Article Text

Abstract
Iron deficiency anaemia is one of the most common disorders in the world. Also, one third of inflammatory bowel disease (IBD) patients suffer from recurrent anaemia. Anaemia has significant impact on the quality of life of affected patients. Chronic fatigue, a frequent IBD symptom itself, is commonly caused by anaemia and may debilitate patients as much as abdominal pain or diarrhoea. Common therapeutic targets are the mechanisms behind anaemia of chronic disease and iron deficiency. It is our experience that virtually all patients with IBD associated anaemia can be successfully treated with a combination of iron sucrose and erythropoietin, which then may positively affect the misled immune response in IBD.
- IBD, inflammatory bowel disease
- ID, iron deficiency
- IDA, iron deficiency anaemia
- TPMT, thiopurine methyltransferase
- MCV, mean cell volume
- Epo, erythropoietin
- ACD, anaemia of chronic disease
- RBC, red blood cell
- NRAMP-1, natural resistance associated macrophage protein
- IFN-γ, interferon γ
- TNF-α, tumour necrosis factor α
- NO, nitric oxide
- RES, reticuloendothelial system
- inflammatory bowel diseases
- anaemia
- iron deficiency
- anaemia of chronic disease
- iron sucrose
- erythropoietin
Statistics from Altmetric.com
- IBD, inflammatory bowel disease
- ID, iron deficiency
- IDA, iron deficiency anaemia
- TPMT, thiopurine methyltransferase
- MCV, mean cell volume
- Epo, erythropoietin
- ACD, anaemia of chronic disease
- RBC, red blood cell
- NRAMP-1, natural resistance associated macrophage protein
- IFN-γ, interferon γ
- TNF-α, tumour necrosis factor α
- NO, nitric oxide
- RES, reticuloendothelial system
- inflammatory bowel diseases
- anaemia
- iron deficiency
- anaemia of chronic disease
- iron sucrose
- erythropoietin
SUMMARY
Iron deficiency anaemia is one of the most common disorders in the world. The World Health Organization estimates that more than 30% of the population have iron deficiency anaemia yet it remains an under managed feature of many gastroenterological conditions. Also, one third of inflammatory bowel disease (IBD) patients suffer from recurrent anaemia. Anaemia has significant impact on the quality of life of affected patients. Chronic fatigue, a frequent IBD symptom itself, is commonly caused by anaemia and may debilitate patients as much as abdominal pain or diarrhoea. Both iron deficiency and anaemia of chronic disease contribute most to the development of anaemia in IBD. Cobalamin or folate deficiency and various other causes of anaemia such as haemolysis occur infrequently. Common therapeutic targets are the mechanisms behind anaemia of chronic disease and iron deficiency. Oral iron treatment is limited by poor absorption, intolerance, and induction of oxidative stress at the site of bowel inflammation. Intravenous iron sucrose has a good safety profile and a 65–75% response rate within 4–8 weeks, which is paralleled by improvement in the quality of life. Combination therapy with erythropoietin (Epo) leads to a faster and larger haemoglobin increase. It is our experience that virtually all patients with IBD associated anaemia can be successfully treated with a combination of iron sucrose and Epo, which then may positively affect the misled immune response in IBD.
IRON LOSS IN INFLAMMATORY BOWEL DISEASE
Iron deficiency anaemia (IDA) can be considered a gastroenterological condition. The leading causes of iron deficiency (ID) in the developed world are menstruation and blood loss associated with gastrointestinal disease. In the latter case, blood loss in the stomach or intestine cannot be matched by duodenal iron absorption, creating a negative iron balance. This imbalance is often seen in IBD, leading to anaemia. While our understanding of IBD has grown over the past decades, the prevalence of IBD associated anaemia has changed only little: one third of IBD patients still have haemoglobin levels below 12 g/dl.1,2
“Anaemia is a consistent clinical feature of IBD”
Anaemia has been recognised as a key symptom of IBD. For a long time, the only laboratory parameter included in disease activity scores (such as the Crohn’s disease activity index) was the haematocrit/haemoglobin ratio. Intestinal bleeding (either visible or occult blood) is a major symptom of the disease itself, and red blood cells (RBCs) may be lost with each flare. Indeed, anaemia is probably too common to be specifically recognised as a complication of IBD—anaemia is a consistent clinical feature of IBD. For patients, this can be the most debilitating aspect of their disease. Although efficient therapeutic options have been developed for the treatment of IBD associated anaemia, treating anaemia often has a low priority for gastroenterologists. Compared with other manifestations of the disease, such as arthritis or osteopathy, anaemia in IBD has been given scant attention. The purpose of this review is to transfer the current knowledge on IBD associated anaemia into the daily management of IBD.
ANAEMIA
RBCs circulate throughout the body engaged in gaseous exchange, oxygen transport, and carbon dioxide removal. Erythropoiesis must maintain steady state levels of circulating RBCs and respond to acute challenges. The bone marrow is a highly dynamic organ that produces two to three million red cells every second. These red cells are filled with haemoglobin and are replaced after 75–150 days. This process is controlled by the hypoxia sensing mechanism of the kidney which responds by modulating the output of Epo, which in turn determines the level of erythropoietic activity. When red cell production fails to match red cell destruction, the result is anaemia.
Clinical consequence
For a long time it was thought that the clinical symptoms of anaemia (such as fatigue, headache, dizziness, shortness of breath, or tachycardia) occurred only when the haemoglobin level dropped abruptly. It had been argued that patients would adapt to low haemoglobin levels if anaemia developed slowly. This has led to the concept of asymptomatic anaemia. In truth, asymptomatic reflects the fact that impairments in physical condition, quality of life, and cognitive function may be unrecognised by both patients and their doctors. This is a non-IBD specific dilemma. Nephrologists have learned this lesson in the recent past.3 They showed that the process of adaptation to chronic anaemia was in fact adaptation to lower quality of life and that this could be reversed.
Key symptoms such as dyspnoea and tachycardia are due to a decrease in blood oxygen levels and peripheral hypoxia. Compensatory blood shifting from the mesenteric arteries may worsen perfusion of the intestinal mucosa.4 Motility disorder, nausea, anorexia, and even malabsorption have been attributed to anaemia. Reduced metabolic and energy efficiency during physical activity also contribute to weight loss in anaemia.5 A common finding is menorrhagia and amenorrhoea among women. Men may suffer from impotence. Loss of libido may contribute to impaired quality of life in both sexes.6 Central hypoxia may lead to symptoms such as headache, dizziness, vertigo, or tinnitus. Several studies have confirmed that treatment of anaemia improves cognitive function.7 As iron is not only a component of haemoglobin and myoglobin but also of cytochromes and many other enzymes, ID alone may impair cognitive function. Indeed, correction of ID in non-anaemic girls improves verbal learning and memory.8
Chronic fatigue
Anaemia reduces the ability to perform normal daily activities. Chronic fatigue is a common symptom in IBD with anaemia, ID being one of the primary causative factors.9 Fatigue is associated with significant physical, emotional, psychological, and social consequences, with virtually every aspect of daily life being affected. On successful treatment of anaemia with Epo, most studies observed an improvement in energy and activity level and overall quality of life.10 Surprisingly, over the range 8–14 g/dl, the largest improvement in quality of life occurred when haemoglobin levels increased from 11 to 13 g/dl.11
“Concern regarding the fatigue of IBD patients is probably as important as concern for their abdominal pain or diarrhoea”
Changes in quality of life were also studied in anaemic Crohn’s disease patients treated with iron sucrose and Epo.12 The feeling of well being, mood, physical ability, and social activities accounted for most of the improvement in quality of life. Also, individual patients reported relief of disturbed sleep and increased appetite or libido. Using the same questionnaire, quality of life data were compared with data that had been assessed in anaemic patients.13 It is remarkable that the absolute quality of life in Crohn’s disease associated anaemia matched well with data collected in patients with advanced cancer.2
Oncologists have documented a significant communication gap between patients and physicians regarding fatigue.14 Concern regarding the fatigue of IBD patients is probably as important as concern for their abdominal pain or diarrhoea.
AETIOLOGY OF ANAEMIA IN IBD
The anaemia in IBD is complex and commonly represents a particular example of the combination of IDA and anaemia of chronic diseases (ACD).
Iron deficiency
In normal subjects, daily iron loss amounts to 1–2 mg and this requires a similar amount to be taken up from the diet. Dietary iron occurs in two forms: haeme (from myoglobin meat, poultry, and fish) and non-haeme (mostly from plants).15 The molecular pathway of iron absorption has recently been reviewed.16 Non-haeme iron absorption depends on many factors, including the presence of gastric acid, ascorbic acid, and inhibitors such as phytic acid and polyphenols (in vegetables). Haeme iron is released after mechanical and enzymatic digestion of myoglobin. Food aversions and self reported intolerance are common in IBD17,18 and this will affect the amount of iron available in the diet (table 1). Various reports have pointed to diminished iron intake in IBD (specifically in women) predominantly due to avoidance of high fibre fortified breakfast cereals which may be perceived to exacerbate abdominal symptoms.19 Changing dietary advice may not be easy, especially if it is viewed as exacerbating abdominal symptoms. Low dose iron supplementation is likely to be preferred.
Iron intake in patients with inflammatory bowel disease (IBD) and controls
The only way to lose iron is by menstrual and intestinal bleeding. Chronic intestinal bleeding in IBD may exceed the amount of iron that can be absorbed from the diet, resulting in a negative iron balance.20 Although iron absorption in IBD is not generally abnormal, it can be occasionally impaired in Crohn’s disease of the duodenum or upper jejunum.21
When the rate of iron supply to the developing erythroblast is limited as a result of ID, red cell haemoglobinisation would be impaired. The red cells which then emerge from the marrow are microcytic and hypochromic. The Epo response to the fall in haemoglobin will stimulate erythropoiesis further, creating an even greater demand for iron which cannot be met. As a result there is a high degree of ineffective erythropoiesis in this condition.22
Iron and immunity
Iron is essential for erythropoiesis but is an active component of many enzymes also relevant for the growth and function of other dynamic cell compartments, such as immune cells. Iron is involved in immune effector pathways of neutrophils and macrophages by formation of toxic hydroxyl radicals. Iron restriction affects the proliferation and differentiation of B and Th1 lymphocytes, while iron overload leads to dysfunction of natural killer cells, impaired neutrophil cytotoxicity, and changes in the ratio of CD4+ to CD8+ lymphocytes.23,24
Monocytes/macrophages have evoked different pathways by which they can acquire iron. Therefore, they are not affected as much by iron limitation. Macrophages may act as an iron storage pool which may expand in ACD.25,26 Intracellular iron availability in macrophages is important for fighting infection. The natural resistance associated macrophage protein (NRAMP-1) has been identified as a transmembrane iron transporter that confers resistance towards infection with intracellular pathogens.27,28
Imbalances in iron homeostasis influence cytokine activities and cell mediated immune effector mechanisms of macrophages. High iron load reduces the responsiveness towards interferon γ (IFN-γ) leading to lower expression of tumour necrosis factor α (TNF-α), MHC class II antigens, neopterin, or intercellular adhesion molecule 1, and to a Th1/Th2 imbalance with Th1 effector function being weakened and Th2 mediated cytokine production being increased.29–32 As a consequence, such macrophages loose their ability to kill intracellular pathogens by IFN-γ mediated pathways. This can be partially explained by inhibition of transcription of inducible nitric oxide (NO) synthase,33,34 the enzyme for cytokine inducible high output formation of NO. NO is a critical molecule of macrophages for defence against infectious pathogens.35,36
“A certain amount of iron appears to be necessary for lymphocyte development but iron deposition in immune cells blocks essential immune functions and host resistance towards invading pathogens”
Such in vitro findings are supported by clinical evidence. In human cerebral malaria, the iron chelator desferrioxamine resulted in an improved clinical course.37,38 In contrast, patients with iron overload in Africa are at higher risk of tuberculosis.39,40 However, patients with severe ID are also susceptible to infection.41 Thus a certain amount of iron appears to be necessary for lymphocyte development but iron deposition in immune cells blocks essential immune functions and host resistance towards invading pathogens. It is tempting to speculate that ID enhances the IFN-γ response in Th1 driven inflammation in immune mediated inflammatory disorders such as Crohn’s disease.
Anaemia of chronic disease
ACD is the most frequent anaemia in hospitalised patients and develops in subjects suffering from diseases that are associated with chronic activation of cell mediated immunity, such as chronic infections, immune mediated inflammatory disorders, or malignancy.42 Thus ACD is primarily an immune driven disorder with cytokines such as TNF-α or IFN-γ and acute phase proteins being the major players. Several factors contribute to the development of ACD.
Diversion of iron traffic
A hallmark of ACD is hypoferraemia, and accordingly iron limitations at the erythron, while iron is taken up by macrophages and dendritic cells of the reticuloendothelial system (RES). Thus ACD can be easily diagnosed by the presence of hypoferraemia and increased serum levels of ferritin (fig 1).

Iron and erythropoiesis in chronic disease. When erythropoiesis is suppressed, iron which is released at the end of the red cell lifespan and which would normally have been recycled into new haemoglobin is diverted into iron stores. As a result, serum ferritin levels are increased. Iron absorption is driven mainly by erythropoiesis. When this is suppressed, iron absorption is likewise decreased.
Macrophages can acquire iron by multiple pathways, including transferrin receptor mediated iron uptake, NRAMP-1, lactoferrin, the haemoglobin receptor, and erythrophagocytosis.43 Cytokines modulate the expression and activity of these iron uptake pathways and also cause iron retention by downregulating expression of the transmembrane iron transporter ferroportin 1.44,45 Acute phase proteins such as α1 antitrypsin block transferrin mediated iron uptake into erythroid progenitor cells but not into cells of the RES.46 The recently discovered interleukin 6 inducible peptide hepcidin downregulates iron absorption in the duodenum and may interfere with iron release from cells of the RES.47
Inhibition of erythroid progenitor proliferation and differentiation
Apart from modulating iron homeostasis, cytokines directly affect erythropoiesis by inhibiting the growth of erythroid progenitor cells. TNF-α and type I and II interferons block BFU-e and CFU-e colony formation48 and IFN-γ appears to be the most potent inhibitor of erythropoiesis in directly blocking CFU-e proliferation.49 The latter is nicely reflected by an inverse correlation between IFN-γ levels and haemoglobin concentration and reticulocyte counts in ACD patients.50 NO may directly block erythropoiesis by inhibition of erythroid progenitor cell proliferation and haeme biosynthesis.51,52
Blunted Epo response
Serum Epo levels in patients with ACD appear to be inadequately low for the degree of anaemia. However, this does not hold true for all diseases underlying ACD53 but has been shown for Crohn’s disease and ulcerative colitis.54,55 In fact, cytokines may directly inhibit Epo production in the kidney.56 Moreover, Epo responsiveness of erythroid progenitor cells may be associated with the severity of disease and the degree of immune activation. In vitro, in the presence of IFN-γ or TNF-α, higher amounts of Epo are needed to restore CFU-e colony formation.57
Erythrocyte life cycle
Application of sublethal doses of TNF-α or endotoxin to mice reduces red blood cell (RBC) half life, decreases the incorporation of iron, induces hypoferraemia, and causes anaemia.58 Stimulation of erythrophagocytosis is also reflected by increased amounts of erythrocyte derived iron in splenic macrophages and Kupffer cells under inflammatory conditions.59
Vitamin B12 and folate deficiency
Vitamin B12 (or cobalamin) and folic acid are vitamins and coenzymes involved in a series of complex biochemical reactions, including DNA synthesis.
Clinical evidence of Vitamin B12 deficiency occurs late as body stores have to be depleted to less than 10%. Vitamin B12, which is bound to the stomach derived intrinsic factor, is primarily absorbed in the terminal ileum. Chronic ileal inflammation or resection, particularly in Crohn’s disease, may give rise to deficiency and clinical symptoms. An association with gastric Crohn’s disease had also been recognised.60 Folate is absorbed in the duodenum and jejunum and deficiency may be due to inadequate diet, malabsorption, or drug interactions (sulphasalazine, methotrexate). Clinical manifestation occurs earlier as folate stores last only 1–2 months.
Anaemia due to treatment
Apart from folate deficiency, therapy with sulphasalazine or 5-aminosalicylic acid has been related to a minor degree of haemolysis or aplasia.61–64 More importantly, both 6-mercaptopurine and azathioprine have a direct myelosuppressive effect. The risk of developing leucopenia or aplasia is high in individuals with low thiopurine methyltransferase (TPMT) activity.65 The enzyme activity of TPMT is genetically determined and genotyping has been suggested as a means of detecting patients at risk.66 In clinical practice, however, concerns have been raised about the predictive accuracy of this test.67,68
There are many other less common causes of anaemia in IBD (reviewed by Schreiber and Wedel69) which are best dealt with by those who see them more frequently, such as the local haematologist (table 2).
Aetiology of inflammatory bowel disease associated anaemia
DIAGNOSTIC TESTS
Monitoring of IBD patients with complete blood counts is a routine measure. The lower haemoglobin cut off level in women (12.0 g/dl v 13.5 g/dl in men) may fail to trigger doctors to provide adequate therapy when needed. Of course, menstruating women lose more blood than their male counterparts and are therefore at higher risk of ID. The consequence of this biological fact should be superior care for haemoglobin and iron stores in menstruating or pregnant women and not a lower treatment trigger.
“Monitoring of IBD patients with complete blood counts is a routine measure”
Red cell size is reflected in mean cell volume (MCV) and mean cell haemoglobin, which allow a first diagnostic clue. Hypochromia and microcytosis indicate red cell ID with or without concomitant ACD. Macrocytosis points to a vitamin B12 or folic acid deficiency. An increase in MCV without significant anaemia is useful in monitoring treatment response or compliance during azathioprine or 6-mercaptopurine therapy.70 Apart from a complete blood count, iron parameters need to be checked regularly. Measurement of serum ferritin reflects the level of iron in stores. When serum ferritin is less than 15 μg/l, iron stores are definitely depleted. When ferritin is above 20 μg/l, there is iron in the stores but it may be insufficient to meet the demands of the proliferating progenitors of red cells, and this is true even up to levels of 700 μg/l.71 C reactive protein is useful to estimate the level of inflammation.
Further evaluation may include reticulocyte counts, vitamin B12, and folic acid. The per cent hypochromic RBC and reticulocyte haemoglobin content have been proposed for evaluation of functional ID during Epo therapy.72,73
Because of different therapeutic consequences, it is important to distinguish ACD from ID. Patients with “classical” ACD present with increased ferritin levels while transferrin concentrations as well as transferrin saturation are reduced. In contrast, all of these parameters are decreased in ACD patients with ID. Pure ID is recognised by low ferritin and transferrin saturation but increased transferrin concentrations. The ratio of soluble transferrin receptor/log ferritin has been proposed for differential diagnosis of these overlapping conditions.74 In IBD patients, high levels of serum transferrin, soluble transferrin receptor, and serum Epo predict response to intravenous iron supplementation and low levels indicate a need for concomitant Epo therapy.75
QUALITY OF LIFE: THE THERAPEUTIC GOAL
The ultimate therapeutic goal is improvement in quality of life but the only objective measure we have to hand is change in haemoglobin concentration. Quality of life improvements of anaemic cancer patients were detected at haemoglobin levels of up to 14 g/dl.11 As most IBD patients are young, they may have even higher physical and cognitive demands than cancer patients. Normalisation of haemoglobin level (12.0 g/dl in women and 13.5 g/dl in men) should be sought.
The mechanisms of IBD associated anaemia involve particularly ID and ACD. In cases of vitamin B12 or folic acid deficiency, appropriate substitution is needed. This leaves the major problem of directing iron therapy and improving erythropoiesis in chronic disease.
Iron supplementation
Oral iron preparations
Oral iron supplements commonly contain iron in the form of ferrous salts (ferrous sulphate, ferrous gluconate, and ferrous fumarate). All ferrous compounds are oxidised in the lumen of the gut or within the mucosa with release of activated hydroxyl radicals, which will attack the gut wall and produce a range of gastrointestinal symptoms and discomfort.76,77 Enteric coated ferrous formulations attempt to avoid this by minimising iron release in the stomach. If this is successful it also prevents iron absorption.
“Because there is no excretory route, iron homeostasis in organisms is regulated at the level of iron uptake”
Because there is no excretory route, iron homeostasis in organisms is regulated at the level of iron uptake. If iron absorption is not tightly regulated, iron overload and associated toxicity occurs such as seen in hereditary haemochromatosis. Another obstacle of oral iron supplementation is therefore the limited capacity of iron absorption. The efficacy of oral iron therapy in patients with IBD may be further hindered by some IBD specific factors. Firstly, gastrointestinal side effects of oral ferrous iron such as nausea, bloating, diarrhoea, or upper gastrointestinal pain are more pronounced compared with those observed in non-IBD patients taking oral iron therapy.78 Secondly, in chronic inflammatory disease, absorption of iron appears to be reduced which would limit the growth of microbes in chronic infections.79 The acute phase protein hepcidin may play a central role in this as its overexpression in the liver leads to decreased iron uptake by the duodenum.47 Thirdly, body iron distribution is altered. Most of the iron that is absorbed is directed into the RES while only minor amounts may reach the sites of erythropoiesis.
Ferric iron polymaltose complex, ferric trimaltol, or haeme iron polypeptide are also available in some countries. Ferric iron has less pro-oxidant potential but is sparingly insoluble and generally biounavailable. Surprisingly, in an open study, oral administration of ferric trimaltol complexes has been found to be safe and effective.80 The newer non-ionic iron polymaltose has been shown to have no oxidative potency on lipoproteins in healthy subjects81 and a better compliance than ferrous sulphate but data on efficacy are lacking.82 Haeme iron polypeptide takes advantage of alternative absorption pathways. This product is thought to have improved bioavailability83 and promises lower side effects but has an animal origin and larger series have not yet been treated.
Intravenous iron preparations
The limitations of oral iron therapy in IBD patients mean that alternative routes of iron administration must be considered. Direct administration of iron into the circulation requires formulations that prevent the cellular toxicity of iron salts.84 Three different products are currently available:
Iron dextran is a stable parenteral iron product with a molecular weight of 100–500 kDa. These iron complexes show high structural homogeneity and only slow and competitive delivery to endogenous iron binding proteins. Complexes are actively phagocytosed by macrophages of the RES before they are released and become available for haemoglobin synthesis. Plasma half life is 3–4 days. The stability of the dextran complex allows administration of high single doses (so called “total dose therapy”). The molecule however may cause well know dextran induced anaphylactic reactions.
Iron gluconate is a labile type with fast degradation kinetics and direct release to plasma proteins (apotransferrin, apoferritin, and others). Potential toxicity of iron gluconate is caused by oversaturation of the transferrin binding capacity.85 Non-transferrin bound free ionic iron may induce acute endothelial cell injury and a transient capillary leak syndrome. Clinical symptoms in such circumstances include nausea, hypotension, tachycardia, dyspnoea (lung oedema), and bilateral oedema of the hands and feet, and should not be misread as anaphylaxis. The use of iron gluconate for iron deficiency in patients on dialysis has been found to be safe and superior to iron dextran.86,87
Iron sucrose (previously referred to as iron saccharate) is much smaller than iron dextran (34–60 kDa) and carries no risk of dextran induced anaphylactic reactions. Iron sucrose is a partially stable type with medium degradation kinetics and partial uptake of released iron by plasma proteins such as (apo)-transferrin but also by the RES. Its half life is relatively short (5–6 hours).88
During the last few years, experience of using iron sucrose in various forms of ID has evolved.88 Single doses of up to 300 mg are safe.89 The maximal recommended dosage is 600 mg/week but this amount exceeds the physiological needs of the proliferating erythroblast.89 If the infusion speed is too fast (above 4 mg Fe3+/min) or the single total iron dose too high (above 7 mg Fe3+/kg), non-transferrin bound free iron may cause transient hypotension, tachycardia, and dyspnoea, as described for iron gluconate. Increased levels of non-transferrin bound iron have been detected in asymptomatic haemodialysis patients following iron sucrose injections which may potentially promote atherosclerosis.90
More than 1000 infusions have been given in trials in IBD associated anaemia without major side effects, using 200 mg iron sucrose, diluted in 250 ml of 0.9% sodium chloride, twice weekly during the first two weeks and once weekly thereafter.12,55,75 After 1200 mg of iron sucrose (four weeks) approximately 65% and after 2000 mg (eight weeks) approximately 75% of patients responded (fig 2). Iron sucrose has also been safely used after the first trimester of pregnancy and postpartum.91–93

Response to iron sucrose in ulcerative colitis and Crohn’s disease. A total of 2 g of iron sucrose were given intravenously within eight weeks: 400 mg/week during the first two weeks and 200 mg/week thereafter. Response was defined as increase in haemoglobin of equal to or above 2 g/dl. Data were collected from two trials.12,55
In general, the intramuscular or subcutaneous routes of parenteral iron administration are obsolete because of the increase in side effects and decrease in efficacy.
Iron therapy and intestinal inflammation
As iron homeostasis and cellular immunity are closely linked, it is suggestive that the different therapeutic regimens of iron supplementation may have subtle effects on immune function and intestinal inflammation in IBD. As outlined above, iron inhibits IFN-γ activity and thereby has deactivating effects on macrophage function and the Th1 response. Thus intravenous iron therapy could ease Th1 driven intestinal inflammation in Crohn’s disease. Although specific data in Crohn’s disease are missing, this notion is supported by the fact that (i) intravenous iron supplementation to anaemic dialysis patients significantly reduced circulating levels of TNF-α and peroxides94 and (ii) combined treatment of anaemia in subjects with active rheumatoid arthritis with iron and Epo significantly reduced disease activity.95
“Oral iron may induce oxidative stress within the lumen of the gut”
Oral iron may induce oxidative stress within the lumen of the gut. This mechanism increases the intestinal production of proinflammatory cytokines in rodent models of IBD and was the hypothesis for studying iron chelation therapy in Crohn’s disease.96,97 Most of the ingested ferrous iron is not absorbed but is passed on to the ileum and colon, sites of inflammation in Crohn’s disease and ulcerative colitis, before appearing in the stool. When iron attaches to the ulcerated intestinal surface, it may increase local production of reactive oxygen species and thereby enhance inflammation. This has been demonstrated in animal models of IBD 96 as well as in patients with Crohn’s disease.78
Although there are no data at present, we do not expect an intestinal increase in oxidative stress from intravenous iron products because ferric iron does not have an oxidative potential and the route of administration does not favour intestinal accumulation.
Recombinant human Epo
Specific drugs for the treatment of ACD have not yet been developed. Anti-inflammatory drugs may inhibit cytokine production but may also inhibit erythropoiesis (for example, azathioprine). Although theoretically anti-TNF and anti-IFN-γ strategies such as infliximab or natalizumab may specifically counteract ACD driven erythropoietic inhibition,98 such effects have not been reported in clinical trials in IBD.
Supraphysiological doses of Epo can overcome the inhibition of erythropoiesis in ACD, which is the rationale for Epo therapy.57 Epo has been studied in a variety of different types of ACD.99,100 In IBD, successful treatment was reported after restoration of iron stores.101 Double blinded controlled trials followed, with either oral102 or intravenous12 iron supplementation (fig 3). All trials demonstrated a significant effect of Epo on haemoglobin increase. Epo treatment of iron refractory cases with IBD associated anaemia also proved to be safe and effective in children.103 The specificity of the Epo downstream events limits the array of possible adverse events. Thrombosis, hypertension, and seizures have been rarely observed in patients with renal failure and are likely due to the underlying rise in haematocrit and total blood volume. Next generation Epo analogues, such as the novel erythropoiesis stimulating protein (NESP), have a longer serum half life but a decreased binding affinity to the Epo receptor.104 We are not aware of any studies that have been performed in IBD.

Iron sucrose versus ferrous sulphate for inflammatory bowel disease associated anaemia. Two controlled studies, both of which were demonstrating the effect of erythropoietin (Epo) in IBD associated anaemia, are outlined. Baseline haemoglobin levels and total Epo dosage were identical. In one trial (A), ferrous sulphate was used for iron supplementation102 and in the other (B) iron sucrose was given.12 On ferrous sulphate alone, 100 mg/day, mean haemoglobin level dropped over the 12 week study period. In contrast, iron sucrose caused a considerable haemoglobin increase that was faster and larger when combined with Epo.
As iron sucrose was found to be highly effective on its own, Epo was spared for those cases who primarily failed on iron sucrose alone.55 In an attempt to identify parameters that predict failure of iron sucrose therapy, plasma Epo levels, soluble transferrin receptor, and transferrin concentrations were studied.75 Low Epo (below 100 U/l), soluble transferrin receptor (below 50 nmol/l), or transferrin levels (below 2.9 g/l) strongly indicated resistance to iron sucrose. However, it is our experience that virtually all patients with IBD associated anaemia can be successfully treated with the combination of iron sucrose and Epo (fig 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
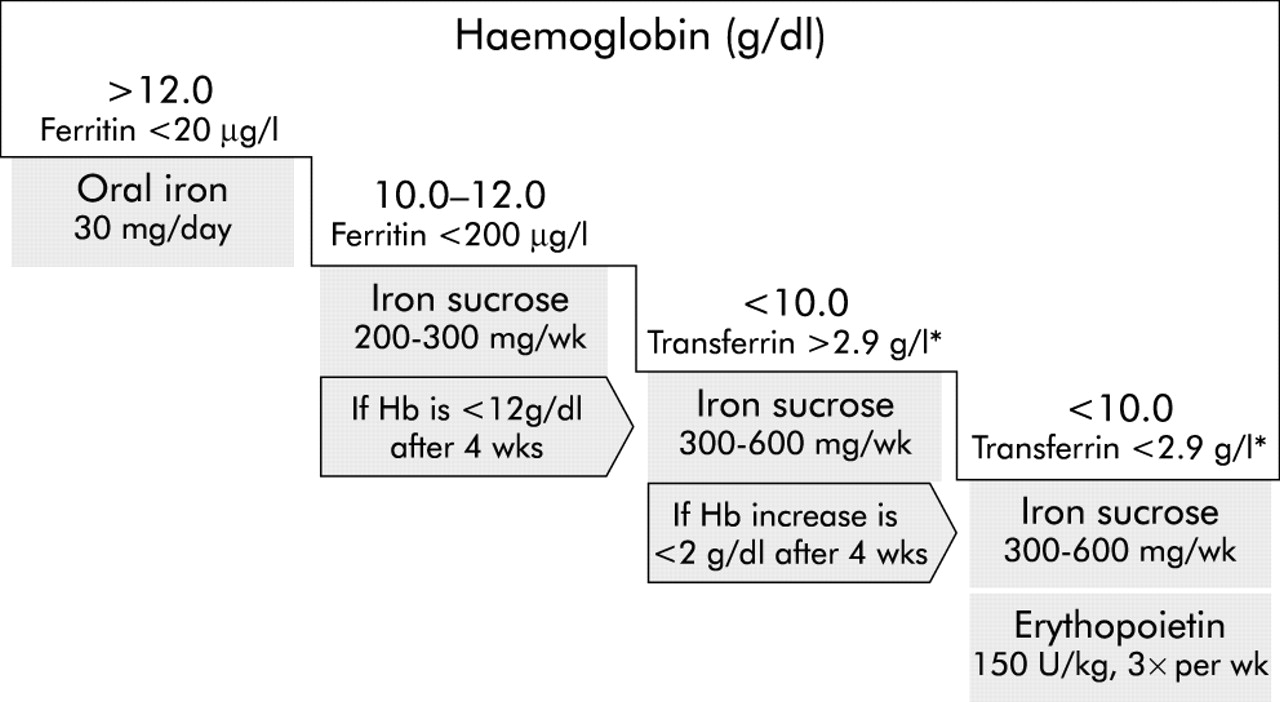
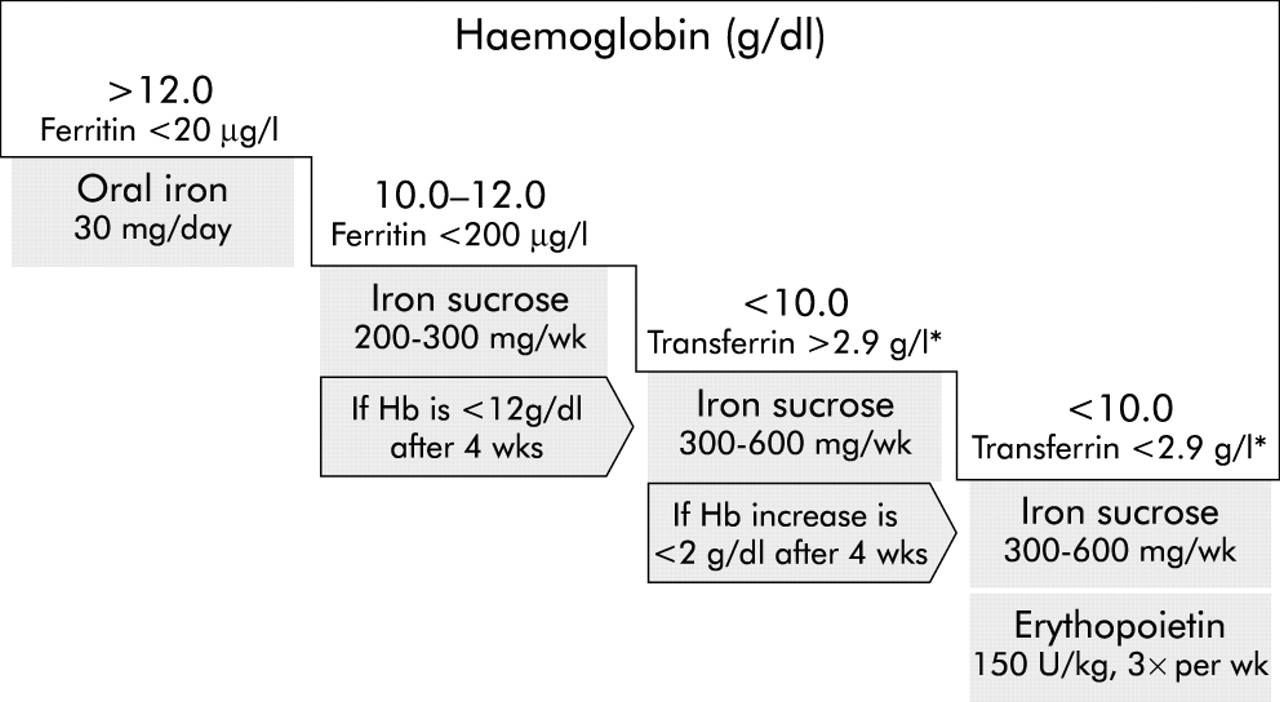
Adjusting therapy to the degree of anaemia. The place of oral iron therapy is mainly prevention of iron deficiency anaemia. In patients with normocytic or microcytic anaemia, iron sucrose demonstrates the best efficacy and tolerability. The amount of iron needed relates to the degree of anaemia and can be estimated using the approximation that an increase of 1 g/dl haemoglobin (Hb) requires about 200 mg of intravenous iron. It is recommend that iron therapy is suspended in cases of acute infection (for example, abscess) or at a transferrin saturation >50%. *Instead of transferrin, the soluble transferrin receptor (below 50 nmol/l) or erythropoietin concentration (below 100 U/l) can be applied.
“Until we cure IBD, our prime goal is optimisation of supportive care in order to enhance the patient’s quality of life”
When dealing with IBD patients, there are good reasons to pay more attention to iron metabolism and erythropoiesis than ever before. Anaemia in IBD is still a frequent complication that affects the ability to perform normal daily activities, but the tools to effectively prevent or treat anaemia have been identified and are readily available. Until we cure IBD, our prime goal is optimisation of supportive care in order to enhance the patient’s quality of life. Aiming for anaemia treatment in IBD is rewarding for both the patient and the caring physician.
Acknowledgments
CG received grants from the Austrian Science Fund (P15314) and the OeNB Anniversary Fund (ONB10543). MCEL is supported by the PPP Foundation and the DH NHS R&D Programme.