Article Text

Abstract
Background Seronegative villous atrophy (SNVA) is commonly attributed to coeliac disease (CD). However, there are other causes of SNVA. More recently angiotensin-2-receptor-blockers (A2RBs) have been reported as an association but data on SNVA have been limited to centres evaluating complex case referrals and not SNVA in general.
Objectives To provide clinical outcomes and associations in a large prospective study overseeing all newcomers with SNVA.
Design Over a 15-year period (2000–2015) we evaluated 200 adult patients with SNVA at a UK centre. A diagnosis of either seronegative CD (SNCD) or seronegative non-CD (SN-non-CD) was reached. Baseline comparisons were made between the groups, with 343 seropositive CD subjects serving as controls.
Results Of the 200 SNVA cases, SNCD represented 31% (n=62) and SN-non-CD 69% (n=138). The human leucocyte antigen (HLA)-DQ2 and/or DQ8 genotype was present in 61%, with a 51% positive predictive value for SNCD. The breakdown of identifiable causes in the SN-non-CD group comprised infections (27%, n=54), inflammatory/immune-mediated disorders (17.5%, n=35) and drugs (6.5%, n=13; two cases related to A2RBs). However, no cause was found in 18% (n=36) and of these 72% (n=26/36) spontaneously normalised duodenal histology while consuming a gluten-enriched diet. Following multivariable logistic regression analysis an independent factor associated with SN-non-CD was non-white ethnicity (OR 10.8, 95% CI 2.2 to 52.8); in fact, 66% of non-whites had GI infections. On immunohistochemistry all groups stained positive for CD8-T-cytotoxic intraepithelial lymphocytes. However, additional CD4-T helper intraepithelial lymphocytes were occasionally seen in SN-non-CD mimicking the changes associated with refractory CD.
Conclusions Most patients with SNVA do not have CD, in particular those who are not white. Furthermore, a subgroup with no obvious aetiology will show spontaneous histological resolution while consuming gluten. These findings suggest caution in empirically prescribing a gluten-free diet without investigation.
- CELIAC DISEASE
- SMALL INTESTINAL BIOPSY
- SMALL BOWEL DISEASE
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Seronegative villous atrophy (SNVA) is a diagnostic and therapeutic dilemma.
The causes of SNVA are vast but can be broadly grouped into seronegative coeliac disease (SNCD) and seronegative non-coeliac disease (SN-non-CD).
To date no study has systematically evaluated all newcomers with SNVA.
What are the new findings?
SNCD accounts for 31% of SNVA cases, with the remaining 69% due to SN-non-CD.
A positive human leucocyte antigen DQ2 and/or DQ8 status is seen in 61% of SNVA cases; its positive predictive value for SNCD is roughly 51%.
An independent risk factor associated with SN-non-CD is non-white ethnicity, suggestive of infective aetiology.
Overall, almost one in five patients with SNVA will have no identifiable cause; reassuringly, the majority of these will spontaneously normalise duodenal histology despite undertaking a gluten challenge.
How might it impact on clinical practice in the foreseeable future?
Individuals with SNVA should not be prescribed a gluten-free diet prior to further investigations. This is because of the wide differential diagnoses and that a subgroup with no obvious aetiology spontaneously normalises its duodenal histology while maintaining gluten intake.
Introduction
Coeliac disease (CD) affects 0.7–1% of the population and can be defined as a state of heightened immune response to ingested gluten in genetically susceptible individuals.1 ,2 All patients with CD carry the human leucocyte antigen (HLA)-DQ2 and/or DQ8 genotypes, although these alleles are also present in approximately 40% of the general population.3 A cast-iron diagnosis of CD can be made on the basis of demonstrating duodenal villous atrophy in the presence of serum IgA endomysial and/or tissue transglutaminase antibodies.4–6 This mode of presentation may be termed seropositive CD (SPCD) and following a systematic review accounts for approximately 93% of cases with villous atrophy,7 although some international groups have reported a lower prevalence (table 1).8–15
Studies where coeliac serology have shown low sensitivities in villous atrophy.
With this in regard, diagnostic and therapeutic dilemmas occur when villous atrophy is found in the context of negative coeliac serology.8–15 This clinical entity is termed seronegative villous atrophy (SNVA), the causes of which can be broadly grouped into CD or non-CD related.16 ,17 The reasons for seronegative CD (SNCD) include patients who have reduced gluten intake prior to investigations,18 lesser degrees of villous atrophy,13 selective IgA deficiency,19 immunosuppressive therapy or those with long-standing advanced CD within the spectrum of ulcerative jejunitis/enteropathy associated T cell lymphoma.15 The causes of seronegative non-CD (SN-non-CD) are vast ranging from infective, inflammatory, immune-mediated and drug-related.16 ,17 Such examples include autoimmune enteropathy,20 bacterial overgrowth,16 common variable immunodeficiency,21 Crohn's disease,22 gastroenteritis,23 giardiasis,24 ,25 graft versus host disease,26 HIV enteropathy,27 mycobacterium tuberculosis,25 ,28 peptic duodentitis±H. pylori,17 ,29–32 radiation enteritis,33 tropical sprue25 ,34 and Whipple's disease.35 Medications include non-steroidal anti-inflammatory drugs,36–38 azathioprine,39 methotrexate,40 mycophenolate mofetil41 and, most recently, angiotensin-2-receptor-blockers (A2RBs), in particular olmesartan.16 ,42–45 Finally, in some instances no unifying cause can be found and such patients are classified as idiopathic/unclassified sprue, the natural history of which is unknown.16 ,17
Studies attempting to evaluate diagnostic outcomes in SNVA have thus far been limited to a US centre overseeing complex case referrals from a wide catchment area.16 In such circumstances a high prevalence of SNCD and olmesartan-related enteropathy has been reported, the latter accounting for a striking 22% of SNVA cases.16 However, we hypothesise that this may not be reflective of SNVA as seen in routine GI practice. Furthermore, the clinical and histological phenotype of SNCD and SN-non-CD has not been established, nor how these entities contrast to the more conventionally seen SPCD. Such an evaluation may prove useful in understanding the spectrum of villous atrophy while also aiding clinicians towards the correct diagnosis when posed with the challenges of SNVA.
In light of this, the aim of our study was to provide a large comprehensive overview of all patients with SNVA seen at a UK centre over a 15-year period. Furthermore, we sought to identify differences between SNCD and SN-non-CD, using SPCD as controls.
Material and methods
Setting
This study was carried out between the time periods of 2000 and 2015 at the Royal Hallamshire Hospital, Sheffield, South Yorkshire, UK. The hospital is located in northern England and provides a secondary/tertiary-care service to a population of 500 000 people. The unit undertakes approximately 6000 oesophagogastroduodenoscopies per year.
Participants
Over the 15-year period we prospectively recruited 200 consecutive adult patients presenting with SNVA. The identification of SNVA was based upon duodenal biopsies showing villous atrophy yet with negative serum IgA endomysial and tissue transglutaminase antibodies from the outset.
As for our control group we recruited 343 patients with SPCD diagnosed within the same department between the years 2005 and 2011.
Histology
Throughout the study period the gastroenterology department had a policy of taking four duodenal biopsy specimens from the second part of the duodenum in those with suspected malabsorption. All duodenal biopsy specimens were fixed in buffered formalin and embedded in paraffin wax. Standard 3 μm thick sections at three levels were stained with H&E. The duodenal biopsies were routinely reported by one of a team of seven GI histopathologists. Agreement was then performed by one of two expert GI histopathologists reviewing SNVA biopsy samples (coauthors SSC and PV). Intraepithelial lymphocytosis was defined as >25 per 100 enterocytes. Villous atrophy was identified according to the Marsh-Oberhuber criteria, using the most severe lesion present: Marsh 3a (partial villous atrophy, PVA); Marsh 3b (subtotal villous atrophy, SVA); or Marsh 3c (total villous atrophy, TVA).46 ,47
The groups were also assessed for differences in immunohistochemistry based on CD3 pan-lymphocyte marker and specific CD8-T cytotoxic and CD4-T helper intraepithelial lymphocyte expression.
Coeliac serology
The initial panel of coeliac serology testing was IgA based, with endomysial antibodies detected by immunofluoresence on primate oesophagus sections from The Binding Site (Birmingham, UK). IgA tissue transglutaminase antibodies were assayed by using ELISA kits (Aesku Diagnostics, Wendelsheim, Germany), with titres less than or equal to 15 U/mL taken as negative. Of note, our immunology department does not automatically test for immunoglobulin or total IgA levels when processing coeliac serology. Rather, these have to be specifically requested as does IgG coeliac serology.
Baseline characteristics
We collected baseline characteristic data on the SNVA and SPCD cohorts. Taking into consideration the potential aetiologies and clinical manifestations this included age, gender, ethnicity, city residence, clinical symptoms, past medical history, current medication, grading of villous atrophy, HLA-DQ2/8 status, as well as laboratory parameters in the form of haemoglobin, ferritin, folate, vitamin B12, albumin, calcium, erythrocyte sedimentation rate and/or C reactive protein.
All the data (other than age) were inputted as categorical. This included converting numerical laboratory values into either within the normal or abnormal range, thereby overcoming the difficulties that arise over a 15-year period with departmental changes in testing kits and reference values.
Diagnostic workup for SNVA
All patients with SNVA were investigated in line with a systematic protocol, similar to that proposed by other expert groups, aiming to diagnose either SNCD or SN-non-CD (figure 1).16 ,17 It is important to bear in mind that, despite several international guidelines on CD, there is no consensus on how to approach subjects with SNVA.4–6 Some physicians may suggest a trial of a gluten-free diet (GFD) followed by clinical and histological reassessment.4–6 However, this can be fraught with uncertainty given that up to 32% of patients with SN-non-CD report favourable clinical response to a GFD.17 Furthermore, mucosal recovery in adult CD is slow with histological abnormalities often persisting beyond 2–5 years and in some cases never normalising.48–50 Therefore, adopting such an approach in SNVA could potentially lead to unnecessary delays given the wide differential diagnoses. Hence, patients with SNVA in our study were asked to continue a gluten-containing diet until investigations were complete and a firm diagnosis reached. This approach is also useful in that it allows progression of villous atrophy and detectable serum antibodies in some cases of SNCD.51

Stepwise proposed algorithm used to investigate and diagnose causes of seronegative villous atrophy (SNVA). GFD, gluten-free diet; HLA, human leucocyte antigen; SNCD, seronegative coeliac disease; SN-non-CD, seronegative non-coeliac disease.
Mortality
At the end of December 2015 mortality rates were calculated. Overall survival was calculated in years and defined as the time from diagnosis to death. Surviving patients were censored at the time of last follow-up.
Statistics
Statistical analysis was carried out using SPSS V.21.0 software (SPSS, Chicago, USA), with significance set at a p value of <0.05. A complete-case analysis approach was adopted to address the limited data which were missing completely at random. Categorical variables were summarised by descriptive statistics, including total numbers and percentages, with comparisons between groups performed using the χ2 test or Fisher's exact test. Normally distributed continuous variables were summarised by mean and SD with comparisons between groups performed using the unpaired Student's t-test. We performed dichotomous logistic regression between the SNCD and SN-non-CD groups using a forward stepwise method with a p value of <0.1 for entry into the analysis with all variables available for inclusion into the model. Finally, overall survival was analysed using Kaplan-Meier curves and significance compared using the log-rank test.
Results
Characteristics of SNVA
The baseline characteristics of the 200 patients with SNVA are provided in table 2. The patient cohort comprised 83% (n=166) who were residents of Sheffield and thus classed as secondary-care referrals. There were 17% (n=34) who were referred from another city for a tertiary-care opinion. The mean age was 51.2 years, with 63.5% (n=127) female and 82.5% (n=165) of white ethnicity.
Baseline characteristics of SNVA subjects and SPCD controls
The most frequently reported clinical symptoms were diarrhoea (60%, n=120), abdominal pain (49%, n=98), weight loss (35.5%, n=71) and bloating (31%, n=62). Autoimmunity was present in 18.5% (n=37) of cases, with 3.5% (n=7) also having a family history of CD. A recent history suggestive of gastroenteritis was elicited in 11.5% (n=23) of cases. The use of A2RBs was seen in 4% (n=8), of which 7 were on candesartan and 1 was on irbesartan; no patient was taking olmesartan.
Blood tests revealed anaemia in 30.8%, with associated haematinic deficiencies ranging from 16.1% to 39.5%. A raised erythrocyte sedimentation rate and/or C reactive protein was present in 26.6% of patients. The presence of positive HLA-DQ2 and/or DQ8 was seen in 61.1% (n=118/193).
Finally, histological grading of duodenal biopsies showed intraepithelial lymphocytosis in 88.5% (n=177), with the majority of patients found to have PVA at 79.5% (n=159). In contrast, SVA was seen in 12.5% (n=25) and TVA in 8% (n=16).
Aetiology of SNVA
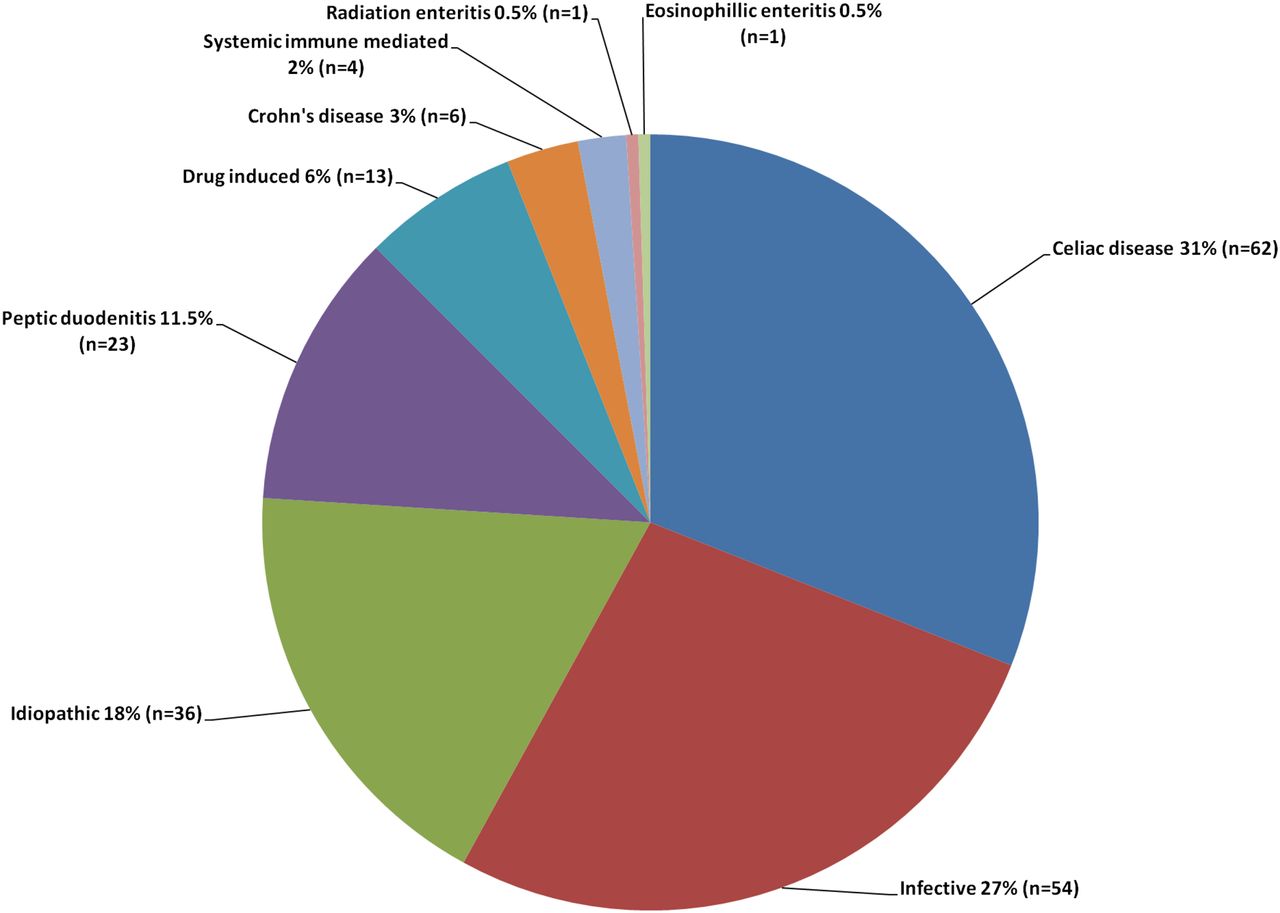
Following systematic evaluation of 200 SNVA cases, we diagnosed SNCD in 31% (n=62) of cases with the remaining 69% (n=138) due to SN-non-CD. The breakdown of all causes is shown in figure 2.
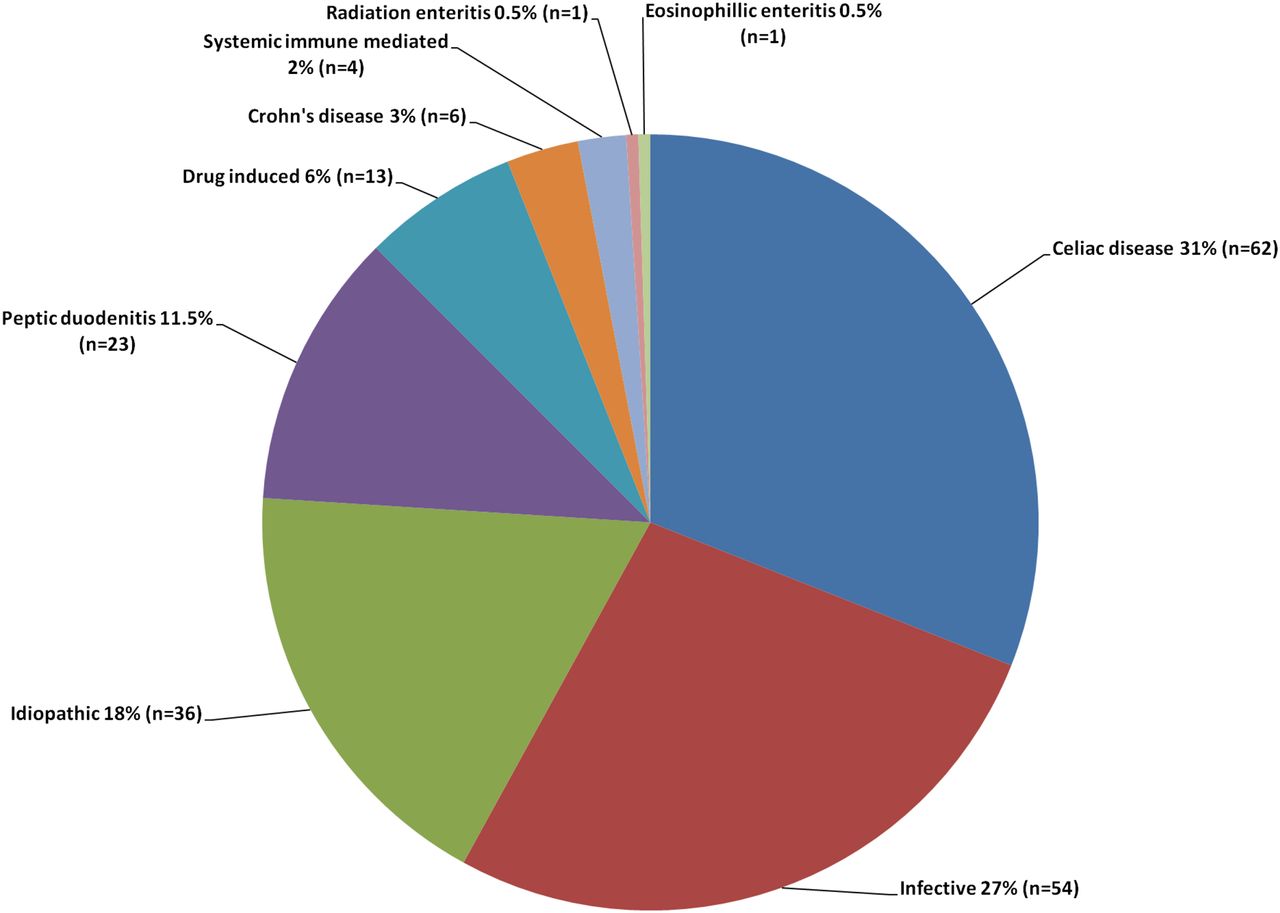
Causes of seronegative villous atrophy (SNVA) at a UK centre (n=200).
In the 62 cases identified as having SNCD, 14 were diagnosed with relative ease based on (1) selective IgA deficiency but with raised IgG coeliac serology (n=9, three also had associated first degree family history of CD), (2) first degree family history of CD alone with subsequent response to a GFD (n=4) and (3) dermatitis herpetiformis (n=1). The other 48 patients were diagnosed with SNCD on the basis of having positive HLA-DQ2 and/or DQ8 status, no alternate cause found, persisting villous atrophy following a gluten rechallenge, with subsequent clinical±histological response to a GFD.
A wide range of aetiologies was established in the 138 SN-non-CD cases, commonly infective, medication-induced and inflammatory in nature. In total, there were 54 cases attributed to an infection. This included Helicobacter pylori induced duodenitis alone (n=21) or in conjunction with Mycobacterium tuberculosis (n=2), Mycobacterium avium intracellulare (n=1) and HIV (n=1). Other causes included viral gastroenteritis based upon clinical history (n=7), giardiasis (n=6), small bowel bacterial overgrowth (n=4), HIV enteropathy (n=2), ascariasis (n=2), Mycobacterium tuberculosis (n=2), tropical sprue (n=2), Campylobacter (n=1), candidiasis (n=1), Whipple's disease (n=1) and Mycobacterium avium intracellulare (n=1). There were 13 cases which occurred as a result of medication; 9 due to non-steroidal anti-inflammatory drug-related duodenitis, and the others were a case each related to methotrexate, mycophenolate mofetil, irbesartan and a possible association with candesartan. There were 23 cases of non-specific peptic duodenitis, 6 cases of Crohn's disease and 4 cases due to systemic immune-mediated disorders which included a case each of sarcoidosis, graft versus host disease, autoimmune enteropathy and common variable immunodeficiency. There was a case each of radiation enteritis and eosinophilic enteritis. Following appropriate treatment these showed clinical and histological improvement.
Finally, in 36 cases of SN-non-CD, despite extensive investigations, we were unable to elicit any cause and these patients were labelled as idiopathic/unclassified sprue. Interestingly, 72% (n=26/36, 11 of whom were HLA-DQ2/8 positive) had spontaneously normalised their duodenal biopsies when rechallenged with gluten, suggesting transient villous atrophy. This was seen on average 9 months after the index biopsy had shown villous atrophy. Of the remaining 10 cases, all HLA-DQ2/8 negative, 4 required immunosuppressive therapy for persisting unexplained villous atrophy with the other 6 either lost to follow-up or refusing further endoscopic investigations given their clinical stability.
Risk factors for diagnostic outcomes
Univariate analysis comparing the SNVA subgroups and SPCD controls are shown in table 2. In summary, the SNVA cohort was older at the time of presentation and more likely to present with symptoms of diarrhoea, abdominal pain, nausea and weight loss.
In contrast, subjects with SPCD or SNCD were more likely than SN-non-CD to have autoimmunity, family history, and HLA-DQ positivity; however, the positive predictive value of HLA-DQ2/8 for SNCD in the context of SNVA was only 51% (n=60/118). There was also a significant trend towards lesser degrees of villous atrophy from SPCD towards SNCD and then SN-non-CD.
Factors significantly associated with SN-non-CD included non-white ethnicity, dyspepsia, negative HLA-DQ status, lack of intraepithelial lymphocytosis/crypt hyperplasia and hypoalbuminaemia. Multivariable logistic regression analysis of the SNVA cohort showed that an independent factor associated with a diagnosis of SN-non-CD was non-white ethnicity (OR 10.8, 95% CI 2.2 to 52.8, p=0.003). Indeed, 23 of the 35 (66%) non-white subjects presenting with SNVA had a GI infection, commonly H. pylori induced duodenitis; table 3. Only 2 of 35 (5.7%) non-whites with SNVA had SNCD compared with 60 of 165 (36%) whites.
Characteristics and diagnostic outcomes in non-whites with SNVA seen at a UK centre
Immunophenotyping of intraepithelial lymphocytes
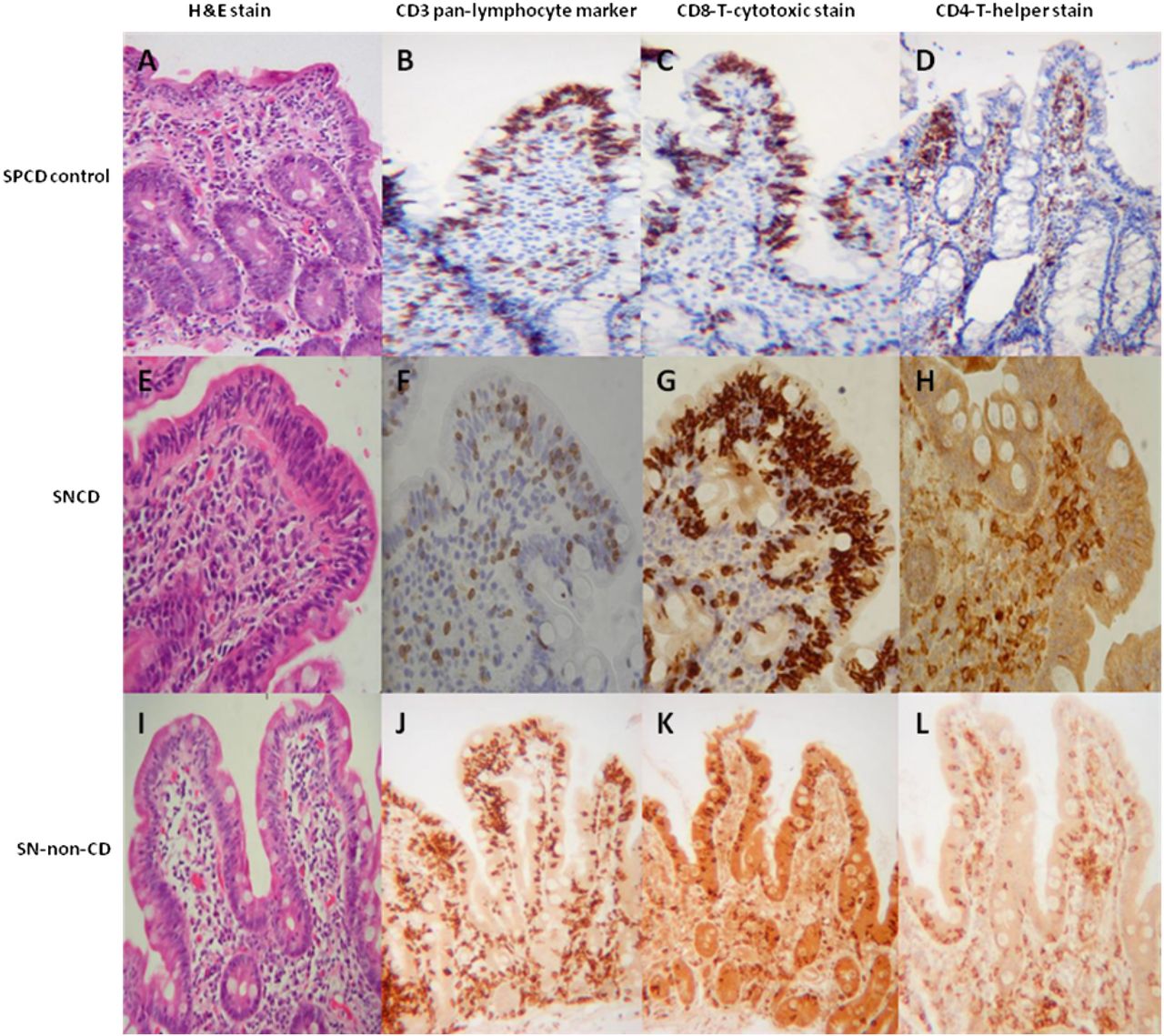
Immunohistochemistry was performed in 19 SNVA cases of which 14 were SN-non-CD and 5 SNCD. Both groups showed CD8-positive T cytotoxic intraepithelial lymphocytes, similar to that seen in SPCD controls. However, four cases of SN-non-CD also contained CD4-positive T helper cells among the intraepithelial lymphocytes; these cells are associated with refractory CD within the context of CD but in other contexts, such as GI infection, they are a normal component of the immune response (see figure 3 and online supplementary figure S1).

Plates A to D: SPCD control. A white female presenting with anaemia and positive serum IgA endomysial antibody. Duodenal biopsy demonstrated subtotal villous atrophy when stained with haemotoxylin and eosin (H&E). It can also be seen that there is an increased number of intra-epithelial lymphocytes stained by the pan-lymphocyte marker CD3. Furthermore, staining of antibodies against different intraepithelial lymphocyte phenotype revealed that they are all of the CD8-T-cytotoxic stain and not CD4-T-helper cells. This is the classical pattern of coeliac disease. Plates E to H: SNCD patient. A white female presenting with diarrhoea. Serum IgA endomysial antibodies were negative but duodenal biopsy showed subtotal villous atrophy. There were increased intraepithelial lymphocytes noted following CD3 pan-lymphocyte stain, which on immunophenotypic differentiation revealed CD8-T-cytotoxic cells but not CD4-T-helper cells. Her HLA-DQ2 was positive, no alternate cause was found, and she responded to a gluten-free diet. Plates I to L: SN-non-CD patient. Bengali female presenting with diarrhoea, anaemia, night sweats and fevers. Her serum IgA endomysial antibody was negative but duodenal biopsy showed partial villous atrophy with raised intraepithelial lymphocytes. She stained positive for CD8-T-cytotoxic cells but also for CD4-T-helper cells. This could have been mistaken for refractory coeliac disease. However, her HLA-DQ2/8 genotype was negative and on microbiology assessment her duodenal sample revealed mycobacteria (supplementary Figure S1). She was commenced on anti-tuberculosis therapy. Duodenal histology of seronegative villous atrophy (SNVA) and seropositive coeliac disease (SPCD) control. HLA, human leucocyte antigen; SNCD, seronegative coeliac disease; SN-non-CD, seronegative non-coeliac disease.
supplementary figure
Survival analysis
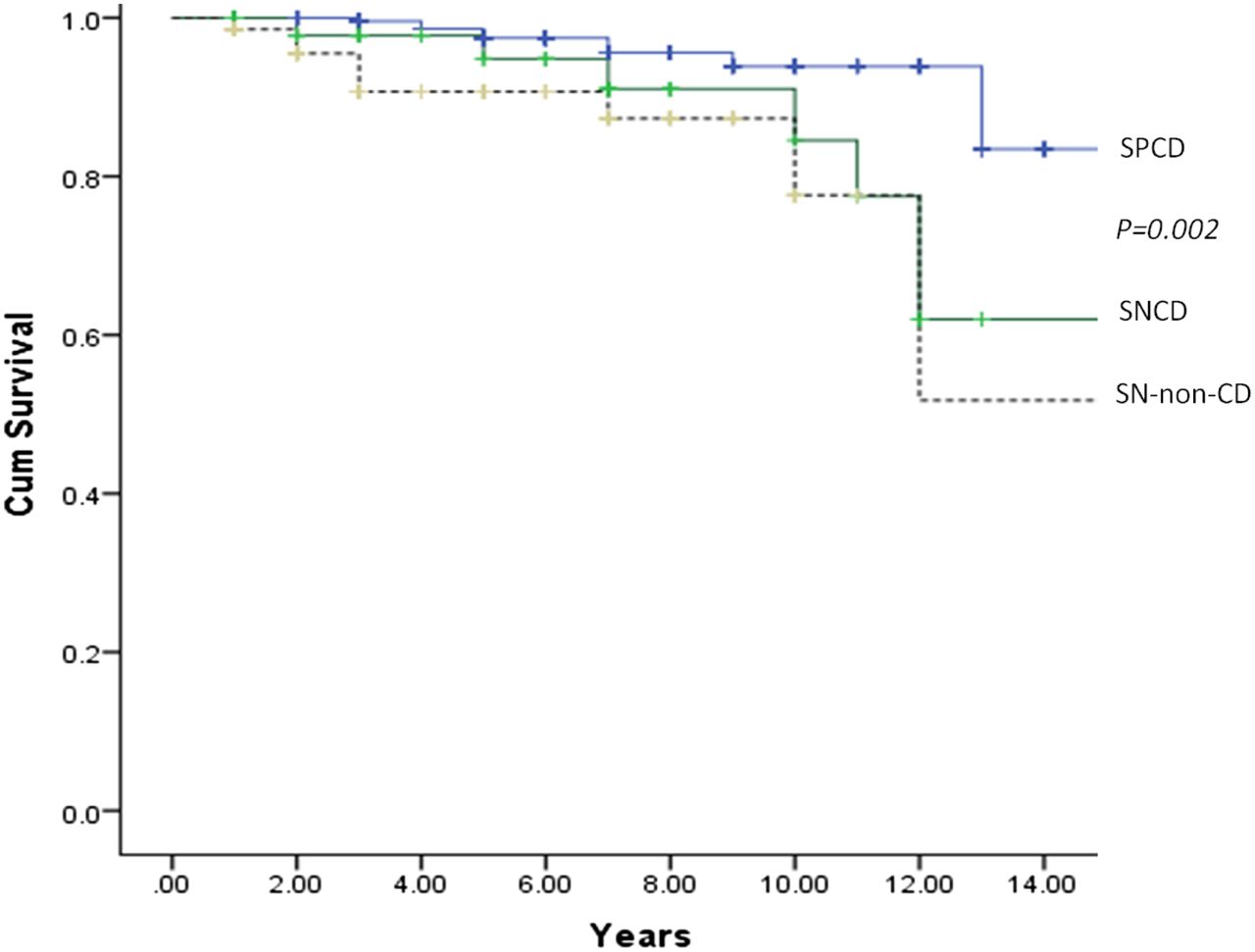
There have been 19 deaths within the 200 SNVA cohort, of which 7/60 (11.2%) were in the SNCD group and 12/138 (8.7%) in the SN-non-CD group. In comparison there have been 11/343 (3.2%) deaths in the SPCD controls. On Kaplan-Meier analysis there were no statistical differences in estimated survival between the SNVA groups although this was less favourable compared with SPCD (figure 4: log-rank p=0.002).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier estimated survival curves for seronegative villous atrophy (SNVA) and seropositive coeliac disease (SPCD) controls. SNCD, seronegative coeliac disease; SN-non-CD, seronegative non-coeliac disease.
Discussion
Main findings
We believe that our findings represent a major conceptual change in the understanding and management of SNVA. Having used a systematic clinical algorithm we have shown that SNCD accounts for 31% of SNVA cases, with the remaining 69% due to SN-non-CD related causes. Furthermore, HLA-DQ2 and/or DQ8 genotype was present in 61% of SNVA cases, with a positive predictive value of only 51% for a diagnosis of SNCD. This is not surprising given that these alleles are common as seen in approximately 40% of the general population.3
Importantly, we have identified that non-white ethnicity is a risk factor to alert clinicians to the possibility of SN-non-CD, in particular with regards to an infective aetiology. These findings are the first to be reported outside of the tropics and in a Western society.25 The clinical relevance of this also expands to the USA where results from a national pathology database have identified that among patients undergoing duodenal biopsies it is those from the Punjab region of India that constitute the ethnic group with the highest prevalence of villous atrophy.52 It remains to be determined whether such patients had SNVA given that the US National Health and Nutrition Examination survey has found positive coeliac serology to be rare among non-whites.1
In addition, in almost one in five cases of SNVA no identifiable cause was found although, reassuringly, the majority spontaneously normalised duodenal histology while being investigated on a gluten-enriched diet; had these patients been commenced on a GFD at the outset instead, they would have erroneously been diagnosed with SNCD and wrongfully subjected to a lifelong, restrictive diet. This, along with previous studies showing an empirical trial of a GFD to be a poor predictor of CD,17 further supports the notion that clinicians must not start a GFD in SNVA until investigations are complete and a firm diagnosis of SNCD has been established.
Finally, differences in survival outcomes between SNVA and SPCD controls were noted. A recent English study involving more than 10 000 patients with CD found no major excess risk of cancer, digestive disease or respiratory disease related or cardiovascular mortality compared with the general population.53 However, it is recognised that those with SNCD tend to be older and run a more advanced disease course than SPCD.15 With regards to SN-non-CD this entity has a number of heterogeneous disease associations (ie, HIV, tuberculosis, common variable immunodeficiency) which are associated with poorer outcomes.
Strengths and limitations
The main strength of this study is that it is the largest and most comprehensive to date, having prospectively evaluated 200 consecutive adult patients with SNVA at a UK secondary/tertiary-care centre over a 15-year period. The cohort studied included both inner and outer city referrals. Moreover, systematic and rigorous investigations were performed using testing modalities available among most gastroenterology departments. We therefore feel that our findings can be used as a benchmark and generalised to other physicians seeing similar patients.
However, our study does have several limitations. First, we do not perform serum deamidated gliadin peptide antibodies or intestinal coeliac antibody deposits, both of which are relatively novel markers and can aid towards the diagnosis of CD.54–56 Second, it may also be perceived that by identifying and including IgA deficient patients who were subsequently found to be IgG coeliac serology positive (n=9) is a weakness in that this should be common knowledge. However, our findings are those of real life practice and would be supported by other groups who have shown that inadequate evaluation of IgA deficiency occurs frequently when testing for CD.57 Nevertheless, had we excluded such patients from our analysis then the prevalence of SNCD would have been 27.7% (n=53/191) instead of the 31% (n=62/200) stated. Third, we have unanswered questions in those in whom no cause was found (so called idiopathic/unclassified sprue) but spontaneously normalised duodenal biopsies while consuming high-dose gluten. A recent case series has highlighted that self-limiting enteropathies can occur in the context of GI infections,23 which raises the possibility that our patients may have experienced a similar insult although this was not recalled from their clinical history nor isolated from stool cultures. Furthermore, these individuals had their repeat biopsy performed on average 9 months after the index case which had shown villous atrophy. We do not know when their histology started improving and at what exact time point it had normalised. Had the biopsies been performed earlier then these patients may still have had persisting villous atrophy and, in those with the correct HLA-DQ genotype, subsequently categorised as having CD. However, our study was performed pragmatically and is a reflection of routine outpatient clinical practice. Nevertheless, future research studies should aim to perform biopsies at sequential time points. Finally, of those carrying the HLA-DQ genotype it could be hypothesised that these individuals may still belong to the spectrum of CD and have simply experienced an unexplained GI insult transiently manifesting as SNVA but having not yet reached the cumulative threshold required for CD to become apparent.58 Hence, longitudinal follow-up data are now required in this particular group.
Other studies
To our knowledge only one other study has evaluated diagnostic outcomes in SNVA.16 This was performed by the New York group who evaluated 72 complex case referrals of SNVA over a 10-year period. The investigators found that 22% (n=16/72) of their SNVA cases were due to olmesartan-related enteropathy.16 This novel association has generated substantial interest and is of importance given its presentation may be that of a severe form of enteropathy necessitating hospitalisation for the management of intractable diarrhoea, weight loss, dehydration, hypotension, acute renal failure and metabolic acidosis.16 ,42–45 Yet, these findings are in contrast to ours where the use of A2RB was seen in 8 of 200 SNVA cases, with A2RB a responsible cause for enteropathy in two patients; overall prevalence of A2RB enteropathy being 1% (n=2/200). In the other six patients we found an alternate aetiology for SNVA with patients well maintained on their A2RB; these include CD (n=2), giardiasis (n=1), eosinophilic enteritis (n=1), small bowel bacterial overgrowth (n=1) and loss to follow-up (n=1). Given that A2RBs, including olmesartan, are dispensed in the UK, the discrepancy in the results raises two main points. First, the high prevalence of olmesartan-related enteropathy reported elsewhere may not be reflecting SNVA in general but rather groups overseeing and presenting the outcomes of cases referred from wide catchment areas with presumed ‘poorly responsive/refractory CD’.16 In fact, the initial case series highlighting this association came from the Mayo Clinic where 22 patients with olmesartan-related enteropathy were reported following referrals from 16 US states over a 3-year period.42 Following on, a nationwide multicentre French survey identified 36 patients with olmesartan-related enteropathy.44 Most recently, the crude incidence rates of olmesartan and other A2RB enteropathy in France has been calculated at 5.6 and 1.8 per 100 000 patient years, respectively.45 These findings suggest that olmesartan-related and in particular other A2RB-related enteropathies are rare adverse events. Second, despite the growing awareness of A2RB-related enteropathy clinicians must still remain vigilant that on occasions A2RBs will merely be innocent bystanders and an alternate aetiology for SNVA will be found.
Conclusion
This large UK centre study provides a prospective, systematic and clinically pragmatic evaluation of SNVA. We have shown that most patients with SNVA do not have CD or A2RB enteropathy. Further, a subgroup in whom no cause is found will show spontaneous histological resolution while still consuming gluten and this phenomenon requires further evaluation. The presence of non-white ethnicity was found to be a factor predicting a non-coeliac cause, in particular infective aetiology.
References
Footnotes
Contributors IA designed the study, recruited patients, collected data, performed statistical analysis, wrote and edited the manuscript. MFP, J-HB, VK, JCW, DP, PV collected data. SSC collected data, performed statistical analysis, and edited the manuscript. PHG edited the manuscript for important intellectual content. DSS conceived and designed the study, recruited patients, collected data, and edited the manuscript. All authors reviewed and approved the final version of the manuscript.
Competing interests None declared.
Ethics approval The initial ethics was from the South Sheffield Research and Ethics Committee, then the Humber Research and Ethics Committee 09/H1304/69. The study was also registered under Sheffield Teaching Hospitals audit number 2954.
Provenance and peer review Not commissioned; externally peer reviewed.