliximab (95% CI 6.2 to 8.3) and 4 months (95% CI 2.9 to 5.0), respectively (p<0.0001).1184 In some infants, drugs remained detectable until 12 months of age.
Discontinuing anti-TNF therapy in the second trimester will limit drug exposure during the time of highest transmission of immunoglobulins from the mother to the fetus. Although the timing of the last anti-TNF administration appears to correlate with maternal serum and cord blood levels, this is not so in a linear fashion with variability due to differences in maternal dose and interval, individual pharmacokinetics and the immaturity of the newborn reticuloendothelial system. There is more variability for infliximab levels than for adalimumab in maternal blood during pregnancy.1185 This may suggest a role for therapeutic drug monitoring while using infliximab in pregnancy.
While low levels of infliximab, adalimumab, certolizumab, natalizumab and ustekinumab can be detected in breast milk from mothers receiving these biologics, breastfed infants of mothers receiving biologics, immunosuppressants or combination therapy have similar risks of infection and similar milestone achievement at 12 months to non-breastfed infants or infants unexposed to these drugs.1186
5.14.2 Cessation of anti-TNF therapy in the second trimester in quiescent IBD
Active IBD prior to conception is associated with poor pregnancy outcomes, including premature delivery, low birth weight and higher spontaneous abortion, compared with quiescent or controlled disease.1187–1190 Discontinuing anti-TNF therapy during pregnancy, in order to minimise exposure to the fetus, is feasible if there is no significant increase in the risk of disease flare. Case–control and cohort studies of pregnancy in women with quiescent IBD do not show any increase in risk of flare if anti-TNF therapy is stopped at week 25–30.1182 1191 Anti-TNF medications therefore may be safely discontinued in the second trimester in women with quiescent disease.
5.14.3 Continuation throughout pregnancy in IBD patients at high risk of flare
A Danish study of 219 women with IBD treated in the third trimester with anti-TNF therapy revealed no increased risk of low birth weight or preterm birth associated with the drug.1192 The same group found that, in women with moderate to severe IBD on anti-TNF during pregnancy, 66% experienced disease activity during their pregnancy. Disease activity was associated with low birth weight (OR 2.05) and preterm birth (OR 2.64, increasing to an OR of 3.6 in moderate to severe disease).1192 There is also evidence that discontinuation of therapy may be associated with a risk of relapse during pregnancy and in the postpartum period.1181–1184 Additionally, low trough levels may lead to anti-drug antibody formation with subsequent loss of response to treatment.
5.14.4 Risk to the fetus of continuing anti-TNF until delivery
A recent UK study of 364 363 singleton pregnancies including 1969 in women with IBD revealed only a small increased risk of preterm birth, and in Crohn’s disease a higher risk of low birth weight or post-partum haemorrhage.1193 Most women with IBD will have an uncomplicated pregnancy. Despite significant fetal exposure to anti-TNF drugs, there is no evidence that continuing anti-TNF therapy through pregnancy has a negative impact on the pregnancy or neonatal outcomes, including neonatal susceptibility to infection. Meta-analysis of six studies confirmed no increased risk of adverse pregnancy outcomes, congenital abnormality, preterm birth or low birth weight.1194 A study of all 1097 individual safety reports received by the Food and Drug Administration adverse event reporting system did not show an increased risk of maternal or neonatal adverse outcome for thiopurine, anti-TNF or combined therapy.1195 In contrast, a prospective study of 80 pregnancies in women exposed to anti-TNF showed no adverse neonatal outcome on anti-TNF monotherapy but did report an increased risk of neonatal infection (bacterial infections in 5% and viral infections in 20%, all with benign course) with combined therapy with thiopurines (relative risk 2.7, 95% CI 1.09 to 6.78, p=0.02).1184 The largest retrospective cohort study to date has recently published the outcomes in 1457 pregnancies in women exposed to anti-TNF therapy for IBD.1196 Treatment was associated with a higher risk of overall maternal complications (adjusted OR 1.49, 95% CI 1.31 to 1.67) and infections (adjusted OR 1.31, 95% CI 1.16 to 1.47). Ongoing use of anti-TNF therapy beyond 24 weeks did not increase maternal complications, but interrupting treatment was associated with relapse (adjusted OR 1.98, 95% CI 1.25 to 3.15). No increased infection rates were seen in children born to mothers exposed to anti-TNF in this study (adjusted OR 0.89, 95% CI 0.76 to 1.05).
5.14.5 Long-term outcomes of anti-TNF therapy during pregnancy
A multicentre retrospective study from the Netherlands has recently been presented in abstract form reviewing outcomes up to 5 years for children born to mothers with IBD.1197 Of 1000 children born, 20% had been exposed to anti-TNF in utero, 24% to thiopurine monotherapy and <1% to systemic steroids. Neither anti-TNF nor thiopurine exposure was associated with adverse birth outcomes, whereas use of steroids was associated with preterm birth (adjusted OR 2.67, 95% CI 1.59 to 4.47). Exposure to IBD therapy did not influence long-term adverse health outcomes, adverse reaction to vaccination or infection rates.
The TEDDY study, a retrospective multicentre study, followed children born to women with IBD who were exposed to anti-TNF either during pregnancy or within 3 months prior to conception and a non-exposed comparator group.1198 The incidence rate of severe infections, however, was similar between groups and anti-TNF exposure during pregnancy was not associated with a higher risk of severe infections (HR 1.2, 95% CI 0.8 to 1.8). The exposed group had more Caesarean sections, more with low birth weight and more intensive care unit admissions.
The PIANO registry (Pregnancy and Neonatal Outcomes in Women with IBD), a prospective USA registry with over 1000 patients, has presented data on up to 4 years of follow-up in patients exposed to biological therapy during pregnancy. The use of anti-TNF during pregnancy was not associated with developmental delay or increased risk of infection in this cohort.1199
Although the majority of data are for infliximab and adalimumab, there are data to suggest that golimumab is also associated with a low risk of adverse maternal and neonatal outcome.1200
In conclusion, a decision to stop anti-TNF therapy between weeks 22 and 24 of gestation must hinge on disease quiescence (sustained remission for 12 months prior to conception with endoscopic and radiological evidence), driven by strong patient preference. Patients at increased risk of flare may continue anti-TNF therapy throughout pregnancy.
5.14.6 Infant vaccinations after exposure to biologics
Statement 129. We suggest that BCG vaccination (if indicated) should be withheld until at least 6 months after birth, and rotavirus vaccine should not be given, for infants exposed in utero to biological therapies. Non-live vaccinations may be given according to standard vaccination schedules (GRADE: weak recommendation, very low-quality evidence. Agreement: 97.7%).
Offspring exposed to anti-TNF drugs, vedolizumab and ustekinumab in utero are able to mount appropriate antibody responses to inactivated vaccines and should complete the inactivated vaccine programme as scheduled.1201 A multicentre observational retrospective study from 22 French gastroenterology departments was recently presented in abstract form.1202 The study aimed to determine the rate and tolerance of live vaccines in children before and following 6 months of life when exposed in utero to anti-TNF therapy and in children breastfed by mothers receiving anti-TNF. Anti-TNF therapy was stopped before 26 weeks gestation in 74 (52%) women and resumed following delivery in 92%. Sixty-three women (45%) breastfed and no complications were reported. BCG vaccination was administered in 33 children (27.5%) prior to 6 months in 19 children (16%). One local abscess was reported with ‘favourable evolution’. Seven children received rotavirus, five children before 6 months. One case of fever was reported. MMR was administered in 72 children (60%), before 6 months in six cases.
Data from the Dutch National Vaccination Programme in children exposed in utero to anti-TNF therapy shows that child vaccination against hepatitis B is effective compared with a control group.1203 There were no differences in birth outcomes, growth and infections in the first year of life.
Thus, non-live vaccination should be given as usual in infants exposed in utero to anti-TNF drugs, BCG should be deferred to 6 months of age and rotavirus should not be given at all (as there is no value in giving rotavirus later than 6 months).
5.14.7 Vedolizumab, ustekinumab and tofactinib in pregnancy
There are very limited data about outcomes of pregnancies with vedolizumab. A review of pregnancies that occurred within the vedolizumab trials revealed 27 unintended pregnancies in female participants and 19 pregnancies in female partners of male participants.1204 No significant safety concerns were identified, although most women did not continue vedolizumab through to term. One case series presented four pregnancies while on vedolizumab, all successful (live offspring, not premature, normal APGAR scores, achieved developmental milestones).1205 The data for ustekinumab in pregnancy are also limited to case studies and registry data. These data from rheumatology suggest that ustekinumab is not associated with increased risk of miscarriage or congenital malformation.1206 However, controlled data are lacking. Data in pregnancy in women with IBD pregnancy are limited to case reports.1207 Data are also limited for tofacitinib in pregnancy associated with UC, where 11 cases of maternal exposure and 14 cases of paternal exposure have been identified across intervention studies.1208 Outcomes include 15 healthy infants, with no neonatal or fetal deaths, no congenital malformations, two spontaneous abortions and two medical terminations.
The lack of data confirming safety and the consequences of withdrawing treatment should be discussed as part of pre-conception counselling. It is unknown whether exposed infants are susceptible to pathogenic infection from live vaccines. Until further data are available, it is recommended that the same practice that is used for anti-TNF drugs is applied to the newer biological agents. General guidance on pregnancy in IBD patients, summarised from ECCO and Toronto guidance,1209 1210 is shown in box 12.
General guidance on pregnancy in IBD patients
Prior to conception:
Education: Importance of keeping well (‘you need to be well for your baby to be well’). Discuss potential adverse fetal outcomes of uncontrolled IBD (eg, pre-term birth and low birth weight), the risk of flare versus risk of current medications.
Optimise: Is the patient as well as possible with their IBD? Investigate and, if necessary, treat.
General health: Consider folic acid, nutrition, cervical smear, smoking cessation, vaccinations.
Consider: Is the patient receiving the safest possible combination of medicines for pregnancy?
During pregnancy:
Treat both maintenance and flares as normal with 5-ASA, thiopurines, anti-TNF, nutrition and steroids. Indications for surgery in pregnant women with IBD are the same for non-pregnant patients
Use therapies with the best evidence base for safety in pregnancy.
Use imaging as needed but minimise radiation exposure with emphasis where possible on ultrasound and MR. Essential endoscopic investigations only when needed for clinical decision making (ideally in second trimester).
VTE prophylaxis is particularly important if in hospital (including following Caesarean section) or unwell.
Involve the MDT and patient in your decisions and include an obstetrician with appropriate experience.
Delivery and postpartum:
Mode of delivery should be determined by obstetric considerations and patient preference except active perianal disease and ileoanal pouch or ileorectal anastomosis where caesarean section is often preferred.
VTE prophylaxis is important after Caesarean section.
Medicines safe in pregnancy are also safe in breastfeeding and should continue.
Breastfeeding is the preferred method of feeding and does not impact the course of IBD.
5.15 Genetics
Statement 130. We suggest that genetic testing for monogenic disorders should be considered in adolescents and young adults who have had early onset (before 5 years of age) or particularly aggressive, refractory or unusual IBD presentations (GRADE: weak recommendation, very low-quality evidence. Agreement: 95%).
Most children and the vast majority of adults with IBD do not have a monogenic predisposition to intestinal inflammation. However, this possibility should be considered in individuals either with very early onset of disease (ie, often in infancy, but up to 5 years old by the definition) or early onset in whom there are atypical features including susceptibility to unusual or frequent infections (suggesting a possible underlying immune deficiency). Mutations in the IL-10 signalling pathway have a Mendelian inheritance pattern and complete penetrance of the IBD-like phenotype, while a number of other genetic defects that disturb intestinal epithelial barrier function or affect innate and adaptive immune function have incomplete penetrance of intestinal inflammation. The importance of not missing such cases lies in the aggressive nature of the IBD-like phenotype and the fact that they are often very resistant to conventional IBD therapies. Some, such as XIAP and IL-10 receptor mutations, require allogeneic bone marrow transplantation for effective treatment and to prevent premature death. Increasingly, the diagnostic pathway relies on exome sequencing, but the analysis is complex and accurate diagnosis of the multiplicity of monogenic conditions that can produce IBD-like phenotypes in or soon after infancy relies on the laboratory being familiar with this clinical spectrum.1211
Pharmacogenetic testing for thiopurines is discussed in the Section on 5.2.2.1: Common Disease Considerations, Thiopurine methyltransferase and NUDT15.
5.16 Travel advice for IBD patients
Statement 131. We recommend that IBD patients travelling abroad should receive pre-travel health advice, taking into account any immunosuppressive medication. Standard vaccination advice should be given, but those on immunosuppressive drugs should not receive live vaccination unless treatment has been discontinued for a minimum of 3 months (GRADE: strong recommendation, very low-quality evidence. Agreement: 95.7%).
Patients can be very anxious about the risks of travelling abroad and issues surrounding vaccination during treatment for their IBD. Knowledge among patients and health professionals is poor, so education for both is important.1212 1213 The IBD Passport website provides comprehensive information about travel with IBD (www.ibdpassport.com). Comprehensive information, aimed at health professionals but available to the public, is also available in the CDC Travellers Health – Yellow Book (https://wwwnc.cdc.gov/travel/page/yellowbook-home). Live vaccinations should not be given to patients on immunosuppressive drugs and can only be given a minimum of 3 months after stopping this treatment. In relation to travel, this will include yellow fever and oral cholera vaccine. Clear advice is provided in the UK Green Book.730
Patients should also be counselled about dietary precautions when travelling, managing their medication, dealing with diarrhoea and travel insurance. They should be advised not to stop immunosuppressive therapy during an exacerbation of symptoms or potential infection.1214 In fact, immunosuppressed IBD patients who may be travelling abroad need to be optimised medically to try and prevent opportunistic infection where possible.1215
Good Practice Recommendation 26. IBD patients travelling abroad should be advised to take adequate supplies of medication with them and should not stop their immunosuppressive therapy. Those on immunosuppressive drugs should be advised to have a low threshold for treating possible traveller’s diarrhoea with quinolones or azithromycin (Agreement: 95.7%).
Travellers with IBD to developing countries (particularly if likely to be staying in accommodation with poor sanitation) are advised to carry a fluoroquinolone course (such as ciprofloxacin 500 mg twice daily) for empirical self-treatment of traveller’s diarrhoea. Azithromycin is comparable to quinolones for self-treatment of traveller’s diarrhoea in certain circumstances: (i) patients who take a fluoroquinolone as part of their treatment for IBD; (ii) travellers to countries where endemic bacteria are known to have high levels of fluoroquinolone resistance; (iii) patients who have no response to a quinolone within 36–48 hours; (iv) pregnant women and children <16 years (for whom a fluoroquinolone is contraindicated).1216 Currently, there is no evidence to support empirical treatment with rifaximin. Overall, the immunocompromised traveller with diarrhoea should have a lower threshold than immune competent travellers for initiating self-therapy, but stool samples should be obtained for microbiology in patients whose diarrhoeal symptoms do not respond to initial antibiotics.700 All patients should be advised to seek medical advice if they do not respond to simple measures. Returning travellers with diarrhoea should have stool tests for infection and a full blood count for eosinophilia. Travel and opportunistic infection are covered in more detail in recent ECCO guidance.700
6 Service delivery
6.1 IBD service and the multidisciplinary team
Good Practice Recommendation 27. The IBD multidisciplinary team (MDT) should include a core membership consisting of gastroenterologist, colorectal surgeon, IBD specialist nurse, radiologist, dietitian, histopathologist and pharmacist, all of whom should have expertise in IBD. The MDT should have a designated coordinator and be able to access advice from the following disciplines where necessary for decisions about specific patients: stoma nurse, paediatric gastroenterologist, hepatologist, nutrition support team, psychologist, primary care physician, ophthalmologist, rheumatologist, dermatologist, obstetrician and social worker (Agreement: 97.9%).
A multidisciplinary team (MDT) approach to patient management is recommended by NICE Quality Standards and by expert opinion.1217–1219 MDT management of IBD helps to provide optimised and personalised care, based on available professional expertise, infrastructure and funding.1 1220–1224 Robust evidence in defining adult IBD MDT membership is lacking; however, best practice identifies a minimum per 250 000 population of two gastroenterologists, two colorectal surgeons, 2.5 IBD nurses, 1.5 stoma nurses, 0.5 dietitian (allocated to Gastroenterology), 0.5 administrative support, one histopathologist, one radiologist and one pharmacist – all with arrangements for cover in the event of absence.1225 The wider MDT (see figure 7) should include a psychologist, paediatric IBD team, obstetrician, rheumatologist and dermatologist.1224 Input may be required from hepatology, oral medicine, ophthalmology, general practitioner, social workers and the nutrition support team.

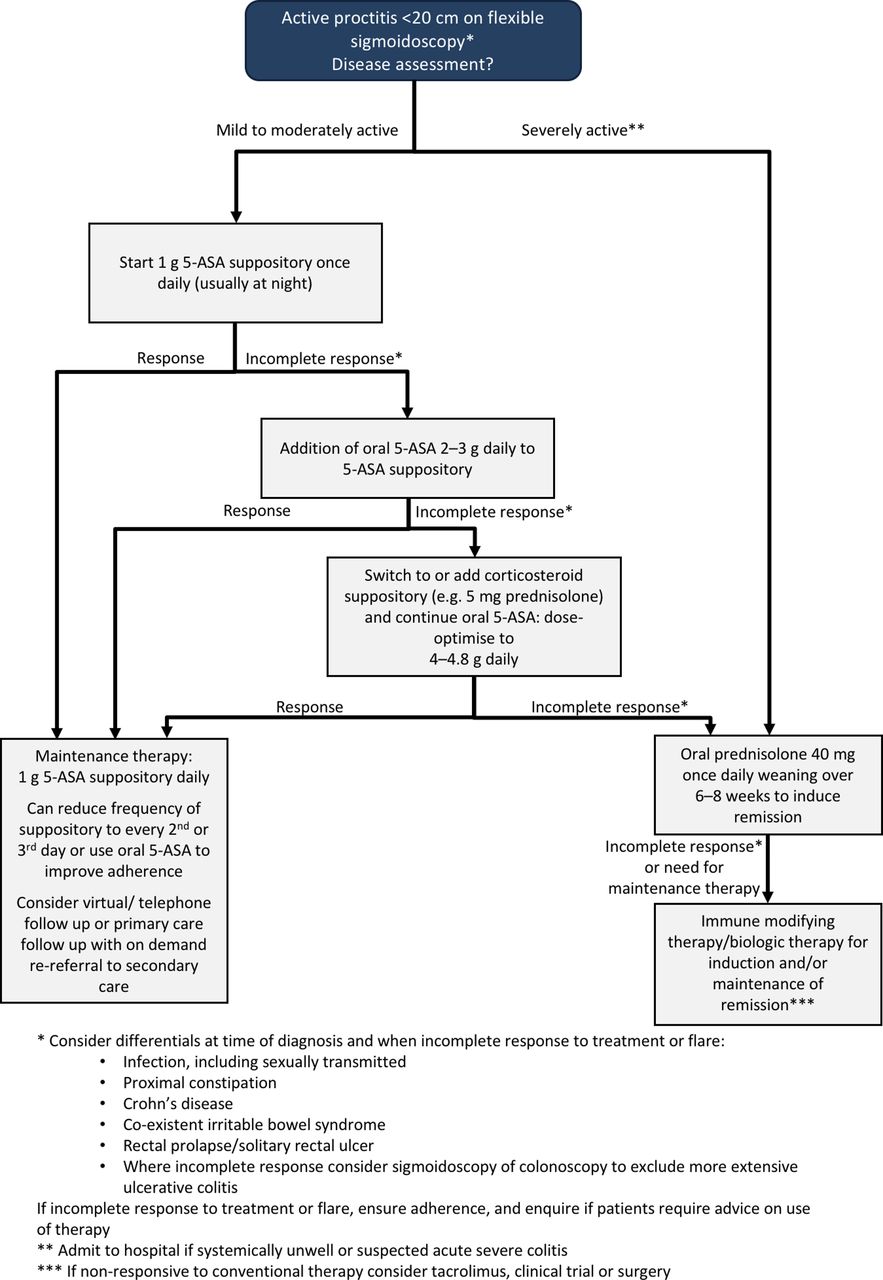{kind=link}
{kind=link}
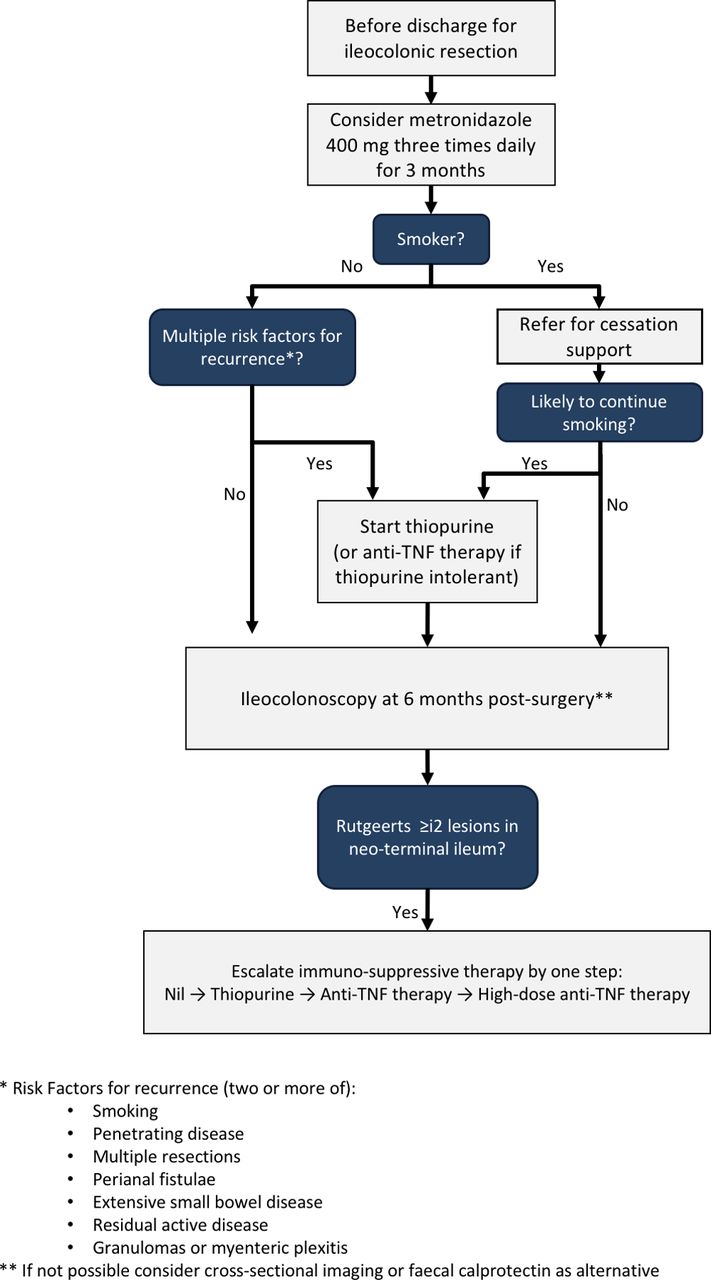{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The IBD multidisciplinary team (MDT). It is important that the MDT meets regularly to review cases and make recommendations. All members of the team should have input as appropriate, but those in the inner box should be present at all regular MDT meetings. Staff in the middle box can and should be encouraged to attend these meetings, but this may not always be possible and they should nevertheless be encouraged to contribute reports or opinions. Staff in the outer box are part of the wider MDT and may contribute to team function through clinical input outside of these team meetings, such as through combined clinics or working to shared protocols. Staff in the grey circle should attend as a valuable part of their training.
The addition of an MDT coordinator has been shown to be effective in cancer management1226 and should be considered in IBD. However, patient advocacy has been shown to be lacking in some MDT meeting models. The systematic review of cancer MDTs demonstrated a biomedical approach to most decisions with nursing staff often not having an active role in decision-making and patient preferences frequently not considered as part of the process.1227 The IBD nurse is well placed to fulfil this role in the MDT. The patient should be provided with information and support at all stages of their illness to enable shared decision-making with the IBD specialist team.1225 In IBD cross-specialty discussion, decision-making and follow-up is of clear importance, especially in surgical management,1221 1228 and should be clearly documented.
6.1.1 MDT meetings
Statement 132. We recommend that regular multidisciplinary team (MDT) meetings should be held to discuss IBD patients with complex needs (GRADE: strong recommendation, very low-quality evidence. Agreement: 97.9%).
Timing of MDT meetings depends on the size of unit and should happen weekly, or frequently enough to ensure decision-making is not delayed, and should have enough capacity to deal with the number of patients. Acute or emergency care decisions should not be delayed for timetabled meetings but should happen separately between relevant specialists. In a UK nationwide audit, the presence of an IBD MDT was an independent factor associated with lower rates of steroid overuse.448
Good Practice Recommendation 28. For each IBD patient discussed in the MDT meeting, a formal record should be kept of management decisions reached (Agreement: 100%).
Limited evidence exists on the specific format of an MDT meeting; however, a colorectal MDT survey highlighted the need for a coordinator and the benefits of training in data management.1226 The cost-effectiveness of the MDT in secondary care has not been demonstrated mainly due to heterogeneity in study methodology.1229 However, a recent Delphi consensus of IBD service quality indicators emphasised the importance of team working and this can be delivered effectively through an MDT process with administrative support, either by a secretary or clerical officer.1230
6.2 Quality improvement and audit
Good Practice Recommendation 29. IBD units should have quality improvement and audit processes embedded within regular clinical activity (Agreement: 100%).
There is much that can be done to improve the quality of care for IBD patients, both in adhering to evidence-based standards of care and also in improving the quality of patients’ experience of their healthcare by provision of information, shared decision-making and improving access to their IBD team.1222 A recent Delphi consensus identified a core set of 56 quality indicators (12 structure, 20 process and 24 outcome).1230 Structure and process quality indicators highlight the need for multidisciplinary management and continuity of care, and that IBD units should be able to provide both outpatient and inpatient care. Outcome quality indicators focused on the adequate prophylaxis of disease complications and drug adverse events, the need to monitor appropriateness of treatment and the need to reinforce patient autonomy by providing adequate information and facilitating patients’ participation in their own care. The IBD MDT is essential to this process.1218
6.2.1 Rapid assessment
All patients referred with suspected IBD should be seen by a specialist within 4 weeks of referral, but patients with severe symptoms may need urgent specialist assessment within a few days.1217 Patients experiencing a relapse of their IBD should have access to a member of the IBD team within five working days, and patients requiring radiological or endoscopic investigations should have tests performed within 4 weeks, or within 24 hours in an acute or emergency situation.1225
6.2.2 Adverse event monitoring
Good Practice Recommendation 30. IBD services should collect data on adverse events and near misses. The service should participate in local and national audit and engage in ongoing quality improvement (Agreement: 100%).
The UK National IBD Audit was a powerful tool to measure and enable IBD services to compare practice. Participation in the Audit was a catalyst for service improvement.1231 Monitoring and reporting adverse events are important aspects of service improvement.1232 1233
6.3 Electronic patient data collection for clinical management and audit
Good Practice Recommendation 31. Patient data on treatment with biological therapies and immunomodulators should be recorded to provide information for clinical management and to monitor adverse events and clinical outcomes for both local and national audit. Biological treatments should be recorded by brand name where biosimilar drugs are also available (Agreement: 97.8%).
The use of an IBD-specific patient management system is essential to capture clinical data on patients receiving immunosuppressive and biological drug therapy. It enables input and presentation of key information at point of care, facilitates effective drug monitoring, and collects data that can be used for audit and research.1234 1235 With the increasing availability of new drugs, including biosimilars, these data can be used locally, but also on a national basis to monitor safety and efficacy.
6.4 IBD specialist nurses
Good Practice Recommendation 32. Clinical nurse specialists are a vital part of the IBD team, where their role may include provision of cost-effective patient education, disease management and therapy monitoring, patient support, continuity of care, audit and rapid access for advice and review during disease flares (Agreement: 100%).
The role of the IBD specialist nurse is integral to the provision of a multidisciplinary service for IBD patients.1230 1236 Although there is little robust RCT evidence to demonstrate the cost-effectiveness of the role,1237 some suggest that the IBD nurse specialist role results in significant reduction in hospital admissions, emergency unit attendances and clinic visits as a result of contact with the nurse.1238 1239 Other small controlled studies suggest cost-effectiveness,1240 while some observational studies have suggested an improvement in patient care.1241–1243
IBD specialist nurses are often responsible for the management of medication and provision of disease information for patients.1220 1239 1244 Adherence to medication can be improved by multiple different interventions including patient education, behavioural change, dose simplification, cognitive behavioural therapy and use of telemedicine.1245 A study of nurse telephone counselling in 524 patients with UC using cognitive-behavioural and motivational interview techniques to address cognitive and emotional barriers to adherence showed significant improvements in adherence, although there was no control group.1246 A Norwegian randomised study of nurse follow-up compared with gastroenterologist follow-up showed that outcomes were as good over 1 year in the nurse follow-up clinics as they were in the gastroenterologist clinics.1236 Time between symptoms of relapse and starting treatment was shorter in the nurse-led clinic and may relate to improved patient access to the IBD service.
6.5 Telephone advice lines/telephone and virtual clinics
Statement 133. We recommend that IBD patients and primary care physicians should be provided with a dedicated IBD telephone line or email service to allow timely advice and care, particularly during times of relapse or to discuss managing medications or treatment side effects. Services must have adequate administrative and funding models (GRADE: strong recommendation, low-quality evidence. Agreement: 100%).
IBD advice telephone or email services are an important communications pathway for IBD patients who need access to specialist support and advice, while not necessarily needing a clinic appointment or hospital admission. A Spanish study of >1200 calls showed that a specialist nurse could manage two-thirds, with the remainder requiring a doctor’s input.1247 Nearly 90% were resolved by telephone call alone. 27% concerned IBD drug treatment, 25% related to disease concerns (mostly possible relapse), 25% related to administrative issues (such as appointment bookings) and 22% were queries regarding disease management. In an Irish survey, over one-third of calls related to flares or patient concerns, but 44% related to administrative issues, including blood test requests/results and repeat prescriptions.1242 Having a system to divert administrative queries to a secretary or clerical staff would free up time for IBD specialist nurses for more appropriate use of their skills—for example, carrying out vigilance and rescue work.
Following introduction of a telephone advice line in 2013 in a Scottish hospital, avoidance of consultant clinic and general practitioner appointments were estimated to have resulted in highly significant cost savings of over £42 000 in a 5-month period.1248 A study in Spain also suggested significant cost savings from availability of telephone consultations with an IBD nurse.1249 In Canada, a survey of over 1000 patients showed that many felt it difficult contacting their physicians, and 77% stated they would make telephone contact with an IBD nurse if available in future, when having acute symptoms. The authors speculated that this would result in fewer emergency department attendances.1250 In a USA study a survey was undertaken of telephone calls to nurse coordinators supporting IBD providers in a tertiary centre.1251 Patients with high call rates (>10 per year) had more complex disease and drug treatments, markers of increased disease activity and high service utilisation. In order to effectively run telephone and email services, adequate funding and administrative support must be available.
6.6 Alternatives to clinic attendance for follow-up
Statement 134. We recommend that telephone or video virtual clinics can allow for the timely follow-up of stable IBD patients as an alternative to face-to-face clinic visits. These clinics need adequate administrative support and documentation, and methods to ensure contact with patients is maintained. Patients must have easy access to telephone or email advice and clinic access in the event of disease flare or patient concern about their IBD (GRADE: strong recommendation, low-quality evidence. Agreement: 95.7%).
A recent USA study showed that patients attending outpatient clinic appointments travel more than 25 miles each way to attend, have to take half a day off work and incur personal out-of-pocket expense of 62 US dollars to attend.1252 Coupled with increasing demands on health service appointments, many strategies have been introduced to reduce the need for face-to-face clinic appointments for patients in stable long-term remission. This includes telephone clinics, email contact and other electronic management or web-based systems. Telephone contact as an alternative to clinics are acceptable to most patients,1253 with a Danish survey showing that 87% approved, particularly in younger patients who were working.1254 Quality outcome measures have been shown as comparable with telemedicine clinic in comparison to standard in-office appointment.1252 A pharmacist-led telephone clinic for patients on immunomodulators has been shown to be popular and effective.1255
Supported self-management systems, including telephone contact, may improve monitoring and colonoscopic surveillance adherence for stable patients who could otherwise be lost to follow-up.1256 Other e-health technologies have gained popularity in recent years including smart phone applications and web-based interventions. These tools may serve as a method of engaging rural or isolated populations.1257 A review of six randomised controlled trials of a variety of distance management systems (web-based self-management and education, email contact, open-access clinics, and three that included telephone contact) showed a significant reduction in clinic visits with an average reduction from two to three down to one clinic visit per year.1258 The review suggested that more interaction between patient and professionals may be associated with greater benefits in terms of quality of life, but overall there was no significant change in quality of life, relapse rates or hospital admissions. A further recent systematic review identified six randomised controlled trials and nine observational studies showing improvements in relapse duration (18 days vs 77 days, p<0.001 in one study), disease activity, improved medication adherence, quality of life, IBD knowledge, costs, reduced outpatient clinic attendance and high patient satisfaction with these technologies.1259 IBD services should have provision for remote follow-up methods, which should be offered to motivated patients who are happy not to attend conventional clinic follow-up appointments.
6.7 Self-management
Statement 135. We suggest that IBD patients who wish to participate in guided self-management should be provided with education sessions and written or electronic personalised information about their management, with ongoing support and access to the IBD service in the event of relapse (GRADE: weak recommendation, moderate-quality evidence. Agreement: 93.6%).
Guided self-management describes empowerment of patients to manage their condition and be involved in treatment decisions through provision of written information in understandable terminology regarding anticipated treatment or surveillance algorithms or when and how to contact primary or secondary care professionals. A randomised trial of guided self-management showed a reduction in clinic visits and more rapid treatment of flares in the self-management group.1260 There was no significant increase in quality of life overall. A subsequent randomised controlled trial recruiting 700 patients demonstrated that, over 1 year, self-management techniques led to fewer hospital visits (difference −1.04; 95% CI −1.43 to −0.65, p<0.001).1261 This was not associated with increased numbers of visits to primary care. Satisfaction and quality of life were similar between guided self-management and standard care. The self-management group reported increased confidence in being able to manage their condition. Longer term, specialist nurse contact was required in additional to guided self-management in order to ensure colorectal cancer surveillance is undertaken, that patients receive osteoporosis screening and that annual reviews are completed.1262
A systematic review, meta-analysis and meta-regression of 15 studies of self-management interventions showed that these strategies do result in some improvement in health-related quality of life, but there were no significant differences between the different components of the self-management strategy, perhaps because of the range of interventions that were included.1263 There was a trend for those with tailored management (eg, including guidance according to individual symptom diaries, personalised guided self-management advice, or individual psychotherapy support), for those with information components that improved IBD knowledge, and for those with detailed symptom management, to result in better outcomes. The only significant difference was shown between the two web-based programmes, which had a greater effect size compared with the remaining 13 with face-to-face interventions.
A multicentre controlled trial of telemedicine incorporating guided self-management has recently been published by a group in the Netherlands. The ‘myIBDcoach’ system utilises algorithms to request patients to complete questionnaires monitoring disease activity between 3 months when in remission and weekly during a flare. Questionnaires are undertaken in preparation for outpatient review. Parameters above a pre-defined threshold were flagged to the IBD clinic. The system also includes a personalised output including visualised health parameters, PROs and quality metrics, and interactive patient-tailored information on topics including medications, adherence, smoking cessation, nutrition, self-management to prevent or reduce symptoms, fatigue, work productivity, anxiety and depression. It also contains a secure messaging service between patient and clinician. After 1 year, those assigned to telemedicine (n=465) compared with standard care (n=444) attended fewer outpatient clinics (1.55 vs 2.34, p<0.0001) and had fewer hospital admissions (0.05 vs 0.10, p=0.046). Quality of care scores did not vary between groups.1264
6.8 Primary care
Good Practice Recommendation 33. Integrated care pathways and shared management guidelines should recommend primary care prescribing and monitoring of IBD treatments including mesalazine, thiopurines and methotrexate once patients are in remission on stable dose. Primary care physicians should arrange monitoring blood tests, relevant vaccinations and encourage treatment adherence, supported by regular communication with secondary care (Agreement: 95.7%).
Primary care is often the first point of contact for IBD patients with deteriorating symptoms. Clear and comprehensive communication between hospital and primary care is essential (box 13). Recommended information should be included in correspondence between secondary and primary care. The development of local pathways taking into consideration available resources is encouraged. Patients with clinical features of severe disease, defined as six or more bloody stools per day plus one of temperature >37.8°C, heart rate >90 beats/min, anaemia <105 g/L or ESR >30 mm/hour should be admitted as an emergency for specialist assessment.102 1265 For patients with moderate or severe IBD not requiring urgent admission, it is important that early contact is made with their IBD clinic, either by the patient or the general practitioner (GP), to ensure that response to therapy is monitored. GPs often prescribe prednisolone, but may be less familiar with increasing the 5-ASA dose to manage flares of UC. An adequate response should be expected within 2–3 weeks1266 and, if not evident, review is required to assess the need to escalate treatment or arrange hospital admission.
Recommended information to be included in correspondence between secondary and primary care
Information to be included in correspondence from secondary to primary care:
Main diagnosis/diagnoses: type and location of IBD and date of diagnosis
Date(s) of surgery
Secondary diagnosis/diagnoses—for example, anaemia, vitamin D deficiency, osteoporosis, extraintestinal manifestations
Date of last endoscopy with findings and timing of next planned endoscopy
Date of next planned contact with secondary care
Current medical therapy including any previous treatments with thiopurines, methotrexate or biologics and reasons for discontinuation
Recommended length of current medical therapy
Treatment recommendations in case of a flare: 5-ASA dose increase, prednisolone, budesonide, calcium and vitamin D. Details of who to contact if treatment is initiated in primary care
Contact details for local IBD team
Weblink for advice and guidance for primary care (eg, RCGP Spotlight Project toolkit www.rcgp.org.uk/ibd)
Information to be included in correspondence from primary to secondary care:
Date last prescription issued
All current and recent medications. Any recent antibiotics
Number of courses of oral prednisolone issued in last 12 months
Key results of last blood tests
Functional impact for example, impact of IBD on employment, family and social functioning
Any newly diagnosed comorbidities
A recent study of IBD patients managed in primary care in London showed a high standard of monitoring blood tests and avoidance of unnecessary steroid use, but underprovision of vaccination where recommended by guidelines and overuse of 5-ASA in Crohn’s disease.1267 A primary care study of UC patients taking 5-ASA showed that dosage, monitoring and adherence were suboptimal,1268 and vaccination levels poor.1269 Integrated referral pathways have been shown to reduce waiting times for advice and specialist investigations, improve clinical and patient reported outcomes and reduce costs to the healthcare system.1270 Internet-based programmes can facilitate structured monitoring for patients being followed up in the community.1271 Adherence to medication can be improved by simplifying dose regimens and promoting better understanding and communication between the patient, primary care and IBD clinic team.1272 Better education for patients and for community and hospital teams is likely to improve vaccination uptake.1239 1273–1276
7 Future research priorities
By reviewing the original 414 clinical questions that the guideline development group defined as those facing multidisciplinary clinicians in everyday clinical practice, with comparison to evidence returned from the systematic review process and results from the eDelphi, 20 research priority themes have been determined and are presented in table 12. An essential aspect of any research priority identification process is determination of the importance of this research to those living with UC and Crohn’s disease. Accordingly, each research priority theme was drafted in healthcare professional language and for a general audience, with readability testing shown in online supplementary table 4. Feedback on the importance of each theme was received from two electronic surveys conducted by the UK patient charity Crohn’s and Colitis UK (table 12). The 931 respondents to survey 1 and 1448 respondents to survey 2 were anonymous but identified themselves as a UC or Crohn’s disease patient, a relative, partner, parent, friend or carer. Subgroup analyses of research priority theme importance are presented in online supplementary table 5. Identified as of particular importance to those living with UC and Crohn’s disease were: prevention, risk stratification, diagnosis and management of neoplasia; aetiology and management of pain and fatigue; precision medicine; surgical techniques to minimise postoperative disease recurrence in Crohn’s disease; management of non-perianal fistulae in Crohn’s disease; and the microbiome including faecal microbial transplantation and the impact of dietary modification in UC. All 20 research priority themes were found to be important to those living with UC and Crohn’s disease, with mean scores and confidence intervals for each falling in the upper tertile of the 1–9 Likert scale, with the exception of research regarding improvement of adherence to therapy and the impact on patient outcome. Our findings are complementary to those of the James Lind Alliance and build on the importance of a strong patient voice in research priority setting.1277 1278 It is hoped that this exercise will highlight to the academic community, research funders and policy makers where further high-quality research is required to support and advance future clinical practice in UC and Crohn’s disease.
Research priority themes identified by guideline development group, with measures of importance determined from two surveys conducted by Crohn’s and Colitis UK
8 Concluding remarks
These British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults have been developed along with all major UK stakeholders in UC and Crohn’s disease healthcare, including patient representation through close collaboration with Crohn’s and Colitis UK.
They are published at a time of rapid change in many aspects of IBD. Recent developments highlighted include new imaging techniques; increasing numbers of new drugs; changes in the way these drugs are used with accelerated treatment and reduction in prolonged use of older therapies with greater toxicity; the increasing importance of infection screening at diagnosis; changes in therapeutic goals (such as mucosal healing) and advances in therapeutic monitoring. This makes IBD treatment ever more complex and highlights the importance of multidisciplinary working, and finding more effective ways to deliver services. We have also emphasised the vital importance of patient education, empowerment and partnership in order to ensure that the patient’s needs (and not the technology) remain the focus of all those treating IBD patients.
We have drawn together concise guidance and evidence supporting a wide range of statements that inform best practice in the care of patients with UC and Crohn’s disease, including the quality of the evidence available and the strength of recommendations, with a Delphi consensus process to show level of agreement. Many areas are clearly in a state of rapid evolution, and there remain obvious gaps in our understanding. In reference to this, we have presented the key unmet research themes arising from our systematic review and have also presented the importance of each from a patient’s perspective. We hope this exercise will highlight aspects of care that are of importance to IBD patients and the healthcare community, and thus may inform government, Research Councils, medical research funding bodies and industry as to areas of research priority in order to advance care for UC and Crohn’s disease patients in 2019 and beyond.
Acknowledgments
We are grateful to the Clinical Standards and Services Committee of the British Society of Gastroenterology for commissioning this guidance, and to the following Stakeholders and Societies who have provided valuable review and comment during the guideline development process: British Society of Gastroenterology, Crohn’s and Colitis UK, Association of Coloproctology of Great Britain and Ireland, Royal College of Nursing, British Society of Paediatric Gastroenterology, Hepatology and Nutrition, British Dietetic Association, British Society of Gastrointestinal and Abdominal Radiology, Primary Care Society for Gastroenterology and IBD UK. We are grateful to Sophie Bassil, Mitesh Gandhi and the wider Crohn’s and Colitis UK team for conducting two electronic surveys regarding the importance of research priority themes identified by the guideline development process, and to the patients, their relatives, partners, parents, friends and carers for completing these surveys. We are grateful to Professor Juliet Compston, Professor Emeritus of Bone Medicine, Cambridge Biomedical Campus, UK for peer review of our osteoporosis prevention and management in IBD figure. The guideline development process was funded by the British Society of Gastroenterology. CAL is a Clinical Lecturer supported by the NIHR.
References
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
Footnotes
Contributors The guideline development group forms the authorship of this manuscript. All fulfil the ICMJE recommendations for authorship with appropriate involvement at all required stages of the guideline development process which followed GRADE methodology as described. All have contributed to manuscript drafting. The additional named contributors formed the IBD guidelines eDelphi consensus group, contributing to voting over three rounds of Delphi to develop the statements and good practice recommendations set out in this guideline.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests Conflicts of interest for authors and contributors are presented in online supplementary table 2.
Provenance and peer review Commissioned; externally peer reviewed.
Collaborators IBD guidelines eDelphi consensus group: Ian Arnott; Kevin J Barrett; R Mark Beattie; Stuart Bloom; Keith Bodger; Richard R Brady; Matthew J Brookes; Steven R Brown; Jeffrey R Butterworth; Christopher R Calvert; Rachel Campbell; Tom Creed; Nicholas M Croft; Fraser Cummings; R Justin Davies; David Devadason; Anjan Dhar; Chris Dipper; Julie Duncan; Malcolm Dunlop; Dharmaraj Durai; Martyn D Evans; Omar Faiz; Nicola S Fearnhead; Alexander C Ford; Aileen Fraser; Vikki Garrick; Daniel R Gaya; James Goodhand; Nigel Hall; Richard Hansen; Marcus Harbord; A Barney Hawthorne; Bu’Hussain Hayee; Sarah Hearnshaw; Paul Henderson; Philip Hendy; Tariq Iqbal; Paul D Johnston; Nicholas A Kennedy; Christopher A Lamb; Jimmy K Limdi; James O Lindsay; Alan J Lobo; Miranda Lomer; Richard E Lovegrove; John C Mansfield; Simon Mclaughlin; Christopher G Mountford; Rafeeq Muhammed; Nurulamin M Noor; Simon Panter; Gareth C Parkes; Miles Parkes; Thomas D Pinkney; Chris Probert; Tim Raine; Richard K Russell; Matthew D Rutter; Mark A Samaan; Jeremy D Sanderson; Christian P Selinger; Ashit Shah; Steve J Short; Baljit Singh; Philip J Smith; Melissa Smith; R Alexander Speight; Catherine Stansfield; Helen Steed; Stuart A Taylor; Helen Terry; Tony C Tham; Nick P Thompson; Gareth J Walker; Catherine L Wall; Janindra Warusavitarne; Gethin L Williams; R Graeme Wilson; David C Wilson; Lisa C Younge. See online supplementary table 1 for affiliations of the IBD guidelines eDelphi consensus group.
Patient consent for publication Not required.