Article Text

Abstract
Background: Inflammatory bowel disease (IBD) has a typical onset during the peak reproductive years. Evidence of the risk of adverse pregnancy outcomes in IBD is important for the management of pregnancy to assist in its management.
Aim: To provide a clear assessment of risk of adverse outcomes during pregnancy in women with IBD.
Design: The Medline literature was searched to identify studies reporting outcomes of pregnancy in patients with IBD. Random-effect meta-analysis was used to compare outcomes between women with IBD and normal controls.
Patients and setting: A total of 3907 patients with IBD (Crohn’s disease 1952 (63%), ulcerative colitis 1113 (36%)) and 320 531 controls were reported in 12 studies that satisfied the inclusion criteria.
Results: For women with IBD, there was a 1.87-fold increase in incidence of prematurity (<37 weeks gestation; 95% CI 1.52 to 2.31; p<0.001) compared with controls. The incidence of low birth weight (<2500 g) was over twice that of normal controls (95% CI 1.38 to 3.19; p<0.001). Women with IBD were 1.5 times more likely to undergo caesarean section (95% CI 1.26 to 1.79; p<0.001), and the risk of congenital abnormalities was found to be 2.37-fold increased (95% CI 1.47 to 3.82; p<0.001).
Conclusion: The study has shown a higher incidence of adverse pregnancy outcomes in patients with IBD. Further studies are required to clarify which women are at higher risk, as this was not determined in the present study. This has an effect on the management of patients with IBD during pregnancy, who should be treated as a potentially high-risk group.
- ASA, aminosalicylic acid
- IBD, inflammatory bowel disease
- LBW, low birth weight
- RPC, restorative proctocolectomy
- SGA, small for gestational age
- WMD, weighted mean difference
Statistics from Altmetric.com
- ASA, aminosalicylic acid
- IBD, inflammatory bowel disease
- LBW, low birth weight
- RPC, restorative proctocolectomy
- SGA, small for gestational age
- WMD, weighted mean difference
The incidence of inflammatory bowel disease (IBD) peaks during the reproductive years. In European countries, the incidence rates of ulcerative colitis and Crohn’s disease, reported from a large multi-centre epidemiological study, are 10.4/100 000 and 5.6/100 000 per year, respectively.1 Opinion on the effect of IBD on pregnancy is varied, with several studies reporting that IBD does not have an adverse effect on the outcome of pregnancy.2–5 Several population-based case–control studies have reported no increase in still birth, neonatal death or spontaneous abortion.6–8 An association between IBD and premature births (<37 weeks) and low-birthweight (LBW) infants (<2500 g) has been described.6–9
Premature births result in 75% of neonatal deaths and most neonatal intensive care admissions.10 A substantial effect of premature birth on long-term physical and mental health is observed.11 Babies born at <28 weeks gestational age spend 85 times longer in hospital than babies born at term, representing a considerable healthcare cost.12 Even among babies born after 32 weeks, educational and behavioural problems can occur in 1 in 3 children at 7 years of age,13 with 25% of children born between 32 and 35 weeks gestational age requiring support from non-teaching assistants at school.14
LBW is associated with poor outcomes in cognitive function, academic achievement, behaviour and social adaptation.15,16 LBW is also associated with an increased risk of cardiovascular disease and other chronic illnesses.17 In view of the potential for adverse pregnancy outcomes in IBD, such women should be referred routinely as cases of high-risk, regardless of disease activity.
The present study uses meta-analytical techniques to compare the incidence of adverse outcomes during pregnancy in patients with IBD with that in controls.
METHODS
Study selection
A Medline literature search was conducted on all studies published between 1980 and 2006 reporting comparisons of pregnancy outcomes between women with and without IBD. The following MESH search headings were used “inflammatory bowel disease”, “pregnancy”, “outcomes”, “ulcerative colitis” and “Crohn’s disease”.
The articles were also identified using hand searching of references and the related articles function in PubMed. No language restrictions were observed. All of the abstracts, studies and citations scanned were reviewed. The latest date for this search was 18 May 2006.
Data extraction
Data extraction was conducted independently by JC and ET. The following information was extracted from each study: first author, year of publication, characteristics of the study population, study design (prospective, retrospective or other), inclusion and exclusion criteria, number of participants in each group (controls, ulcerative colitis and Crohn’s disease), quality of study, gestation, birth weight, mode of delivery, still births, congenital abnormalities and size for gestational age. Definitions of the outcomes of interest are given in appendix A.
Inclusion criteria
We included only studies comparing patients with IBD with normal controls, and those that reported on pregnancy outcomes.
Exclusion criteria
Studies in which the outcomes of comparison were not reported or it was not possible to extract the data from the published results and those that did not report on the pregnancy outcomes being analysed were excluded.
Statistical analysis
The meta-analysis was performed in line with the recommendations from the Cochrane Collaboration and the Quality of Reporting of Meta-analyses (QUORUM) guidelines.18,19 Statistical analysis of dichotomous variables was carried out using odds ratio (OR) as the summary statistic, whereas continuous variables such as birth weight or gestational age were analysed using the weighted mean difference (WMD)20; both were reported with 95% confidence intervals (CI). ORs represent the odds of an adverse event occurring during pregnancy in a patient with IBD compared with a control. The WMD summarises the differences between the two groups with respect to continuous variables, accounting for sample size. For studies that presented continuous data as means and range values, the standard deviations (SD) were calculated using statistical algorithms and checked using “bootstrap” resampling techniques. Thus, all continuous data were standardised for analysis. An OR of <1 favoured the control population and the point estimate of the OR was considered significant at the p<0.05 level if the 95% CI did not include the value 1. In the tabulation of results, squares indicate the point estimates of the effect of disease (OR, WMD), with 95% CI indicated by horizontal bars. The diamond represents the summary estimate from pooled studies with 95% CI.
The quality of the non-randomised studies was assessed by using the Newcastle-Ottawa scale.21 The quality of a study was evaluated by examining patient selection methods, comparability of the study groups and assessment of outcome. Studies achieving ⩾7 stars were considered to be higher quality. Heterogeneity was assessed by two methods. Firstly, graphical exploration with funnel plots was used to evaluate the publication bias. Secondly, sensitivity analysis was undertaken using the following subgroups: studies of higher quality, those published in or after 2000, and those reporting on >40 patients overall. Analysis was conducted by Review Manager V.4.2.
RESULTS
Eligible studies
The literature search identified 13 studies comparing the pregnancy outcomes of women with and without IBD. One study was excluded from the meta-analysis as the incidence of the outcomes of interest was not clearly reported.22 The remaining 12 studies, published between 1986 and 2005, matched the selection criteria and were therefore included in this meta-analysis.6–9,23–30 Analysis was carried out on a total of 3907 patients with IBD and 320 531 controls. Of the 10 studies that identified subgroups of IBD, 63% had Crohn’s disease (n = 1952) and 36% ulcerative colitis (n = 1113). Table 1 shows the study characteristics. One of the 12 studies was prospective,6 with the remaining 11 being retrospective case–control studies. Ten studies matched their patients with controls for ⩾1 variable, with two studies not matching for any variables.8,28
Study characteristics
Gestation
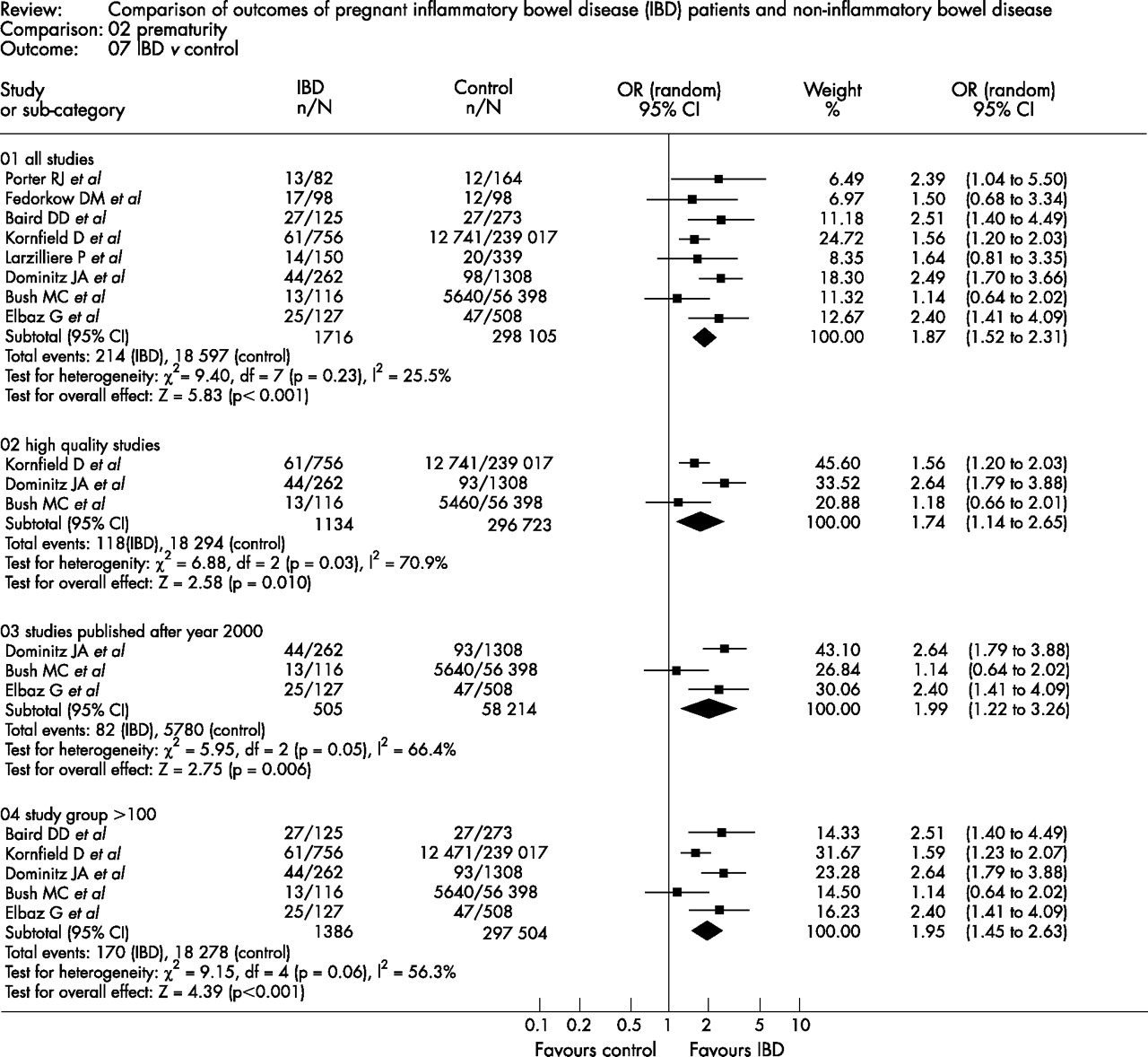
Eight of the 12 studies reported on the incidence of premature birth (<37 weeks gestation) in 1716 patients with IBD versus 298 105 controls(table 2).6,9,23–27,30 Patients with IBD were more likely to have premature infants than controls (OR 1.87; 95% CI 1.52 to 2.31; p<0.001). Analysis of patients with Crohn’s disease versus controls7,9,23–25,29,30 (OR 1.97; 95% CI 1.36 to 2.87; p<0.001) and patients with ulcerative colitis versus controls8,9,23–25,30 (OR 1.34; 95% CI 1.09 to 1.64; p<0.005) also showed significant differences in the incidence of premature gestation. In the five studies that compared Crohn’s disease with ulcerative colitis, there was no significant difference in the incidence of prematurity (fig 1).9,23–25,30.
Pregnancy outcomes in inflammatory bowel disease versus controls
Test for heterogeneity: χ2 statistic with its degrees of freedom (df) and p value. Inconsistency among results: I2 test for overall effect; Z statistic with p value. OR, odds ratio, CI, confidence interval.
Birth weight
Three studies reported on the incidence of LBW (<2500 g) in infants born to patients with IBD versus controls.6,9,26 A significant difference was observed in the incidence of LBW in infants born to mothers with IBD (OR 2.1; 95%; CI 1.38 to 3.19; p<0.001). The incidence of LBW in ulcerative colitis8,9 was not significant, but there was a significant difference in the incidence of LBW in infants born to mothers with Crohn’s disease7,9 (OR 2.82; 95% CI 1.42 to 5.60; p = 0.003).
Mode of delivery
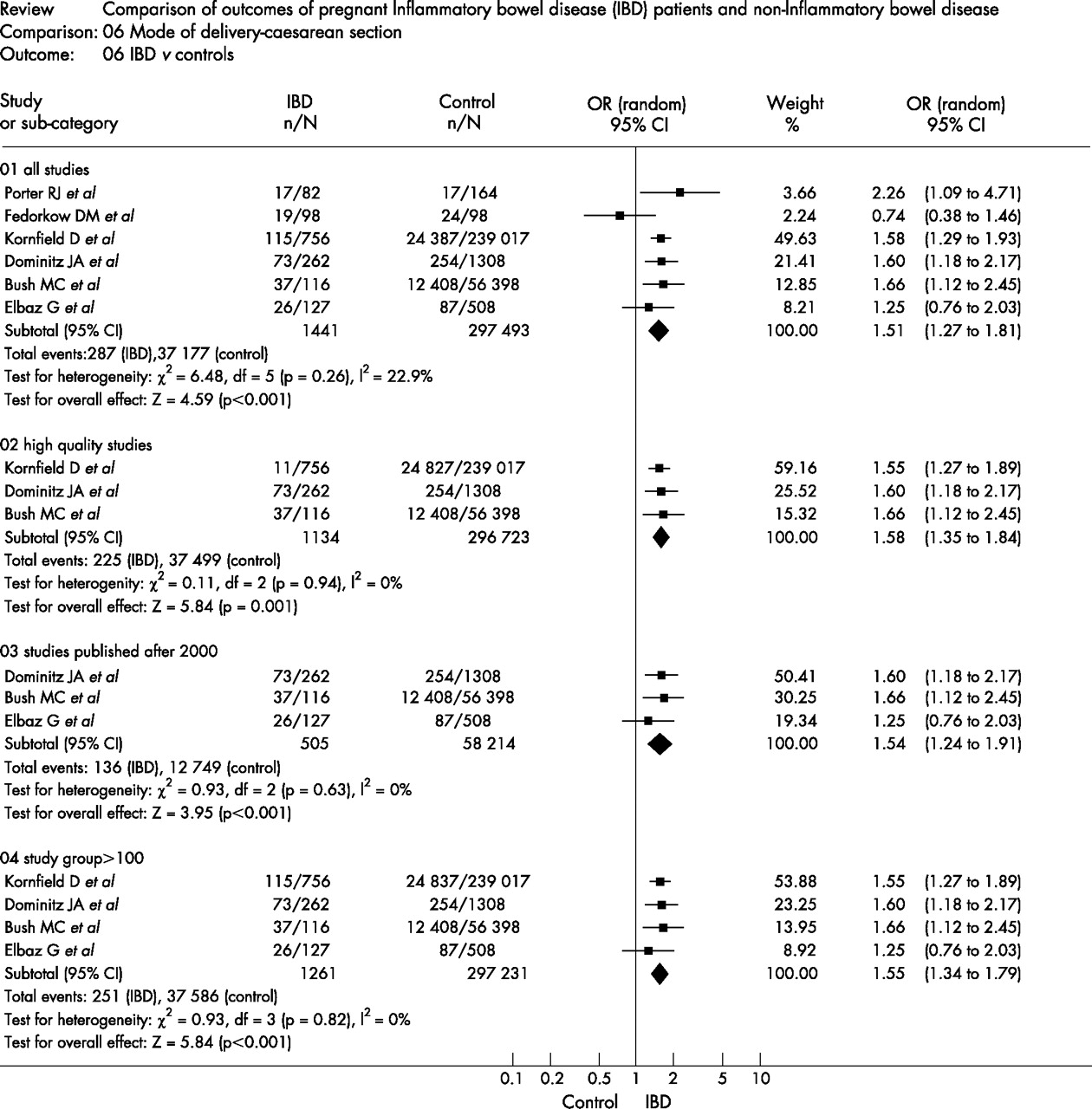
Six studies reported on the caesarean section rates in patients with IBD and in controls6,24–27,30 (table 2). A significant increase was seen in the incidence of caesarean section in patients with IBD versus controls (fig 2; OR 1.5; 95% CI 1.26 to 1.79; p<0.001). The incidence of caesarean section in patients with Crohn’s disease versus controls24,25,29,30 was also significant (OR 1.65; 95% CI 1.19 to 2.29; p = 0.003), but not in patients with ulcerative colitis versus controls.24,25,30 No significant difference was seen between ulcerative colitis and Crohn’s disease.24,25,28,30
Test for heterogeneity: χ2 statistic with its degrees of freedom (df) and p value. Inconsistency among results: I2 test for overall effect: Z statistic with p value. OR, odds ratio, CI, confidence interval.
Small for gestational age
Four studies reported on the incidence of small for gestational age (SGA) in patients with IBD versus controls.6,25–27 No significant difference was seen between patients with IBD and controls, ulcerative colitis and controls,8,25 Crohn’s disease and controls,25,29 and between Crohn’s disease and ulcerative colitis.24,25
Still births
Four studies reported on the incidence of still births in a group of patients with IBD versus a control group.6,25–27 No significant difference was found in the rates of still births between patients with IBD and controls. No significant difference was found in the incidence of still births between patients with Crohn’s disease and controls.7,23,30
Congenital abnormalities
Four studies reported on the incidence of congenital abnormalities between patients with IBD and controls9,25–27 and did not show a significant difference. A significant difference was found in the incidence of congenital abnormalities in patients with ulcerative colitis versus controls9,25 (OR 3.88; 95% CI 1.41 to 10.67; p = 0.009), but not in patients with Crohn’s disease versus controls (p = 0.06).9,25,29
Sensitivity analysis
Higher quality studies (⩾7 stars)
Analysis of the higher quality studies6,7,24,25,27,29 showed that there was a significant difference between patients with IBD and control populations in three outcomes(table 3). An increase in the risk of premature birth (OR 1.74; 95% CI 1.14 to 2.65; p = 0.01), small for gestational age (OR 1.96; 95% CI 1.01 to 3.81; p = 0.05) and the rates of caesarean section (OR 1.58; 95% CI 1.35 to 1.84; p<0.001) was seen for patients with IBD.
Sensitivity analysis of pregnancy outcomes in subgroups with inflammatory bowel disease versus controls
Studies published in or after 2000
More recent studies were analysed, with six studies published in or after 2000(table 3).8,24–26,28,29 Results remained consistent with the overall analysis of all studies and the high-quality studies for the outcomes of premature birth24–26 (OR 1.99; 95% CI 1.22 to 3.26; p<0.01) and incidence of caesarean section 24–26 (OR 1.54; 95% CI 1.24 to 1.91; p<0.001). However, the later studies did not find that the incidence of SGA was significantly increased in the population with IBD. A significant difference was observed in the incidence of congenital abnormalities in patients with IBD25,26 (OR 2.39; 95% CI 1.28 to 4.48; p<0.01), which was not reported in the higher quality studies or in the overall analysis.
Studies reporting on ⩾100 patients
Analysis of the studies that reported on ⩾100 patients with IBD6–8,23–26 showed that the result was consistent with the overall results and the analysis of later studies (table 3). Significant differences were observed in the risk of LBW (OR 1.77; 95% CI 1.36 to 2.31; p<0.001), premature birth (OR 1.94; 95% CI 1.43 to 2.64; p<0.001), congenital abnormalities (OR 2.39; 95% CI 1.28 to 4.48; p<0.01) and the rates of caesarean section (OR 1.55; 95% CI 1.34 to 1.79; p<0.001) in women with IBD. No significant difference was found for the risk of SGA.
Publication bias
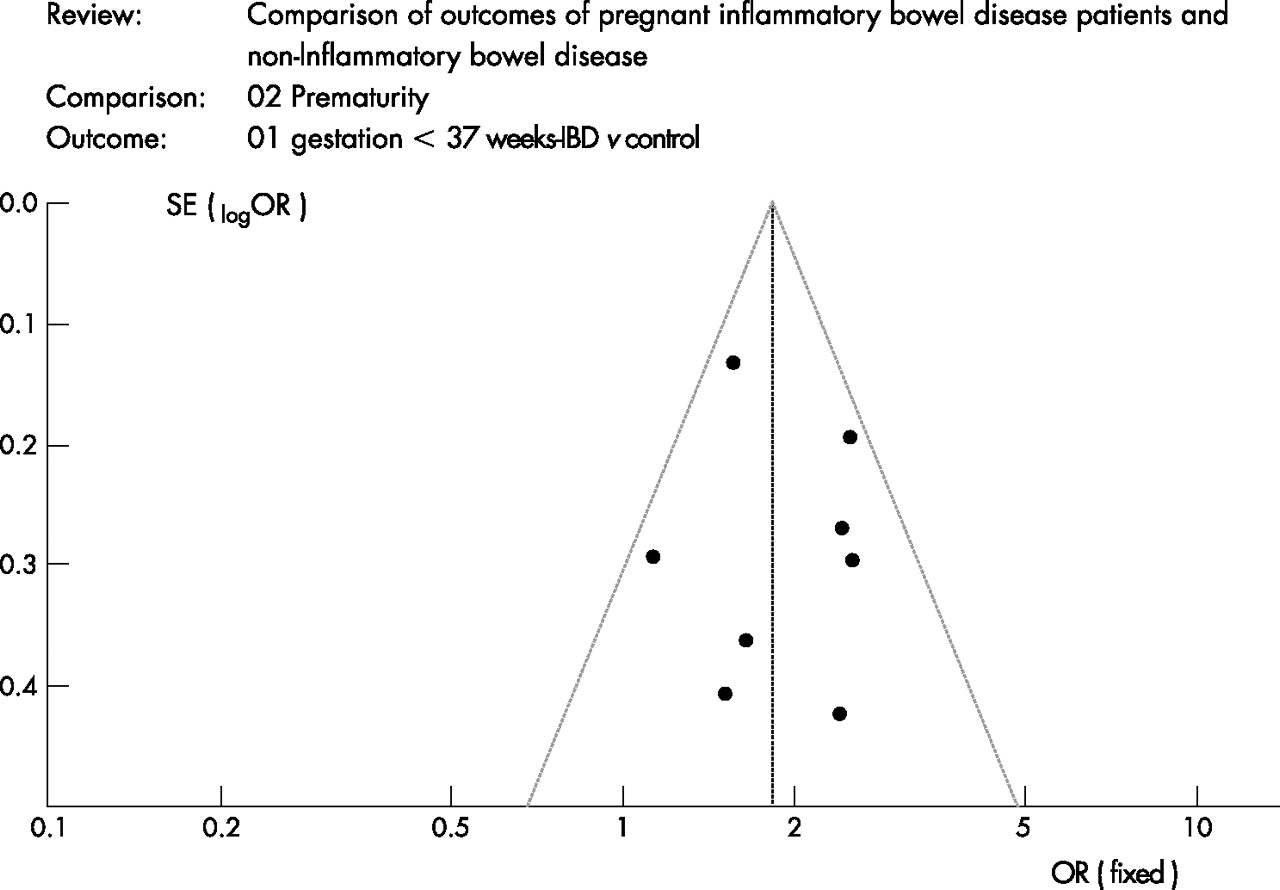
Figure 3 shows a funnel plot of the studies used in this meta-analysis reporting on the incidence of premature birth. This is a scatter plot showing the incidence estimated from individual studies plotted on the horizontal axis (OR), against the standard error (SE) of the estimate shown on the vertical axis (SE (logOR)). None of the studies lay outside the 95% CI limits. No evidence of publication bias or heterogeneity among the studies was seen; all of the studies were equally distributed around the vertical axis (p = 0.23). No evidence of bias was found in the incidence of LBW, caesarean section or congenital abnormalities.
{kind=link}
{kind=link}
{kind=link}
Funnel plot analysis of premature birth in patients with inflammatory bowel disease (IBD) versus controls. This is a scatter plot of the incidence estimated from individual studies plotted on the horizontal axis (OR), against the standard error (SE) of the estimate shown on the vertical axis (SE (logOR)).
DISCUSSION
The results of the present meta-analysis suggest that women with IBD are more likely to experience adverse pregnancy outcomes, in particular premature birth, LBW and a caesarean section. Patients with IBD were nearly twice as likely to have a premature delivery (<37 weeks gestation) as the normal population, a result which remained significant after the sensitivity analysis. No significant difference was seen in premature birth between patients with Crohn’s disease and those with ulcerative colitis. The effect of premature delivery on an infant’s physical, mental and social health may be substantial,12,13,16,17 and women with IBD must be aware of the increased risk of prematurity in their babies.
The OR of a woman with IBD having an infant with LBW (<2500 g) was 2.1 (p<0.001). This remained consistent in the sensitivity analysis of studies reporting on ⩾100 patients with IBD; the outcome was not reported in the higher quality studies or studies published after 2000. Women with Crohn’s disease were nearly three times more likely to have an infant with LBW (p = 0.003), but not those with ulcerative colitis.
A higher rate of caesarean sections was seen in women with IBD than in the normal population. This was corroborated in all of the sensitivity analysis subgroups. A higher rate of caesarean sections was seen in patients with Crohn’s disease versus controls, but not in those with ulcerative colitis. No significant difference was observed between ulcerative colitis and Crohn’s disease; however, the number of patients was small. A large study to specifically compare the mode of delivery between the two groups is required in the future. The rationale behind the increased number of caesarean sections in patients with IBD is not dealt with in the studies analysed. No data exist on whether the caesarean sections were elective or emergencies or whether the outcomes of the infants differed after vaginal delivery and caesarean section. Controversy exists over the most appropriate method of delivery for patients with IBD, with some studies reporting that the risk of incontinence and anal sphincter tears is less in caesarean section than in vaginal delivery.31–34 This is disputed in other studies, which say that anal sphincter tears that occur in vaginal deliveries do not affect continence35 and that vaginal delivery reduces surgical procedures and adhesion formation in a group of high-risk patients.
Previous studies have suggested an association between patients with IBD—in particular, patients with Crohn’s disease—and SGA29; however, this was not shown in this meta-analysis. The results of the present study showed no increase in the incidence of SGA (small for gestational age) in the population with IBD in comparison to the normal population, or in patients with Crohn’s disease versus ulcerative colitis. This was confirmed in the sensitivity subgroup analysis for studies published in or after 2000 and for studies reporting on ⩾100 patients with IBD.
No significant difference was found in the incidence of still births in women with IBD and the normal population. The results of the sensitivity analysis also found no significant differences. There have been previous reports of an association of IBD with an increased risk of still births, although often in active disease.36
No significant difference was found in the risk of congenital abnormalities in women with IBD and the normal population; however, a significant difference was found in the subgroup analysis for later studies and those with larger patient groups. The analysis of all of the studies did find a significant difference in the risk of congenital abnormalities in patients with ulcerative colitis versus controls, but not in patients with Crohn’s disease. The studies that reported on congenital abnormalities did not distinguish between the major and minor malformations; one study included chromosomal disorders,25 which may result in overestimation of the risk. One large case–control study37 compared the Hungarian congenital abnormality registry with data from the national birth registry office. The authors reported no overall increase in the risk of congenital abnormalities for patients with ulcerative colitis compared with controls; however, they did report an increased risk of selected congenital abnormalities. Further prospective studies are required, with clarification of the type of malformations.
It is important to mention the limitations of this meta-analysis. It would be difficult and potentially unethical to perform a randomised controlled trial for the pregnancy outcomes; we must therefore base our clinical decisions on observational studies that are vulnerable to bias and confounding variables. The low frequency of the adverse outcomes makes statistical precision difficult. The studies included in the meta-analysis did not report on disease activity in relation to adverse outcomes. Previous studies have suggested that if a woman conceives while her disease is active, she is more likely to have a premature infant or one with LBW than a woman who has quiescent disease activity.23,38 The incidence of still births and spontaneous abortions is also related to disease activity.39 A prospective study reporting on adverse outcomes and the association with disease activity is still required. In view of the probable increased risk of adverse pregnancy outcomes with active disease, the management of pregnancy in patients with IBD needs to focus on maintaining disease remission before and during pregnancy.
A total of 19 articles have been published to date on the effect of 5-aminosalicylic acid (5-ASA), corticosteroids, azathioprine and anti-tumour necrosis factor α drugs (anti-TNFα) for inflammatory bowel disease on pregnancy outcomes (table 4). These included two prospective studies and 17 retrospective studies on 1626 women. The results of a pooled analysis suggested no significant increase in the incidence of still births, ectopic pregnancies, spontaneous abortions or LBW for five ASA group of drugs, corticosteroids, azathioprine or anti-TNFα. An increase was seen in the number of congenital abnormalities for 5-ASA, anti-TNFα and azathioprine; however, this may relate to the increased risk for women with IBD and not drug effects. A substantial increase was observed in the number of therapeutic terminations for fetuses exposed to anti-TNFα during pregnancy, with one study reporting a 19% rate of therapeutic terminations.40 Whether the reason for the termination was drug exposure or another factor is not known. This has substantial implications if the number of adverse events in pregnancy is not increased after exposure to the drug.
Effect of drugs for inflammatory bowel disease on outcomes of pregnancy
Heterogeneity was seen in some results, which we tried to account for by sensitivity analysis. One limitation of the sensitivity analysis is that many of the larger studies have been published recently, and thus were in both subsets. Most of the studies did not report on disease activity of the patients with IBD or the drugs that the women were taking. Patients with a higher disease activity are reported to have an increased incidence of adverse pregnancy outcomes.23 However, this meta-analysis also has its strengths, with large numbers of patients being analysed at once, which would have been difficult to gather in one primary randomised controlled trial.
In conclusion, women with inflammatory bowel disease have an increased risk, twice that of the normal population, of having a small or premature baby. Women who have IBD are more likely to have a caesarean section, especially those with Crohn’s disease. The surgeon and obstetrician need to discuss between themselves the management of delivery in women with IBD. A definitive study is required to settle the issue of best management and from this a new set of guidelines, to help both patients and their clinicians determine best practice.
APPENDIX A
OUTCOMES OF INTEREST AND DEFINITIONS
Premature birth: <37 weeks gestation.6,23–25,27
Birth weight: low birth weight (LBW) was defined as <2500 g and very low birth weight (VLBW) as <1500 g.6,24,25,27
Size for gestational age: birth weight <10th centile of the gestational age.26,29
Incidence of congenital abnormalities: diseases existing at birth and often before birth, or that develop during the first month of life (infant, newborn, diseases), regardless of causation. Of these diseases, those characterised by structural deformities are termed abnormalities.
Still births: babies born dead in the last 12 weeks of pregnancy.41
Perinatal mortality: number of still births and deaths in the first week.7,8
Mode of delivery: vaginal delivery, caesarean section, forceps and vacuum delivery.
REFERENCES
Footnotes
-
Published Online First 21 December 2006
-
Funding: None.
-
Competing interests: None.
Linked Articles
- Digest