Article Text

Abstract
Background Reported incidence rates of oesophageal adenocarcinoma (OAC) in Barrett's oesophagus (BO) vary widely. As the effectiveness of BO surveillance is crucially dependent on this rate, its clarification is essential.
Methods To estimate the rate of malignant progression in patients with BO, all patients with a first diagnosis of BO with no dysplasia (ND) or low-grade dysplasia (LGD) between 1991 and 2006 were identified in the Dutch nationwide registry of histopathology (PALGA). Follow-up data were evaluated up to November 2007.
Results 42 207 patients with BO were included; 4132 (8%) of them had LGD. Re-evaluation endoscopies at least 6 months after initial diagnosis were performed in 16 365 patients (39%), who were significantly younger than those not re-examined (58±13 vs 63±16 years, p<0.001). These patients were followed-up for a total of 78 131 person-years, during which 666 (4%) high-grade dysplasia (HGD)/OACs occurred, affecting 4% of the surveillance patient population (mean age: 69±12 years, 76% male). After excluding HGD/OAC cases detected within 1 year after BO diagnosis (n=212, 32%), incidence rates per 1000 person-years were 4.3 (95% CI 3.4 to 5.5) for OAC and 5.8 (95% CI 4.6 to 7.0) for HGD/OAC combined. Risk factors for HGD/OAC were increased age (eg, >75 years HR 12; 95% CI 8.0 to 18), male sex (2.01; 1.68 to 2.60) and presence of LGD at baseline (1.91; 1.53 to 2.40).
Conclusion In this largest reported cohort of unselected patients with BO, the annual risk of OAC was 0.4%. Male sex, older age and LGD at diagnosis are independent predictors of malignant progression, and should enable an improved risk assessment in BO.
- Barrett's carcinoma
- Barrett's oesophagus
- epidemiology
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Published estimates of the annual risk of cancer in patients with Barrett's oesophagus (BO) are highly heterogeneous.
As the effectiveness of BO surveillance is primarily dependent on this rate, its clarification is essential.
Large-scale and long-term follow-up studies of unselected patients with BO are lacking.
What are the new findings?
In this large nationwide cohort of unselected patients with histologically confirmed BO, the annual risk of oesophageal adenocarcinoma (OAC) was 0.4%.
The annual OAC risk decreased to 0.14%, in case cancer risk for all BO patients was analysed, regardless of whether surveillance endoscopy was performed.
Male sex, older age and low-grade dysplasia at initial diagnosis of BO are independent predictors of malignant progression.
Introduction
Barrett's oesophagus (BO) is an acquired condition, in which the squamous epithelium lining the distal oesophagus is replaced by columnar intestinal-type mucosa.1 It is considered to be a complication of longstanding gastro-oesophageal reflux and constitutes the prime risk factor for oesophageal adenocarcinoma (OAC).2 3 OAC usually has a poor prognosis, with a 5-year survival rate of <15%.4 Hence, in order to detect early-stage cancers suitable for curative treatment, surveillance endoscopy of patients with BO is advised, at intervals dictated by the absence or presence and grade of dysplasia.5
The effectiveness of surveillance of BO is, however, equivocal. Increased survival has been observed in patients with OAC enrolled in BO surveillance programmes. This may have resulted from early detection of cancers. On the other hand, this effect may also have resulted from lead-time bias, as, in particular, young patients without concomitant diseases were included in surveillance programmes.6–11 In addition, most patients with BO die from unrelated causes, as according to a cohort follow-up study from our department only 5.6% of total mortality in BO patients was related to OAC.10 Moreover, some patients may not be fit for surgery even if OAC is detected at an early stage.12 13
A primary determinant of cost-effectiveness of BO surveillance strategies is the risk of BO progressing to OAC.14–16 Unfortunately, published estimates of the annual risk of cancer in patients with BO are highly heterogeneous, ranging from 0% to 2.9% per annum.17 These estimates were based primarily on patients referred to tertiary centres, whose cancer risk may exceed that for patients managed by non-referral centres. Moreover, published data predominantly come from small retrospective cohort studies with relatively short follow-up, showing higher cancer incidence than may be observed in larger surveillance studies. Consequently, US investigators reported evidence of publication bias in surveillance studies, favouring publication of small studies with high cancer incidence rates.18
As a result of the low degree of ascertainment of BO in the general population,19 20 there is a lack of both large-scale and long-term follow-up studies of patients with BO, providing more reliable risk estimates for malignant progression. Such studies are essential, both in re-appraising the potential value of surveillance endoscopy for patients with BO and in optimising the recommended follow-up intervals. We therefore estimated the progression rate of BO to high-grade dysplasia (HGD) and OAC in a nationwide cohort of patients with BO in The Netherlands, and assessed the value of the factors age, sex and initial histology as predictors of malignant progression in BO.
Methods
Histopathology database
In The Netherlands all histopathology and cytopathology reports are collected in a national archive (PALGA database), which encompasses all 64 pathology laboratories in The Netherlands. Since 1991, PALGA has had nationwide coverage and currently contains ∼42 million excerpts from nearly 10 million patients.21 Every excerpt in the database contains encrypted patient identification, a part of the summary of the original pathology report and diagnostic codes similar to the Systematised Nomenclature of Medicine (SNOMED) issued by the College of American Pathologists.22 This diagnostic code contains a topological term, the type of sample, and a morphological term describing the finding, for example ‘oesophagus*biopsy*intestinal metaplasia’. The SNOMED morphology codes are identical to the codes in the International Classification of Diseases for Oncology (ICD-O-2; WHO).23 Details with regard to the number and intraoesophageal location of biopsies, or information on the indication for performing an endoscopic procedure, are not uniformly registered. Each pathology report can, however, be traced to an individual patient with a unique identifier, allowing follow-up of subsequent histology, irrespective of where subsequent biopsies were taken or resections were performed.24 For each report, gender, date of birth, date of pathology review, summary text and diagnostic codes were made available. It was not, however, possible to access additional clinical data. The present study was based on data recorded in the PALGA database between 1991 and 2007.
Data collection
All patients registered in the database between 1991 and 2006 with an initial, histological diagnosis of BO with no baseline dysplasia (ND), or maximally low-grade dysplasia (LGD), were identified.25 BO was defined as the presence of intestinal metaplasia in oesophageal biopsies. Codes that were used for identification of our patient cohort were (1) a combination of ‘oesophagus’ (T62000) and ‘intestinal metaplasia’ (M73320) or (2) ‘Barrett's metaplasia’ (T62310M73330) (see appendix). To validate the accuracy of the latter code, we manually reviewed the summary text of a random sample of 700 pathology reports that were coded as ‘Barrett's metaplasia’, and examined whether the presence of intestinal metaplasia or goblet cells was mentioned. In only 16 of 700 reports (2.3%) were these terms not specifically mentioned. However, in seven of these patients, the presence of intestinal metaplasia could be confirmed in a follow-up pathology report.
Patients with a baseline diagnosis of HGD in BO were excluded, as were patients with either gastric or oesophageal surgery or malignancy, registered prior to, or simultaneously with, the first diagnosis of BO.
For each patient admitted to the cohort, all pathology excerpts concerning oesophageal biopsies from the first diagnosis of BO to the end of the study period (November 2007) were retrieved. Follow-up excerpts were scrutinised for codes indicating HGD and/or OAC. Where present, the pathology reports of the surgical resection specimens were reviewed; only carcinomas of which the bulk was macroscopically located above the gastro-oesophageal junction and those clearly originating from BO were diagnosed as OAC.26 27
Data analysis
Person-years of follow-up were calculated for each member of the cohort. Here we distinguished between patients who underwent one or more re-evaluation endoscopies with biopsy sampling and patients without further histology after BO diagnosis. The former group was censored at the date of either HGD or OAC diagnosis or of last patient contact with biopsy sampling, the latter at date of death. The date of death of patients registered in the PALGA database is, however, not uniformly recorded, unless an autopsy has been performed, reports of which are also registered in the system, but are fairly rare in The Netherlands. Therefore, for the latter cohort, censoring was imputed to evaluate the number of person-years at risk, as they were unlikely to have developed symptomatic OAC throughout the study period. As the ascertainment of symptomatic OAC in The Netherlands is presumed to be very high,28 the disease practically always results in histological analysis, which is registered in the PALGA archive. Survival data from the general Dutch population were collected, starting from age and gender of the patients, and calendar year (Dutch Cancer Registry 2007). A data set with an approximately unbiased number of person-years at risk was subsequently created, by drawing from a binomial distribution for every year, as was done previously.29 30 Multiple imputation did not significantly change the results. Finally, imputed survival estimates were corrected for an assumed 16% risk of excess mortality in patients with BO, based on previous reports.31
Within the first analysis, OAC risk and combined HGD/OAC risk were calculated for those patients with actual documented follow-up in the PALGA registry. Within the second analysis, OAC risk was calculated for the whole cohort of patients, including those who did not receive one or more follow-up endoscopies with biopsies after initial BO diagnosis. Additional analyses of OAC risk based on survival estimates for the general Dutch population without a correction for an assumed mortality excess in patients with BO were also performed. To avoid misclassification of prevalent cases of HGD/OAC, only those cases that were detected at least 1 year after initial BO diagnosis were included in cancer risk analysis. Crude OAC and combined HGD/OAC incidence rates are presented as number of cases per 1000 patient-years of follow-up. Kaplan–Meier survival analysis was performed to evaluate the interval between initial BO diagnosis and occurrence of HGD/OAC. Survival curves for patients with BO without baseline dysplasia were compared with those with baseline LGD, using the log-rank test, at the p<0.05 level of significance. Cox regression analyses were performed to identify independent risk factors for progression of BO to HGD/OAC. Estimates of relative risks are expressed as HRs with 95% CIs. Statistical analyses were conducted using S-PLUS (S-PLUS 6.0; Insightful, Seattle, Washington, USA) and SPSS software (SPSS 16.0; SPSS, Chicago, Illinois, USA).
Results
Study cohort
In total, 42 207 patients with a first diagnosis of BO were identified in the PALGA database, with a 1.0/0.6 male to female ratio (table 1). Of those, 4132 (9.8%) were classified with LGD at baseline. Patients with LGD were significantly older than patients without dysplasia (mean age±SD: 64±14 vs 61±15 years, p<0.001) and more often male (63% vs 61%, p=0.003). In addition, men were also significantly younger than women at initial diagnosis of BO without dysplasia (58±15 vs 65±15 years, p<0.001) and BO with LGD (61±14 vs 67±13 years, p<0.001).
Baseline characteristics of the study population
Follow-up endoscopies with biopsy sampling
Follow-up upper gastrointestinal endoscopy with biopsy sampling, at least 6 months after the initial diagnosis, was performed in 16 365 patients with BO (39%). Mean length of total follow-up in these patients was 4.8 years (SD 3), for a total of 78 131 patient-years. In total, 43 568 re-evaluation endoscopies were performed, with an average of 3 (range 1–22) endoscopies per patient. Patients with histological follow-up were significantly younger than those not undergoing follow-up (58±13 vs 63±16 years, p<0.001), and more often male (65% vs 59%, p<0.001). Only 38% of patients without dysplasia at baseline underwent at least one histological follow-up, as compared with 52% after a diagnosis of baseline LGD (p<0.001). The mean interval between initial and follow-up endoscopy was 2.0±2 years for patients with BO without baseline dysplasia and 1.4±2 years for those with LGD at baseline (p<0.001).
Diagnosis of HGD and/or OAC
Malignant progression was observed in 666 (1.6%) patients (HGD, 161; OAC, 505). Five additional patients were diagnosed with an adenocarcinoma of which the bulk was located below the gastro-oesophageal junction. These cases were excluded from the analysis. Mean age of patients at HGD/OAC development was 69.0 years (SD 12), and the majority of HGD/OACs occurred in males (76%). Male patients were significantly younger at diagnosis of HGD/OAC than females (67±11 vs 74±11, p<0.001). This overall male predominance gradually disappeared with increasing age, as the rise in incidence rate of HGD/OAC in males levelled off over age 85, whereas in women, especially in those aged >85, it continued to rise with age (figures 1 and 2).

Age distribution of 666 detected cases of high-grade dysplasia (HGD)/oesophageal adenocarcinoma (OAC) in 42 207 patients with Barrett's oesophagus during the study period January 1991 to November 2007.

Age-specific incidence rates of high-grade dysplasia (HGD)/oesophageal adenocarcinoma (OAC) for males and females with a first diagnosis of Barrett's oesophagus (BO).
Risk of HGD and/or OAC
The distribution of detected HGD/OAC cases in relation to the duration of follow-up is shown in figure 3. During the study period, 180 (0.4%) patients with BO developed HGD/OAC within 6 months, and 32 patients (0.08%) within the subsequent 6 months after BO diagnosis. Another 215 patients (0.5%) progressed to HGD/OAC between the second and fifth year after BO diagnosis, and the remaining 239 (0.6%) patients after 5 years. In the majority (n=357, 54%) of patients with malignant progression, HGD/OAC was already detected at the second endoscopy. In 53% of these patients, this second investigation with biopsy sampling was performed after >1 year following initial BO diagnosis, and in 21% after >5 years. The remaining 309 (46%) patients with malignant progression underwent one or more surveillance endoscopies with biopsies yielding negative for HGD/OAC, before being diagnosed with HGD/OAC. Patients with prior negative endoscopies were significantly younger at BO diagnosis than those in whom HGD/OAC was diagnosed at the second endoscopy (60±12 vs 67±11, p<0.001). Furthermore, the mean latent period from BO to HGD/OAC was significantly longer in those with prior intermittent endoscopies as compared with those without (7.0±4 vs 2.5±3, p<0.001).
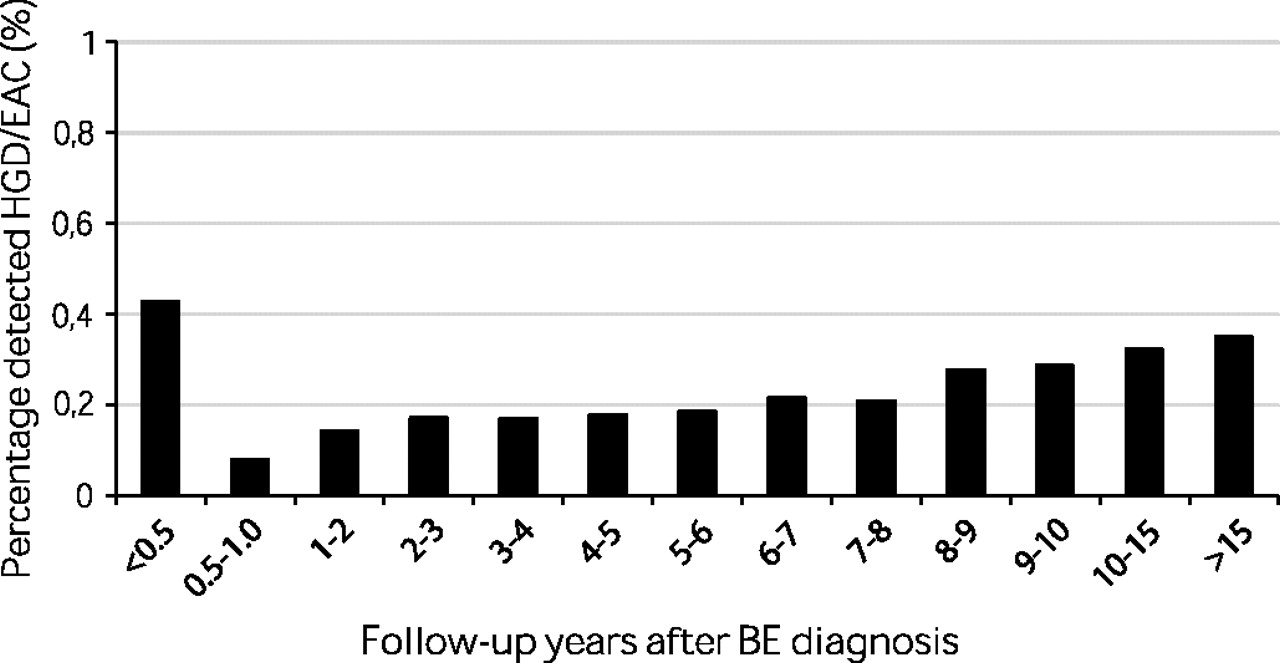
Time distribution of 666 detected cases of high-grade dysplasia (HGD)/oesophageal adenocarcinoma (OAC) in 42 207 patients with Barrett's oesophagus (BO) during the study period January 1991 to November 2007. (Number of cases relative to number of patients with BO (%) with corresponding years of follow-up.)
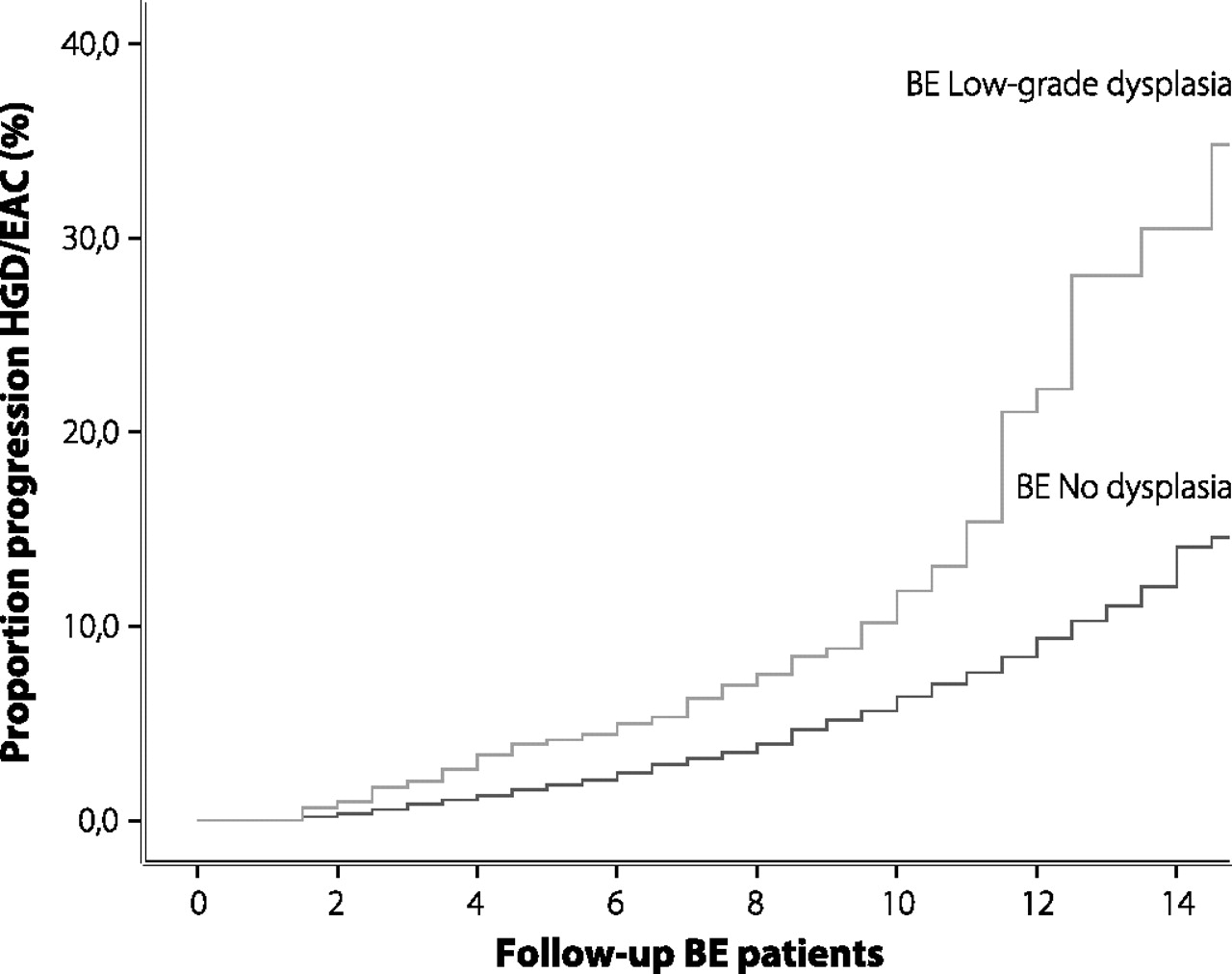
After excluding prevalent cases of HGD/OAC (detection <1 year after BO diagnosis), crude OAC and combined HGD/OAC incidence rates among 16 333 patients with BO with at least one re-evaluation endoscopy were calculated, on the basis of a total of 78 105 patient-years of follow-up (table 2). Overall incidence rates per 1000 patient-years at risk were 4.3 (95% CI 3.4 to 5.5) for OAC and 5.8 (95% CI 4.6 to 7.2) for HGD/OAC combined. Survival curves for patients with BO (n=16 333) with or without baseline LGD are shown in figure 4. Within 2, 5 and 10 years of follow-up after initial diagnosis, HGD/OAC was diagnosed in 1, 2 and 6%, respectively of patients with BO without baseline dysplasia, and in 2, 4 and 13%, respectively, of patients with BO with baseline LGD (p<0.001) (figure 4). Men with baseline LGD experienced a faster progression to HGD/OAC as compared with women (both p<0.001). The same difference was observed between men and women without baseline dysplasia (p<0.001).
Crude incidence rates of OAC and combined HGD/OAC in patients with BO (n=16 333)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Progression rate to high-grade dysplasia (HGD)/oesophageal adenocarcinoma (OAC) in 16 333 patients with Barrett's oesophagus.
For patients who did not undergo re-evaluation and were unlikely to have developed symptomatic OAC throughout the study period, life expectancy based on general survival data of the Dutch population was imputed. This rendered a total follow-up of 234 821 patient-years for the whole cohort of 42 207 patients with BO. Overall incidence rates of OAC per 1000 patient-years were 1.4 (95% CI 1.2 to 1.6) for both sexes combined, 1.9 (95% CI 1.7 to 2.1) for males and 0.8 (95% CI 0.7 to 1.0) for females. For patients with BO with baseline LGD, the OAC incidence rate rose to 3.6 per 1000 patient-years (95% CI 2.5 to 4.2) versus 1.2 (95% CI 1.1 to 1.5) for those without baseline dysplasia (p<0.05). Additional analyses of annual OAC risk based on survival estimates for the general Dutch population without a correction for an assumed mortality excess in patients with BO did not significantly alter the results.
Risk factors for malignant progression
Multivariate Cox regression analysis showed that male sex was independently associated with an increased risk of progression to HGD/OAC (HR 2.12, 95% CI 1.70 to 2.65) (table 3). In addition, older age as well as the presence of LGD at initial BO diagnosis were independently associated with development of HGD/OAC.
Risk factors for malignant progression in Barrett's oesophagus (n=16 333)
Discussion
In this, to our knowledge, largest reported cohort of patients with BO, the overall annual risk of cancer in BO was 0.4% (95% CI 0.3 to 0.6), and the annual risk of cancer and HGD combined only 0.6% (95% CI 0.5 to 0.7). These figures are lower than previously published estimates.17 In fact, the annual cancer risk decreased to 0.14%, in case cancer risk for all BO patients was analysed, regardless of whether any follow-up was performed. Against this background, male sex, older age and LGD at initial BO diagnosis were identified as independent predictors for malignant progression.
To date, there have been four published systematic reviews on the incidence of cancer in BO.17 18 32 33 Our finding of an annual cancer risk of 0.4% in BO is lower than those reported in these studies. Several explanations may account for this discrepancy. First, the population of our BO cohort consisted of a large number of unselected patients with BO with long-term follow-up, from all hospitals in The Netherlands. Our cohort therefore reflects daily clinical ascertainment and management of BO. This nationwide registry minimises selection bias, which is a particular drawback of small retrospective studies. This obviously differs from previous studies describing referral-based cohorts and from small studies with short follow-up, which may have included a biased selection of patients with BO with high cancer risk. For instance, only three studies with >1000 patient-years of follow-up were included in a review from the USA.18 A large study size results in lower reported cancer risks, as was also previously demonstrated in two systematic reviews.17 33 Another explanation for variations in outcome can be found in our strict exclusion of HGD and OAC cases occurring within the first year after initial BO diagnosis, and the exclusion of patients with BO with HGD at baseline. Only two reviews excluded incident cancers occurring within the first year after initial BO diagnosis.17 33 The inclusion of prevalent cancers will obviously inflate cancer risk for patients with uncomplicated BO. In the most recently published review, annual cancer incidence decreased to 0.41%, after limiting the analysis to the occurrence of only incident cancers, which is in line with our estimate of annual cancer risk.33
Several authors have used mathematical models to explore the cost-effectiveness of BO surveillance.14–16 US researchers concluded that, for a cancer risk of 0.5% per annum, surveillance every 4 years was indicated and, if the annual risk was 0.4%, surveillance every 5 years was the only strategy that increased quality of life.16 Others reported that screening 50-year-old men with gastro-oesophageal reflux disease (GORD), followed by surveillance of those with dysplasia only, is probably cost-effective, but that surveillance of BO, even at 5-yearly intervals, is very expensive even though more quality-adjusted life years (QALYs) may be gained.15 According to a British study using an economic model, an annual cancer risk of 0.5% would mean that surveillance conferred less benefit and more costs than no surveillance at all, irrespective of the surveillance interval used.14 The overall annual cancer risk obtained from our study is even lower than those incorporated in these models, especially with regard to the annual cancer risk of the whole cohort of patients with BO (0.14%), including those who did not receive any histological follow-up, and who did not in all probability develop symptomatic OAC. Our findings indicate that both quality of life benefit and cost-effectiveness of surveillance of BO are highly questionable unless it can be targeted at those patients with BO who are at the highest risk of cancer.
Despite the development of new cancer biomarkers, the presence and grade of dysplasia in random oesophageal biopsies obtained at BO surveillance still remain the best indicators of cancer risk.34 This was confirmed in our study by the fact that, despite its generally criticized lack of reproducibility, the initial diagnosis of LGD by a large variety of pathologists proved to have been a predictor of a twofold increased risk of malignant progression as compared with patients with BO without dysplasia. This was consistent with other studies.35–41 It is likely that an even better accuracy of risk prediction may be achieved by a consensus LGD diagnosis of more than one pathologist.37 40 In addition, the extent of the spread of LGD has been suggested to be another significant risk factor for the development of OAC.42
Male sex and older age at initial diagnosis were identified as other important independent risk factors for progression to HGD/OAC. Moreover, men showed a significantly faster progression of BO to HGD/OAC as compared with women (p<0.001). This observation remained unchanged after stratifying patients by age. In addition, BO was diagnosed at a significantly older age in women. These findings are in agreement with others,35 43–50 and are in accordance with the male predominance in OAC incidence, as we have demonstrated previously.44 51 52 This is compatible with the concept of women entering the carcinogenic cascade at an older age,53 54 and suggests that women progress less rapidly through subsequent stages of LGD and HGD. This observation has also been made in a recent study from Scotland.55 However, currently, age and gender have not been routinely included in planning BO surveillance programmes.
Some limitations of our study warrant consideration. First, as both sampling error and interobserver variability in the interpretation of dysplasia between non-expert and expert gastrointestinal pathologists exist,56 misclassification of baseline dysplasia status in our patients could have influenced our results. Nevertheless, differential misclassification to absence of baseline dysplasia would bias the difference between non-dysplastic and dysplastic patients with BO towards the null value, thereby underestimating rather than overestimating cancer risk in patients with BO with baseline LGD without affecting the overall cancer risk. In addition, overclassification of BO by community pathologists could have led to underestimation of reported cancer risks. However, reproducibility of intestinal metaplasia is high, with agreement rates between community pathologists of up to 88%.57 Secondly, some patients with intestinal metaplasia of the cardia could have been misclassified as having BO in our cohort, as endoscopic data were not available. We believe, however, that such misclassifications would only have played a minor role, as only pathology excerpts specifically reporting Barrett's epithelium in oesophageal biopsies were included. In addition, obtaining biopsy specimens from the gastric cardia is not routine practice during oesophagogastroduodenoscopy or in the diagnosis of BO in The Netherlands. Thirdly, as data on the length of the Barrett's segment, presence of hiatal hernia, presence of oesophagitis, body mass index and use of selected medications were not available, cancer risk could not be stratified for these factors. Unfortunately, it was also impossible to collect information with regard to the indication of performing re-evaluation endoscopies in these patients. As a result, no clear distinction could be made between patients participating in a surveillance programme and those undergoing re-evaluation endoscopies for investigation of symptoms. This could have led to an underestimation of our reported annual risk of cancer and HGD combined, as asymptomatic HGD cases might have been overlooked in this cohort. Nevertheless, we think that this has had only little influence on our findings, as a recent systematic review reported an incidence rate of cancer and HGD combined of 7.7 per 1000 person-years, which is only slightly higher compared with our findings.33 Fourthly, we could not provide data on the stage of cancers diagnosed in our cohort, as these data are not uniformly registered in the database. The younger age at diagnosis of cancer within the group receiving follow-up as compared with the group without follow-up suggests the detection of cancers at an earlier stage. In addition, we could not investigate the effect of the migration rate on our results. As the migration out of The Netherlands during the study period was small, with an average of 0.6% of the population annually, and there has been a predominant migration of populations with similar oesophageal cancer rates towards The Netherlands, we expect that these rates have only marginally affected the reported cancer rates. Finally, in order to calculate progression rates to OAC for the whole cohort of patients, a virtual life expectancy was calculated for all patients without follow-up until November 2007, based on the life expectancy of the general population. This assumption may have led to a slight underestimation of cancer risk, as there is conflicting evidence of increased co-morbidity and mortality in patients with BO as compared with the general population.8 9 31 58–60 However, as we assumed a high, 16%, increased risk of all-cause mortality in patients with BO, as reported by Cook et al,31 it is highly unlikely that this caused underestimation of our incidence rates.
In conclusion, in this large nationwide cohort of unselected patients with histologically confirmed BO, the annual risk of malignant progression was lower than previously reported. This further undermines the cost-effectiveness of generalised BO surveillance, from which an even smaller minority of patients than previously estimated is likely to benefit. However, we have demonstrated three independent predictors of neoplastic progression enabling tailoring of surveillance programmes towards a better selection of high-risk patients. Future large studies from other unselected populations should be performed to develop further risk stratification. A multicentre trial with randomisation of patients to varying surveillance intervals based on age, sex and the presence and grade of dysplasia is urgently needed.
Appendix
PALGA diagnosis codes used in the analysis:
Barrett's oesophagus: T62310M73330, M73320
Low-grade dysplasia: M74000, M74006, M74007
High-grade dysplasia and esophageal adenocarcinomas: M74008, M80003, M80011, M80101, M80102, M80103, M80104, M80105, M80123, M80193, M80203, M80213, M80413, M81403, M81404, M81453, M82003, M82113, M82603, M84303, M84803, M85603
PALGA terminology: http://www.palga.nl/palga/thesaurus.nsf
References
Footnotes
Competing interests GAM is a member of the executive board of the PALGA registry. The other authors have no conflict of interest to disclose.
Ethics approval This study was conducted with the approval of the Stichting PALGA.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Digest