Article Text

Abstract
Background and aims: The Danish Polyposis Register was established in 1971 with the aim of improving the poor prognosis of familial adenomatous polyposis (FAP), and in 1975 the register became national. The aim of the present study was to evaluate the prevalence of colorectal cancer and survival rate in FAP patients before and after the establishment of the Danish Polyposis Register.
Patients and methods: The Danish Polyposis Register was established by collecting information on probands and construction of their pedigrees. Family members at risk were offered prophylactic endoscopic and molecular genetic examination, and affected individuals were treated by colectomy.
Results: At the end of 2001, the Danish Polyposis Register included 434 patients from 165 families. The incidence rate was 1.90×10−6 and the prevalence rate 4.65×10−5. Colorectal cancer on the basis of FAP constituted 0.07% of all colorectal cancers in the 1990s. Colorectal cancer was diagnosed in 170/252 probands (67%) and in 5/182 call-up patients (3%) (p<0.001). The cumulative crude survival was 94% in call-up patients compared with 44% in probands (p<0.0001). A comparison of two periods, 1900–1975 and 1976–2001, demonstrated a decreased prevalence of colorectal cancer from 60% to 27% (p<0.0001), and an increased use of colectomy from 52% to 93% (p<0.00001). The cumulative crude survival in FAP showed substantial improvement with time (p<0.00001).
Conclusion: Since the establishment of the Danish Polyposis Register, the prevalence of colorectal cancer has decreased considerably and the prognosis has improved substantially. The work of the Danish Polyposis Register is probably the main cause of this improvement.
- familial adenomatous polyposis
- hereditary colorectal cancer
- national registration
- FAP, familial adenomatous polyposis
Statistics from Altmetric.com
Familial adenomatous polyposis (FAP) is a rare autosomal dominant disease caused by a defect in the apc gene on chromosome 5q21, and traditionally characterised by at least 100 colorectal adenomas. Almost all affected untreated patients will die from colorectal adenocarcinoma at the age of 40–50 years, and this was the general fate of polyposis patients in most countries until the second half of the 20th century.1 Furthermore, FAP includes a variety of extracolonic manifestations: osteomas, epidermoid cysts, desmoid tumour, upper gastrointestinal polyps, congenital hypertrophy of the retinal pigment epithelium, and other malignancies (duodenal carcinoma, thyroid carcinoma, and hepatoblastoma).
In 1925, Lockhart-Mummery demonstrated that prophylactic examination of family members at risk and colectomy in affected individuals reduced the frequency of colorectal cancer. On this basis, the St Mark’s Hospital Polyposis Registry was founded as the first polyposis register in the world.2 Since then several national and regional polyposis registries have been established around the world, and the Leeds Castle Polyposis Group was established in 1985 as an international polyposis research forum.3 Reduction in the prevalence of colorectal cancer has prolonged the life of the majority of polyposis patients, and the mortality pattern has changed substantially over the past decades. Today, the most frequent causes of death in screen detected patients are duodenal cancer and desmoid tumour.4–7
The aim of the present study was to evaluate changes in the prevalence of colorectal cancer and the prognosis of FAP on the basis of data from the Danish Polyposis Register over a period of 25 years after the register became national.
METHODS
Definitions
-
Familial adenomatous polyposis: Autosomal dominant hereditary disease caused by a defect in the apc gene and characterised by the development at least 100 colorectal adenomas (less in young first degree relatives of probands).
-
Proband: Patient diagnosed due to bowel symptoms and without any knowledge of hereditary bowel disease.
-
Call-up patient: Screen detected patient diagnosed at a prophylactic examination due to a diagnosis of FAP in his/her first degree relatives.
-
Verified patient: Patient with histologically verified FAP.
-
Assumed patient: Patient with clinical and genealogical indications of FAP but without histological verification.
Diagnostic strategy
Sigmoidoscopy was used as the only primary diagnostic procedure in first degree relatives, and colonic examination was not performed in individuals with a normal sigmoidoscopy. In the last decade, rigid proctosigmoidoscopy was replaced by flexible sigmoidoscopy. Polyps found during sigmoidoscopy were removed for histological examination to ensure a histological diagnosis of adenomas, and in patients with adenomas a further evaluation was performed by colonoscopy (double contrast barium enema until about 1980). Gastroduodenoscopy has been recommended in adult polyposis patients since 1985,8 and a five nation prospective trial (DAF study) was performed in 1990–2000.9
Register and patients
The Danish Polyposis Register was established in 1971 with the aim of improving the prognosis in FAP by: (1) registration of patients and their family members; (2) initiation and coordination of screening of family members at risk; and (3) treatment of those diagnosed as being affected. In 1975 the register was extended and became national. The first phase of the national register included collection of information on probands and assumed patients from multiple sources: the Danish Cancer Registry, hospital records, general practitioners, and specialists in private practice. During the second phase, the pedigrees of the probands and assumed patients were constructed by additional information from the Central Office of Civil Registration (founded 1968), local population registers, the National Patient Register (founded in 1976), parish registers, death certificates, and probate courts. The third phase comprised prophylactic examination of all first degree relatives of affected family members in collaboration with the general practitioners of these family members. They were asked to inform their patients about the disease and the cancer risk, and to arrange a proctosigmoidoscopy. In first degree relatives with normal endoscopy, regular examination was planned every second year until age 40 years, and general practitioners were asked to report the continuous results of the surveillance to the Register.10 Since 1987 molecular genetic analysis has been added to the diagnostic armamentarium,11 but only a small number of first degree relatives have been examined. Newly diagnosed call-up patients (gene carriers with or without adenomas) were referred to the regional department of surgery for further endoscopic evaluation and surveillance, and eventually prophylactic colectomy. No further surveillance was planned in non-gene carriers. Children of affected patients were offered genetic counselling and DNA analysis at the age of 10 years, and regular sigmoidoscopic surveillance was performed in families without a known mutation and in at risk persons who did not want DNA analysis. All results were collected in the Polyposis Register, which includes a computerised database. The register has been approved by the Danish Data Protection Agency (Jr No 1992-1223-005).
There was little information on FAP in the Danish medical community before the establishment of the Danish Polyposis Register. Since 1975 the register has been continuously active in spreading information and education about the disease: a patient information leaflet has been produced in cooperation with the Danish Cancer League and sent to all patients, an information leaflet for medical colleagues has been sent to all surgical departments and specialists in private practice, courses have been arranged for specialists and general practitioners, oral presentations have been made in the national societies of surgery and gastroenterology, and articles have been published in national and international journals. Furthermore, comprehensive direct contact has been established between the Register and numerous colleagues involved in the management of FAP.
Epidemiological analysis
The annual incidence rate for a decade was calculated by dividing the number of newly diagnosed FAP cases within this decade by the mean population in the same decade.11 The point prevalence rate was calculated by dividing the number of FAP patients alive on the 31 December by the total population on the same date. The proportion of newly diagnosed FAP patients with colorectal cancer among all Danish colorectal cancer patients was calculated by dividing the number of newly diagnosed FAP patients with colorectal cancer in a period by the number of newly diagnosed patients with colorectal cancer in the same period.12
Statistical analysis
The χ2 test was used to compare differences in proportions of events, and the Kaplan-Meier estimate to calculate cumulative crude survival rates. Differences between subgroups were analysed by the log rank test. The level of statistical significance was chosen at p<0.05. Analyses were performed using SPSS software, version 10.1.
RESULTS
Patient series
At the end of 2001, the register included information on 165 families with 508 affected members (275 males, 232 females, one sex unknown). Seventy four were assumed cases and 434 (85%) were verified cases, including 252 probands (58%) and 182 call-up patients (42%). The year of diagnosis of verified patients is shown in fig 1. A total of 163 (65%) were familial cases and 89 (35%) were isolated cases. The apc mutation was known in 34/76 families (45%) with more than one affected member, and in 18/89 isolated cases (20%).
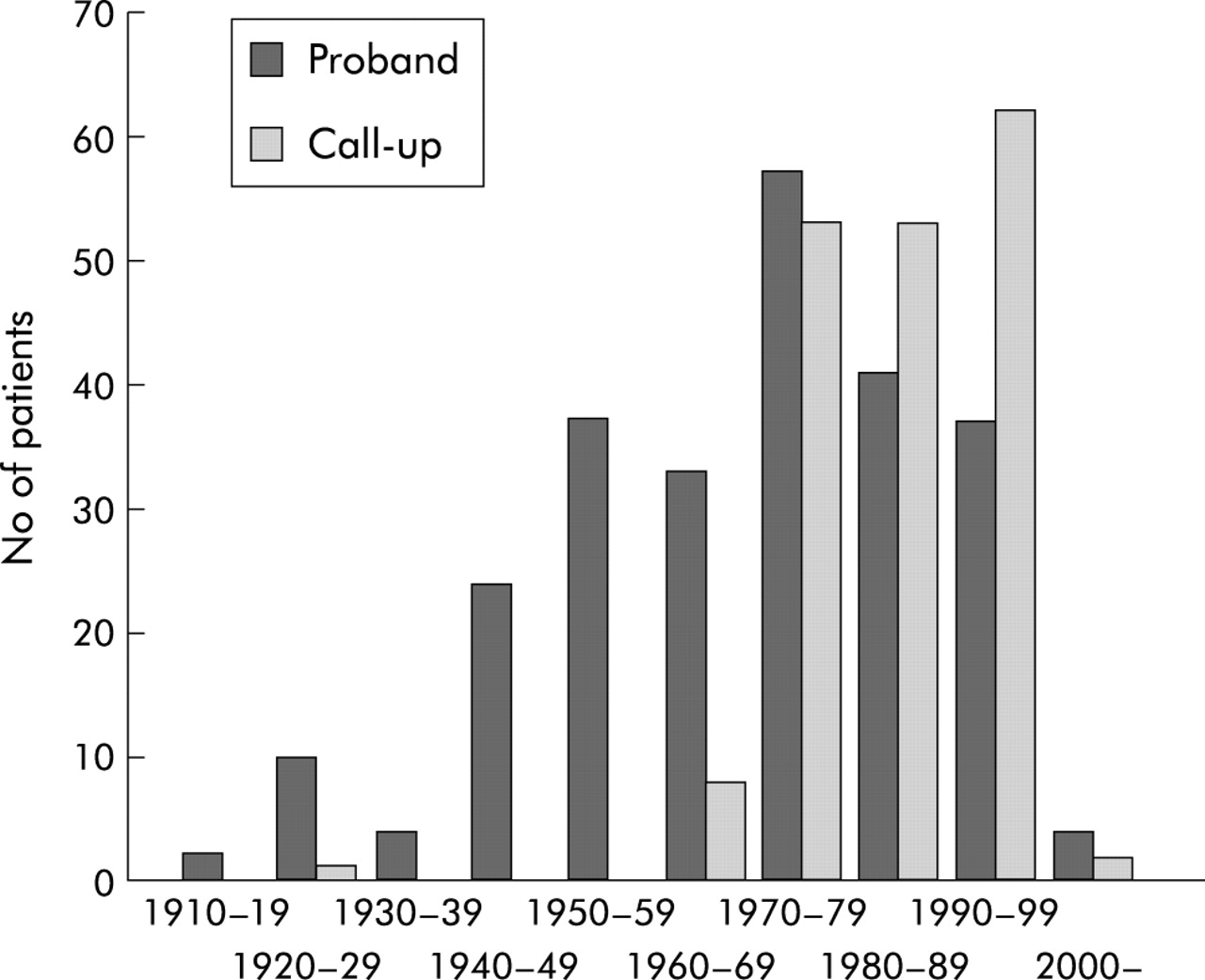
Year of diagnosis in 434 verified patients.
The families included 585 first degree relatives (297 males, 284 females, four sex unknown) with no evidence of colorectal adenomas. Forty four had emigrated or were untraceable. Among the remaining 541 individuals, 130 have not been examined due to age >60 years (n=75) or <10 years (n=55). A total of 343 are followed in a regular endoscopic surveillance programme, 29 have refused, and the status of 39 is unknown. To date, 91 first degree relatives have been classified as non-gene carriers by DNA analysis.
Epidemiology
The mean annual incidence rate in 1970–1979 was 2.04×10−612 and the present calculation showed 1.84×10−6 in 1980–1989 (94 new FAP cases, mean population 5 128 737) and 1.90×10−6 in 1990–1999 (99 new FAP cases, mean population 5 232 715). The point prevalence rate increased steadily to 3.19×10−5 at the end of 199213 and to 4.65×10−5 at the end of 1999 (248 live FAP patients, population 5 330 020). FAP constituted 0.12% of Danish colorectal cancer patients in 1970–79.13 The proportion was 0.09% in 1980–89 (28 FAP patients with colorectal cancer, 32 157 colorectal cancers) and 0.07% in 1990–1998 (24 FAP patients with colorectal cancer, 30 005 colorectal cancers).14 National colorectal cancer figures for 1999 are not yet available.
The completeness of the registration was 90% for the period 1976–198215 and 97% in 1983–1992.13
Course of the disease
The natural course of the disease is characterised by five stages: (1) development of adenomas (estimated in call-up cases followed from normal endoscopic findings to the first adenomas), (2) bowel symptoms (probands), diagnosis of adenomas due to symptoms (probands), (3) diagnosis of colorectal cancer (probands), and (4) death from colorectal cancer (untreated assumed cases) (table 1). In call-up cases the median age at diagnosis of FAP was 19 years (range 5–66) and the median age at diagnosis of cancer was 48 years (range 40–58).
Natural course of familial adenomatous polyposis (FAP)
Colorectal cancer was diagnosed at the time of diagnosis of FAP in 170/252 probands (67%) and in 5/182 call-up patients (3%) (p<0.001). The 175 patients with colorectal cancer had 223 tumours: 137 patients had one cancer, 38 patients (22%) had synchronous cancer, 28 had two tumours, and 10 had three tumours. The most advanced tumour stage in 124 patients with classifiable tumours showed Dukes’ A in 19 (15%), Dukes’ B in 34 (28%), and Dukes’ C in 71 (57%). Four of five call-up patients with cancer had a Dukes’ B tumour and one had a Dukes’ C tumour.
A total of 109 Danish patients in the DAF study were examined with gastroduodenoscopy every two years in 1990–2000. One patient had duodenal carcinoma at the first examination and another patient had duodenal cancer diagnosed at the fifth endoscopy.9
Twenty six probands (10%) had no colorectal surgery: 12 had disseminated cancer, three refused surgery, and the cause was unknown in 11. Thirty eight call-up patients had no surgery: 32 had not yet had their planned prophylactic colectomy performed, one refused operation, and the cause was unknown in five. The surgical procedures are shown in table 2. Colectomy was performed in 134/226 probands (59%) compared with 143/145 call-up cases (99%) (p<0.0001).
Surgical treatment
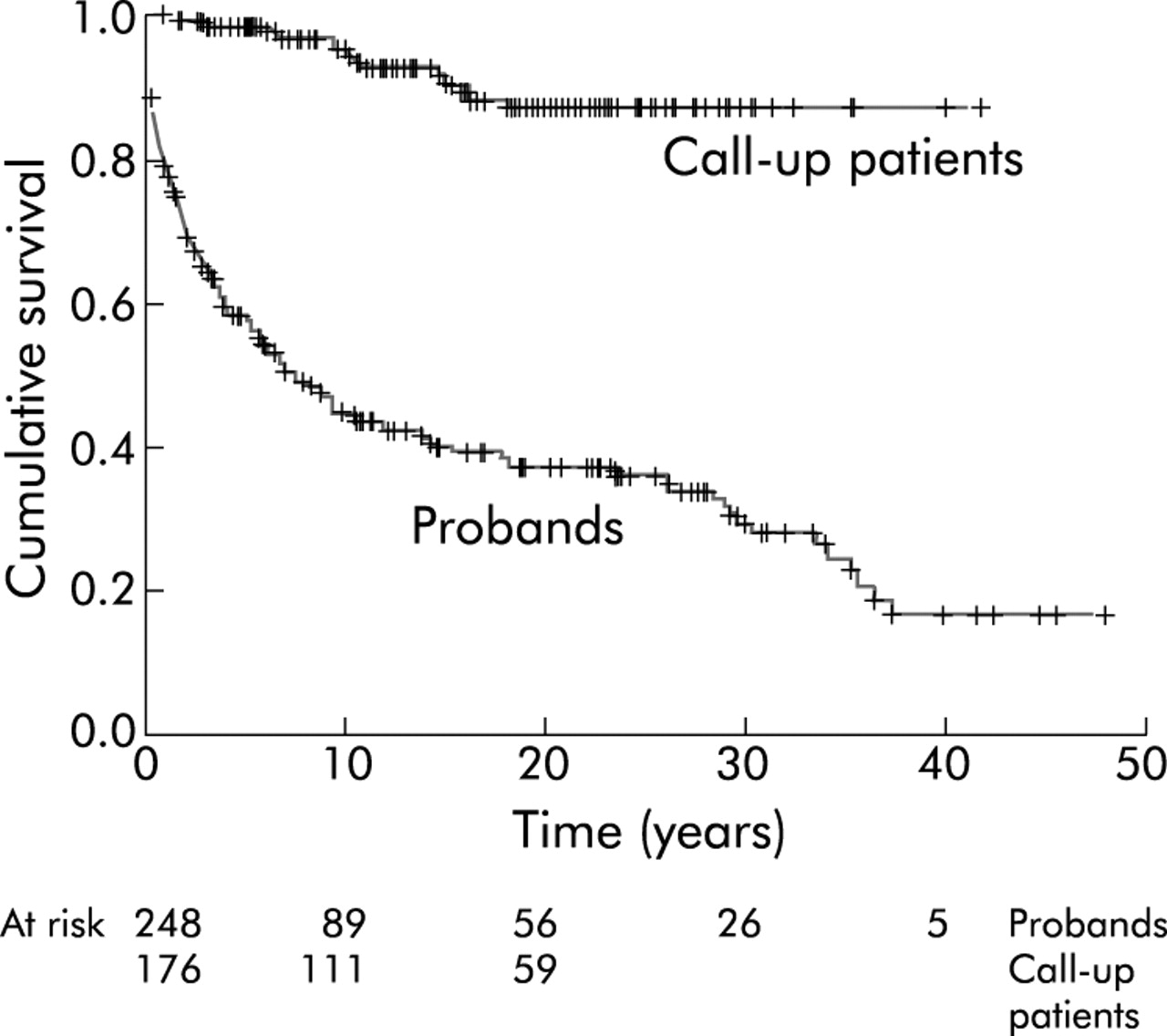
At the end of 2001, 248 verified patients were alive, 175 had died, eight had emigrated, and three were lost to follow up. The cause of death was colorectal cancer in 121 (69%), non-malignant disease in 24 (14%), non-FAP related cancer in 14 (8%), duodenal cancer in five (3%), postoperative complications in four (2%), desmoid tumour in three (2%), hepatoblastoma in one (1%), and unknown in three (2%). The cumulative crude 10 year survival was 94% (95% confidence limits 92–96) in call-up cases compared with 44% (95% confidence limits 41–47) in probands (p<0.0001) (fig 2).

Crude survival in probands and call-up cases (p<0.0001).
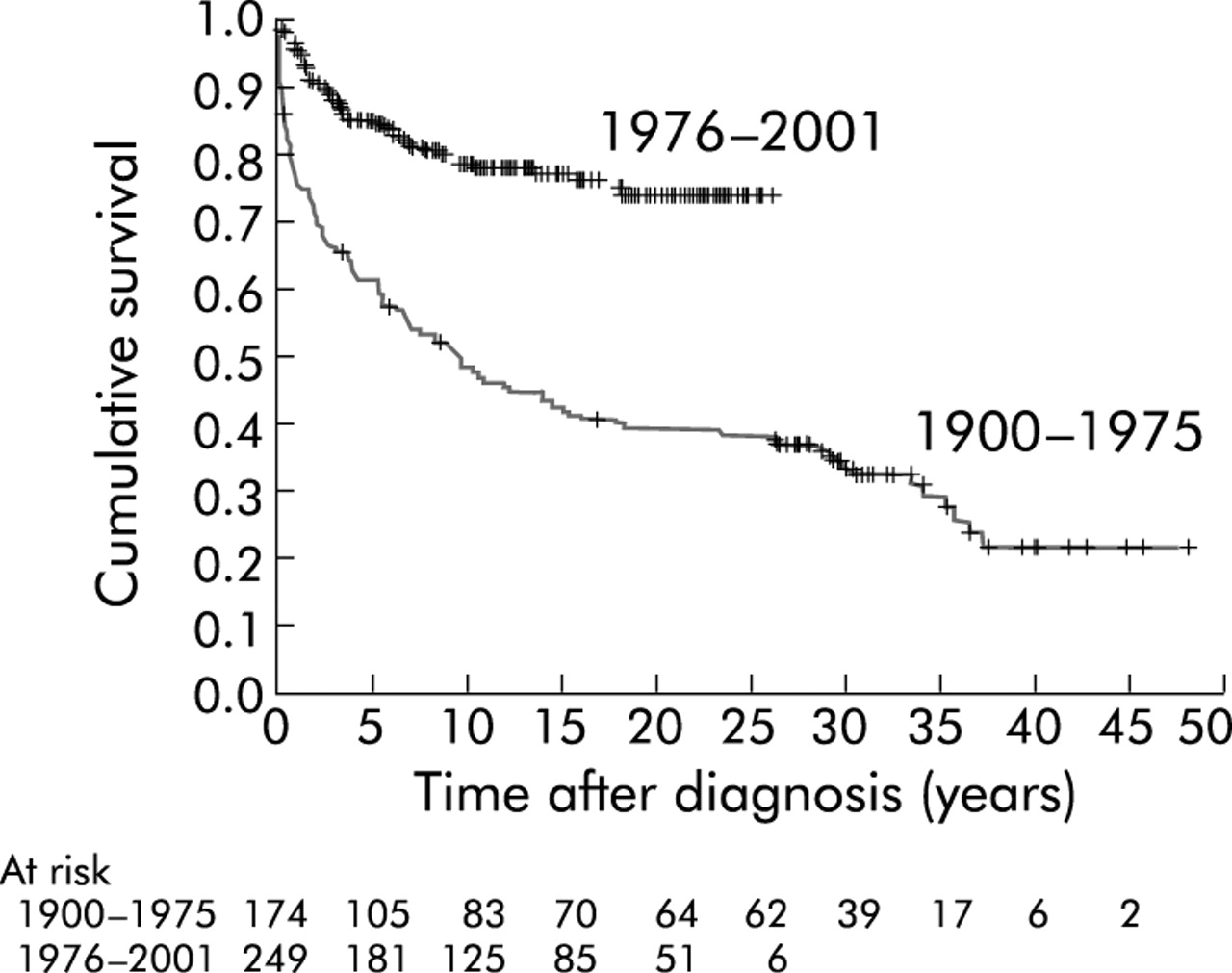
To compare the course and prognosis of FAP before and after establishment of the Polyposis Register, selected variables were calculated for the periods 1900–1975 and 1976–2001. The proportion of call-up cases among all verified patients increased from 19% (33/176) in 1900–1975 to 58% (146/252) in patients diagnosed in 1976–2001 (p<0.00001). The occurrence of colorectal cancer at diagnosis of FAP decreased from 60% (105/175) in 1900–1975 to 27% (68/250) in 1976–2001 (p<0.00001), which is a 55% reduction. The use of colectomy increased from 52% (82/159) in 1900–1975 to 93% (193/208) in 1976–2001 (p<0.00001). The cumulative survival of all FAP patients showed improvement with time (p<0.00001) (fig 3).
{kind=link}
{kind=link}
{kind=link}
Crude survival of verified patients diagnosed in 1900–1975 and 1976–2001 (p<0.0001).
DISCUSSION
Since the establishment of the Danish Polyposis Register, the prevalence of colorectal cancer has decreased by 55% in newly diagnosed polyposis patients, and a substantial improvement has taken place in long term survival.
Population based studies of FAP have only been carried out in the Nordic countries.16–19 The prerequisites for such studies are a stable population, long term and complete registration of all citizens, a longstanding national polyposis register with a high completeness of registration, and a health care system of an equal high standard and open to all citizens, independent of their social or economic status. These conditions are all met in Denmark, which therefore provides excellent possibilities for epidemiological studies.
Over the last decades national polyposis registers have been established in Europe7,10,19–24 and Japan.25 Several regional registers have been founded in Europe,26–31 North America,32,33 and Australasia.34–37 The overall results from some of these registers are shown in table 3. The finding of 68% of probands with colorectal cancer in the present series is similar to most other major series. The low frequency of colorectal cancer in call-up patients (3%) was also similar to other Nordic registries and the Dutch registry, indicating the efficacy of the prophylactic work in these countries.
Results from national and regional polyposis registries
The annual incidence rate is approximately 2×10−6 and the rate has been stable since the 1970s.13 The rate is higher than in Finland18 and Sweden17 for unknown reasons. The prevalence rate is similar to the Swedish result17 and slightly higher than that in Finland.21 In Denmark, the polyposis based proportion of all colorectal cancer cases has been reduced by 42% since the 1970s to 0.07% in the 1990s. This is three times higher than the Swedish estimate of 0.023 for the period 1977–1996 which is, however, based on colorectal cancers in 1996 only and not on all colorectal cancers in the 20 year period.17 This may cause bias towards a low value due to the increasing incidence of colorectal cancer. The Finnish proportion of 0.1422 may be explained in part by the fact that the incidence of colorectal cancer in Finland is only about half that of the incidence in Denmark. Age at the five stages of the natural course of the disease is very similar to values in the literature.1,17,19,27,38
In the present series, 3% of cases died from duodenal cancer, which is similar to the Dutch result19 but lower than the 8% seen in the Cleveland Clinic series,4 possibly due to differences between a national series and a major referral centre. Desmoids were the cause of death in 2% in our series, in contrast with 7% in the Dutch series19 and 11% published by Arvanitis and colleagues.4 It is not known whether these variations represent true differences.
The cumulative crude survival estimates showed a substantial and expected difference between probands and call-up cases, which demonstrates the effect of prophylactic examination and treatment, and confirms our previous findings16 and the Finnish results.18 Heiskanen et al were the first to present a calculation of the relative 10 year survival and found a cumulative rate of 60% in probands and 98% in call-up cases.18 A comparison of the survival rate between probands and call-up patients with colorectal cancer may further illustrate the overall progress in the treatment of FAP. However, such an analysis is not possible due to the low number of call-up patients with cancer.
Comparison of the two periods before and after the establishment of the Polyposis Register demonstrated a pronounced change from a majority of probands to a majority of call-up cases. A 55% reduction in the prevalence of colorectal cancer was seen. Moreover, the treatment has improved considerably as colectomy has been performed in almost all polyposis patients during the past 25 years compared with approximately 50% before this period. Finally, there has been a pronounced improvement in survival since the establishment of the register.
In conclusion, the prevalence of colorectal cancer has decreased considerably, and the prognosis has improved substantially since the establishment of the National Danish Polyposis Register. This is probably a result of the work of the Polyposis Register as there was limited knowledge of FAP before its establishment. A precise evaluation of the effect of the national registration is however not possible without a comparison with a population from the same time period and without a national polyposis registration. Other factors which may have influenced the results are the general improvement in endoscopic and surgical methods and the increasing information on the disease from multiple sources.
Colorectal cancer has become a rare finding when diagnosing polyposis in families under regular surveillance, and from now on colorectal cancer ought to occur almost entirely in probands who are new mutations. Furthermore, the increasing use of restorative proctocolectomy may contribute to a reduction in another major polyposis problem, rectal cancer after ileorectal anastomosis. Future FAP research can then be directed towards the two remaining major and yet unsolved problems, duodenal neoplasia and desmoid tumour.
Acknowledgments
The study was funded by a grant from “Ingeborg Roikjer’s Fund”. The author is indebted to numerous general practitioners, specialists in private practice, and colleagues in hospital departments for excellent longstanding cooperation.