Article Text

Abstract
The British Society of Gastroenterology (BSG) and the Association of Coloproctology for Great Britain and Ireland (ACPGBI) commissioned this update of the 2002 guidance. The aim, as before, is to provide guidance on the appropriateness, method and frequency of screening for people at moderate and high risk from colorectal cancer. This guidance provides some new recommendations for those with inflammatory bowel disease and for those at moderate risk resulting from a family history of colorectal cancer. In other areas guidance is relatively unchanged, but the recent literature was reviewed and is included where appropriate.
- Colorectal cancer
- inflammatory bowel disease
- colorectal adenomas
- colorectal cancer screening
- family cancer
Statistics from Altmetric.com
- Colorectal cancer
- inflammatory bowel disease
- colorectal adenomas
- colorectal cancer screening
- family cancer
Introduction
The British Society of Gastroenterology (BSG) and the Association of Coloproctology for Great Britain and Ireland (ACPGBI) commissioned this update of the 2002 guidance.1 The aim, as before, is to provide guidance on the appropriateness, method and frequency of screening for people at moderate and high risk from colorectal cancer. This guidance provides some new recommendations for those with inflammatory bowel disease and for those at moderate risk resulting from a family history of colorectal cancer. In other areas guidance is relatively unchanged, but the recent literature was reviewed and is included where appropriate.
Identifying moderate and high risk subjects is important, as is ensuring that subjects accept surveillance. The screening test comes at the end of a series of events dependent upon a number of issues including social, family and personal factors and the doctor's knowledge and perspective. Barriers to screening include the doctor's knowledge of risk and the subject's knowledge and perception of risk and fears about diagnosis and screening.2 A National Health Service (NHS) Bowel Cancer Screening Programme (http://www.cancerscreening.nhs.uk/bowel) is currently being introduced across the UK, providing general population screening for colorectal cancer and raising public awareness, which may help acceptance of screening. This document includes guidance for those at moderate and high risk from colorectal cancer, and for them advice and referral to local experts and clinical geneticists is essential. Clinicians should encourage those individuals falling outside of the moderate and high risk groups and those who have completed screening in accordance with this guidance to participate in their country's bowel cancer screening programme. It is recommended that some months before surveillance is due, there is a clinical validation of all patients considered at increased risk to ensure it is still appropriate and conforms to the latest guidance.
The National Health Service (NHS) Cancer Reform Strategy (http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_081006) acknowledges the need for high quality risk assessment and counselling for those at high risk from bowel cancer as a consequence of their family history, but currently there is variability in service delivery according to local circumstances and availability of resources. Further guidance on commissioning these services is awaited, but increasing demand and complexity of advice in this developing area makes this a matter of some urgency.
Process of guideline formulation
Experts within the fields of medical and surgical gastroenterology and clinical genetics have reviewed and evaluated the published evidence in their field and written guidelines based on this evidence. Authors used electronic sources including Medline, Embase and systematic reviews such as the Cochrane Library where appropriate. The authors did not all convene in face-to-face discussion but discussed electronically and amended manuscripts by email and after telephone conference. The guidelines conform to the system proposed by the North of England evidence based guidelines development project.3 4
Validity and grading of recommendations
Categories of evidence are as follows:
Ia: Evidence obtained from meta-analysis of randomised controlled trials
Ib: Evidence obtained from at least one randomised controlled trial
IIa: Evidence obtained from at least one well-designed controlled study without randomisation
IIb: Evidence obtained from at least one other type of well-designed quasi-experimental study
III: Evidence obtained from a well-designed non-experimental descriptive study, such as comparative studies, correlation studies and case studies
IV: Evidence obtained from expert committee reports or opinions or clinical experiences of respected authorities.
The evidence category is indicated in parentheses within the reference section.
Grading of recommendations
The strength of each recommendation is dependent upon the category of the evidence supporting it, and is graded according to the following system:
A: Evidence categories Ia and Ib
B: Evidence categories IIa, IIb, III
C: Evidence category IV.
These guidelines will be reviewed again in 2014.
Guidelines for follow-up after resection of colorectal cancer
Executive summary
The debate continues on the subject of patient follow-up after curative treatment for colorectal cancer. Further evidence in the research literature has failed to clarify the issue since publication of the last guidelines.
It is reasonable to offer CT imaging of the liver to asymptomatic patients within 2 years after potentially curative resection. Recommendation grade: B
Although there is no evidence that colonoscopic follow-up improves survival, it does yield some treatable tumours. It is recommended that a colonoscopy is done 5 years after surgery and thereafter every 5 years until the benefit is outweighed by co-morbidity. Patients found to have adenomas at the time of diagnosis of colorectal cancer or on follow-up surveillance should follow adenoma surveillance guidance, continuing surveillance at least 5-yearly until benefit is outweighed by co-morbidity Recommendation grade: B
Prevalence and incidence
There are around 30 000 new cases of colorectal cancer in England and Wales per annum. There is some evidence that the incidence of colorectal cancer is beginning to fall, probably because of greater public awareness of the disease and removal of adenomas at colonoscopy.5 6
Intervention
Follow-up for patients after resection of colorectal cancer is very variable but usually includes out-patient visits for a combination of clinical, haematological, radiological and endoscopic evaluation.
Detection of potentially curable recurrent disease
Four well-conducted systematic reviews are supportive of clinical follow-up, but three of them conclude that there is a lack of evidence to confirm or refute the premise that follow-up detects potentially resectable disease.7–11 However, one of these systematic reviews suggests that intensive follow-up can improve survival after colorectal cancer.8 Interestingly, this latter study largely relies upon the same trials as the other reviews but reaches a different conclusion.
Of five prospective randomised trials, those from Sweden,12 Finland,13 Denmark,14 and Australia15 failed to show a survival benefit at 5 years between patients subjected to intensive follow-up compared with minimal, or no, follow-up. An Italian trial found benefit for intensive follow-up.16 However, these five studies do not provide a definitive answer to possible survival benefit from follow-up for a variety of reasons:
All of the published trials were of low statistical power owing to small numbers and the fact that only a small proportion of patients with metastatic disease are potentially curable. The authors of the largest trial, which included almost 600 patients, concluded that their study was too small to demonstrate a reduction in mortality rate of less than 20% by intensive follow-up.14
There is no agreement as to what constitutes a ‘minimal’ follow-up regimen. In one study this included regular appointments every 3 months for 2 years, then 6-monthly visits. Each visit included clinical examination, liver function tests, faecal occult blood and carcino-embryonic antigen tests and colonoscopy at 5 years.15 In contrast, another study carried out no follow-up in the ‘minimal’ group.12
There is no uniform definition of ‘intensive’ follow-up. For example, liver scanning was not included in one study.14
Many centres have now adopted a policy of CT scanning to look for liver metastases at 1 and 2 years after treatment. This has happened largely as a result of data from liver resection specialists showing that patients with resectable liver disease have a 30% rate of 5-year survival compared with a very small prospect of 5-year survival if left untreated.7 8
In summary, despite a substantial number of new publications since the initial guidelines, the recommendations remain essentially unchanged. There is no evidence that intensive follow-up has a significant effect on survival, but neither is there evidence to the contrary. It is possible that liver imaging by ultrasound or CT may improve the likelihood of being able to offer a potentially curative hepatic resection in <5% of patients. It is therefore reasonable to undertake a CT scan in asymptomatic patients at some time in the first two postoperative years after curative resection. It must be stressed that many issues around the values of follow-up scans remain unresolved: the optimal timing and frequency of this investigation have not been determined, nor have the role of adjuvant chemotherapy and its timing in relation to hepatic surgery. More information on which to base the recommendation is urgently required. Relevant trials in the UK and Europe are in progress: the Follow-up After Colorectal Surgery (FACS) and the Gruppo Italiano di Lavoro per la Diagnosi Anticipata (GILDA) trials.
Surveillance for metachronous cancers
There is no evidence that colonoscopic surveillance improves survival after colorectal cancer resection. However, it is important to ensure that the colon has been completely visualised prior to resection or soon thereafter, because a proportion of patients will have synchronous polyps and cancers at the time of the original resection.17 18 The age at which endoscopic surveillance should cease should be a decision between doctor and patient and based on the risks and benefits of colonoscopy and comorbidities.
Provision of psychological support
There is limited evidence that follow-up is reassuring to most patients.19 20
Polyp cancers
Population screening for colorectal cancer will lead to the detection of more polyp cancers, which are defined as adenomatous polyps containing a focus of invasive adenocarcinoma (differing from severe dysplasia by breaching the basement membrane of the epithelium). Completeness of excision is easier to determine for lesions with a stalk than for those that are sessile. If there is doubt about completeness of the original excision, repeat endoscopic examination is recommended within 3 months of the index procedure; if the previous polypectomy site is identifiable at this examination, biopsy of the site and tattooing of the area are recommended. A further endoscopic examination of the area is recommended after a further 6 months. If the area appears healthy at this time the patient should revert back to BSG/ACPGBI guidance for adenoma surveillance.
Costs and benefits
The NHS tariff permits an estimate of costs for colorectal cancer follow-up, using £80 for a review out-patient visit, £170 for a CT scan of chest abdomen and pelvis and £476 for a colonoscopy. Assuming a relatively modest follow-up regime, a 6-monthly out-patient visit (over 5 years), with a CT scan at 1 year and a colonoscopy once in the 5 years of follow-up would cost £1100 per patient over 5 years, but only around half of colorectal cancer patients would survive to 5 years and some would be too frail for regular follow-up or invasive investigations. For a community with a population of 300 000, such a follow-up programme would probably cost around £250 000 per annum. This figure highlights the expense of clinical practice with uncertain benefits.
Audit
Surgeons are required to audit their practice as a part of their clinical governance arrangements. In order to audit the results of surgery some form of follow-up is essential.
Guidance on surveillance following detection of colorectal adenomas
This document revisits the guideline published in 2002,21 the recommendations of which are summarised below and in figure 1, and recommends no change.

Surveillance following adenoma removal.
The 2002 guideline provided evidence that the future risk of developing colorectal cancer or advanced adenomas (≥1 cm or high-grade dysplasia) after polypectomy varies according to the number and size of the adenomas removed at baseline colonoscopy. It suggested that patients could be divided into low, intermediate and high risk groups, and that the interval to the first follow-up examination could vary accordingly. The guideline also provided for reassessment of patient risk based on findings at the first and subsequent follow-up examinations.
No change is recommended because no data have been published since the last guideline to suggest otherwise. This situation could change within the next 2 years with publication of the results of research that is re-examining the long term safety of the no surveillance regimen for patients in the low risk group, and seeking to identify optimum surveillance intervals for patients in the higher risk groups. A National Institute for Health and Clinical Excellence (NICE) and an EU guideline on surveillance following polyp detection are in preparation.
The recommendations in this guideline are categorised as grade B, that is they are supported by evidence from well-designed but not randomised studies. Three randomised trials have examined the safety and efficacy of varying intervals for colonoscopic surveillance following adenoma removal.22–24 However, within these studies, the data from different surveillance groups were pooled for the purpose of risk stratification.
Executive summary
Risk of colorectal cancer or advanced adenomas (≥1 cm as measured at endoscopy or high-grade dysplasia)
Patients with only one or two small (<1 cm) adenomas are at low risk, and need no colonoscopic surveillance or 5-yearly until one negative examination then cease surveillance. Recommendation grade: B
Patients with three or four small adenomas or at least one adenoma ≥1 cm are at intermediate risk and should be screened 3-yearly until two consecutive examinations are negative. Recommendation grade: B
If either of the following is detected at any single examination (at baseline or follow-up): five or more adenomas, or three or more adenomas at least one of which is ≥1 cm, the patient is at high risk and an extra examination should be undertaken at 12 months before returning to 3-yearly surveillance. Recommendation grade: B
Patients can be offered surveillance until age 75 years and thereafter continue depending on relative cancer risk and co-morbidity. Colonoscopy is likely to be less successful and more risky at older ages. Further, the average lead time for progression of an adenoma to cancer is 10 years which is of the same order as the average life expectancy of an individual aged 75 years or older, suggesting that most will not benefit from surveillance. Recommendation grade: B
These guidelines are based on accurate detection of adenomas, otherwise risk status will be underestimated. Patients with a failed colonoscopy, for whatever reason, should undergo repeat colonoscopy or an alternative complete colonic examination. Recommendation grade: B
The site of large sessile adenomas removed piecemeal should be re-examined at 2–3 months. Small areas of residual polyp can then be treated endoscopically, with a further check for complete eradication in 2–3 months. India ink tattooing aids recognition of the polypectomy site at follow-up. If extensive residual polyp is seen, surgical resection needs to be considered, or alternatively referral to a colonoscopist with special expertise in advanced polypectomy techniques. If there is complete healing of the polypectomy site, then there should be a colonoscopy at 1 year, to check for missed synchronous polyps, before returning to 3-yearly surveillance. Recommendation grade: B
Intervention
Quality of colonoscopy
The efficacy and safety of the guideline depends on accurate detection of adenomas, otherwise risk status will be underestimated. Colonoscopy is not 100% sensitive, even when intubation to the caecum is achieved. Adenomas, advanced adenomas and cancers can be missed,25–29 particularly by endoscopists using poor technique. Miss rates for small adenomas are of the order of 25–50%,25–27 but the significance of this is as yet unclear. Of more concern is the observation that around 6–12% of larger adenomas (≥1 cm)26 29 and around 4% of cancers are missed at colonoscopy.28 Undertaking colonoscopy more frequently may not help. In two recently published chemoprevention studies, colorectal cancers were detected in 11 of 2915 patients within 2 years,30 and in 5 of 1561 patients within 1 year of colonoscopy.31
Most endoscopists examine the colon for polyps during withdrawal of the scope. Higher detection rates are associated with adequate distension, suction and cleaning, position change, and slow and meticulous examination of the colonic mucosa, including behind folds. The duration of the withdrawal phase, excluding time for biopsy and polypectomy, is a measure of quality of the examination. A withdrawal time of at least 6 min is associated with a higher adenoma detection rate compared to shorter withdrawal times.32 33 51
When a small polyp is detected during insertion, it is frequently difficult to relocate it on withdrawal. Where possible, consideration should be given to removing small polyps immediately on detection. Scanning the colonic mucosa during both insertion and withdrawal allows for essentially two examinations and potentially a reduction in the miss rate of small lesions. Removing larger lesions on insertion leaves an open area where tumours could seed and is therefore not generally advisable.
The ano-rectal junction is an area not easily visualised during insertion or withdrawal of the endoscope. Retroflexion and digital rectal examination reduce the risk of missing low rectal lesions. Retroflexion has been shown to increase the detection rate of lower rectal lesions safely, with acceptable levels of discomfort.34
There has recently been renewed interest in pancolonic indigo carmine dye spraying as an aid to polyp detection and characterisation. Several randomised trials have assessed its value.35–37 Although not totally consistent, they suggest that pancolonic dye spraying may improve the detection of small or flat lesions (both adenomatous and hyperplastic), particularly in the proximal colon, which may be of value in higher risk patients.
Incomplete or inadequate colonoscopy
The decision about whether to undertake a repeat examination after an incomplete or inadequate colonoscopy depends on patient factors such as age, risk group, the findings at the current examination, the difficulty of the examination and the potential risks of repeating it, along with the general health and concerns of the patient. It also depends on local factors such as waiting lists and whether the examination could be performed by a more experienced endoscopist.
Incomplete polypectomy
The importance of complete polyp removal and careful surveillance following piecemeal removal of large, flat adenomas was stressed (see Executive summary above). In a recent study of 830 cancers diagnosed in the USA, 45 (5.4%) cancers developed within 5 years of a complete colonoscopy, of which 27% developed at the site of a previous polypectomy.38 A similar observation was recorded in the St Mark's pre-colonoscopy era retrospective study, in which 11 of the 14 interval rectal cancers observed during 30 years of follow-up developed in patients who had had large sessile adenomas removed piecemeal and had refused follow-up to detect local recurrence.39
Impact of guideline on waiting lists
The publication of BSG/ACPGBI adenoma surveillance guidelines in 2002 produced a great deal of interest, and several units have performed audits to assess the impact of the guidelines on surveillance recall rates. One study reported a 47% reduction in adenoma surveillance colonoscopies resulting from adherence to the BSG/ACPGBI guidelines.40 A further audit of adenoma surveillance reported in abstract form confirmed a similar 49% reduction in adenoma surveillance workload,41 and two other abstracts have reported that a large proportion of patients with polyps are recalled either too early or unnecessarily.42 43 Several other abstracts report broadly similar results when assessing the BSG/ACPGBI colonoscopic surveillance guidelines as a whole.44–50
Adoption of the guideline by the NHS Bowel Cancer Screening Programme
With the introduction of the NHS Bowel Cancer Screening Programme (BCSP) and the consequent increase in the volume of colonoscopy, ensuring that surveillance colonoscopy is restricted to those who are most likely to benefit has assumed greater importance. The NHS bowel screening pilot studies undertaken in England and Scotland have shown that the detection rate of adenomas is 6–9 per 1000 examinations. The BCSP has adopted this guideline with a small modification in that it does not include an option for a 5-year follow-up colonoscopy in the low risk group. The reason is that the NHS needs to provide clear, unequivocal guidance for management of this large, relatively homogeneous group of asymptomatic individuals who would not in the past have been identified. The BSG guideline, in contrast, is designed essentially for all-comers, including symptomatic patients of all ages and physical conditions, and therefore has to offer some flexibility.
Conclusion
Although this update recommends no change from the advice given in the 2002 guideline, it emphasises two important factors which, in addition to individual patient factors, have a profound effect on risk: these are the quality of the performance of the examination, and ensuring complete removal of large sessile lesions.
In addition to the potentially therapeutic value of polyp removal, colonoscopy is an opportunity to identify a small, high risk group comprising patients who require careful surveillance to prevent the development of cancer. It is also an opportunity to identify a much larger group of patients who can be informed with some confidence that their risk is low. The overall effectiveness of an adenoma surveillance programme in preventing colorectal cancer depends on each colonoscopy being undertaken slowly, carefully and thoroughly with a fail-safe system in place for recall of higher risk patients.
Guidelines for screening and surveillance for asymptomatic colorectal cancer in patients with inflammatory bowel disease
This document updates the previous guideline published in 2002.52 For the sake of brevity, only changes to the previous guideline have been included. It is now widely accepted that surveillance for colorectal cancer is necessary for patients with inflammatory bowel disease (IBD), and that patients with ulcerative colitis have a similar risk to those with Crohn's colitis for a similar extent and duration of colonic involvement. Changes to the surveillance intervals have been made in the light of recent data demonstrating that endoscopic appearance is an important predictor of future dysplasia or cancer development.53 54 The surveillance intervals also take into account other recognised risk factors.
Executive summary
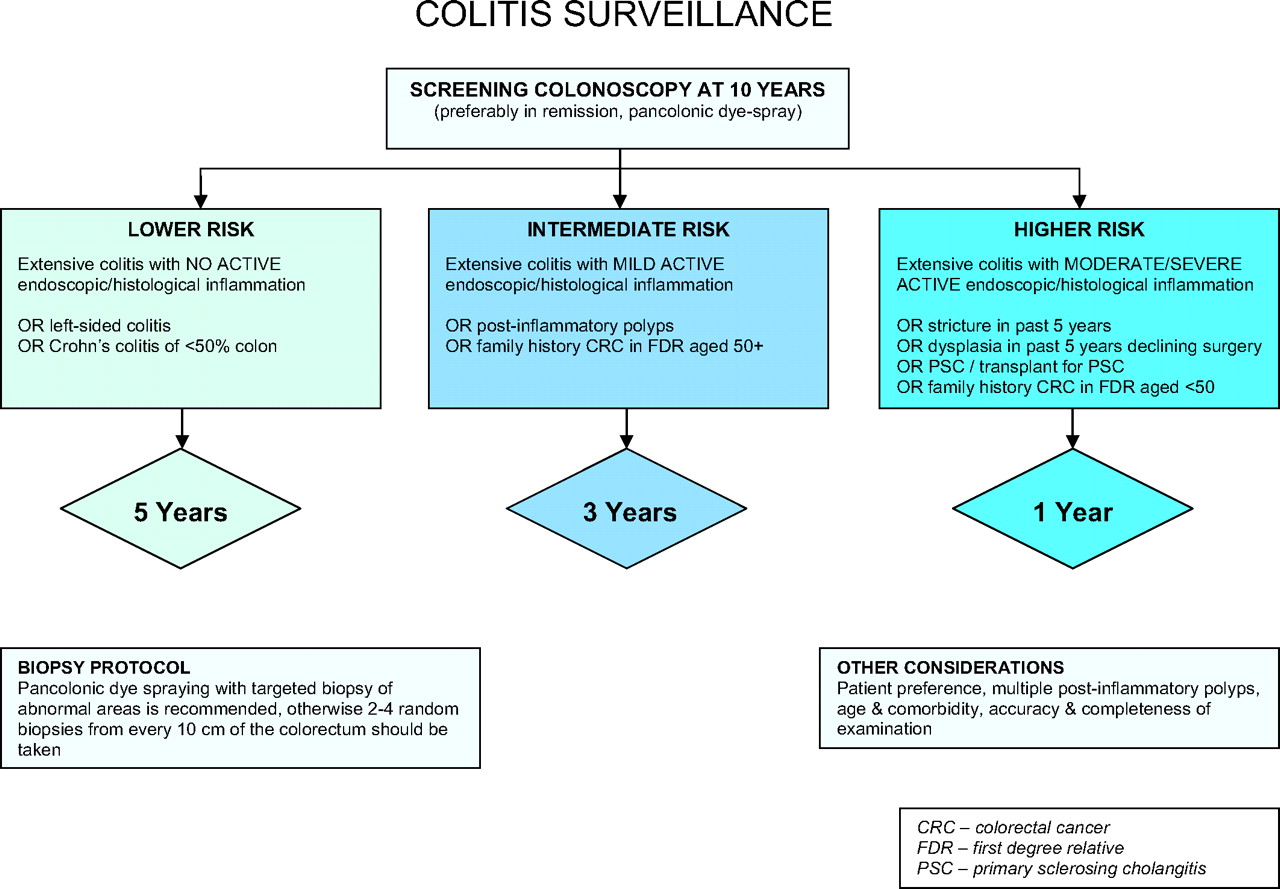
All patients with ulcerative colitis or Crohn's colitis should have a screening colonoscopy approximately 10 years after the onset of colitic symptoms to assess disease extent and other endoscopic risk factors. Recommendation grade: C (figures 2, 3)
Surveillance colonoscopies should be performed, where possible, when the disease is in remission. However, a surveillance procedure should not be unduly delayed if remission cannot be achieved. Recommendation grade: C
The risk of cancer is influenced by the duration and extent of disease and additional risk factors (such as primary sclerosing cholangitis and a family history of colorectal cancer) and is also linked to the endoscopic and histological appearances at colonoscopy. The screening intervals recommended account for such variables. Surveillance colonoscopies should be conducted yearly, 3-yearly or 5-yearly accordingly. Recommendation grade: C
Pancolonic dye spraying with targeted biopsy of abnormal areas is recommended. Recommendation grade: A. If chromoendoscopy is not used, the strategy of random biopsy outlined in the 2002 guideline should be followed. Recommendation grade: C
If a dysplastic polyp is detected within an area of inflammation and can be removed in its entirety, it is not necessary to recommend colectomy. Recommendation grade: C
Surveillance recommendations for patients with Colitis

{kind=link}
{kind=link}
{kind=link}
Surveillance recommendations post-colectomy.
Prevalence and incidence
See previous guideline for prevalence and incidence.52 Since the previous guideline was published several other epidemiological studies have examined the risk of dysplasia/colorectal cancer. Jess et al reported data from Olmstead County, Minnesota, and found no increased risk for ulcerative colitis patients overall, but the risk did appear to be increased in those with extensive ulcerative colitis (standardised incidence ratio (SIR) 2.4, 95% CI 0.6 to 6.0).55 Similarly, the risk was also increased among patients with Crohn's disease (SIR 1.9, 95% CI 0.7 to 4.1). The most recent data from the St Mark's Hospital surveillance programme has reported the cumulative incidence of colorectal cancer or dysplasia to be 7.7% at 20 years and 15.8% at 30 years.56 This is lower than shown in a previous meta-analysis.57 Of importance is the observation in the St Mark's study that there was a constant cancer incidence with increasing disease duration at least up to 40 years' disease duration. This finding would not support a policy of increased surveillance intensity with increasing disease duration.
Most cancers arise in pancolitis, and there is general agreement that there is little or no increased risk associated with proctitis, whereas left-sided colitis carries an intermediate cancer risk.52 The definitions for extent of disease have been elucidated in the Montreal disease classification.58 Disease extent may change over time in any individual with ulcerative colitis.59 For the purpose of simplifying surveillance in any individual, it may be advisable to continue with a strategy based on the maximum documented extent of disease. There is no evidence to support such a strategy and a clinician may decide to cease surveillance if, for example, proctitis is documented on two consecutive colonoscopies.
The optimal surveillance interval has yet to be defined. For greatest risk reduction, the interval should be no longer than the time it takes for dysplasia to progress to colorectal cancer. However, in IBD this lead time is not known. The more frequent the surveillance, the greater the probability of detecting dysplasia at an earlier stage, but the higher the cost, workload, risk of complications and inconvenience to patients. Each successive interval reduction will have less return in terms of additional dysplasia detection. Thus surveillance frequency is a compromise, taking these factors into account. The surveillance intervals recommended here draw on current data on the natural history of dysplasia and surveillance efficacy.
Intervention
A number of risk factors for colorectal cancer in IBD have been elucidated. These include duration and extent of disease,57 60 primary sclerosing cholangitis,61 family history of sporadic colorectal cancer,62 63 and possibly young age at colitis diagnosis.60 Patients who have a first-degree relative with a history of colorectal cancer have twice the risk of developing colorectal cancer compared with those who do not. Patients with a first-degree relative diagnosed with colorectal cancer before 50 years of age have a ninefold increased risk.63 Evidence has emerged indicating that colorectal cancer is also more likely to develop if there is persistent inflammation in the colon (even at a microscopic level).53 54 64 65 Thus, if active inflammation is found on a surveillance colonoscopy, a stepwise increase in medication should be initiated promptly. Two studies have demonstrated a higher than expected frequency of malignant neoplasms in patients with post-inflammatory polyps: Rutter et al and Velayos et al both showed the risk to be doubled (OR 2.14, 95% CI 1.24 to 3.70 and OR 2.5, 95% CI 1.4 to 4.6, respectively).64 66 Likewise, strictures have a propensity for colorectal cancer (OR 4.22, 95% CI 1.08 to 15.54).64 A series of case reports in patients with Crohn's disease also demonstrated that those with chronic complicated anorectal disease and excluded loops of bowel after bypass surgery are at increased risk of colorectal cancer.67 68 Not all factors confer the same degree of risk, and the strategy outlined below reflects this.
Surveillance strategy
Index (screening) colonoscopy is advised for all patients with ulcerative or Crohn's colitis at approximately 10 years after onset of symptoms, then:
Lower risk—5-yearly colonoscopy
Five-yearly colonoscopy is recommended for patients with extensive colitis (either ulcerative colitis or Crohn's colitis) with no endoscopic/histological active inflammation on the previous colonoscopy (histological chronic or quiescent changes acceptable) or left-sided colitis (any grade of inflammation) or Crohn's colitis affecting <50% of the surface area of the colon (any grade of inflammation).
Intermediate risk—3-yearly colonoscopy
Three-yearly colonoscopy is recommended for patients with extensive colitis (either ulcerative colitis or Crohn's colitis) with mild endoscopic/histological active inflammation on the previous surveillance colonoscopy or presence of post-inflammatory polyps or family history of colorectal cancer in a first-degree relative aged 50 years or over.
Higher risk—yearly colonoscopy
Yearly colonoscopy is recommended for patients with extensive colitis (either ulcerative colitis or Crohn's colitis) with moderate or severe endoscopic/histological active inflammation on the previous surveillance colonoscopy or stricture within past 5 years or confirmed dysplasia within past 5 years in a patient who declines surgery or primary sclerosing cholangitis/post-orthotopic liver transplant for primary sclerosing cholangitis or family history of colorectal cancer in a first-degree relative aged <50 years.
Extensive colitis is defined as ulcerative colitis extending proximal to the splenic flexure (E3 according to the Montreal classification) or Crohn's colitis affecting at least 50% of the surface area of the colon (L3 according to the Montreal classification).58
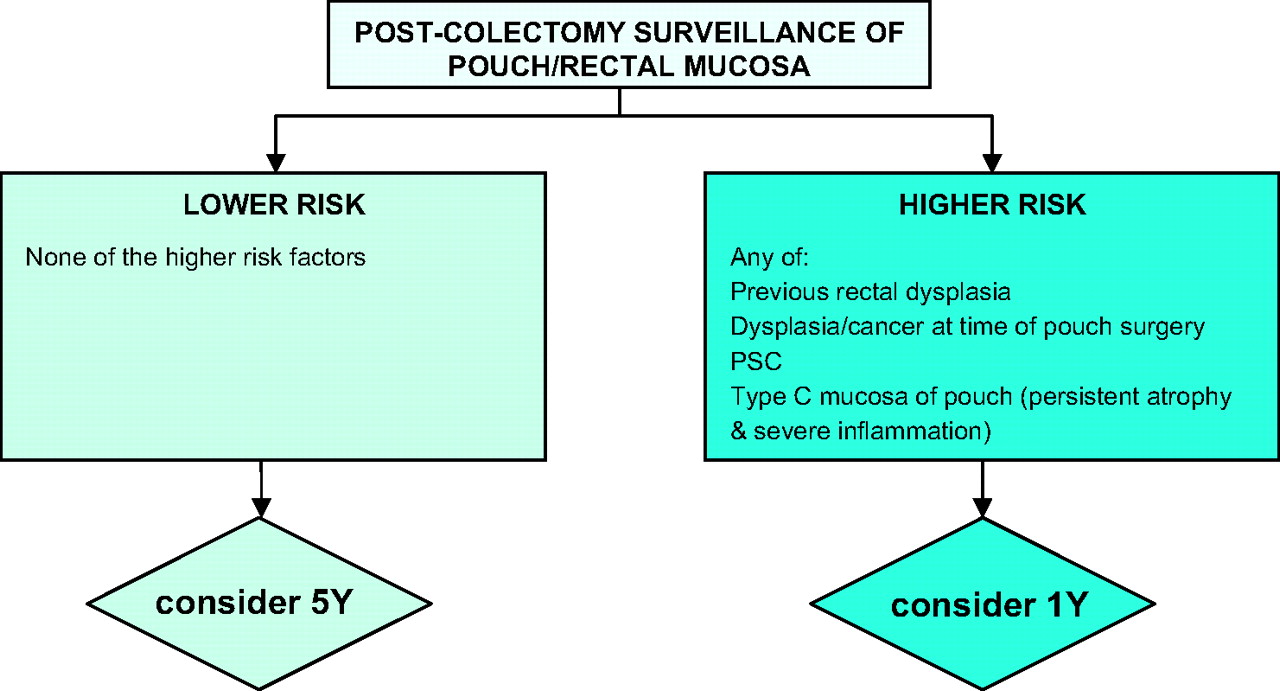
Higher risk post-colectomy patients
Consider yearly flexible sigmoidoscopy of pouch/rectal mucosa in patients with previous rectal dysplasia or dysplasia or colorectal cancer at the time of pouch surgery or primary sclerosing cholangitis or type C mucosa (mucosa exhibiting permanent persistent atrophy and severe inflammation) in the pouch.
Lower risk post-colectomy patients
Consider 5-yearly flexible sigmoidoscopy of pouch/rectal mucosa in patients with none of the risk factors above.
Pancolonic dye spraying
A number of studies show improved detection rates for dysplasia and cancer if targeted biopsies are taken rather than random biopsies.69–71 In addition, clinician adherence to endoscopic protocols for random biopsies is poor and the endoscopic and pathology staffing costs are high. Thus it is recommended that pancolonic dye spraying is adopted as the technique of choice. A prospective randomised cross-over trial has demonstrated that narrow band imaging is no better than standard white light colonoscopy and therefore cannot be recommended as an alternative to chromoendoscopy.105 Although confocal endomicroscopy may enhance the in vivo characterisation of lesions, it is not a technology for lesion detection (as lesions must be detected by other means before confocal endomicroscopy can be employed).106 If chromoendoscopy is not used, the strategy outlined in the 2002 guidelines should be followed (ie, two to four random biopsies from every 10 cm of the colon).52 Details of the dye spraying technique are published elsewhere.72
Patient preparation
Surveillance colonoscopies should ideally be performed when the colitis is in remission, to aid histological discrimination between dysplasia and inflammatory changes. However, surveillance should not be unduly delayed if patients fail to respond to therapy, as those with chronic active inflammation are at increased risk of colorectal neoplasia.53
Assessing severity of inflammation
There are a number of different scoring systems for the endoscopic assessment of severity of inflammation. In the study by Rutter et al, a non-validated five-point scale was used: 0, entirely normal appearance; 1, quiescent disease (mild oedema or chronic features, but no active inflammation); 2, mild active inflammation; 3, moderate active inflammation; 4, severe active inflammation.53 The four-point Mayo score is similar and contains useful descriptors for each category: 0, normal; 1, mild disease (erythema, decreased vascular pattern, mild friability, no contact bleeding); 2, moderate disease (marked erythema, absent vascular pattern, friability, erosions, contact bleeding); 3, severe disease (spontaneous bleeding, ulceration).73
There are a number of different scoring systems for the histological assessment of severity of inflammation. In the study by Rutter et al, a non-validated five-point scale based on epithelial neutrophils was used: 0, normal (no inflammatory cells); 1, chronic inflammation only; 2, mild active inflammation (cryptitis but no crypt abscesses); 3, moderate active inflammation (few crypt abscesses); 4, severe active inflammation (numerous crypt abscesses).53
These scales may act as a guide to the clinician during colonoscopic surveillance.
What to do with macroscopically visible dysplasia
It is essential to biopsy the flat mucosa surrounding any dysplastic polyp to assess the extent of disease (as it may not be apparent macroscopically) and also to assess whether there is any dysplasia in the surrounding flat mucosa. If a dysplastic polyp occurs in an area proximal to the microscopic level of inflammation, with no dysplasia in flat mucosa, it can be regarded as a sporadic adenoma and treated accordingly.74 75
Dysplastic polyps arising within an area of inflammation have been termed dysplasia-associated lesions/masses (DALMs).76 However, the definition of a DALM has evolved over time, and recently a new entity, the ‘adenoma-like mass’ (ALM) has been proposed.77 These terms are often unhelpful as there is no clear-cut endoscopic, histological or immunohistochemical discriminator between adenomas, ALMs and DALMs.79 However, studies have shown that where dysplastic polyps detected within an area of inflammation are judged to be broadly similar in appearance to sporadic adenomas and are endoscopically resected, the prognosis is good. In one study, 70 such dysplastic polyps were resected from 48 patients. Although 48% developed further dysplastic polyps, none developed cancer over a mean 4.1-year follow-up.75 Another follow-up study of 24 patients with endoscopically resected dysplastic polyps within inflamed mucosa showed that after a mean follow-up of 82 months, 59% had developed further dysplastic polyps, with one patient developing low-grade dysplasia and a further patient with primary sclerosing cholangitis developing adenocarcinoma 7.5 years later.79 The study concluded that there was no significant difference in the prevalence of dysplastic polyp formation on follow-up between that cohort and a comparator cohort of patients with non-ulcerative colitis following sporadic adenoma polypectomy. A third study of 40 patients undergoing endoscopic resection of dysplastic polyps within inflamed mucosa reported one case of adenocarcinoma after a mean follow-up period of 4.2 years.78 This was not significantly different from the frequency of cancer within the surveillance population as a whole (p=1.0, Fisher's exact test).
Thus, if a dysplastic polyp is detected within an area of inflammation but can be removed in its entirety, it is usually not necessary to recommend colectomy.74 75 78 79 However, if the dysplastic polyp cannot be completely excised, either urgent re-assessment of resectability by an experienced colonoscopist or urgent surgery is required irrespective of the grade of dysplasia.78 If a dysplastic polyp is arising within a field change of dysplastic tissue in the surrounding flat mucosa, colectomy should be recommended as full excision of the lesion will not be possible endoscopically.
What to do with low-grade dysplasia
The diagnosis of low-grade dysplasia (LGD) in flat mucosa is fraught with controversy owing to the problems outlined in the 2002 guidelines.52 Several papers have provided evidence on the progression of LGD to high-grade dysplasia, a DALM or cancer (table 1). The reported rates of progression to advanced neoplasia vary greatly, which makes it difficult for clinicians when advising their patients. Most studies have found that between a fifth and a half of all patients with LGD will develop a more advanced lesion.56 80–84
Progression of low grade dysplasia to high grade dysplasia or cancer
With the controversies in mind, if a diagnosis of LGD in flat mucosa is made, the histological slides should be reviewed by a second expert gastrointestinal pathologist. If there is agreement, a careful discussion of the potential risk of developing cancer and the options of colectomy or increased surveillance should take place.
A colectomy may be the best option to allay any fears for future development of carcinoma.
If a patient is unwilling to undergo colectomy, yearly surveillance is recommended.
If there is any uncertainty about the diagnosis of LGD following the histological review, a repeat colonoscopy within 3 months using chromoendoscopy should be conducted to confirm or refute the diagnosis.
What to do with a patient who has multiple post-inflammatory polyps
Patients who have post-inflammatory polyps have an increased risk of developing colorectal neoplasia.64 However, the colonoscopic detection of subtle mucosal irregularities in the context of multiple post-inflammatory polyps may be difficult or even impossible. Where the colonoscopist feels the value of colonoscopic surveillance is compromised, further discussion with the patient is important, as prophylactic colectomy might sometimes be more appropriate.
What to do after pouch surgery
Dysplasia following restorative proctocolectomy with ileal pouch anal anastomosis is rare but can develop in either the pouch ileal mucosa or in any retained anorectal mucosa (commonly but erroneously called the ‘anal transition zone’). The few cases of cancer reported in the literature each occurred more than 10 years after the onset of the patient's ulcerative colitis.85 Risk factors include patients with previous rectal dysplasia, dysplasia/colorectal cancer at the time of pouch surgery, and primary sclerosing cholangitis.86 87 Type C mucosa in the pouch (mucosa exhibiting permanent persistent atrophy and severe inflammation) has a greater propensity for the development of colonic type metaplasia.88 89 Consequently, type C mucosa (and refractory pouchitis) is associated with a higher, albeit small, risk of neoplasia.90 There is no clear evidence that pouch surveillance is beneficial and thus it cannot be strongly recommended. However, if a clinician wishes to offer surveillance, a policy of annual pouch surveillance by flexible sigmoidoscopy, taking four proximal and four distal pouch biopsies, would seem reasonable. The occurrence of neoplasia is extremely rare if there was no colorectal cancer at the time of the proctocolectomy and if no other risk factor is present.91 No data exist on whether to survey such patients, but it may be reasonable to perform surveillance by flexible sigmoidoscopy every 5 years.
Costs and benefits
The previous guideline has already estimated there will be approximately 100 patients requiring surveillance in a population of 300 000.52 Of these 100 patients it is estimated that 15 patients would fall into the higher risk category, 30 would be in the intermediate risk group and 55 in the lower risk group. Based on these figures, 36 colonoscopies would be required per annum. The National Tariff cost of a colonoscopy is £476. The cost of surveillance would therefore be (36×£476)=£17 136 per year. This compares favourably with the previous surveillance strategy which would have cost £37 604 (79×£476).
Audit
See previous guideline.52 In addition, the yield of dysplasia and cancer should be audited to determine whether the revised strategy improves detection rates.
Prevention of colorectal cancer
The evidence is mounting for the chemopreventive role of aminosalicylates (5-aminosalicylic acid, 5-ASA).92–94 Although more data are required, it is recommended that patients are kept on 5-ASA at a dose of at least 1.2 g/day.95 One published study, which looked specifically at thiopurines, did not demonstrate a chemopreventive role for azathioprine or 6-mercaptopurine.96 Other studies reached similar conclusions, although this was not their primary endpoint.53 97 98 Thus, it may be beneficial for patients to remain on a 5-ASA preparation even if their disorder is well controlled with a thiopurine.
Data are also emerging on the chemopreventive potential of other agents in IBD such as ursodeoxycholic acid in patients with primary sclerosing cholangitis,99 100 although the data are not conclusive.97 Folate supplementation may also be beneficial,98 101 especially in patients who may have folate deficiency due to sulphasalazine therapy, but again the data are sparse. Other chemotherapeutic agents such as calcium and probiotics have been reviewed elsewhere, but no recommendation can be made.102
Screening guidelines for colorectal cancer and polyps in patients with acromegaly
Acromegaly is characterised by excessive levels of circulating growth hormone and its tissue mediator, insulin-like growth factor 1 (IGF-1). Prior to effective treatment and lowering of growth hormone and IGF-1 levels, the majority of patients with the disease died by the age of 60 years, largely due to diabetes mellitus and cardiovascular and cerebrovascular diseases. It is probable that with more effective and aggressive treatment of both the underlying acromegaly and its metabolic and vascular complications, patients are now surviving long enough to develop malignant complications of the disease. More recently, it has become apparent that patients with acromegaly have an increased prevalence of colorectal adenomas and cancer.107 Analysis of prospective colonoscopic screening studies involving almost 700 patients gives an overall prevalence of 3.7% (relative risk 7.4).107 That this increased risk might be related to serum growth hormone and/or IGF-1 levels is supported by recent epidemiological studies in the non-acromegalic population that have demonstrated an association between serum IGF-1 levels and risk of colorectal cancer.108–110
Executive summary
Patients with acromegaly should be offered regular colonoscopic screening, starting at the age of 40 years. Recommendation grade: B
The frequency of repeat colonoscopy should depend on the findings at the original screening and the activity of the underlying acromegaly. Recommendation grade: B
Patients with an adenoma at first screening or elevated serum IGF-1 level above the maximum of the age-corrected normal range should be offered 3-yearly screening.
Patients with a negative first colonoscopy or a hyperplastic polyp or normal growth hormone/IGF-1 levels should be offered screening every 5–10 years.
Total colonoscopy is required rather than sigmoidoscopy, although the former is associated with technical difficulties. Recommendation grade: B
Prevalence and incidence
Acromegaly is a rare disease with an annual incidence of approximately 4–6 per million. There are approximately 2500 patients with acromegaly in the UK. Owing to the complexity of the disease and its treatment, tertiary referral centres manage the majority of these cases, with the number of patients in each centre varying between 20 and approximately 350. The recognition that these patients have an increased prevalence of colorectal neoplasia originally came from retrospective epidemiological surveys. These suspicions have been repeatedly confirmed during the past 15 years by a number of prospective colonoscopic surveys involving almost 700 patients.107 Analysis of these studies reveals an overall odds ratio of 2.4 for adenoma and 7.4 for colorectal cancer.107 In the two largest series, comprising more than 400 patients with acromegaly, almost identical prevalence rates were recorded of 23–24% of patients having an adenoma and 4.3–4.5% having a cancer.111 112 The increased prevalence of cancer compared with adenoma may reflect an increased propensity for malignant transformation in acromegaly. A recent large retrospective cohort study has shown a 2.5-fold increase in mortality from colon cancer in acromegaly.113
Intervention
The majority of prospective series have recorded a positive association between prevalence of adenomas and increasing age, although a recent large series reported significantly increased prevalence in patients under 40 years of age compared with a control group (19% vs 4.4%).112 In order to determine which people with acromegaly are at particular risk of colorectal neoplasia, and to obtain preliminary data on appropriate screening levels, two groups have performed repeat colonoscopy on their original cohort of patients.112 114 At a mean interval of approximately 32 months after the original screening colonoscopy, new adenomas were observed in 14–15% of the cohort overall, but in 25–41% of those who had an adenoma at the original screening. Additional significant risk factors were elevated growth hormone or serum IGF-1 levels. Thus, more than 90% of patients who developed new adenomas had either neoplasia at the original colonoscopy or elevated serum IGF-1 levels.112 114
In the largest series, 25–40% of adenomas and 50% of carcinomas occurred in the ascending or transverse colon.111 112 Total colonoscopy is therefore recommended.
Practical issues affect the success of total colonoscopy in people with acromegaly. These patients have increased length of colon, particularly the sigmoid section, as well as increased circumference.115 116 In addition, these patients have colonic transit times that are more than twice that of normal individuals and thus standard bowel preparation is usually inadequate.117 In the authors' experience, twice the ‘standard’ preparation of polyethylene glycol electrolyte solution gives good results. Despite this, inadequate bowel clearance still occasionally occurs and individual patients may require considerably more preparation. In view of the technical difficulties of the examinations, an experienced colonoscopist should perform the tests.
Costs and benefits
The small number of cases of acromegaly in the UK means that assessment of the cost–benefit ratio is difficult. There are approximately 2500 patients with acromegaly in the UK, of whom about 2000 are aged 40 years or over. According to the data, about 25% of these (500) will have an adenoma and thus would be offered 3-yearly screening, while the remainder would be offered screening every 5–10 years. Thus the number of extra examinations in each centre due to acromegaly is likely to be small.
Audit
The suggested guidelines will be revised as further data become available. The small number of patients affected means that collaboration between centres will be required to increase the number of patients under study.
Guidelines for monitoring patients with ureterosigmoidostomy
Neoplasms can occur at an anastomosis between ureter and bowel. In practice the only patients now at risk have had ureterosigmoidostomies or one of the variations that allow urine and faeces to be mixed, such as the Mainz II or Mansoura operations. The neoplasms are adenomas or adenocarcinomas. It is thought that adenomas develop first and subsequently undergo malignant degeneration after a mean of 5 years. It is uncertain whether the tumours arise from the intestinal or ureteric epithelium or from the anastomosis itself. Although other neoplasms have been reported in patients with ureterosigmoidostomy, they are rare and probably an unassociated chance finding.
Executive summary
Neoplasia at the anastomosis of the ureters and colon in patients with any urinary diversion that mixes urine and stool (in effect, ureterosigmoidostomy and its variations) occurs in about 24% of patients at 20 years of follow-up. The earliest recorded is 10 years after formation.
All patients should have a flexible sigmoidoscopy once per year.
In patients who have had a ureterosigmoidostomy which has subsequently been converted to an alternative diversion, flexible sigmoidoscopies should still be carried out unless it is known that the ureteric anastomoses were removed. Recommendation grade: C
Intervention
Timing
It seems that the neoplastic process is initiated in a short time and is not reversed if the urinary diversion is changed but the original ureterocolic anastomosis is left intact. In one patient the ureterosigmoidostomy was in place for only 9 months before a change was made to an ileal conduit; the anastomosis was left in place and was found to have developed an adenocarcinoma 14 years later. The shortest time from formation of the ureterosigmoidostomy to the development of a neoplasm is 10 years.118
Risk
Estimates of the risk of neoplasia vary between 100 and 7000 times that expected in the normal population. In a definitive review of the literature in 1982, Stewart accepted the lower figure.119 Neoplasia can occur in intestinal reservoirs in the absence of stool. Eleven cases have been reported in colon, five of which were anastomotic.120
Recommendation
Patients who have a ureterosigmoidostomy or any of the modern variations such as the Mainz II or Mansoura operations, should have a flexible sigmoidoscopy to visualise the colon up to and just beyond the higher ureteric anastomosis. The examinations should begin on the tenth anniversary of the original operation and should be repeated annually. Recommendation grade: C
The anastomosis normally looks like a small cherry, 4–5 mm in diameter. If a polypoid lesion is thought to be at the ureteric anastomosis, clinical experience suggests it should not be removed with an endoscopic snare as the anastomosis might be damaged leading to urinary leakage, although they can be biopsied. Lesions that are found clearly remote from the ureteric anastomosis can probably be removed endoscopically although there are no data in the literature that confirm this impression.
Small lesions found to be adenomas or adenocarcinomas of the anastomosis have been removed by open resection of the lower ureter and a cuff of colon around it. Patients may, after proper advice, opt for a different diversion or for another ureterosigmoidostomy. Large and invasive lesions have been removed by colonic and lower ureteric resection.121 Again, however, there is no comparative series to confirm the validity of these procedures.
Patients who have had a ureterosigmoidostomy but with subsequent conversion to a different diversion should also have an annual examination with flexible sigmoidoscopy unless the ureteric anastomosis is known to have been removed.
Audit
Patients with ureterosigmoidostomy should be identified by their urologist. A central urology unit record should be kept. Thus non-attendance and colonoscopic findings can be monitored.
Guidance on gastrointestinal surveillance for high risk genetic disorders: hereditary non-polyposis colorectal cancer, familial adenomatous polyposis, MUTYH-associated polyposis, juvenile polyposis and Peutz–Jeghers syndrome
Executive summary
People with a greatly elevated personal risk of gastrointestinal malignancy can be identified on the basis of one or more of the following criteria: a family history consistent with an autosomal dominant cancer syndrome; pathognomonic features of a characterised polyposis syndrome personally or in a close relative; the presence of a germline pathogenic mutation in a colorectal cancer susceptibility gene; molecular features of a familial syndrome in a colorectal cancer arising in a first-degree relative. This guidance specifically excludes individuals not fulfilling these inclusion criteria. Lifetime cancer risk ranges from 10% to ∼100%. Recommendation grade: B
People fulfilling the above criteria should be referred to a regional genetics centre for assessment, genetic counselling and mutation analysis of relevant genes where appropriate. Recommendation grade: B
There is substantial rationale for cancer surveillance in Lynch syndrome, familial adenomatous polyposis (FAP), MUTYH-associated polyposis (MAP), juvenile polyposis (JPS) and Peutz–Jeghers syndrome (PJS) because of the associated high risk of gastrointestinal malignancy. Recommendation grade: B
Families fulfilling Amsterdam criteria, but without evidence of DNA mismatch repair gene defects (following negative analysis of constitutional DNA and negative tumour analysis by microsatellite instability testing/immunohistochemistry), require less frequent colonoscopic surveillance. Recommendation grade: B
Gastrointestinal surveillance should cease for people tested negative by an accredited genetics laboratory for a characterised pathogenic germ-line mutation shown to be present in the family, unless there was a significant, coincidental finding on prior colonoscopy. Recommendation grade: B
Prophylactic surgery has a central place in the management of these disorders. The evidence is best developed in FAP, but the optimal surgical procedure remains under debate.
The evidence for upper gastrointestinal surveillance in all of these disorders is weak, but limited evidence suggests it may be beneficial. Recommendation grade: C
Surveillance for extra-intestinal malignancy is not discussed, but clinicians should be aware of these risks and make appropriate referral.
Introduction
People with an increased risk of colorectal cancer due to high-penetrance genetic disorders are identified in one or more of the following ways:
Recognition of a family history of colorectal cancer that fulfils empiric family history criteria.
Presence of pathognomonic clinical/pathology features in the consultand or in a close relative, including extra-intestinal manifestations such as cranio-facial osteomata and desmoid disease in FAP, pigmented peri-orbital and peri-oral lesions associated with various cancers in Peutz–Jeghers syndrome and early-onset endometrial or upper urinary tract urothelial neoplasia in Lynch syndrome.
Identification of a germ-line molecular genetic defect in the consultand or relative.
Collectively, such cases account for a small proportion (3–5%) of all cases of colorectal cancer. However, the absolute cancer risk is high and so the intensity of surveillance reflects that elevated level of risk and the natural history of the resultant neoplasia.
Although there are other, even more rare, syndromes associated with excess colorectal cancer risk, this guidance is restricted to discussion of hereditary non-polyposis colorectal cancer (HNPCC; also known as Lynch syndrome), familial adenomatous polyposis (FAP), MUTYH-associated polyposis (MAP), juvenile polyposis (JPS) and Peutz–Jeghers syndrome (PJS). The syndromes are defined and summarised in Online Mendelian Inheritance in Man (OMIM; see box 1). All, except MAP, are due to dominant germline transmission of a gene defect associated with susceptibility to colorectal cancer and other cancer types. MAP is an autosomal recessive disorder, and so the implications for surveillance in relatives are different from the dominant syndromes. Genes responsible for these syndromes have been identified and large numbers of mutations characterised. Penetrance is incomplete and so not all people who carry a pathogenic mutation develop cancer themselves. Therefore, a striking family history is not a prerequisite. Furthermore, mutations in causative genes have not been identified for all families. Hence, identification of at-risk individuals may be through family history criteria and/or pathological criteria and/or presence of a pathogenic mutation in one of the genes listed in the appendix. It is also important to note that these syndromes may become apparent through identification of mutations or associated clinical features in an index case with an associated cancer type (eg, endometrial cancer in Lynch syndrome, breast or pancreatic cancer in Peutz–Jeghers syndrome, upper gastrointestinal cancer in FAP). Such individuals and their relatives should then be managed by the surveillance described here for gastrointestinal malignancy.
Box 1 Genes responsible for defined genetic syndromes predisposing to colorectal cancer
Lynch syndrome/hereditary non-polyposis colorectal cancer (HNPCC)
Genes responsible: MLH1, MSH2, MSH6, PMS2.
OMIM 114500, 120435, 120436, 276300, 609309, 600678, 600259.
Familial adenomatous polyposis (FAP)
Gene responsible: APC.
OMIM 175100.
Peutz-Jeghers syndrome
Gene responsible: LKB1.
OMIM 175200.
Juvenile polyposis
Gene responsible: SMAD4, BMPR1A (Juvenile polyposis).
OMIM 174900.
Rare subtype hereditary mixed juvenile/adenomatous polyposis
Gene responsible: locus on chr15q (GREM1 or SGNE1 may be responsible).
OMIM 601228.
MUTYH associated polyposis (MAP)
Gene responsible: MUTYH.
OMIM 608456.
Search OMIM ID numbers at www.ncbi.nlm.nih.gov/omim
Definition and aetiology
Hereditary non-polyposis colorectal cancer (Lynch syndrome) (MIM 114500, 120435, 120435)
Lynch syndrome is an autosomal dominant genetic disorder characterised by a markedly elevated cancer risk and is due almost exclusively to mutations in one of the DNA mismatch repair (MMR) genes. There are reports of the condition segregating with other genes in a minority of families. Prior to the discovery of the role of MMR genes, Lynch syndrome was defined empirically by family history criteria: the Amsterdam and subsequently the modified Amsterdam criteria.122 These criteria comprise: three or more family members affected by colorectal cancer or with a Lynch syndrome cancer (endometrium, small bowel, ureter or renal pelvis) in >2 generations; at least one affected relative must be no more than 50 years old at diagnosis and one of the affected relatives must be a first-degree relative of the other two, while FAP should be excluded.123 124 Subsequent to the identification of the causative genes,125 126 these criteria have been shown to be specific, but not sensitive, predictors of MMR gene carriers. Gene carriers have been identified who do not fulfil Amsterdam criteria.127 128 Nonetheless, the criteria remain a useful clinical tool to pinpoint families most likely to carry mutations in DNA MMR genes.129 While the strength of family history correlates with the likelihood of detecting an MMR gene mutation,127–130 a diagnosis of colorectal cancer at a young age (<50 years) should alert the clinician to the possibility of Lynch syndrome, even without an obvious family history. It should be noted that a germ-line mutation cannot be detected using current methodologies in around 20% of Lynch families, even though they meet Amsterdam criteria and exhibit tumour microsatellite instability (MSI) or loss of DNA MMR gene expression on tumour immunohistochemistry. MSI is the hallmark of DNA MMR gene deficiency and is frequently associated with loss of expression of one of the DNA MMR genes. Those patient groups who develop colorectal cancer at a young age are enriched for DNA MMR gene mutations and should be offered tumour MSI and immunohistochemistry testing. However, it should be noted that MLH1 is frequently lost by epigenetic silencing through promoter hypermethylation and so isolated cases of MSI tumours showing MLH1 loss are very unlikely to be due to heritable mutations.
Lifetime gastrointestinal cancer risk associated with Lynch syndrome is variously reported as around 80% for colorectal cancer and 13–20% for gastric cancer in studies that have selected families by Lynch syndrome criteria.131 132 However, as molecular diagnosis identifies families with lower penetrance, the overall cancer risk estimates have reduced.128 133–136 Available evidence indicates that the colorectal cancer risk for males is higher than that for females.127 133–136
Familial adenomatous polyposis (MIM 175100)
Familial adenomatous polyposis (FAP) is an autosomal dominant syndrome with very high penetrance, characterised by the presence of more than 100 adenomatous polyps of the colon and rectum.137–139 The condition is due to germ-line mutations of the APC gene on chromosome 5q. Although until recently mutations could not be detected in 10–20% of FAP patients,140 141 current techniques comprising sequence analysis of the whole gene and assays for larger structural defects detect mutations in ∼95% of FAP cases. There is evidence of phenotypic heterogeneity in FAP, with some mutations being associated with a severe phenotype and others being associated with a milder, attenuated phenotype with relatively fewer polyps and a later age of onset.142 The attenuated FAP phenotype (AFAP) is associated with fewer than 100 adenomatous polyps, later onset polyposis and colorectal cancer and inactivating mutations in specific regions of the APC gene (5' region, exon 9 and the very 3' region). The phenotype overlaps with that due to MUTYH mutations and merits testing both genes in suspected cases. In classical FAP, the risk of developing colorectal cancer exceeds 90% by age 70 years without prophylactic surgery.137–139 The risk of gastroduodenal cancer is about 7%.137 138 143 Around 25% of all cases are due to new mutations in the APC gene and so there is no previous family history. Nonetheless, children of individuals with a new mutation are at 50% risk of inheriting the condition.
MUTYH-associated polyposis (MIM 604933, 608456)
Around 25–30% of polyposis cases with more than 20 polyps and without evidence of a dominant inheritance pattern, in whom genetic analysis has not identified an APC mutation, are due to bi-allelic mutations in the base excision repair (BER) gene, MUTYH (previously MYH).144 145 Polyps can be exclusively adenomatous or mixed adenomatous/hyperplastic. Since the mode of inheritance is autosomal recessive, lack of vertical transmission of the polyposis phenotype in the family should raise the possibility of MUTYH-associated polyposis (MAP). Siblings are at 25% risk of carrying bi-allelic deleterious mutations. Children of a bi-allelic carrier are at high risk if the other parent also carries at least one mutant allele. Large, systematic studies of MUTYH mutation frequency in colorectal cancer cases and controls suggest penetrance in bi-allelic carriers is very high, and probably >90%.146–148
Peutz–Jeghers syndrome (MIM 175200)
Peutz–Jeghers syndrome (PJS) is an autosomal dominant syndrome with high penetrance, defined by the presence of hamartomatous polyps of the small intestine, colon and rectum, in association with mucocutaneous pigmentation.149 150 Gastrointestinal cancer risks include gastro-oesophageal, small bowel, pancreatic and colorectal cancers with a cumulative risk of 57% by the age of 70.151–154 There is a ∼50% lifetime risk of breast cancer, and clinicians managing PJS patients should ensure breast screening arrangements are in place. In 20–63% of cases, inactivating mutations can be identified in the gene STK11 (LKB1).155 156 There is evidence for genetic heterogeneity with a possible further locus on chromosome 19q.157
Juvenile polyposis (MIM 174900, 601228)
Juvenile polyposis (JPS) is defined by the presence of multiple hamartomatous polyps of the colon and rectum. Histological differences and topographical distribution within the gastrointestinal tract serve to distinguish between this disorder and Peutz–Jeghers syndrome. The term ‘juvenile’ refers to the polyp type rather than to the age of onset, although most individuals with juvenile polyposis have some polyps by 20 years of age. Juvenile hamartomatous polyps have an apparently normal epithelium with a dense stroma, an inflammatory infiltrate, and a smooth surface with dilated, mucus-filled cystic glands in the lamina propria with smooth muscle fibres, which distinguishes these from PJS polyps. The glandular proliferative characteristics of adenomas are typically absent.
Juvenile polyposis usually manifests during childhood, but diagnosis of the condition is confounded by the occurrence of isolated juvenile-type polyps in children. These solitary polyps are noteworthy because their identification in childhood does not necessarily indicate a heritable cancer predisposition syndrome, and they do not appear to be associated with excess cancer risk.158 In contrast, juvenile polyposis is associated with a colorectal cancer risk of around 10–38%159 160 and a gastric cancer risk of 21%.159 161 Around 20% of cases are due to mutations in the SMAD4 gene,162–164 while a further 20% are due to mutations in another gene in the same molecular signalling pathway, BMPR1A,165 indicative of genetic heterogeneity.166 Mutations in BMPR1A have been particularly implicated in European populations and SMAD4 mutations may have a more aggressive clinical phenotype.
Frequency
Lynch syndrome
Between 0.3% and 2.4% of all patients with colorectal cancer fulfil family history criteria to indicate Lynch syndrome.167–170 The proportion of colorectal cancer cases due to mutations in DNA MMR genes is 2–3%,127 129 171 172 and the estimated population carrier frequency is about 1:3100.173
Familial adenomatous polyposis
The population prevalence of FAP is estimated at 1:14 000.174 Owing to highly effective surgical prophylaxis, FAP accounts for only 0.07% of incident colorectal cancers in modern practice.174 As registries and genetic services improve detection of at-risk family members, the proportion of colorectal cancer cases due to FAP should reduce, limited only by the proportion due to new mutations, which account for 25% of cases.
MUTYH-associated polyposis
MAP is the most recent of the polyposis syndromes to be characterised at the molecular level.175 176 Penetrance estimates for homozygous carriers are not robust because relatively small numbers of bi-allelic carriers have been identified so far and all were selected on polyposis or cancer phenotype. However, available evidence from colorectal cancer case–control studies148 and from polyposis studies176 suggests that the cancer risk is high (>90%). Estimates are robust for homozygote and heterozygote carrier frequencies in the general population and in cancer cases because large numbers of controls and colorectal cancer cases have been genotyped.148 The heterozygote carrier frequency in the UK is ∼2% and around 1:10 000 homozygous or compound heterozygotes for two MUTYH mutations.148 The proportion of polyposis syndromes due to MUTYH in clinical practice is less clear because studies have so far focused on selected research case series of multiple polyps that have been screened negative for APC mutations. In one study 4% of multiple polyp cases (3–100) and 8% of APC mutation negative polyposis cases carry MUTYH mutations.176
Peutz–Jeghers syndrome and juvenile polyposis
Robust prevalence estimates for these conditions are not available because of their rarity, the lack of comprehensive clinical phenotype ascertainment and the fact that there are no population-based molecular studies. However, estimates of the population prevalence of Peutz–Jeghers syndrome suggest a frequency of around 1:50 000,149 177 similar to that of juvenile polyposis, although the latter may be as low as 1:120 000. Both conditions probably explain less than 0.01% of colorectal cancer cases.
Intervention
Hereditary non-polyposis colorectal cancer
There are many published expert reviews of recommended management (178) and many national and international focus groups and commissioned task forces which have come together to suggest management guidelines.128 179 The guidance laid out here is largely in line with such recommendations but is particularly pertinent to the UK NHS situation.
Establishment of Lynch syndrome registries
Families with Lynch syndrome should be referred to the regional clinical genetics service or other specialist service to facilitate risk assessment, genetic testing and screening of family members.128 178 179 Recommendation grade: C
Large bowel surveillance for Lynch syndrome family members and gene carriers
Total colonic surveillance (at least biennial) should commence at age 25 years. Surveillance colonoscopy every 18 months may be appropriate because of the occurrence of interval cancers in some series.128 180–183 Surveillance should continue to age 70–75 years or until co-morbidity makes it clinically inappropriate. If a causative mutation is identified in a relative and the consultand is a non-carrier, surveillance should cease and measures to counter general population risk should be applied. Recommendation grade: B
The effectiveness of colonoscopic surveillance for people with MMR gene mutations and Lynch family members has been examined in retrospective case–control comparisons.181–187 Screened individuals were compared to control subjects who declined, or did not receive, regular colonoscopy with respect to outcomes of cancer incidence,185 187 tumour stage and mortality,181–185 or mortality alone.187 Surveillance appears to provide an average of 7 years of extra life for Lynch syndrome family members.188 Thus, available evidence supports regular colonoscopic surveillance as a means of early colorectal cancer detection, leading to mortality reduction as well as reduction in cancer incidence.
Surveillance should consist of total colonoscopy, since the risk of polyps and cancer is high and a substantial proportion of patients have neoplasia restricted to the proximal colon.181 183–190 Colonoscopy is preferable to flexible sigmoidoscopy combined with barium enema. Because the cancer risk is high, it is not appropriate to accept an incomplete colonoscopy until the next surveillance interval. Incomplete colonoscopy should be followed soon after, or even the same day, by completion CT colonography in centres skilled in providing this technique to a high quality, but repeated radiation exposure should be avoided wherever possible. Repeat full colonoscopy or barium enema remain as options. Chromoendoscopy and narrow wavelength visible light (narrow band) endoscopy may have a place in the detection of small or flat lesions, but there is very limited experience and evidence is restricted to descriptive studies of their use in Lynch syndrome surveillance. Hence, the utility of such techniques requires further assessment and is neither recommended nor discouraged in high risk surveillance, but should not replace conventional endoscopic approaches. Evidence for commencing surveillance at 25 years of age is based on observational data that indicate that the risk increases substantially from age 25 in groups defined by family history131 189 and in groups defined by presence of a mutation.133 134 191–194 Colorectal resection has a place as prophylaxis and for established cancer in Lynch syndrome family members and/or MMR gene carriers.
Patients who have developed a colorectal malignancy and who come from a Lynch syndrome family, or carry a mutation in an MMR gene, should be counselled and offered a surgical procedure that includes both a cancer control element and prophylaxis to counter future cancer risk. At present there is no evidence to guide decision-making on primary prophylactic surgery for patients who do not yet have cancer. Recommendation grade: C
People with MMR gene mutations or those from Amsterdam-positive Lynch syndrome families who have cancer will require surgery unless treatment is palliative. Case series evidence shows that the risk of metachronous colorectal cancer is high following segmental resection (16%), but substantially lower after colectomy and ileorectal anastomosis (3%).131 Hence, incorporating a prophylactic element to the cancer resection is appropriate. For patients with proximal tumours, colectomy and ileorectal anastomosis is most relevant, but the retained rectum must be screened because cancer risk in the retained rectum is 3% every 3 years for the first 12 years.195 196
Upper gastrointestinal surveillance for Lynch syndrome family members and/or MMR gene carriers
In families manifesting gastric cancer as part of the phenotype, biennial upper gastrointestinal endoscopy should be considered. The evidence is limited and a pragmatic recommendation is to screen from age 50 since the incidence is very low until that age. Surveillance should continue to age 75 or until the causative mutation in that family has been excluded. This recommendation is based on observations that some Lynch syndrome families have a particular propensity for gastric cancer.131 132 There is as yet no evidence that this reduces mortality. Recommendation grade: C
Familial adenomatous polyposis
As with Lynch syndrome, recommendations for intervention in FAP have been proposed by many groups and guidance published.139
Establishment of FAP registries
Families with FAP should be referred to the regional clinical genetics service or other specialist service that can facilitate risk assessment, genetic testing and screening of family members. Some regional services have specific FAP registers that facilitate regular follow-up. FAP registries have been shown to improve outcomes by systematic and structured delivery of management, monitoring interventions and surveillance, as well as serving as a focus for audit.174 197 Recommendation grade: B
Large bowel surveillance for FAP family members
Annual flexible sigmoidoscopy and alternating colonoscopy should be offered to mutation carriers from diagnosis until polyp load indicates a need for surgery.198 In a small minority of families where no mutation can be identified and genetic linkage analysis is not possible, family members at 50% risk should have annual surveillance from age 13–15 until age 30 years, and every 3–5 years thereafter until age 60. Surveillance might also be offered as a temporary measure for people with documented APC gene mutations and a significant polyp load but who wish to defer prophylactic surgery for personal reasons. Such individuals should be offered 6-monthly flexible sigmoidoscopy and annual colonoscopy. As in Lynch syndrome, chromoendoscopy or narrow band endoscopy may have a place in surveillance for attenuated FAP, but the utility of these techniques merits further appraisal and must not replace conventional endoscopic approaches. Surgery can be deferred if careful follow-up is instigated and the patient is fully aware of the risks of cancer. This is especially the case for attenuated FAP but can also be useful in the management of classical FAP for individuals who have a low polyp burden in terms of size, multiplicity and degree of dysplasia. The cancer risk increases substantially after 25 years, and so surgery should be undertaken before then unless polyps are sparse and there is no high-grade dysplasia. If colectomy and ileorectal anastomosis are performed, the rectum must be kept under review annually for life because the risk of cancer in the retained rectum is 12–29%.138 199 200 The anorectal cuff after restorative proctocolectomy should also be kept under annual review for life. Recommendation grade: B
Prophylactic colorectal surgery
Patients with typical FAP should be advised to undergo prophylactic surgery between the ages of 16 and 25 years, but the exact timing of surgery should be guided by polyp numbers, size and dysplasia and fully informed patient choice influenced by educational and child-bearing issues. Surgical options include proctocolectomy and ileoanal pouch or a colectomy with ileorectal anastomosis. Recommendation grade: B
People with proven FAP require prophylactic surgery to remove the majority of at-risk large bowel epithelium. Colectomy and ileorectal anastomosis is associated with a 12–29% risk of cancer in the retained rectum,199–202 whereas restorative proctocolectomy is associated with a very low risk of cancer in the pouch or in the retained mucosa at anorectum. Ileoanal pouch construction may be associated with impaired fertility.202 203 It is clear that case identification and prophylactic surgery have markedly improved survival in FAP.139 197
Upper gastrointestinal surveillance in FAP
Because of the substantial risk of upper gastrointestinal malignancy in FAP, surveillance of this tract is recommended. While gastroduodenal polyposis is well recognised in FAP and surveillance practice is established practice in the overall management, there is limited evidence on which to gauge the potential benefit of surveillance. However, the approach seems reasonable, and 3-yearly upper gastrointestinal endoscopy is recommended from age 30 years with the aim of detecting early curable cancers. Patients with large numbers of duodenal polyps should undergo annual surveillance. Recommendation grade: C
Gastroduodenal and periampullary malignancies account for a small, but appreciable, number of deaths in patients with FAP.135 136 139 Duodenal polyposis occurs in approximately 90% of FAP patients and the overall lifetime risk of periampullary cancer is 3–5%.143 204 205 Advancing age and mutation location within the APC gene appear to have an effect on duodenal carcinoma risk.206 Almost all FAP patients have some abnormality on inspection and biopsy of the duodenum by age 40.204 The degree of duodenal polyposis can be assessed using an endoscopic/histological scoring system (Spigelman classification143), which can be helpful in predicting the risk of duodenal cancer. The worst stage (IV) has a 10-year risk of 36% and stage 0 negligible risk.207 Hence, it seems reasonable to offer 3-yearly upper gastrointestinal surveillance from age 30 years and more frequently if there is extensive polyposis. However, it should be noted that the effectiveness of this intervention in reducing mortality is unknown, especially since duodenal polypectomy is unsatisfactory208 and prophylactic duodenectomy is a major undertaking with substantial attendant morbidity and mortality.
MUTYH-associated polyposis
Colorectal surveillance
Large bowel surveillance colonoscopy every 2–3 years is recommended from age 25 years for patients who are bi-allelic MUTYH carriers (or homozygous carriers of other BER gene defects). Colonoscopy is the preferred modality because of the likelihood of polyps requiring polypectomy. Recommendation grade: C
Experience is limited because the role of MUTYH and other BER genes has only relatively recently been demonstrated. Hence, available evidence comes from pooled descriptive experience and opinion.144–148 However, there is a substantial colorectal cancer risk for those who are bi-allelic carriers.148 Although indirect evidence suggests colonoscopic surveillance and polypectomy may be effective in colorectal cancer control, this has yet to be definitively determined. Indeed, we are not aware in the literature to date of any control subjects with bi-allelic MUTYH mutations who have reached the age of 55 years without developing colorectal cancer or polyposis . Hence, the risk may be sufficiently high to merit at least considering prophylactic colectomy and ileorectal anastomosis or even proctocolectomy and ileo-anal pouch if dense rectal polyposis is a feature. The patient should be counselled about the limited evidence available to guide decisions on either surveillance or pre-emptive surgical strategies.
Upper gastrointestinal surveillance
Gastro-duodenal polyposis is reported in over 20% of cases of MUTYH bi-allelic carriers209 and so upper gastrointestinal surveillance is recommended. There is only indirect evidence that this might be beneficial, even less so than for FAP. However, the approach seems reasonable, and 3–5-yearly upper gastrointestinal endoscopy is recommended from age 30 years. Recommendation grade: C
Peutz–Jeghers syndrome
Colorectal surveillance
Large bowel surveillance is recommended 2-yearly from age 25 years. The intervention should visualise the whole colon and so colonoscopy is the preferred mode of surveillance. Recommendation grade: C
PJS is rare and so evidence on effectiveness of surveillance is limited to case series and anecdote, underlined by the fact that available evidence comes from pooled descriptive experiences. Nonetheless, it is clear that there is a substantial increase in overall cancer risk and colorectal cancer risk in particular for affected individuals.154 The risk of colorectal cancer increases with age being 3%, 5%, 15%, and 39% at ages 40, 50, 60, and 70 years, respectively. Males may be at greater risk. There is also an excess risk of small bowel, pancreatic and oesophago-gastric cancer. The risk for all gastrointestinal cancers combined is 1%, 9%, 15%, 33%, and 57% up to ages 30, 40, 50, 60 and 70 years, respectively.154
Upper gastrointestinal surveillance
Upper gastrointestinal surveillance is recommended 2-yearly from age 25 years, comprising gastro-duodenoscopy. Intermittent MRI enteroclysis or small bowel contrast radiography is recommended. Recommendation grade: C
There is an elevated risk of gastric malignancy in Peutz–Jeghers syndrome amounting to around 5–10%.149–154 Although evidence from pooled case series indicates that small intestinal cancer is rare, the risk is sufficient to merit intermittent imaging.154 MRI enteroclysis appears appropriate for surveillance because it avoids repeated radiation exposure in young individuals and has very good sensitivity and overall accuracy for small bowel polyps in PJS210 as well as for patients with small bowel tumours who do not have PJS.211 However, video capsule endoscopy is also an option, with evidence of better sensitivity than MRI enteroclysis for smaller lesions in small bowel polyposis syndromes in one small comparative study.212 It should be stressed that experience with both techniques is limited and robust a evidence base is lacking.
Juvenile polyposis
Colorectal surveillance
Large bowel surveillance for at-risk individuals and mutation carriers every 1–2 years is recommended from age 15–18 years, or even earlier if the patient has presented with symptoms. Screening intervals could be extended at age 35 years in at-risk individuals. However, documented gene carriers or affected cases should be kept under surveillance until age 70 years and prophylactic surgery discussed. The intervention should visualise the whole colon and so colonoscopy is the preferred modality. Recommendation grade: C
Although isolated juvenile polyps are relatively common, juvenile polyposis is rare and consequently experience is limited. There are few large descriptive studies, and no comparative study to demonstrate potential benefit. Nonetheless, there is a substantial risk of colorectal cancer amounting to 10–38%.152 153 Many polyps are located in the right colon,161 and so the whole colon should be visualised. There is particular risk of malignancy in cases where there is adenomatous change, or where there is a dysplastic element to the polyps.
Upper gastrointestinal surveillance
Upper gastrointestinal surveillance every 1–2 years is recommended from age 25 years, contemporaneously with lower gastrointestinal surveillance. Recommendation grade: C
The risk of gastric and duodenal cancer in juvenile polyposis is around 15–21%.159 160
Projected workload
Hereditary non-polyposis colorectal cancer
Annual caseload can be estimated for MMR gene carriers or people at 50% risk within families fulfilling Lynch syndrome criteria for a population of 300 000 (150 000 within the screening age group) served by a district general hospital. The Lynch syndrome alleles are autosomal dominant and population frequency is around 1:3000. However, many Lynch syndrome family members on screening programmes have not undergone mutation testing or no mutation has been detected. Hence, when family history criteria are employed, twice the number of people are offered screening than if only mutation carriers are screened (ie, about 1:1500 of the population). Thus implementing a biennial colonoscopy strategy would require 50 colonoscopies in people within the surveillance age group each year for a population of 300 000. The associated surveillance costs are £23 800, and cost per life saved is £47 500. However, because of the high cancer risk, the cost of not offering surveillance intervention exceeds that of offering the surveillance.188
Familial adenomatous polyposis
Within a population of 300 000 served by a district general hospital, there will be an estimated 22 cases of FAP; most of these patients will already have undergone prophylactic surgery. Hence, there may be two to three patients annually requiring colorectal surveillance, representing a small cost and requirement for resource provision. However, upper gastrointestinal surveillance recommendations may affect workloads, as this is not routinely undertaken by all centres in the management of FAP. However, the numbers remain small, with only an extra five or six upper gastrointestinal endoscopies required per year. The workload of flexible endoscopy of retained rectum will depend on the proportion of patients undergoing surgery, but is not estimated to be more than five or six per year.
Peutz–Jeghers syndrome and juvenile polyposis
These disorders are considered together in view of their similar population frequency, similar uncertainty about the value of surveillance, and similar degrees of cancer risk. Taking both conditions together, there are likely to be 12 affected and at-risk individuals in a population of 300 000 served by a district general hospital. Hence, a maximum of six extra colonoscopies and six upper gastrointestinal endoscopies would be required. One or two patients would require MRI enteroclysis or small bowel imaging annually.
Recommendations for audit
Audit is an essential component of the management of the conditions discussed in this guidance. Setting up registries to manage surveillance in individuals from families with cancer syndromes will enable rolling audit of caseload, compliance, service delivery and outcomes. Such audit can inform future management, since randomised trials of surveillance are unlikely. In particular, audit of practice and experience of MUTYH-associated polyposis is important, because there is a lack of experience in clinical management of this disorder. For Peutz–Jeghers syndrome and juvenile polyposis, linking of national registries will provide more refined population prevalence estimates.
Guidance on large bowel surveillance for individuals with a family history indicating a moderate risk
Executive summary
Predicted future absolute risk of colorectal cancer can be estimated using empiric family history information. Recommendation grade: A
Referrals on the basis of family history are best coordinated through centres with a specialist interest, such as regional genetics services or medical/surgical gastroenterology centres. Such centralisation enables audit of family history ascertainment, assigned level of risk, collection of outcome data and research. Recommendation grade: C
Total colonoscopy is the preferred mode of surveillance for the moderate risk categories defined here, owing to the propensity for proximal colonic lesions and the opportunity for snare polypectomy. Incomplete colonoscopy should initiate an alternative imaging modality on the same day, such as double-contrast barium enema or CT colonography. A repeat colonoscopy soon after an incomplete examination is acceptable, but success must be assured. However, radiation exposure should be minimised and regular radiological surveillance is not recommended. Recommendation grade: B
High–moderate risk group inclusion criteria comprise familial aggregations where affected relatives are first-degree relatives of each other (first-degree kinship) with at least one being a first-degree relative of the consultand. If both parents are affected, these count as being within first-degree kinship:
Three affected relatives any age in a first-degree kinship (eg, a parent and a blood-related aunt/uncle and/or grandparent), at least one of whom is a first-degree relative of the consultand, or two siblings/one parent or two siblings/one offspring combinations, or both parents and one sibling. However, there should be no affected relative <50 years old, as otherwise the family would fulfil high risk criteria.
Two affected relatives aged <60 years in a first-degree kinship or mean age of two affected relatives <60 years. At least one relative must be a first-degree relative of the consultand and so this category includes a parent and grandparent, >2 siblings, >2 children or child+sibling. The risk is sufficiently increased to merit low-intensity surveillance comprising 5-yearly colonoscopy between age 50 and age 75 years. Polyps should be snared; adenoma surveillance applies thereafter if a benign neoplasm is confirmed. Recommendation grade: B
Low-moderate risk group. Inclusion criteria are:
One affected first-degree relative under 50 years old or
Two affected first-degree relatives, aged 60 or older.
In both high-moderate and low-moderate categories, pathology tumour material from an affected relative may be available to test for Lynch syndrome gene involvement. Excluding such instances, there is a modest excess risk meriting a single colonoscopy at age 55 (if older at presentation then instigate forthwith), in the low–moderate group to identify polyp formers. Polyps should be snared; adenoma surveillance applies thereafter if a benign neoplasm is confirmed. If colonoscopy is clear, reassure and discharge with recommendations relevant to population risk (uptake of faecal occult blood test screening in the UK). Recommendation grade: B
Early-onset colorectal cancer (<50 years). The elevation of risk in relatives of an early-onset case is modest. However, the heightened anxiety and emotive nature of cancer in this age group merit special mention because this frequently initiates requests for surveillance. Such cases are covered by the above risk categorisation, but algorithms can also be used to predict whether the affected relative is a carrier of a mutation in a Lynch syndrome gene. These approaches identify affected individuals where tumour immunohistochemistry and/or microsatellite instability analysis could lead to identification of a DNA mismatch repair gene mutation. Bethesda criteria are not discriminatory within this group because all patients fulfil these criteria due to age alone. Recommendation grade: B
People with only one affected relative and who do not fulfil any of the above criteria, and do not fulfil high risk criteria, should be reassured and encouraged to avail themselves of population-based screening measures. The low level residual risk over that of the general population should be explained. Recommendation grade: B
Introduction
People with a family history of colorectal cancer but who do not have one of the high risk genetic disorders (see pages 675–680) have an increased personal risk of the disease. This guidance addresses the cancer risk of asymptomatic individuals who have one or more affected relatives.
Colorectal cancer is common and so many people have an affected relative by chance. In various studies, 4–10% of control subjects report at least one affected first-degree relative.213–216 The greater the number of affected relatives and the younger the age at onset, the greater the personal risk.213–216 However, there are no pathognomonic features of this category of familial clustering of colorectal cancer and so, apart from hereditary non-polyposis colorectal cancer (Lynch syndrome), familial adenomatous polyposis (FAP) and other cancer susceptibility syndromes, at-risk groups are currently defined by empiric family history risk criteria. Guidance concerning people with a family history that fulfils criteria for Lynch syndrome (hereditary non-polyposis colorectal cancer, HNPCC) or other autosomal dominant genetic syndromes associated with colorectal cancer susceptibility, and people with mutations in known colorectal cancer susceptibility genes (eg, adenomatous polyposis coli or DNA MMR genes), irrespective of the family history, is given on pages 675–680.
Although risk of colorectal cancer can be stratified by family history parameters for groups of people, it is important to emphasise that the risk is heterogeneous for individuals within such categories. Furthermore, because the population lifetime risk in the UK is around 1:20, some people without any family history will develop colorectal cancer, and this residual population risk should be made explicit.
Family history and personal colorectal cancer risk
Risk of colorectal cancer can be estimated empirically from the individual's current age, the age at onset of affected relatives, and the number and relationship of those relatives (table 3). It is important to consider the underlying basis of excess familial risk within populations, which is comprised of a heterogeneous composite of high-penetrance single gene disorders, multiple low-penetrance genetic factors (polygenic inheritance) and shared familial environmental exposure. While it is important to recognised those with a defined colorectal cancer susceptibility syndrome, a ‘positive family history’ is best seen as a risk factor due to genetics and familial environment. While there is an excess risk to people with any affected family member (relative risk 2.24),217 not all familial aggregations indicate sufficiently high absolute risk to merit colonoscopic surveillance.218 Close relationship, early age at onset and number of affected relatives are each indicators of elevated risk. Thus the function of the familial groupings presented here is to categorise risk. However, it is important to be aware that rarely, a first-degree relative dying of unrelated causes might connect a second-degree kinship with a high incidence of colorectal cancer. It is important to emphasise that the absolute population risk for younger age groups is low and so even relatively high relative risks do not necessarily indicate a requirement for surveillance. Estimates of absolute 10-year colorectal cancer risk emphasise the critical importance of current age of the person at risk.217 218
Frequency: prevalence and incidence
Because colorectal cancer is common in the general population, the prevalence of a family history is commensurately high. In control groups from the general population, the prevalence of a family history of one or more affected first-degree relatives is 4–10%.213 214 219–222 However, the majority of estimates in controls are not representative of population prevalence because controls were age-matched with colorectal cancer cases, reflecting the older age distribution of the disease. Cohort studies minimise this potential bias, and one large study of 119 116 participants (mean age about 50 years) reported at least one affected first-degree relative in 9.8% of participants.216 Another cross-sectional study of population controls evenly distributed in age groups from 30 to 75 years showed that 9.4% had one or more affected first-degree relatives after exhaustive pedigree tracing.223 Population prevalence of a family history is high when a non-restrictive inclusion criterion is employed such as ‘any family history’. The prevalence is lower for more stringent family history criteria such as ‘two or more affected first-degree relatives’. In two large case–control studies, 0.4% of the control group fulfilled the latter criterion,213 214 although in a cohort study only 0.006% had two or more affected first-degree relatives.216 An Australian study suggests the prevalence of a family history of an affected relative aged <45 years in control populations is around 0.2%.213 Overall, around 10% of the general population have at least one affected first-degree relative, whereas approximately <1% fulfil family history criteria for which intervention is recommended in this guideline.
Intervention
Surveillance of individuals at moderate risk has been the focus of much controversy, due primarily to the absence of randomised trial evidence. Here, observational data are compared using surveillance-detected neoplasia in various family history risk categories. A substantial proportion of neoplasms are located in the proximal colon in people with a family history of colorectal cancer, particularly women.214 224 225 Around 30% of proximal lesions would not have been identified if flexible sigmoidoscopy had been used to target those requiring colonoscopy. However, colonoscopy is not without problems, since about 6% of adenomas >1 cm are missed in average risk populations,226 while serious complication rates are around 1:300–500 (see below). Nonetheless, full colonoscopy is the recommended form of surveillance for people in this risk category, as it affords opportunity for therapeutic intervention and biopsy. Surveillance experience using risk categories described in previous iterations of these guidelines has been reported,227–229 and few significant lesions are missed when the guidelines are applied. However, it is important to be aware that blanket application of such guidance to all family history categories is inadvisable because high risk families can initially manifest as a moderate risk family cluster.229 Prevalence of neoplasms at initial or subsequent surveillance colonoscopy in patients fulfilling moderate risk criteria is particularly low for those less than 45 years old.228 Hence, observational case–control data combined with clinical studies in patients fulfilling family history criteria strongly support the premise that initial surveillance should commence at age 55 years for people with one affected relative <45 years old (note: age criteria are heterogeneous across studies between age <50 years and <45 years) or at least two affected first-degree relatives. People with only one affected relative aged <45 years and those with only two affected first-degree relatives (at older ages) have a low subsequent observed frequency of significant neoplasia,230 and so there is no rationale for continued surveillance and therefore once-only colonoscopy is recommended.
It should be noted that early-onset cancer represents a special case because of the enhanced risk of high-penetrance disorders such as FAP and Lynch syndrome. Cases of FAP should be sought, alerted through clinical features, dominant family history of polyposis or mutation analysis; web-based and other algorithms have been developed and validated to predict groups likely to be a carrier of a DNA MMR gene mutation.127 231 232 In practice, all incident cases of colorectal cancer aged <50 years could have tumour material tested for high-frequency microsatellite instability (MSI-H) or have immunohistochemistry. This may be implemented systematically through pathology departments depending on local arrangements, but subsequent referral to clinical genetics departments is essential for cases exhibiting MSI-H or loss of expression of DNA MMR genes. If no local arrangement is available, referral to clinical genetics should be considered, particularly for right-sided tumours. Web-based algorithms (eg, http://hnpccpredict.hgu.mrc.ac.uk/) are helpful in this setting to provide a numerical estimate of the likelihood of mutation carriage, thereby highlighting those who should be referred to clinical genetics, especially when tumour microsatellite instability testing/immunohistochemistry is not available.
Analysis of tumour material from an affected relative may also be feasible because immunohistochemistry for DNA MMR genes (MSH2, MLH1, MSH6, PMS2) or tumour microsatellite instability testing might indicate Lynch syndrome. Where these results indicate a high chance of Lynch syndrome, index patients and relatives should be treated in accordance with the high risk guidance. Where these do not indicate Lynch syndrome, then low intensity screening (see tables 2, 3 and 4) is indicated, since the excess risk is small.233 It has been shown that such a surveillance strategy in familial colorectal cancer is effective and efficient.234 Referral to a clinical genetics service is recommended whenever criteria in table 3 are met.
Summary of recommendations for colorectal cancer screening and surveillance high risk disease groups
Summary of recommendations for colorectal cancer screening and surveillance in moderate risk family groups
Summary of recommendations for colorectal cancer screening and surveillance in high risk family groups
There are two sub-categories within the moderate risk group which take into account recent prospective observational data: high–moderate and low–moderate. Individuals with a lesser family history should be recommended population risk measures.
High–moderate risk: 5-yearly colonoscopy recommended from age 50 to age 75
The high–moderate risk category comprises: people with three or more affected relatives in a first-degree kinship with each other (none less than 50 years old, otherwise they would fulfil high risk criteria), two affected relatives less than 60 years old in a first-degree kinship with each other, or two affected relatives with a mean age less than 60 years old in a first-degree kinship (note this is a pragmatic approach and is not based on strong supporting evidence). Germline transmission to the at-risk individual must be a possibility (ie, affected relatives must include a parent, or at least two siblings or at least two children or a child+sibling).
People in the high–moderate risk category merit low-intensity surveillance comprising 5-yearly colonoscopy commencing at age 50 until age 75 years. Polyps must be snared and histologically characterised; if adenomas are present surveillance should be instigated as per adenoma surveillance. Recommendation grade: B
Low–moderate risk: once-only colonoscopy recommended at age 55
Inclusion criteria comprise those with only one affected relative less than 50 years old or only two affected first-degree relatives aged 60 years or older.
If the colon is clear of neoplasia, then recommend measures relevant to population risk. Polyps must be snared and histologically characterised. If an adenoma is identified, then adenoma surveillance guidance applies. Recommendation grade: B
The projected benefit of surveillance at age 55 years in this group is somewhat more tangible than in younger age groups. The proportion of people aged 55 years with at least one adenoma has been variously reported as 4–21%, but only 2–6% have significant neoplasia.227 230 234 235 Extrapolating from contemporary population incidence data for this age group and applying a relative risk of about 3 due to family history,217 around one in 180 people will harbour a high risk colorectal neoplasm/cancer at screening, assuming a 3-year neoplasia dwell time.
Costs, benefits and adverse events
There has been no formal assessment of the cost effectiveness of a single screening colonoscopy at age 55 years. One analysis indicated that regular colonoscopy is only cost effective in people with two affected first-degree relatives,236 while another indicated that 3-yearly colonoscopy would cost £18 750 per cancer detected, £26 250 per life saved and £3000 per life-year saved.237 Hence, screening does appear to be cost effective in comparison with population breast cancer screening. However, the intensity of screening merits careful consideration, since the risk of surveillance-related morbidity is cumulative with each screening episode.
The perforation rate after polypectomy is 22 (CI 13.8 to 33.3) per 10 000. Post-polypectomy bleeding occurs in a further 89 (CI 71.5 to 109.5) per 10 000. The rate of colonoscopy-related mortality is low but appreciable, being reported in specialist centres as 0.83 per 10 000 procedures (CI 0.025 to 3.69), and 3.9 per 10 000 (CI 1.1 to 8.8) after polypectomy. However, a cross-sectional audit of 68 NHS endoscopy units in the UK revealed an unexpectedly high death rate directly attributable to colonoscopy of six per 10 000.238 Hence, taken together, there is a small but appreciable risk of complications from colonoscopy. Overall frequency of perforation, bleeding and death should be taken as 0.3%, 0.3% and 0.02%, respectively.
Based on current demographic data, there are approximately 150 000 people within the screening age group (35–70 years) in a population of 300 000 served by a district general hospital. Within this group there are a projected 750 individuals with a family history fulfilling high–moderate or moderate risk criteria. Assuming 80% compliance, these criteria would generate a projected 70 additional colonoscopies annually, at a total cost of £33 320 per annum (£476 per colonoscopy). Additional costs associated with treatment of complications would be negligible for such a small target screening population.
Audit
It is recommended that there should be rolling audit of outcomes for people attending because of concern about a family history of colorectal cancer. Such audit will accrue data on effectiveness and acceptability of the strategy laid out in this guidance. Outcomes to be audited should include total number of referrals (including those dealt with using postal advice to general practitioners/patients), extent of family history and risk category assigned, proportion recommended surveillance, compliance with recommended surveillance, surveillance-related morbidity/mortality, adenoma and cancer prevalence in those recommended surveillance, cancer incidence in those not fulfilling criteria for this guideline and overall survival in all referrals by risk category assigned.
Acknowledgments
JAE and MDR thank Professor John Nicholls for his help on the post-surgical surveillance guidance of their section.
References
Footnotes
All authors identified have contributed to the manuscript as indicated. SC and JHS were co-editors.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.