Article Text

Abstract
Objective International guidelines recommend endoscopic surveillance of premalignant gastric lesions. However, the diagnostic yield and preventive effect require further study. We therefore aimed to assess the incidence of neoplastic progression and to assess the ability of various tests to identify patients most at risk for progression.
Design Patients from the Netherlands and Norway with a previous diagnosis of atrophic gastritis (AG), intestinal metaplasia (IM) or dysplasia were offered endoscopic surveillance. All histological specimens were assessed according to the updated Sydney classification and the operative link on gastric intestinal metaplasia (OLGIM) system. In addition, we measured serum pepsinogens (PG) and gastrin-17.
Results 279 (mean age 57.9 years, SD 11.4, male/female 137/142) patients were included and underwent at least one surveillance endoscopy during follow-up. The mean follow-up time was 57 months (SD 36). Four subjects (1.4%) were diagnosed with high-grade adenoma/dysplasia or invasive neoplasia (ie, gastric cancer) during follow-up. Two of these patients were successfully treated with endoscopic submucosal dissection, while the other two underwent a total gastrectomy. Compared with patients with extended AG/IM (PGI/II≤3 and/or OGLIM stage III–IV), patients with limited AG/IM (PG I/II>3 and OLGIM stage 0–II) did not develop high-grade adenoma/dysplasia or invasive neoplasia during follow-up (p=0.02).
Conclusion In a low gastric cancer incidence area, a surveillance programme can detect gastric cancer at an early curable stage with an overall risk of neoplastic progression of 0.3% per year. Use of serological markers in endoscopic surveillance programmes may improve risk stratification.
- premalignant gastric lesions
- surveillance
- endoscopy
- OLGIM
- pepsinogen
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Premalignant gastric lesions predispose to the development of intestinal type gastric cancer.
Helicobacter pylori gastritis is considered the starting point of the carcinogenic pathway.
Identification of patients with increased gastric cancer risk remains difficult.
What are the new findings?
This multicentre prospective cohort study showed stable disease in the majority of patients during an average 4.7 years of follow-up.
In this low gastric cancer incidence area, the overall risk of neoplastic progression was 0.3% per year.
Risk stratification based on only histology was not completely sufficient in discriminating low-risk patients from high-risk patients.
Patients with limited atrophy/intestinal metaplasia (PG (pepsinogen) I/II>3 and OLGIM (operative link on gastric intestinal metaplasia) stage 0–II) did not develop high-grade adenoma/dysplasia or invasive neoplasia during follow-up.
How might it impact on clinical practice in the foreseeable future?
These data highlight the need of proper identification of subjects with an increased risk of gastric cancer, which might be improved by adding serological markers as non-invasive tool.
The data provide important input for international guidelines on the management of patients with premalignant gastric lesions.
Introduction
Gastric cancer is the third leading cause of cancer-related mortality, and the fifth most common malignancy worldwide.1 More than 70% of gastric cancer cases occur in developing countries, with highest incidences in Eastern Asia, Eastern Europe and parts of central and South America. Although the global incidence and mortality rates are declining, the number of new cases and fatalities increase annually due to expansion and ageing of the world population.2 In Western Europe, the age standardised rates of gastric cancer incidence are relatively low with 8.8 cases/1 00 000/ year in men and 4.3 cases in women.1 Nevertheless, mortality rates remain high, as most of the cases are diagnosed at a late stage, leading to 5-year survival rates of approximately 21% in the Netherlands and 24% in Norway.3
Premalignant gastric lesions predispose to the development of intestinal type gastric cancer.4 Helicobacter pylori gastritis is considered the starting point of the carcinogenic pathway, in which inflammation evolves to gland loss, metaplasia, low-grade adenoma/dysplasia (LGD), high-grade adenoma/dysplasia (HGD) and eventually invasive neoplasia (ie, gastric cancer) in 1%–2% of the infected patients.5 As a result, regular endoscopic follow-up is recommended in patients with premalignant gastric lesions.6 7 However, most of the patients with H. pylori and premalignant gastric lesions do not develop gastric cancer. Moreover, premalignant gastric lesions affect a substantial proportion of the population above 50 years of age.8 A proportion of patients show regression of premalignant lesions during endoscopic follow-up, either reflecting an effect of sampling or true regression after H. pylori eradication.9 10 Therefore, proper identification by targeted surveillance of subjects with an increased risk of gastric cancer is indicated. This will additionally result in a decrease in burden for patients and limit the use of endoscopy resources.
Currently, it remains difficult to identify patients with an increased gastric cancer risk and to determine optimal surveillance strategies in order to prevent the development of invasive neoplasia. In 2012, the first international guideline on this topic was published (MAnagement of Precancerous conditions and lesions of the Stomach—MAPS guideline).6 This guideline recommended endoscopic surveillance in patients with moderate to severe atrophic gastritis (AG), in those with marked intestinal metaplasia (IM) in both antrum and corpus, and in patients with dysplasia. Surveillance was not recommended for patients with AG or IM limited to antrum. The gold standard for the phenotype ‘extensive atrophy/IM’ is yet to be defined. So far, this phenotype is mostly based on histological examination obtained by biopsies. In order to evaluate the yield of surveillance of premalignant gastric lesions, prospective cohort studies are needed, also to confirm that the guideline recommendations are also applicable for low-risk areas. Due to a lower incidence of gastric cancer in these areas, there is less experience in a comprehensive endoscopic assessment of the gastric mucosa, which may negatively influence the yield of surveillance.
In this multicentre prospective cohort study, we aimed to evaluate the incidence of neoplastic progression during endoscopic follow-up in patients living in low-incidence countries. The yield of various risk classification systems such as the operative link on intestinal metaplasia assessment (OLGIM) classification and MAPS guideline recommendations was evaluated. We further aimed to assess the potential additional value of serological markers like pepsinogens (PG) and gastrin on risk stratification.
Methods
Patient selection
This prospective study was performed in six hospitals (one academic, five regional) in the Netherlands, and one regional hospital in Norway. Initial results of the study in 140 patients have been published before.9 Patients were eligible for inclusion if they were over 18 years of age and had a previous diagnosis of AG, IM and/or dysplasia of the gastric mucosa. They were identified in the histopathology database of each hospital and selected from the outpatient clinic. Patients were excluded from participation if they had previously undergone upper gastrointestinal surgery, were previously diagnosed with gastric carcinoma, or any other malignancy not being in remission, or if they had severe comorbidity limiting their expected survival to less than 2 years, portal hypertension or a proven CDH1 mutation.
Eligible patients were included after written informed consent. All patients underwent at least one surveillance endoscopy after the index endoscopy. Surveillance endoscopies were performed between April 2006 and January 2015. The institutional review boards of all participating hospitals approved the study.
Baseline data collection
Demographic details, including age, sex and ethnicity were registered for each patient. In addition, all patients were asked to complete a structured questionnaire including several items on lifestyle factors, medical history, medication use and family history of gastric cancer.
Endoscopy procedures at baseline and during follow-up
All endoscopies were done using a standard forward-viewing videogastroscope (HD 180 series). At index endoscopy, biopsies had been taking using the local protocol, with targeted biopsies of visible lesions and non-targeted biopsies from the antrum and/or corpus.
At the surveillance endoscopy, random biopsies were taken according to a standardised biopsy protocol from five standardised intragastric locations for histological assessment of the severity and distribution of premalignant gastric lesions.11 12 Four biopsies were taken from the antrum, two from the angulus, two from the corpus greater curvature, two from the corpus lesser curvature and two from the cardia. In case of endoscopic abnormalities or visible lesions in the stomach, targeted biopsies were obtained before random biopsies were taken according to the standardised protocol. The time interval between surveillance endoscopies was 2 years, except for cases with LGD/HGD. Those patients underwent an endoscopy within 1 year (LGD) or 6 months (HGD) if no visible lesion was observed. In case of a visible lesion, they underwent endoscopic resection as soon as possible.
Histological assessment of surveillance biopsies
All participating hospitals used the same histopathological protocol. Biopsy samples were fixed in formalin, embedded in paraffin blocks, cut into 5 µm sections, stained with H&E and processed for routine diagnosis. Pathologists from the participating hospitals assessed the biopsy samples of each intragastric location and scored them for presence of H. pylori, AG, IM and dysplasia. Although revision of histology before starting surveillance is not recommended by the MAPS guideline, a representative part (n=140) of all samples was reassessed by an expert pathologist, who was not aware of patient data, endoscopic findings, and the baseline and follow-up histological diagnoses of the general pathologist. If differences were observed, the expert score was used.
All specimens were scored according to the updated Sydney classification.13 In general, for every biopsy sample H. pylori density, acute inflammation (neutrophil infiltration), chronic inflammation (mononuclear infiltration), AG and IM were assessed (0=absent, 1=mild, 2=moderate, 3=marked). Dysplasia was scored according to the Vienna system, which includes LGD and HGD.14
The operative link on gastric intestinal metaplasia (OLGIM) system was used to evaluate the severity and distribution of IM throughout the stomach.15 This system combines the Sydney IM score of antrum and angulus, with the score of the corpus lesser and greater curvature, in order to classify patients into five stages (OLGIM 0 to IV).
H. pylori infection
All biopsies were checked for chronic active inflammation and H. pylori colonisation. If positive, patients were offered antibiotic treatment. All patients were asked by questionnaire for previous H. pylori infection and antibiotic treatment.
Follow-up
The MAPS guideline recommends no follow-up in patients with mild or moderate AG or IM limited to antrum, as these patients are thought to have a low risk for progression to invasive neoplasia.6 Only for patients with extended AG/IM (ie, antrum and corpus) surveillance is recommend. The gold standard for this phenotype is yet to be defined. We therefore looked for various ways to define the ‘premalignant stomach’: based on most advanced lesion, OLGIM stage (stage 0–II vs III–IV) or PG level. Subsequently, risk stratification was assessed considering the occurrence of invasive neoplasia during follow-up, in order to define the most optimum stratification method. In case of the OLGIM or MAPS based stratification, index endoscopy was defined as first endoscopy with biopsies from both antrum and corpus. To make all stratification methods comparable with each other (ie, based on the same patients), we chose to stratify only those patients who underwent at least two surveillance endoscopies.
Disease progression was defined as more advanced histology compared with the prior endoscopic evaluation. Regression was defined as the opposite, meaning that histopathology of surveillance biopsies showed less advanced histology. Progression to HGD/invasive neoplasia was defined as neoplastic progression. The neoplastic progression rate was defined as the proportion (%) of neoplastic progression per year. Patients were discharged from surveillance if two surveillance endoscopies confirmed low-risk disease.
Serological determinants
Fasting blood samples were taken at the time of first surveillance endoscopy. Serum samples were stored at −80°C until use for analyses. Serological testing of PGs I and II, gastrin-17 (G-17) and H. pylori antibodies was performed by commercial ELISA tests (GastroPanel, Biohit, Helsinki, Finland). All tests were performed according to the manufacturer’s guideline.
Statistical analyses
Continuous variables were reported as mean with SD or median with 25th and 75th percentiles or range. Categorical variables were reported as counts and percentages. χ2 test was applied to compare HGD/invasive neoplasia development between patients categorised at low and high risk. Analyses of variance were used to compare means of serological markers between MAPS risk groups and OLGIM stages. Two-sided p-values<0.05 were considered statistically significant. Analyses were performed using SPSS V.23.
Results
Baseline characteristics
In total, 295 patients consented for surveillance (figure 1). After reassessment of their baseline histology, 11 subjects (4%) had to be excluded because no premalignant lesions were observed. Four patients did not yet underwent first surveillance endoscopy, and one patient was excluded because of reaching endpoint at index endoscopy, leaving a study population with follow-up data of 279 patients. Main baseline characteristics are summarised in table 1. The median age at baseline was 58 years (range 14–79 years). At index endoscopy, 4% of patients was diagnosed with AG, 87% with IM and 9% with dysplasia as most severe lesion. Histology showed H. pylori infection in 70 patients (26%). In 21 patients (8%) targeted biopsies from visible lesions were obtained. These lesions were located in antrum (n=12), corpus (n=6), angulus (n=1), cardia (n=1), with missing location information for the remainder (n=2). Histopathology of these visible lesions showed gastritis or no abnormalities in eight patients, IM in 10 patients and LGD in three patients.
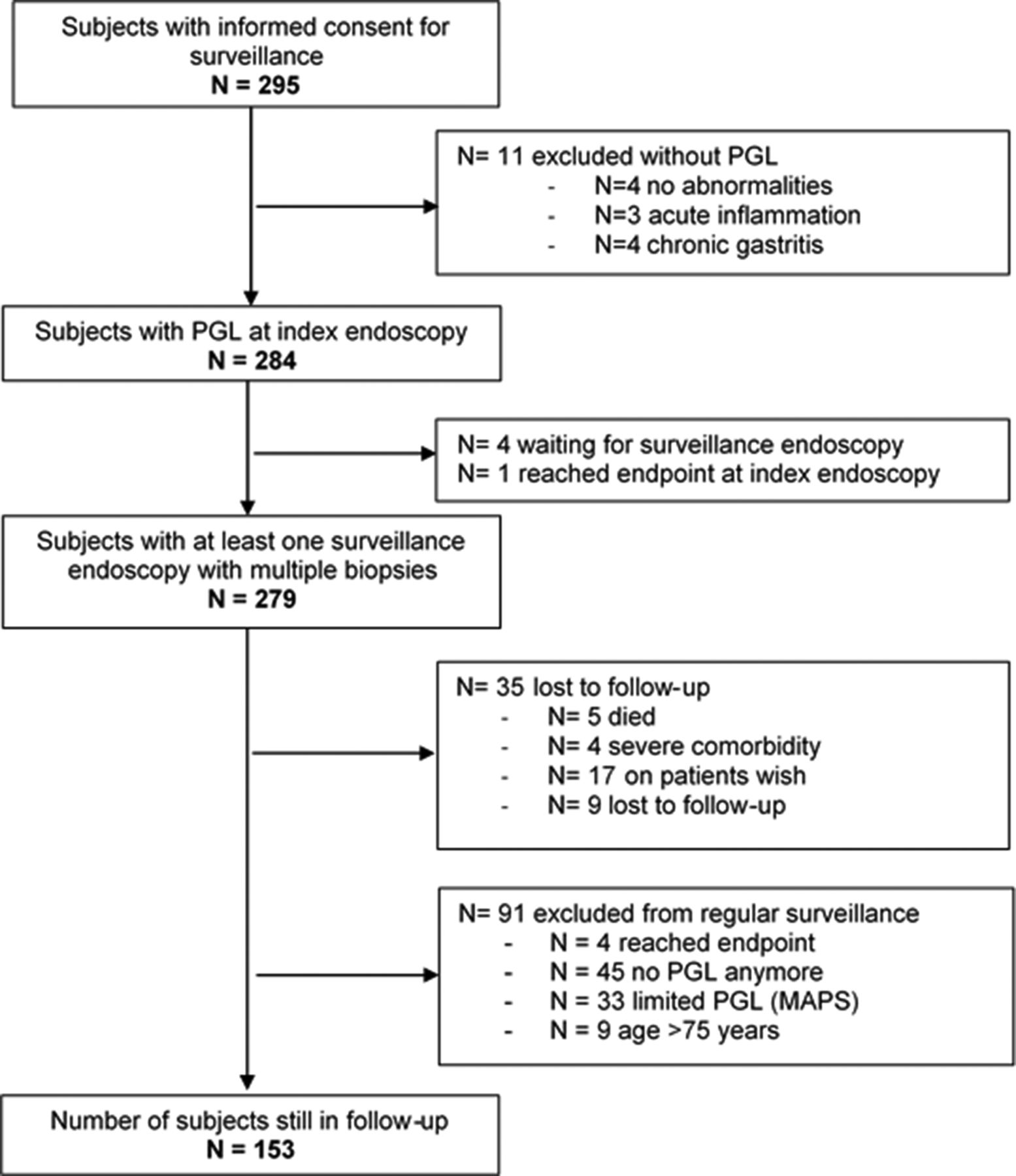
Study flow chart. MAPS, MAnagement of Precancerous conditions and lesions of the Stomach; PGL, premalignant gastric lesion.
Baseline characteristics of 279 patients with premalignant gastric lesions
OLGIM stage at index endoscopy was available for 190 patients (stage 0: n=11; stage I: n=66; stage II: n=58; stage III: n=38; stage IV: n=17; table 1).
Serological markers: PGs, gastrin and H. pylori
During follow-up, serum samples were obtained from 236 patients (85%). Because of insufficient amount of sera, PGs could not be measured in two patients (0.8%). In 61 patients (26%), all biomarkers tests were normal. H. pylori serology was positive in 121 patients (51%). At the time of blood sample collection, only 19 patients were persistently H. pylori positive based on histology. This means that the majority of formerly H. pylori-positive patients had successfully undergone eradication treatment before the time of PG measurement. Although the exact year of eradication was not known for all patients, it was at least 1 year before PG measurement, given the mean time of 35 months between index and first surveillance endoscopy. According to the manufacturers’ references, antral AG was diagnosed in 20 patients (8.5%%), while AG limited to the corpus was diagnosed in 38 (16%) patients. In only one patient an atrophic pangastritis was observed (0.4%) (see also online supplementary table 1). Serological markers with their corresponding OLGIM stage are depicted in figure 2. Mean serological levels of PGI, PGI/PGII and G-17 differed significantly between OLGIM categories but were not consistently correlated with an increase in OLGIM stage.
Supplementary file 1

{kind=link}
{kind=link}
Mean serology markers divided by OLGIM stage. These plots show the mean serological levels with their 95% CI. Data were available for 235 patients, who were divided by OLGIM stage (stage 0: n=85, stage I: n=35, stage II: n=61, stage III: n=42, stage IV: n=12). OLGIM, operative link on intestinal metaplasia.
Progression and regression according to most severe lesion
Two-hundred and seventy-nine patients underwent at least one surveillance endoscopy. The first surveillance endoscopy was performed after a mean interval of 35 months (SD 28.8). In total, 814 endoscopies (average 2.9 per patient, range 1–7) were performed within a mean follow-up time of 57.1 months (SD 35.5) and a total of 1312 patient-years.
Table 2 shows the progression and regression by means of most severe gastric lesions at index endoscopy compared with the last performed surveillance endoscopy. Progression occurred in 11 patients (4%). Progression to a visible dysplastic or invasive neoplasia lesion was observed in four patients (1.4%). This equals one case of progression to neoplasia per 328 patient-years. Three of these four patients had been diagnosed with IM at index endoscopy, and one with HGD (down staged to severe IM at first surveillance endoscopy). Three patients (1.1%) progressed to LGD, which equals one new case per 437 patient-years. In 165 patients (59%), no progression nor regression was found. Histology in these patients revealed IM in 98.2% of patients, AG in 1.2% and LGD in 0.6% of patients. Regression was observed in 103 patients (37%). Twenty-two patients diagnosed with LGD at index endoscopy regressed to IM (73%), AG (5%) or gastritis/normal histopathology (23%). Eight of them (36%) had positive H. pylori histology and/or positive serology. Twenty-seven (32%) patients with IM at index endoscopy regressed to AG (13%), gastritis (40%) and normal histopathology (47%). Four (36%) patients with AG regressed to a lower stage: gastritis (25%) and normal histopathology (75%). No regression was observed in cases with HGD at baseline.
Regression and progression of premalignant gastric lesions in terms of most severe lesion
Table 1 shows the number of H. pylori-positive patients at baseline (n=70, 26%). During follow-up, 57 patients (81%) were eradicated successfully, leaving 12 (18%) patients with persistent H. pylori infection and n=1 with no follow-up data (1%). A total of 5 (8.8%) patients who were eradicated successfully showed progression of most severe lesion, compared with none of the patients with persistent H. pylori infection (p=0.29).
Progression and regression according to OLGIM stage
To assess OLGIM stages over time, only patients with a next surveillance endoscopy after first OLGIM evaluation could be included (n=211). The results between index and last surveillance endoscopy according to the OLGIM stages are shown in table 3. This comparison revealed regression to a lower OLGIM stage in 42% of the cases after a mean follow-up time of 50.8 months (SD 32). In 35% of the patients, the OLGIM did not change over time, whereas progression was observed in 23%. Online supplementary table 3 shows the comparison of OLGIM stage between index and first surveillance endoscopy.
OLGIM stage at index and last surveillance endoscopy
Risk stratification methods of the premalignant stomach and neoplastic progression during follow-up
Based on biopsies
In total 211 patients (76%) were eligible for risk stratification based on biopsies from both antrum and corpus, according to the the MAPS guideline: low risk was defined as AG/IM limited to antrum, and high risk as AG/IM in both antrum and corpus. In our cohort, 86 patients (41%) were categorised as low risk, and 125 (59%) as high risk. Their overall mean follow-up time was 50.8 months (SD 32). Table 4 shows the regression and progression rate of both groups. Progression was observed in 16% of the low-risk group compared with 2% in the high-risk group (p<0.001). One patient of the low-risk group was diagnosed with invasive neoplasia, compared with two patients of the high-risk group (p=0.79). One out of the four cases who progressed to HGD/invasive neoplasia could not be included in above descriptive comparison as endpoint was reached at first surveillance endoscopy.
Regression and progression according to histology-based risk stratification
Based on biopsies and serology
When patients were divided into low-risk and high-risk groups based on a combination of histological and serological results, no patients in the low-risk group progressed to HGD/invasive neoplasia, compared with three patients in the high-risk group (p=0.49) (table 5).
Histological and serological based risk stratification and detection of HDG/gastric cancer during follow-up
Based on OLGIM stage
Low-risk patients for neoplastic progression were defined by OLGIM stage 0–II (n=155), while high-risk patients had OLGIM stage III–IV (n=56). Neoplastic progression occurred in one patient (0.6%) of the low-risk group and in two patients of the high-risk group (3.6%) (p=0.11).
Based on OLGIM stage and PGs
Patients with PGI/PGII ratio ≤3 were added to the high-risk group, consisting of patients with OLGIM III–IV. In total, the low-risk group (ie, OLGIM 0–II and normal PGI/II) consisted of n=132, compared with n=79 in the high-risk group. During follow-up, no patients (0%) in the low-risk group and three patients (3.8%) in the high-risk group had neoplastic progression (p=0.02) (table 6, online supplementary figure 1).
Risk stratification and detection of HDG/gastric cancer during follow-up based on OLGIM and PGI/PGII ratio
HGD/invasive neoplasia: characteristics and neoplastic progression rate
During follow-up, four patients (1.4%) were diagnosed with HGD/invasive neoplasia. Given the mean follow-up time of 57 months (SD 35) or 4.75 years (SD 2.9), the neoplastic progression rate per year is 0.3% (95% CI 0.08 to 0.76). Table 7 summarises these patients. OLGIM stage at index endoscopy varied between stages I and IV. When using the operative link on gastritis assessment (OLGA) system, all four cases had a low stage at baseline: three patients with OLGA stage 0 and one patient with OLGA stage I (see table 6 and online supplementary table 2). Two patients underwent successful endoscopic submucosal dissection (ESD) of the lesion, with a complete resection specimen. One patient died 8 months after ESD, which appeared not to be related to gastric cancer or ESD (ruptured iliac artery aneurysm). Total gastrectomy was performed in two patients. One of them died 3 months postoperative due to septic shock based on massive intestinal ischaemia and perforation.
Description of the location, OLGIM stage and management of all cases with HGD/gastric cancer
Histology of the resected specimens showed HGD without infiltrative growth, two invasive neoplasia and one diffuse type gastric cancer with signet cells. Histology of surrounding tissue of the lesion (assessed after surgery or ESD) showed IM in all specimens, except for the diffuse type carcinoma.
Discussion
Although the incidence of gastric cancer strongly declined in most Western countries over the past 80 years, it remains a relatively common malignancy with marked differences in prevalence between population subgroups. We have over the years come to understand risk factors for progression. Two recent guidelines thus recommended surveillance of patients at highest risk.6 16 These recommendations need to be substantiated by data from prospective cohort studies assessing the incidence of disease progression and the performance of various methods available for risk categorisation. This multicentre prospective cohort study showed stable disease in the majority of patients during an average 4.7 years of follow-up. In total, four cases (1.4%) showed neoplastic progression and were diagnosed with early potentially curable HGD/invasive neoplasia during follow-up. One out of these four patients was diagnosed with diffuse type gastric cancer, which is not correlated with the Correa cascade. Nevertheless, we consider this case as yield of the endoscopic surveillance. The neoplastic progression rate of 0.3% per year is in line with a previous large study from our group in which we included patients based on a histopathological diagnosis only, without any further information on staging and subgroups.17 Risk stratification based on histology only was not completely sufficient in discriminating low-risk from high-risk patients. This study was designed to give insight in outcome of gastric screening in a low-risk gastric cancer area rather than to draw conclusions on histological classification systems used. Neoplastic progression occurred in the same proportion of patients with low OLGIM grade (0–II) compared with high OLGIM grade (III–IV) measured at index endoscopy. It underlines the difficulty we still have in defining low-risk and high-risk patients for neoplastic progression. Preliminary results on the use of serological data combined with endoscopy results showed that this combined strategy might be of additional value in identifying the subgroup without neoplastic progression during follow-up.
The majority of patients with precursor lesions will never develop gastric cancer. Consequently, the yield of surveillance endoscopy in all patients with premalignant lesions is low. This phenomenon is also known for surveillance of Barrett’s oesophagus18 and colorectal surveillance after adenoma removal.19 Surveillance of all patients leads therefore to an unnecessary burden for patient and endoscopic resources. It is known that the gastric cancer risk increases with progression of the lesion according to the Correa cascade.17 20 The international MAPS consensus guideline therefore recommended endoscopic follow-up only for patients with marked AG and IM in both antrum and corpus, and for those with dysplasia.6 To our knowledge, we are the first to evaluate this approach in a prospective study.
The rate of neoplastic progression did not significantly differ between high-risk and low-risk patients, categorised according to histology only. One patient, categorised as not in need for endoscopic surveillance, developed a visible lesion with HGD that was successfully removed by ESD. Nevertheless, the majority of patients (85%) in this low-risk group had stable disease during follow-up. Long-term follow-up is necessary to confirm that indeed most patients will not develop gastric cancer in future. The same applies for the OLGIM classification, which has been shown as an accurate staging system for the extent and severity of IM.15 This staging system is comparable with the OLGA,21 but interobserver agreement for scoring IM was superior to AG (kappa 0.9 vs 0.6).15 High stages of OLGA and OLGIM are associated with a higher risk for progression to invasive neoplasia, and endoscopic surveillance may only be necessary in these patients.22 23 Nevertheless, two out of four patients who developed invasive neoplasia during follow-up had a low OLGIM stage (I–II) at index endoscopy. If using the OLGA classification, none of the cases with HGD/invasive neoplasia during follow-up had a high stage at index endoscopy. The right scoring of atrophy is more difficult than for IM, and therefore more susceptible to errors in the biopsy assessment. Given the good kappa for IM, we preferred to use the OLGIM classification, in terms of reliability and feasibility in daily practice. These results seem to indicate that a risk stratification tool solely based on histopathology might not be sufficient. Given the small number of cases and the limited follow-up of this study we acknowledge that a strong conclusion can only be made based on more cases and longer follow-up.
In our study, combining histopathology data with serological markers adequately discriminated between low-risk and high-risk patients. None of the patients with limited AG/IM (PGI/PGII>3 and OLGIM 0-II) developed HGD/invasive neoplasia during follow-up. PG I and II are proenzymes produced by the gastric mucosa, which can be used in the assessment of the functional status of gastric mucosa.24 A PGI/PGII ratio ≤3 is well related with corpus atrophy.25 26 Serum G-17 correlates with the functional status of gastric antral glands, and levels are reduced in case of severe antrum atrophy.24 A normal PGI/PGII ratio gives greater confidence in stopping endoscopic surveillance in patients with limited AG/IM. Serological tests are non-invasive for patients and its implementation in risk stratification and decision-making on endoscopic surveillance could help reducing patient burden and the use of endoscopic resources.
Regression of histopathological findings was observed in about one-third of the patients. Remarkably, more than 90% of the cases with LDG at index endoscopy showed regression to less-advanced lesions during follow-up. This regression occurred after H. pylori eradication in some patients, but may in part also be related to sampling error. Regression may be considered as a reason for ending the endoscopic surveillance. In a large population-based cohort, no increased incidence for gastric cancer was found in patients with regression to less-advanced lesions after 10 years of follow-up, except patients with dysplasia at baseline.20 In our study, one patient had HGD at index endoscopy. We, however, chose to not exclude this case given the fact that this patient was downstaged to severe IM at first surveillance endoscopy. Endpoint was reached at second surveillance endoscopy, where we found invasive neoplasia of the angulus.
Our study has a limited follow-up time of 4.7 years. Gastric cancer development is usually a slowly ongoing process. This implies that patients at risk ideally should be followed longer. Another potential limitation is that we used regular white-light endoscopy. The use of image-enhanced endoscopy (like narrow band imaging, NBI) coupled with magnification is recommended, but still not routine practice in most countries.6 As such, our study reflects daily clinical practice. Most notably, our study is limited by the small number of patients with neoplastic progression. This is inherent to the geographical setting of the study as both the Netherlands and Norway represent low incidence regions for gastric cancer, with a declining incidence of premalignant gastric lesions observed in the Netherlands.8 The number of four cases with HGD/invasive neoplasia allowed to use descriptive statistics only. Not all biopsy samples were reassessed by an expert pathologist, which may have resulted in histological misclassification. Nevertheless, we have confidence that misclassification is not very likely given the high interobserver agreement we observed for internal metaplasia (k=0.81) and the majority of patients (88%) having IM at index endoscopy.
In conclusion, this multicentre prospective cohort study in a low gastric cancer area showed that with a surveillance programme for premalignant gastric lesions, gastric cancer can be detected at an early curable stage with an overall risk of neoplastic progression of 0.3% per year. Risk stratification based on histopathology may result in excluding patients at risk for gastric cancer from follow-up. Adding serological markers as non-invasive tool can help to improve the identification of patients at risk for gastric cancer.
Acknowledgments
The authors wish to thank the Gastroenterology and Hepatology departments of the Sint Franciscus Hospital, Rotterdam; the Rijnstate Hospital, Arnhem; the IJsselland Hospital, Capelle aan den IJssel; the Deventer Hospital, Deventer; the Canisius-Wilhelmina Hospital, Nijmegen; and the Ålesund Hospital, Ålesund, Norway.
References
Footnotes
Contributors WJdH, ILH, CMdH, LGC, MD, EJK and MCWS contributed to the conception and design, acquisition of data, analyses and interpretation of the data, drafted the article, revised it critically for important intellectual content and gave final approval of the version to be published. TJT, M-PA, IP-B, EMW, FtB, GdH, MJB, MPP and WL contributed to the conception and design and acquisition of data, revised the article critically for important intellectual content and gave final approval of the version to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Ethics Review Board at the Erasmus University Medical Centre Rotterdam, The Netherlands.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note This work was part of a PhD thesis defended by the first author at the Erasmus University in Rotterdam on 14 September 2016.