Article Text

Abstract
Objectives The global prevalence of IBS is difficult to ascertain, particularly in light of the heterogeneity of published epidemiological studies. The aim was to conduct a literature review, by experts from around the world, of community-based studies on IBS prevalence.
Design Searches were conducted using predetermined search terms and eligibility criteria, including papers in all languages. Pooled prevalence rates were calculated by combining separate population survey prevalence estimates to generate an overall combined meta-prevalence estimate. The heterogeneity of studies was assessed.
Results 1451 papers were returned and 83, including 288 103 participants in 41 countries, met inclusion criteria. The mean prevalence among individual countries ranged from 1.1% in France and Iran to 35.5% in Mexico. There was significant variance in pooled regional prevalence rates ranging from 17.5% (95% CI 16.9% to 18.2%) in Latin America, 9.6% (9.5% to 9.8%) in Asia, 7.1% (8.0% to 8.3%) in North America/Europe/Australia/New Zealand, to 5.8% (5.6% to 6.0%) in the Middle East and Africa. There was a significant degree of heterogeneity with the percentage of residual variation due to heterogeneity at 99.9%.
Conclusions The main finding is the extent of methodological variance in the studies reviewed and the degree of heterogeneity among them. Based on this, we concluded that publication of a single pooled global prevalence rate, which is easily calculated, would not be appropriate or contributory. Furthermore, we believe that future studies should focus on regional and cross-cultural differences that are more likely to shed light on pathophysiology.
- IRRITABLE BOWEL SYNDROME
- FUNCTIONAL BOWEL DISORDER
- EPIDEMIOLOGY
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
The prevalence of IBS has been studied extensively.
The methodology used to study IBS prevalence is not uniform among studies.
Estimates of IBS prevalence usually are reported in the range of 10–20%, but the basis for these estimates is not clear.
What are the new findings?
This literature review of IBS prevalence in population-based studies was conducted by a multinational group of investigators, who had facilitated access to articles published in multiple languages because of their familiarity with regional publications and languages.
The main finding of the study is the extent of methodological variance in the studies and the significant degree of heterogeneity among them.
There is a noteworthy lack of data from Africa, Eastern Europe and Arab countries.
The predominance of women who fulfil the different diagnostic criteria for IBS is reaffirmed in this study.
How might it impact on clinical practice in the foreseeable future?
The assessment of prevalence rates is important for understanding the distribution and burden of disease, for the evaluation of treatment modalities, to provide incentive for the development of new drugs and for the allocation of healthcare resources and research funding.
The lack of reliable prevalence data is a barrier to attaining these goals.
The results of the study highlight the need for a global survey of IBS prevalence with multinational collaboration and uniform research methodology. Future studies should focus on regional and cross-cultural differences that are more likely to shed light on pathophysiology.
Introduction
The prevalence of IBS, a common functional GI disorder (FGID), has been studied extensively. Multiple methodologies have been used to assess the prevalence of IBS around the world. It has been investigated in convenience samples among workers or students or during health surveys1 and in urban neighbourhoods and rural areas.2–4 Some studies have been hospital based or clinic based,5 while others were community based. In addition, the methods of data collection have included in-person household interview, mail survey, telephone survey and, recently, internet survey. Finally, different diagnostic criteria have been used in these studies including the Manning criteria (in different studies either two, three or four of the six original Manning criteria were used to diagnose IBS), Rome I–III and others.6–9
Determining population prevalence by self-reported symptoms through a questionnaire, in the absence of an established diagnostic biomarker, could lead to an inaccurate estimation of the actual population prevalence rate. There are differences in symptom interpretation and reporting patterns among different countries, geographical regions, and cultural and ethnic groups.10 ,11 Even if the survey methodology was uniform, there might be cultural and regional differences in perception, for example, relating to pain, bloating, bowel habit and other symptoms. Thus, gaining a global perspective on the prevalence of IBS remains difficult because of methodological heterogeneity and cultural differences in symptom perception and reporting. Potential confounders in multinational comparative prevalence studies for IBS are shown in box 1. These issues are presented and discussed succinctly by Quigley et al.12
Potential sources of methodological confounding in multinational comparative IBS prevalence studies
Variations in diagnostic criteria
Manning (using two, three or four out of the six criteria)
Rome I, II, III
Study population
Age, gender, class
Culture, ethnic group, language
Select group versus representative of general population
Clinic-based
Students, workers, urban versus rural, etc.
Survey instrument
Questionnaire
Validation of translated questionnaires
Survey method
Mail
Personal interview
Telephone
Self-administered questionnaire
Internet
Cultural and regional differences in symptom interpretation and reporting.
Lovell and Ford reported the results of a systematic review of IBS prevalence.13 The authors found a pooled global prevalence of 11.2% (95% CI 9.8% to 12.8%), with a range among countries from 1.1% to 45.0%.
The purpose of the present study was to conduct a literature review of publications reporting the epidemiology and prevalence of IBS in community-based studies in as many languages as possible. A team of experts in the field who represent all regions of the world and are fluent in multiple languages conducted the review.
Methods
The Rome Foundation commissioned a Working Team on Cross-cultural, Multinational Research in the FGIDs to address the issues and challenges related to global research in the FGIDs.10 ,14 The full report of the working team can be downloaded at http://theromefoundation.org/committees/multinational_com.cfm, and an article summarising the full report was published.15 One of the working team's mandates was to conduct a review of IBS global epidemiology. The review was conducted by working team members representing different geographical areas, each responsible for using the study protocol and search parameters to identify all relevant studies in their assigned region. Searched databases were Medline, Embase, Web of Science, Cochrane, Latindex, Bireme, SciELO and other databases including recent abstracts, compilations and meeting procedures. In cases where there were other studies cited in the paper that were not identified in the search, they were reviewed for eligibility. In addition, there were no language restrictions and the investigators were encouraged to survey publications in as many languages as they could, getting help from colleagues in their regions to translate when required. The regions covered and the responsible investigators are shown in table 1.
Delegation of responsibility for regional literature searches
Search terms and eligibility criteria
The medical literature was searched using the following sequence of terms: IBS OR irritable bowel syndrome OR functional bowel disorder AND epidemiology OR prevalence AND region OR country (eg, Latin America OR Mexico OR Guatemala OR Colombia OR Argentina et al).
Papers and abstracts that were identified by the search terms were considered to be eligible for the study and were included in the analyses in accordance with the criteria shown in table 2. The present paper relates only to the subgroup of studies that were conducted in the general population or were community based. Thus, the full study database of extracted articles is larger than the selected database used in the present analysis because it also contains studies that are not of general or community-based populations.
Eligibility criteria for the present report
Study database and data extraction
Each investigator completed the database for their region and then the individual databases were merged into the final study database. The data that were extracted from all papers included the following variables (if cited in the paper): type of paper and year of publication (eg, journal articles published in 1999 and later, abstracts published from 2006 to 2013); country; language of study; study design (eg, cross-sectional); study setting (eg, urban community); survey instrument (eg, Rome II questionnaire); method of data collection (eg, in-person interview, mail survey, telephone survey), number of participants; females (%); response rate (%); mean age; mean years of education; whether the study was multinational/cross-cultural; IBS prevalence (%); IBS prevalence by gender; IBS-constipation (IBS-C) (%); IBS-diarrhoea (IBS-D) (%); IBS-mixed (%); and IBS-unclassified (%). The earliest year of publication was chosen as 1999, the year that the Rome II diagnostic criteria were developed, based on our perception that epidemiological research in the FGIDs became more rigorous at this time and that, in general, earlier research was less methodologically sound than studies that began around 1999–2000.
The representative for each region selected all papers from their region that were included in the final analyses, in many cases with research assistants. All papers were also read and reviewed by the first author (ADS). In cases where the appropriateness of the study was questioned by ADS, an email exchange with the regional representative was conducted to clarify the issues raised. Where necessary, the first author of the paper was consulted for clarification. The final decision on inclusion was reached by agreement between ADS and the regional representative, and, in some cases, papers were excluded from the study based on this joint review.
Statistical analyses
Descriptive analyses were performed using the SPSS software package (V.21, Chicago, Illinois, USA). Descriptive statistics are presented as percentages for categorical variables and means (SD) for continuous variables.
To calculate pooled prevalence rates, we used the appropriate method, as published by Yang,16 which combines separate population survey prevalence estimates into an overall meta-prevalence estimate. For the purpose of pooled analyses, the countries were grouped into (a) Asia, (b) North America/Europe/Australia/New Zealand, (c) Latin America and (d) the Middle East and Africa. For further analysis of the data, we used the Stata software (V.13.1, Stata Corp., Texas, USA). We performed a univariate meta-analysis, in which each group of countries contributes an estimate of a single quantity (eg, IBS, gender), and multivariate meta-analysis, in which groups of countries (geographic regions) contribute estimates of more than one quantity: for example, IBS subgroup by geographic region.
Then, we modelled the effects across regions using consistency and inconsistency models. To analyse variables of interest, we used the univariate random-effects meta-regression model because, compared with a fixed-effect model, it assigns more moderate weights to each study, that is, more weight to small studies and less to large ones. As a result, the CI about each coefficient (and slope) is wider than in the fixed-effect model and the p values corresponding to each coefficient and to the model as a whole are less likely to meet the criterion for statistical significance. This added a negative bias, making statistically significant comparisons more robust.
For the heterogeneity statistic, the weighted sum of squares of the residuals was used as a generalisation of Cochran's Q from meta-analysis to meta-regression. Following this, a test of the null hypothesis of no residual (unexplained) heterogeneity was obtained by comparing Cochran's Q to a χ2 distribution.17 ,18
Results
Studies included in the paper
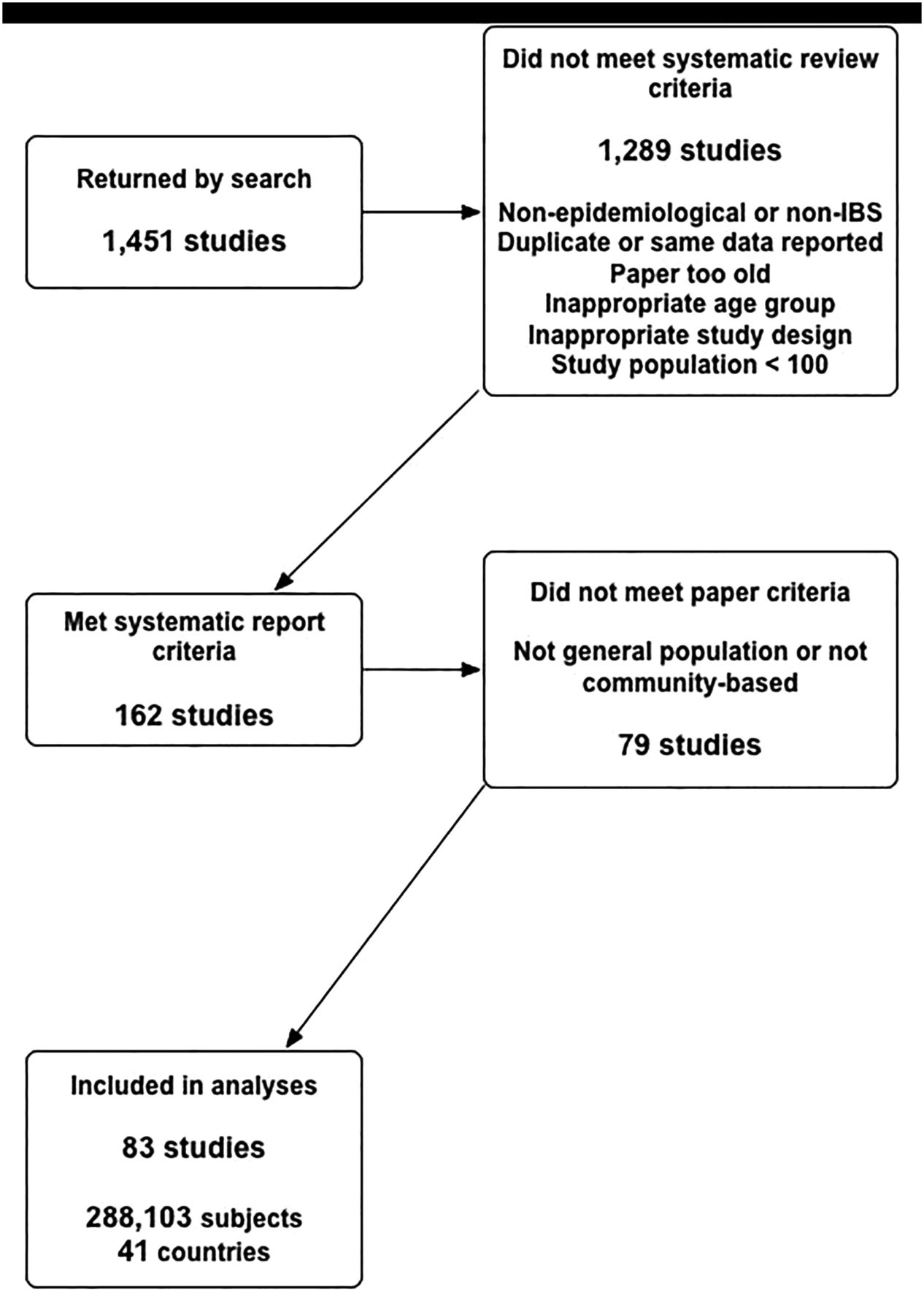
In all, 1451 papers were returned by the search (figure 1). Of these, 162 met the inclusion criteria and the remaining 1289 were disqualified for the following reasons: non-epidemiological or non-IBS study—737; review—236; duplicate (more than one report for same study)—240; earlier than 1999 for article—33; earlier than 2006 for abstract—4; inappropriate population age—23; inappropriate study design—15; and study population less than 100—1.
{kind=link}
Flow diagram of citations retrieved by the literature search and included in the present study.
Of the 162 publications that met the review criteria, 83 were included in the present report.2 ,6 ,9 ,19–98 The other 79 were disqualified after further review because they were not population or community based or they were repeat publications of the same data. Of the 83 studies included in this review, 41 were published in the English-language literature. The others were distributed as follows: Spanish—16; Chinese—13; Persian—3; Turkish—2; Arabic, Dutch, Finnish, Greek, Hebrew, Icelandic, Norwegian and Portuguese—1 each.
The final 83 studies included 288 103 participants in 41 countries (the largest study encompassed eight countries). The mean number of participants per study was 3471.1, and the median sample size was 1624.0. The largest numbers of studies, by country, were from China (N=8), Japan (N=6), and South Korea and Mexico (N=5 each). The mean pooled response rate, reported in 62 studies, was 71.3% (95% CI 71.1 to 71.4). The response rates by region were 89.0% in Asia (N=19), 85.3% in Latin America (N=16), 76.5% in the Middle East and Africa (N=11) and 54.0% in North America/ Europe/Australia/New Zealand (N=19).
In 77 papers (92.8%), the authors reported the method of data collection including personal interview (N=40 (51.9%)), mail (N=16 (20.8%)) and telephone (N=9 (11.7%)). Personal interviews were the method of data collection in 16 of 21 studies from Asia (76.2%), 9 of 12 studies (75%) from the Middle East, 9 of 12 studies (75%) from Africa, and 8 of 14 studies (57.1%) from Latin America. Personal interviews were less commonly employed in North America/ Europe/Australia/New Zealand (7 of 23, 30.4%) with more studies using mailed questionnaires (13 of 23, 56.0%) and some using telephone interviews (3 of 23, 13.0%). IBS prevalence by survey method was 6.8% by personal interview, 10.5% by mail questionnaire and 8.0% by telephone interview for all regions taken together.
Diagnostic criteria
Twelve studies used the Manning criteria (7 as a single criterion), 12 used Rome I (7 as a single criterion), 38 Rome II (36 as a single criterion), 14 Rome III (12 as a single criterion) and 7 used other criteria. IBS prevalence by diagnostic criteria was 7.8% by Rome II (N=38), 8.3% by Manning criteria, 6.7% by Rome I, 9.1% by Rome III and 12.8% in studies in which the diagnostic criterion was not specified. Table 3 presents regional IBS prevalence rates by method of data collection and diagnostic criteria.
Comparison of regional pooled prevalence rates (%) for IBS by sex, survey method and diagnostic criteria
Sociodemographic variables
Of the 288 103 participants, 55.0% (95% CI 46.2% to 69.4%) were females (N=74 studies) with a range from 28%96 to 74.3%.31 The mean age was 40.0 (95% CI 31.2 to 51.0) years with a range from 27.7 years (Vietnam)51 to 53.0 years (Germany).57
Prevalence rates
Individual study rates
The 83 studies were conducted in 41 countries. The mean IBS prevalence by country ranged from 3.3% in France (N=3 studies) to 31.6% in Nigeria (N=1 study). There was a significant difference in the mean prevalence among countries (p<0.0001). The prevalence, in individual studies, ranged from 1.1% in France71 and Iran94 to 35.5% in Mexico.97 Different studies from the same country yielded, in some cases, a broad range of results. For example, in the five studies included in this paper from Mexico, the prevalence rates were 4.4%,86 16.0%,84 16.9%,81 28.9%85 and 35.5%.97
Forty-two studies reported prevalence rates for IBS subgroups (IBS-D, IBC-C, etc). There was a difference in the prevalence of IBS-C among the regions, ranging from 12.7% for Asia, 13.6% for North America/Western Europe/Australia/New Zealand, 39.4% for Latin America, to 43.3% for the Middle East. The data were not sufficient to make other analyses of IBS by subtype.
Pooled rates
Table 4 shows the pooled prevalence rate for IBS per region. Pooled prevalence rates were higher in women than men (10.2% vs 8.8%), and prevalence rates were also higher in women than men in each region separately (table 4).
IBS prevalence, gender and age by geographical region
The highest prevalence rate was found in Latin America at 17.5% (95% CI 16.9% to 18.2%). Although there were many studies conducted in Latin America (N=17, 20.5% of all studies), the total number of participants in that region was low (N=12 805, 4.4% of all subjects). Thus, the studies in that region had substantially lower sample sizes than other regions of the world, with a mean in Latin America of 753, compared with 4491 for North America, Western Europe, Australia/New Zealand, 3999 for Asia and 3844 for the Middle East.
There was a statistically significant degree of heterogeneity among the geographical regions, using North America/Europe/Australia/New Zealand (table 5) as the reference region and confirmed using Latin America as the reference group (not shown) in two separate runs. The results of the univariate random-effects meta-regression for IBS by region appear in table 5.
Univariate random-effects meta-regression for IBS, by region with North America/Europe/Australia/New Zealand as the reference group
Discussion
We conducted a review of IBS prevalence in 83 general population or community-based studies conducted around the world and reported in multiple languages. We believe that the most significant finding of the present study is the extent of methodological variance in the included studies and the statistically significant degree of heterogeneity among them, not the calculated pooled global IBS prevalence or even the prevalence by geographical region. This result should not be surprising in light of the variation in sample size, setting, diagnostic criteria, method of data collection and overall research methodology.99 In fact, our results show very heterogeneous results when comparing IBS prevalence rates by regions and potential confounding factor, for example, method of data collection and diagnostic criteria used (table 4).
Compounding these factors are potential cultural differences in the reporting and interpretation of symptoms15 and the effect of inappropriate translation of study questionnaires.100 ,101
In this respect, our results are compatible with those reported by Lovell and Ford13 since they also found significant heterogeneity between studies in all of their statistical analyses, although they placed less emphasis on this finding. The review by Lovell and Ford included 80 articles, while the present study includes 83. Thus, the question might arise as to why the present study did not contain a much larger number of papers since it has more foreign language articles and could include articles published after the Lovell and Ford paper. We believe that there are several explanations for this outcome: (a) the time frame for the Lovell and Ford review was 1947–2011, while the time frame for the present study was much shorter from 1999 to 2013; (b) the Lovell and Ford review included studies with subjects from the age of 15 and above while the present one included studies with subjects from the age of 18 and above; and (c) the lower limit for the number of study subjects in the Lovell and Ford review was 50, while the lower limit in the present study was 100.
Prevalence rates are important for multiple reasons including (a) for epidemiologists and health economists—the distribution and burden of disease; (b) for clinicians—commonality of disease, probability of diagnosis and evaluation of treatment modalities; (c) for the pharmaceutical industry and regulators—incentive to develop new drugs; (d) for health policymakers—allocation of healthcare resources and research funding; (e) for clinicians, epidemiologists, medical anthropologists, etc—cross-cultural comparisons; and (f) for all—the satisfaction of intellectual and scientific curiosity.
There is a noteworthy lack of data from certain areas of the world. The African continent is almost completely unrepresented, and most studies conducted there5 ,102 were on select populations, which disqualified them from inclusion in the present review. Other regions that were seriously under-represented are Eastern Europe and the Arab world. Surprisingly, there were only two studies31 ,32 from the USA and Canada that were considered to meet the study inclusion criteria. We believe this is a consequence of a shift in emphasis from overall prevalence of IBS in the population to the association of IBS diagnosis with other characteristics such as age, race, ethnicity and socioeconomic status. Also, the absence of a centralised healthcare system could limit epidemiological studies in the USA.
Despite the heterogeneity of results, which makes it difficult to assess the global prevalence of IBS, it is clearly a prevalent disorder. The Lovell and Ford review is a landmark report on global IBS prevalence. Nevertheless, we believe that the results of the present study had an advantage in that it accessed more bibliographic depositories including languages other than English and had a large group of expert investigators who reviewed the literature in their own regions with expert translation at hand when needed. In fact, judging by its list of references, the Lovell and Ford study had less than half the number of articles that were published in a language other than English, compared with the present study, particularly in Spanish and Chinese. One of their conclusions was that there is a scant amount of published data from Central America (eg, Mexico). We have included several relevant studies from that region. Thus, the two reviews can be viewed as complementary, and similar conclusions can be drawn from them, especially relating to the heterogeneity of methodologies used in epidemiological studies of IBS, with the inherent implications for the interpretation of prevalence comparisons.
Another finding that is consistent throughout the studies is the predominance of females. Some individual studies, for example, from India, have shown higher rates among men than women. These studies are usually from a clinical setting and may reflect higher consulter rates among men than women in certain cultures.103–105 Although the prevalence of IBS among men is lower than women, it is still high in absolute terms, justifying and even mandating the inclusion of men in clinical trials.
The main strengths of this study include the rigorous design and search parameters, the exclusion of non-population-based and non-community studies, the composition of the expert team that reviewed all the papers by region, and the inclusion of many non-English-language papers, articles published in journals not included in major repositories and recent abstracts. The meta-regression analysis assured a pooled prevalence that combines separate population survey prevalence estimates to generate an overall combined estimate. The results of the heterogeneity analyses made it clear that we cannot infer that the overall pooled prevalence is a reliable statistic. Thus, the heterogeneity of the results precludes firm conclusions as to the global prevalence of IBS. However, we do not regard this as a study limitation; rather, it is a clear outcome of the study, which can drive future research.
A potential limitation of this study is that we did not have a formal requirement that the data search and extraction be conducted in duplicate. However, there were several safeguards in place. No article was accepted as eligible for review unless both the regional PI and the study PI (ADS) approved it. As mentioned above, in all cases of doubt the paper's eligibility was determined by joint review and, in some cases, papers originally considered eligible for the study were rejected. In addition, although duplicate searches were not mandated, in practice in most regions there was more than one investigator who determined the eligibility of the papers that they extracted and this was followed by the overall review of eligibility by the first author.
Other potential limitations include insufficient or absent data from some areas of the world. Again, since this reflects the actual situation it is less a limitation than an outcome of the study. The allocation of regions for data analyses could be somewhat problematic in that some regions may be more heterogeneous than others. An alternative approach that might reduce heterogeneity could be to assess IBS prevalence in pooled studies by diagnostic criteria or method of data collection, which we did in secondary analyses. However, many papers used more than one diagnostic criterion in the same study and some did not use the more established criteria at all, so this approach also has inherent difficulties. Another strategy could be to define smaller geographical regions, for example, to divide Asia and/or Latin America into smaller, more homogeneous subregions. However, the number of regions for analysis would increase and the number for each region would become small, in some cases to the point of obviating useful analyses. Decisions of this type always entail a trade-off, and the final decision is always likely to engender criticism.
In conclusion, given current methodological limitations, the goal of ascertaining a globally representative prevalence rate for IBS is likely to elude researchers for some time. However, this might actually be less important than determining reliable regional estimates of IBS prevalence and comparing these differences among regions in terms of variables such as diet, exposure to pathogens, healthcare practices, psychological variables, and prevailing cultural and religious beliefs. Studies with this more limited goal may advance our understanding of the pathophysiology of IBS and improve its medical management more effectively than a global estimate of IBS prevalence.
Acknowledgments
The authors would like to acknowledge the contribution of Drs Eamonn Quigley and Enrico Corazziari, who reviewed the draft manuscript and suggested important revisions.
References
Footnotes
Contributors ADS was involved in the study concept and design; acquisition of data; analysis and interpretation of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content; statistical analysis. DD was involved in the study concept and design; acquisition of data; critical revision of the manuscript for important intellectual content. SF, CG, UCG, KAG, J-YK, MS, WW and APSH were involved in the study concept and design; acquisition of data; analysis and interpretation of data; critical revision of the manuscript for important intellectual content. CM was involved in the acquisition of data; critical revision of the manuscript for important intellectual content. AB, MF and TF were involved in the analysis and interpretation of data; critical revision of the manuscript for important intellectual content; statistical analysis. All authors approved the manuscript for submission.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.