Article Text

Abstract
Objective Bile acids may play a role in the pathogenesis of IBS. We investigated the potential effects of bile acids entering the colon and its role in the symptom pattern in IBS.
Design We measured 75Se-labelled homocholic acid-taurine (75SeHCAT) retention, and serum levels of 7α-hydroxy-4-cholesten-3-one (C4) and fibroblast growth factor (FGF) 19 in patients with IBS (n=141) and control subjects (75SeHCAT n=29; C4 and FGF19 n=435). In patients with IBS stool frequency and form, as well as GI symptom severity were registered, and in a proportion of patients colonic transit time and rectal sensitivity were measured (n=66). An 8-week open-label treatment with colestipol was offered to patients with 75SeHCAT <20%, and the effect of treatment was evaluated with IBS severity scoring system and adequate relief of IBS symptoms.
Results Compared with controls, patients with IBS had lower 75SeHCAT values (p=0.005), higher C4c levels (C4 corrected for cholesterol) (p<0.001), but similar FGF19 levels. Abnormal 75SeHCAT retention (<10%) was seen in 18% of patients, whereas 23% had elevated C4c levels. Patients with IBS with 75SeHCAT retention <10% had more frequent stools, accelerated colonic transit time, rectal hyposensitivity, a higher body mass index, higher C4c and lower FGF19 levels. Colestipol treatment improved IBS symptoms (IBS severity scoring system 220±109 vs 277±106; p<0.01), and 15/27 patients fulfilled criteria for treatment response (adequate relief ≥50% of weeks 5–8).
Conclusions Increased colonic bile acid exposure influences bowel habit and colonic transit time in patients with IBS. A high response rate to open label treatment with colestipol supports this, but placebo-controlled studies are warranted.
- Irritable Bowel Syndrome
- Bile Acid
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
-
Excessive amounts of bile acids reaching the colon leads to watery stools and an erratic bowel pattern, and bile acid malabsorption, diagnosed by use of the 75Se-labelled homocholic acid-taurine (75SeHCAT) test, is a frequent finding in patients with chronic diarrhoea.
-
Alternative tests useful in the diagnosis of bile acid malabsorption are serum concentration of 7α-hydroxy-4-cholesten-3-one (C4), which reflects the rate of the hepatic bile acid synthesis, and fibroblast growth factor (FGF) 19, which suppresses bile acid synthesis.
-
Recent small studies have implicated a potential role of bile acid malabsorption in a subset of patients with IBS.
What are the new findings?
-
Abnormal 75SeHCAT retention and/or high C4 levels, indicating increased bile acid exposure to the colon is present in a substantial proportion of patients with predominantly non-constipated IBS.
-
The 75SeHCAT test, as a measure of the bile acid turnover rate, correlates with hepatic bile acid synthesis and relates to bowel habit and colonic transit time in patients with IBS, as well as with body mass index and markers of general metabolism such as plasma lipid profiles.
-
The positive symptomatic response to open label treatment with a bile acid binding agent (colestipol) in patients with IBS with low 75SeHCAT values supports a role of bile acids in IBS symptomatology.
How might it impact on clinical practice in the foreseeable future?
-
Our study highlights a role for bile acids in symptom generation in a subset of patients with IBS, which has important future treatment implications in this large patient group.
Introduction
IBS is one of the most common functional GI disorders, affecting up to 20% of the Western population.1 ,2 The pathophysiology of IBS is incompletely understood, but disturbed motor, sensory3 ,4 and secretory5 function of the GI tract, as well as psychosocial factors are important.6 Altered immune function and intestinal dysbiosis are considered as putative pathogenetic factors for the development of IBS symptoms in at least a subgroup of patients.7 Luminal factors could also play a role8 exemplified by bile acids affecting GI motility9 and secretion,10––12 as well as immune function and microbiota composition.13 Moreover, an effect of bile acids on visceral sensitivity has been suggested and the colonic motor and secretory response to bile acids seems to be exaggerated in patients with IBS.14 ,15 Further, treatment options modulating the colonic bile acid exposure has successfully been tested in different IBS subgroups.16 ,17 Therefore, as bile acids have the potential to affect main pathophysiological factors in IBS, their significance deserves further studies, and recent small studies support the involvement of bile acids in the pathophysiology of IBS.18 ,19
Excessive amounts of bile acids reaching the colon leads to watery stools and an erratic bowel pattern, through their effect on motility and secretion. One well-known example of this is when the enterohepatic circulation is interrupted as a consequence of ileal resection leading to chronic watery diarrhoea,20 which in turn can be treated effectively with bile acid binding resins.21 ,22 There are also idiopathic forms of bile acid malabsorption (BAM), which are prevalent in patients with chronic diarrhoea.23––25 A systematic review found that 20–30% of patients with symptoms compatible with diarrhoea predominant IBS (IBS-D) or functional diarrhoea may have BAM, but existing studies are limited by poor clinical characterisation of patients.26
Most often BAM is diagnosed by use of the 75Se-labelled homocholic acid-taurine (75SeHCAT) test, measuring the retention of radiolabelled (75Se) synthetic homocholic acid conjugated with taurine 7 days after ingestion.27 This test has been thoroughly validated and the results correlate well with faecal bile acid loss.28 ,29 However, the major disadvantage with this test is that it is not available in the USA and several other countries.29 An alternative way of diagnosing BAM is to measure the serum concentration of 7α-hydroxy-4-cholesten-3-one (C4), which reflects the rate of the hepatic bile acid synthesis.19 ,30 Plasma C4 correlates inversely with 75SeHCAT values30––32 in healthy controls and in patients with diarrhoea without morphological evidence of ileal disease.33 ,34 Another possible test in the diagnosis of BAM is fibroblast growth factor (FGF) 19,35 which is produced in the terminal ileum and proposed to suppress bile acid synthesis by reducing the activity of the rate-limiting enzyme cholesterol-7α-hydroxylase in the liver.36
Until now, large scale studies with different measures of colonic bile acid exposure in patients with well-characterised IBS have not been performed. The primary aim of our current study was to assess if increased amounts of bile acids entering the colon have a role in the pathogenesis and pathophysiology of IBS and also to evaluate its role in the complex symptom pattern of these patients. In order to achieve this, we have investigated a large number of phenotypically well-characterised patients with IBS with 75SeHCAT retention and plasma concentration of C4 and FGF19, and compared the results with healthy controls. As a proof of concept we also evaluated the effect of the bile acid binding resin colestipol on IBS symptoms in patients with low 75SeHCAT retention values.
Methods
Subjects
Patients with IBS, fulfilling the Rome II criteria37 referred to our outpatient clinic for evaluation during 2005 and 2006 were included. The patients were further characterised by predominant bowel habit into subtypes; IBS-D, constipation predominant IBS (IBS-C) and alternating type IBS (IBS-A).37 Organic disorders were excluded with appropriate testing based on the presenting symptoms. Exclusion criteria were: another GI condition explaining their symptoms, previous abdominal surgery including cholecystectomy, but excluding appendectomy, other severe non-GI disease, and current treatment with antidiarrhoeals, bile acid binders or statins. Values of C4 and FGF19 from patients were compared with a group of healthy volunteers studied at the Karolinska Institute,38 and the results from 75SeHCAT test with healthy controls investigated at the Sahlgrenska University Hospital.39
All patients gave verbal and written informed consent and the study was approved by the Regional Ethical Review Boards in Gothenburg and Stockholm, and the radiation safety committee at the University of Gothenburg.
Study design
Upon inclusion, patients accepting to participate in the study completed a validated questionnaire assessing the perceived severity of their IBS symptoms, the Gastrointestinal Symptom Rating Scale—IBS (GSRS-IBS),40 and had their body mass index (BMI) measured (kg/m2). Blood samples for analyses of C4, plasma cholesterol, triglycerides and FGF19 were taken after an overnight fast (8:00) at the first 75SeHCAT day, and immediately frozen to −80°C. During the week of the 75SeHCAT test, the patients recorded all bowel movements on a diary card and graded the stool form based on the Bristol Stool Form scale.41 Besides performing a 75SeHCAT test, a proportion of the patients also underwent colonic transit time measurement3 and assessment of rectal sensitivity with a rectal barostat.4
All patients with 75SeHCAT retention values <20% day 7 were offered an open label treatment with a gradually increasing dose of the bile acid binder colestipol (Lestid) during an 8-week period. They received 1 g tablets with the instruction to start with 1 g twice daily, with an increase of the dose by 1 g/day every other day if they had not noticed a positive effect on their IBS symptoms, and had no side effects. They recorded their daily bowel habits in a diary card described above, and every other week they completed the IBS Severity Scoring System (IBS-SSS)42 questionnaire. The dose of colestipol was registered once a week during the treatment period, and the subjects were asked on a weekly basis if they had had adequate relief of their IBS symptoms.
Questionnaires
The Gastrointestinal Symptom Rating Scale-IBS (GSRS-IBS)
This is an IBS specific questionnaire, assessing the severity of IBS-related GI symptoms during the past week using a seven-graded Likert scale, ranging from 1 (no discomfort) to 7 (very severe discomfort).40 This questionnaire consists of 13 questions, which can be grouped into 5 domains: pain, bloating, diarrhoea, constipation and satiety. We used this questionnaire in the first part of the study, where the association between BAM and GI symptom severity was assessed.
The IBS Severity Scoring System (IBS-SSS)
This questionnaire was used to evaluate the severity of IBS symptoms during the colestipol treatment phase.42 It includes five items—pain severity, pain frequency, severity of abdominal distension, bowel habit dissatisfaction and daily life interference—that are combined into an overall IBS score ranging from 0 (no symptoms) to 500 (maximum severity). Use of IBS-SSS is recommended by the Rome Foundation as a valid outcome measure in clinical trials in IBS,43 and was therefore used in the treatment part. The subjects were also asked on a weekly basis if they had experienced adequate relief of their IBS symptoms (‘yes’ or ‘no’) during the preceding week. A responder to colestipol treatment was defined as a patient who reported adequate relief of the IBS symptoms at least 2 of the last 4 weeks of the treatment period, that is, weeks 5–8.
Analyses of blood samples
One mL of blood serum was assayed for C4 by high performance liquid chromatography as previously described.44 As plasma C4 binds to plasma cholesterol containing lipoproteins C4 values were corrected for plasma total cholesterol (C4c) as previously outlined.45 The normal values for C4c were 0.89–8.0 mg/mol for men and 0.76–6.0 mg/mol for women based on centile 5–95% in the healthy control subjects included in this study (n=435). FGF19 was analysed as previously described.46 Normal values for FG19 (centile 5–95% in control subjects) were 48.1–343 pg/mL for men and 51.7–334 pg/mL for women. Plasma triglycerides, total cholesterol, and high density lipoprotein (HDL) cholesterol concentrations were analysed by routine clinical colorimetric technique.
75Se-labelled homocholic acid-taurine
This test was performed according to the method described by Thaysen et al.27 Briefly, a capsule containing 0.3 MBq 75SeHCAT (Amersham AB, Sweden) was swallowed with a glass of water after an overnight fast. Measurements were performed using an uncollimated γ camera (Starcam System, General Electrics, Milwaukee, Wisconsin, USA) with the patient in a supine position and the γ camera positioned at a distance of 60 cm. The basal value (100%) was obtained with a measurement after 3 h. A new measurement was obtained after 7 days. The abdominal retention was calculated as a fraction of the basal value. A retention value of >10% on day 7 was considered as normal,39 even though some centres use the cut-off value of 15%.29 In the treatment part of this study, we chose to include patients with 75SeHCAT up to 20%, as the optimal cut-off value to determine a positive treatment response in patients with IBS has not been studied.
Colonic transit time measurement
Colonic transit time was measured by use of a validated method using radio-opaque markers as described previously.47 Briefly, 10 radio-opaque markers were ingested daily for 6 consecutive days. On the 6th day the patients divided the daily dose of markers and ingested five markers in the morning and five in the evening in order to better define patients with accelerated transit. On the 7th day, a fluoroscopy was performed in the morning and remaining markers were counted (Exposcop 7000 Compact, Ziehm GmbH, Nüremberg, Germany). The colonic transit time expressed in days was calculated by dividing the number of retained radiopaque markers by the daily dose number; that is, 10. The sum of the caecal and ascending regions was considered as right colonic transit, the transverse colon transit assessed on its own, and the anatomical regions distal to the splenic flexure considered as left colonic transit. In order to minimise potential pitfalls with this technique, the methodology has been optimised at our unit in several previous studies.3 ,47––50
Rectal sensitivity
In order to evaluate rectal sensitivity, a balloon distension test was performed, using a barostat (Dual Drive Barostat, Distender Series II; G & J Electronics, Toronto, Ontario, Canada), as described elsewhere.4 We used phasic distensions with stepwise increments starting at the operating pressure (minimal distending pressure +2 mm Hg) and increasing 5 mm Hg until the subject reported pain or when a pressure of 70 mm Hg was reached. For this study only pressure thresholds (mm Hg) for pain were used for the analyses.
Statistical methods
Data are presented as mean±SD or as proportions (%), unless otherwise stated. Means were compared between two groups using the Student t test, whereas nominal data were compared by use of the Pearson's χ2 test. Correlations were calculated using Spearman's correlation coefficients. Comparison of mean values between multiple groups was done by analysis of variance (ANOVA), with post hoc group differences corrected for multiple comparisons (Bonferroni correction). All analyses in the treatment part of this study were performed on an intention to treat basis, including all patients who completed the baseline questionnaires. For dropouts we used the principle of last observation carried forward technique meaning that the missing data post treatment were imputed from baseline assessments and included in the final analyses. Repeated measures ANOVA was used to assess the treatment effect (IBS-SSS scores), with Bonferroni corrections used for post hoc comparisons between baseline scores and the biweekly symptom scores during the treatment period. Statistical significance was accepted at the 5% level.
Results
Subjects
Altogether 141 patients with IBS according to the Rome II criteria37 were included in the study (102 women; mean age 35.3 (range 17–71) years). Based on the Rome II classification 50 patients (35%) fulfilled the criteria for IBS-A (38 women), 26 IBS-C (18%) (22 women) and 65 IBS-D (46%) (42 women). All patients completed the 75SeHCAT test, blood samples were obtained from 133 patients (C4c n=133; FGF19 n=118) and 66 subjects underwent a colonic transit time measurement and a rectal sensitivity test. The 75SeHCAT results were compared with a group of 29 healthy controls without GI symptoms (22 women; mean age 40 (range 25–55) years)39 and the C4 and FGF19 values with a group consisting of 435 healthy individuals (222 women; mean age 49 (range 20–89) years).38
75SeHCAT, C4c and FGF19: IBS versus controls
Patients with IBS had lower 75SeHCAT retention values at day 7 than control subjects (28±19% vs 39±18%; p=0.005), but this only reached statistical significance for men (18±12% vs 34±12%; p=0.002) and only a tendency in the same direction for women (32±21% vs 40±20%; p=0.08), which might be explained by a different distribution of IBS subgroups in men and women, particularly more patients with IBS-C in the female IBS group (χ2=26.4, df=3, p<0.0001). Patients with IBS-D and patients with IBS-A had lower 75SeHCAT retention values than healthy controls and patients with IBS-C, with no difference between patients with IBS-C and healthy controls (ANOVA: F=7.23; p<0.0001) (figure 1). Twenty-six patients with IBS (18%) had abnormal 75SeHCAT retention at day 7 (<10%), where the distribution between subtypes was 8/52 patients with IBS-A (15%), 3/25 with IBS-C (12%) and 15/64 with IBS-D (23%) (χ2=2.08, df=2, p=0.35). There was a trend (χ2=3.42, df=1, p=0.06) for abnormal 75SeHCAT retention to be more common in men (11/39 (28%)) than in women (15/102 (15%)). When using 75SeHCAT retention at day 7 <15% to define an abnormal test, 45 patients with IBS (32%) had an abnormal test. Fourteen patients (10%) had 75SeHCAT retention at day 7 <5% (10 patients with IBS-D, 3 with IBS-A and 1 with IBS-C). Patients with IBS also demonstrated higher C4c levels than healthy controls, in men (7.2±12.9 vs 3.6±2.9 mg/mol; p<0.0001) and women (4.3±3.3 vs 2.8±1.8 mg/mol; p<0.0001). ANOVA comparing IBS subgroups with healthy controls demonstrated group differences in C4c levels (F=9.77; p<0.0001), where post hoc comparisons revealed higher C4c values in patients with IBS-D than in healthy controls (5.9±10.1 vs 3.1±2.5 mg/mol; p<0.0001), but with no significant differences between the other groups. By using normal values from the healthy control group (5–95% centile), 30/133 patients with IBS (23%) had elevated C4c values, indicating increased bile acid synthesis. Only 3/133 patients with IBS (2%) had low C4c values. The distribution of patients with elevated C4c levels did not differ significantly between IBS subgroups (IBS-A 11/50; IBS-C 8/24; IBS-D 11/59) (χ2=2.12, df=2, p=0.35).

75SeHCAT retention values in patients with IBS and healthy controls. Patients with IBS-D and patients with IBS-A had lower 75SeHCAT retention values than healthy controls and patients with IBS-C, with no difference between patients with IBS-C and healthy controls. The box and whisker plots display the 10th, 25th, 50th, 75th and 90th centiles, and outliers are also shown. *p<0.05, ** p<0.01. IBS-A, alternating type IBS; IBS-C, constipation-predominant IBS; IBS-D, diarrhoea-predominant IBS; 75SeHCAT, 75Se-labelled homocholic acid-taurine.
FGF19 values did not differ between patients with IBS and controls, neither in men (138±95 vs 147±89 pg/mL; ns), nor in women (141±105 vs 144±88 pg/mL; ns), and no differences between IBS subtypes and healthy controls were detected (ANOVA: F=0.92; p=0.43). Low FGF19 values, based on the normal values from the control group (5–95% centile) were seen in 14/118 patients with IBS (12%), and only 5/118 patients had high values (4%). The distribution of patients with low FGF19 levels did not differ between IBS subgroups (χ2=0.83, df=2, p=0.66).
Characteristics of the IBS subgroups are summarised in table 1.
Characteristics of IBS subgroups according to Rome II criteria
Of the patients who had an abnormal 75SeHCAT retention value at day 7 (<10%), 11/24 also had abnormally elevated C4c values, and of patients with high C4c, 11/30 also had abnormal 75SeHCAT retention at day 7 (κ=0.26, p=0.003). In the patients moderately strong correlations were seen between the 75SeHCAT retention values at day 7 and the C4 (r=-0.34; p<0.0001), as well as the C4c concentrations (r=0.29; p=0.001), but not with FGF19 (r=0.13; p=0.15). FGF19 levels correlated significantly with C4 (r=−0.24; p=0.01) and C4c values (r=−0.23; p=0.01). The correlation between C4c and C4 was strong (r=0.964, p<0.0001).
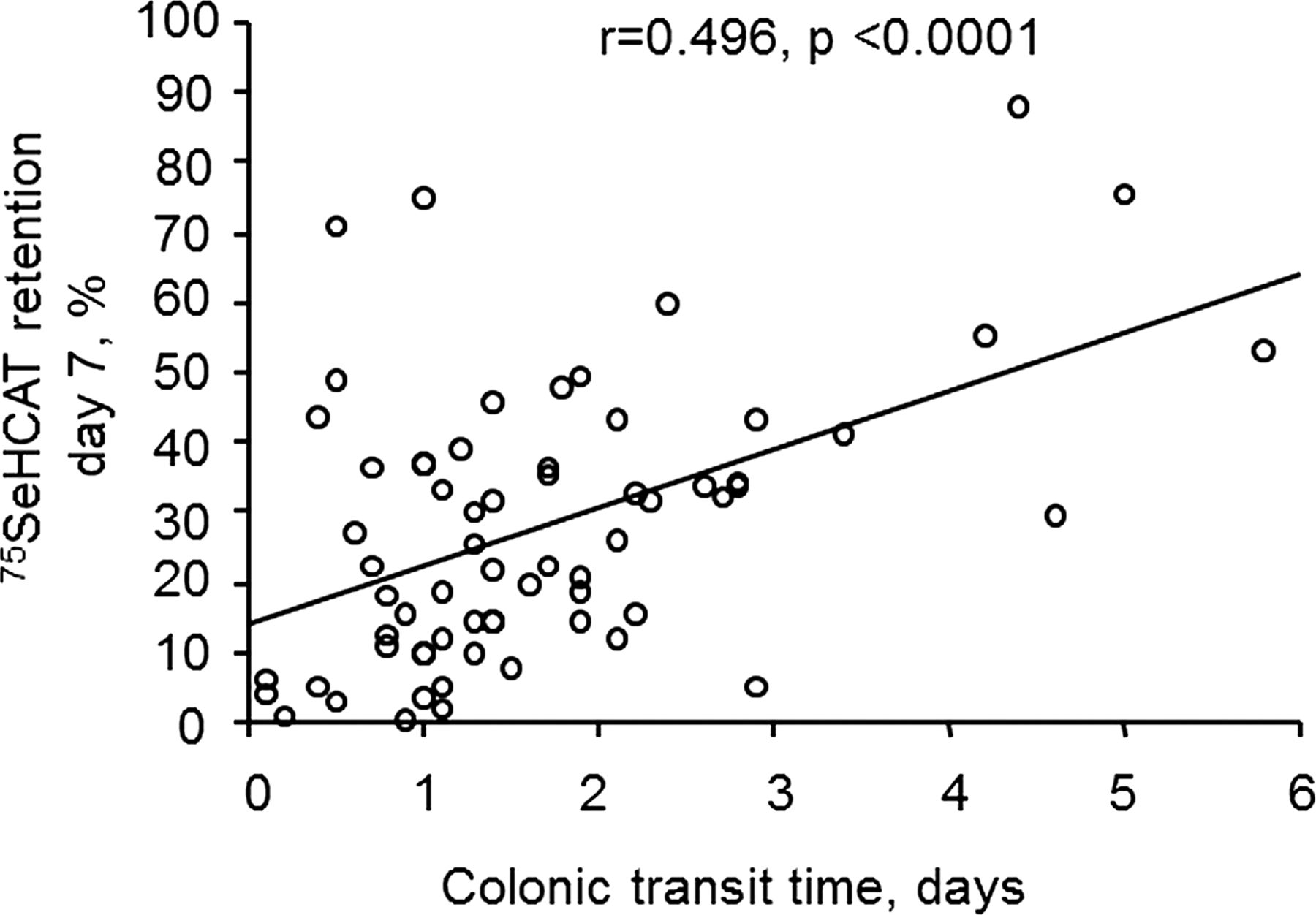
75SeHCAT retention values, C4c and FGF19 concentrations, and clinical parameters
Patients with IBS with 75SeHCAT retention at day 7 <10% were characterised by having more frequent stools, accelerated colonic transit time, especially in the left colon, rectal hyposensitivity, a higher BMI, elevated triglyceride, higher C4c and lower FGF19, and HDL cholesterol levels. However, patients with IBS and abnormal 75SeHCAT retention at day 7 did not rate the severity of their IBS symptoms on GSRS-IBS as being more severe than patients with normal 75SeHCAT values; on the contrary the severity of bloating tended to be less severe in patients with low 75SeHCAT values (table 2). In line with this, 75SeHCAT values correlated significantly with colonic transit time (figure 2), BMI (r=−0.28; p=0.01), stool frequency (r=−0.27; p=0.001) and stool form (r=−0.19; p=0.03) but not with any of the GI symptom severity measures (GSRS-IBS; data not shown). Using alternative cut-off levels when defining abnormal 75SeHCAT retention at day 7 (<15% or <5%, respectively) yielded similar group differences between patients with normal and abnormal retention values as for 75SeHCAT retention at day 7 <10% (data not shown). When evaluating IBS subgroups separately, a significant association between 75SeHCAT values and colonic transit was only seen in the IBS-D group (r=0.58; p=0.001), whereas only borderline significance was found in IBS-A (r=0.38; p=0.06) and no significant association in IBS-C (r=0.17; p=0.17; p=0.6). In line with this, only in the IBS-D group significant correlations between 75SeHCAT values and stool frequency (r=−0.25; p=0.04) and form (r=−0.31; p=0.01) were noted. Fewer differences in clinical parameters were seen when comparing patients with IBS with normal/low (n=103) and high (n=30) C4c values. Only higher triglyceride, lower HDL cholesterol and FGF19 levels, and a higher BMI were characteristic of patients with IBS with elevated C4c concentrations. No differences in symptom severity (GSRS-IBS) were noted between patients with normal and elevated C4c, except for higher perceived severity of constipation in the group with elevated C4c (table 3). In line with these findings, C4c only correlated significantly with FGF19 (r=−0.23: p=0.02), triglycerides (r=0.29; p=0.001), HDL cholesterol (r=−0.20; p=0.02), BMI (r=0.20; p=0.02) and stool frequency (r=0.22; p=0.01).
Comparisons between patients with IBS with and without abnormal 75SeHCAT retention (<10%)
Comparisons between patients with IBS with and without high C4c values (>8.0 mg/mol for men and >6.0 mg/mol for women)

Correlation between colonic transit time and 75SeHCAT retention values in patients with IBS.
When comparing patients with IBS with low (n=14) FGF19 levels with the rest of the patients with IBS (n=104), no significant group differences were noted (data not shown).
Open-label treatment with colestipol
Of the 141 investigated patients, 57 (40%) had a 75SeHCAT retention value < 20%, and 27 of these (47%) agreed to participate in the open-label treatment trial with colestipol. Twenty-three patients completed the 8-week treatment period, whereas four patients discontinued prematurely, one after 3 weeks, two after 4 weeks and one after 6 weeks. All four stated that lack of effect was the reason for discontinuing the medication.
During the treatment IBS-SSS scores were reduced (F=10.38; p<0.001), reaching statistical significance at week 6 and week 8 (figure 3A). The stool frequency was reduced from baseline to week 8 (2.8±1.4 stools/day vs 2.3±1.2 stools/day; p=0.03), but the stool form remained unaltered (Bristol Stool Form score 4.3±1.4 vs 3.9±1.1; p=0.24). Fifteen of the 27 patients (55%) fulfilled criteria for treatment response (reporting adequate relief ≥50% of weeks 5–8). The weekly responder rate is shown in figure 3B. There were no differences in any of the baseline parameters between responders and non-responders (table 4), and no differences in the clinical response were seen between patients with 75SeHCAT retention values at baseline <10% and those with 10–20% (data not shown). The mean colestipol intake per week increased from 21±5 g at week 1 to 74±41 g at week 8, but the colestipol dose had already reached a peak value after week 7 (figure 3C).
Comparisons between responders and non-responders to colestipol treatment (responder definition: reporting adequate relief ≥50% of weeks 5–8)

{kind=link}
{kind=link}
{kind=link}
Treatment response to colestipol treatment demonstrated as the biweekly IBS Severity Scoring System (IBS-SSS) scores (mean±SD) (A) and the weekly proportion of patients reporting adequate relief of their IBS symptoms (B), as well as the weekly colestipol dose in the treatment group (mean±SD) (C). ** p<0.01 versus baseline.
Discussion
This is the first large scale study assessing abnormalities in bile acid absorption and synthesis in phenotypically well-characterised patients with IBS, by use of the 75SeHCAT retention test, as well as C4c and FGF19 concentration in serum. A substantial proportion of patients with IBS had findings consistent with abnormalities in bile acid absorption and/or synthesis, associated with more frequent and looser bowel movements and an accelerated colonic transit time, as well as with overweight and abnormal serum lipid profiles. The major importance of our findings is that they strengthen the involvement of increased bile acid exposure in the colon as a partial mechanism for symptom generation in patients with especially non-constipated IBS, that is, IBS-D and IBS-A.
Few studies have focused on the role of bile acids regarding symptom generation in functional GI disorders apart from some early studies suggesting a role for bile acids in the GI motor15 and secretory responses14 seen in IBS pathophysiology. BAM diagnosed with abnormal 75SeHCAT retention has also been suggested to be a frequent finding in patients seeking healthcare for unexplained diarrhoea, of which some satisfy diagnostic criteria for IBS-D.26 ,51––53 In one recent provocative study, IBS-D was proposed to be a fiction, since the majority of patients included was found to have another diagnosis explaining their symptoms, where BAM was the most common alternative diagnosis (68%),54 indicating that patients with predominant and severe diarrhoea need a more thorough clinical workup than other patients with suspected functional bowel disorder.55 Recently, the Mayo group used measurement of C4 in serum to demonstrate increased bile acid synthesis in patients with IBS-D, and found that a substantial proportion of these patients had evidence of BAM, whereas this was not seen in patients with IBS-C,18 ,19 and in a follow-up study they also showed that unconjugated faecal bile acids were associated with stool characteristics in IBS.56 Our study expands on these previous studies by including a larger group of well-characterised patients with IBS, including all IBS subtypes, and by using complementary techniques to define abnormalities in bile acid absorption and synthesis. A considerable proportion of our patients had demonstrable abnormalities, and this was seen in the IBS-D group, and in the IBS-A group, which has not been reported previously. This fits well with recent transit studies, where a proportion of patients with IBS with mixed/alternating bowel habit has accelerated colonic transit, just like patients with diarrhoea predominance.3 ,57 There was a substantial overlap between abnormal 75SeHCAT retention (18%) and an increased C4c (23%), but also a considerable number of subjects with only one of these tests being abnormal, indicating that the tests are complementary, but not interchangeable for detection of abnormalities in bile acid homoeostasis. Abnormal 75SeHCAT retention values were more closely associated with bowel habit in our IBS population, which make us believe that this is a better method to use in the evaluation of patients with IBS than C4c.
Among the key symptoms of IBS, that is, abdominal pain and/or discomfort and abnormal bowel habit, increased bile acid load to the colon seems to be of importance for loose and frequent stools in IBS, whereas pain, bloating and abdominal discomfort were not associated with abnormal 75SeHCAT retention or serum C4c levels. This is in agreement with a French study, where faecal bile acid concentration was associated with stool frequency and consistency, but not with pain and bloating.58 Moreover, genetic variants in the Klotho β gene, encoding a protein serving as cofactor for FGFR-4, the presumable receptor for FGF19, have been demonstrated in patients with IBS-D and found to be associated with faster colonic transit in these patients, further strengthening the importance of bile acids for colonic transit and bowel habit in IBS.59
Treatment options modulating the bile acid exposure to the colon are under evaluation. An ileal bile acid transporter inhibitor, elobixibat (formerly A3309), enhancing bile acid delivery to the colon accelerates colonic transit and results in looser and more frequent bowel movements in patients with constipation.60 ,61 Moreover, a delayed-release oral formulation of the bile acid chenodeoxycholate was shown to accelerate colonic transit and improve symptoms of constipation in women with IBS-C.17 For patients with IBS-D, the bile acid sequestrant colesevelam has been evaluated in a small proof-of-concept study with a tendency to delay colonic transit and improve symptoms of diarrhoea, and the response seemed to be influenced by genetic variants in proteins involved in the FGF19-mediated negative feedback of hepatic bile acid synthesis.16 In the present study we evaluated the bile acid binding agent colestipol in a small group of patients with IBS with 75SeHCAT retention below 20%, and found a favourable effect on IBS symptoms in approximately half of the subjects. However, this should only be regarded as a pilot study, which has to be confirmed by proper double-blind, placebo controlled trials, but the promising results and other recent treatment options modulating bile acid delivery to the colon, supports the concept that bile acid load to the colon is of importance for symptom generation in IBS and other functional bowel disorders. Disappointingly no factors predicting a positive clinical response to colestipol were detected and the effect on bowel habit was relatively modest.
It is noteworthy that the perceived symptom severity was not linked to either the 75SeHCAT retention, or the C4c. Only the objective characterisation of symptoms, that is, frequency of bowel movements and to some extent stool form was associated with bile acid exposure to the colon in our IBS sample. With the current study design, the underlying mechanisms for other IBS symptoms could not be revealed, but visceral hypersensitivity and brain-gut dysfunction are putative candidates.4 ,62 Interestingly, the pain threshold for rectal distension was higher in patients with low 75SeHCAT retention values compared with those with normal ones. As these same patients also tended to be overweight, this finding is in line with a previous study that found a higher threshold for rectal pain in patients with BMI>25.63 However, opposite results also exist with bile acids increasing colonic sensitivity,9 so the effect of bile acids on colorectal sensitivity needs to be further addressed in future studies. One potential explanation for these somewhat surprising findings is that bile acids entering the colon and not visceral hypersensitivity is of relevance in one particular subset of patients with IBS, hence low 75SeHCAT retention values and normal/high rectal pain thresholds in these patients, whereas visceral hypersensitivity and not colonic bile acids is of importance in another group of patients with IBS, hence low rectal pain thresholds and normal 75SeHCAT retention values in this group. The association between a low 75SeHCAT retention value and an increased C4c and higher BMI, is in line with recent findings demonstrating increased BMI and a higher level of bile acid synthesis in patients with IBS-D.18 Moreover patients with idiopathic BAM often tend to be overweight and have accelerated gut transit,48 and an association between BMI and GI transit in health and different diseases has been observed.47 ,49 ,63 The cause and effect needs to be determined in future studies, but based on current knowledge it seems likely that high BMI may lead to increased bile acid synthesis and an increased bile acid delivery to colon, which accelerates transit resulting in looser and more frequent stools.
Bile acids, when absorbed into the enterocytes, are believed to trigger the synthesis and secretion of FGF19, which in turn may inhibit hepatic bile acid synthesis.46 ,64 We found an inverse correlation between plasma FGF19 and the C4c. If patients with idiopathic BAM have an inadequately low FGF19 response to absorbed bile acids into the enterocyte and a compensatory high hepatic synthesis this could result in an enlarged bile acid pool. This impaired FGF19 feedback inhibition has recently been proposed as a major mechanism in BAM.65 However, in our group of patients with IBS FGF19 levels were not different when compared with the healthy controls despite differences in C4c, whereas patients with IBS and low 75SeHCAT retention values and/or high C4c levels demonstrated reduced FGF19 levels, indirectly implicating a potential role for defect FGF19 feedback inhibition in subgroups of patients with IBS as well. This is in line with a recent study in patients with diarrhoea, where correlations between FGF19, C4 and 75SeHCAT were most marked in patients with low 75SeHCAT retention values.66
To conclude, the 75SeHCAT test, as a measure of the bile acid turnover rate, correlates with hepatic bile acid synthesis and relates to bowel habit and colonic transit time in patients with IBS. The associations with BMI and with markers of general metabolism such as plasma lipid profiles and bile acid metabolism deserve further investigations, including intervention trials. The positive symptomatic response to open label treatment with bile acid binders in patients with IBS with low 75SeHCAT values supports a role of bile acids in IBS symptomatology, but placebo-controlled studies are warranted.
Acknowledgments
The authors thank Ingela Arvidsson for expert technical assistance and RN Jenny Lövdahl for patient management.
References
Footnotes
-
Contributors AB: study concept and design, acquisition of data, analysis and interpretation of data; drafting of the manuscript, critical revision of the manuscript for important intellectual content. HT: analysis and interpretation of data, critical revision of the manuscript. MR and K-AU: acquisition of data, critical revision of the manuscript. MS: study concept and design, acquisition of data, analysis and interpretation of data; critical revision of the manuscript.
-
Funding This study was supported by the Swedish Medical Research Council (grants 13409, 21691 21692 and 2012–1738), Region Västra Götaland ((KVG project Nr 84), the Marianne and Marcus Wallenberg Foundation, University of Gothenburg, Centre for Person-Centred Care (GPCC), Sahlgrenska Academy, University of Gothenburg and by the Faculty of Medicine, University of Gothenburg and by Stockholm County Council (ALF).
-
Competing interests AB and K-AU have served as Consultants/Advisory board members for Albireo and GE Health Care. MR has received a research grant and served as a Consultant for Albireo. HT has served as a Consultant/Advisory Board member for Almirall, Danone and Shire. MS has received unrestricted research grants from Danone and AstraZeneca, and served as a Consultant/Advisory Board member for Danone, Novartis, Almirall, Albireo and Shire.
-
Ethics approval The Regional Ethical Review Boards in Gothenburg and Stockholm.
-
Provenance and peer review Not commissioned; externally peer reviewed.