Article Text

Abstract
Patients with primary biliary cholangitis (PBC) can be stratified into low-risk and high-risk groups based on their response to treatment. Newly published guidelines from the British Society of Gastroenterology suggest low-risk patients can be managed substantially in primary care. This represents a shift from existing practice and makes assumptions about service capacity and the willingness of both patients and health care practitioners (HCPs) to make this change. The aim of this paper is to identify possible barriers to the implementation of these new care pathways through review of the PBC-specific literature and by identifying the experiences of patients and HCPs managing a different condition with comparable patients and disease characteristics. Searches of MEDLINE, CINAHL and EMBASE were undertaken. Within the existing PBC literature there is little data surrounding stakeholder perspectives on place of care. Review of the breast cancer literature highlights a number of barriers to change including primary care practitioner knowledge and work load, communication between healthcare settings, and the significance of the established doctor–patient relationship. Further research is needed to establish the extent to which these barriers may surface when changing PBC care pathways, and the actions required to overcome them.
- primary biliary cirrhosis
- primary care
- health service research
- cholestatic liver diseases
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Primary biliary cholangitis (PBC), formerly known as primary biliary cirrhosis, is a chronic autoimmune liver disease. The incidence of PBC in the UK is 32.2 per 100 000,1 with approximately 20 000 people presently affected. Incidence is higher in females compared with males (10:1) and in the fifth and sixth decade of life such that a woman over 40 years of age has a 1/1000 chance of having this condition.2 While early natural history studies suggested that life expectancy from time of diagnosis was less than 10 years,3 this is no longer true. Increasing understanding of the pathophysiology of the disease, along with the ability to diagnose PBC earlier in its course, and the widespread use of ursodeoxycholic acid (UDCA) has led to the recognition that, for many patients, PBC is a chronic disease but not life limiting. The name changes from ‘primary biliary cirrhosis’ to ‘primary biliary cholangitis’ was adopted into use by clinicians, researchers and patients in 2015 to reflect the emerging evidence that only a minority of patients go on to develop cirrhosis and end-stage liver failure.
Patients with PBC can be categorised or ‘stratified’ into two groups (responders or non-responders) based on whether or not there is an improvement in biochemical parameters following 12 months of treatment with UDCA. Those who respond to treatment with UDCA (between 60% and 70% of all patients) do not go on to develop progressive disease and have a transplant free survival similar to the general population.4–7 Up until a few years ago, in the absence of second line treatment, those who failed to respond to UDCA were at risk of progression to end stage liver disease and liver transplantation, with younger patients and males with PBC over-represented in this group.8 However, following recent positive outcomes in trials, obeticholic acid (OCA), a Farsenoid X receptor agonist has been approved by the National Institute for Health and Care Excellence (NICE) for the treatment of patients who have had an inadequate response to treatment with UDCA or were unable to tolerate UDCA.9 However, despite the availability of effective treatment, there is no cure for the disease and even for those who respond, life-long treatment with UDCA is still required and patients will requirement regular follow-up.
Reflecting both the increased understanding of the natural history of PBC and the availability of second line therapy, recently published guidelines from the British Society of Gastroenterology10 highlight the importance of formal risk stratification for all patients at 1-year postdiagnosis with management of treatment non-response or high-risk patients necessitating discussion with specialist services for consideration of OCA or clinical trials. For those with low-risk disease, while long-term treatment and follow-up are required, it has been suggested that this does not necessarily need to take place in a hospital-based setting and there is the opportunity for an increased role for primary care services in the long-term care of these patients. These recommendations are echoed in the recent guidelines from the European Association for the Study of Liver Disease.11
New models of care for management of chronic liver disease as a whole are essential and timely. In contrast to other countries in Western Europe, rates of liver disease are increasing in the UK; over 600 000 people are known to have liver disease with 10% of these having cirrhosis and liver disease mortality has increased by 400% over the last 40 years.12 The Lancet Commission on Liver Disease has highlighted the numerous challenges currently faced by the National Health Service (NHS) and by patients including inequalities in service provision (the so-called ‘postcode lottery’). The Commission’s recommendations included the need to improve access to specialist care and services for those most in need as well as increasing involvement from primary care and community services.12
However, changing patterns of established care requires ‘buy in’ from all users of the pathways: patients, stakeholders, and health care practitioners (HCPs) in primary, secondary and tertiary settings. This requires an appreciation of the various user’s perspectives of current care, of the possible impacts any changes will have on them as new pathways are introduced, and in turn the identification of potential barriers to change and the facilitators required for these to be overcome. This paper seeks to identify what is already known about these factors in the currently available PBC literature. In addition, we also review the existing literature around patient and HCP perspectives on follow-up in a comparable condition where recent changes in management parallel the proposed evolution of PBC in order to gain insights that may be relevant to reforms in PBC care.
Methods
Review of the PBC literature
A scoping review was chosen with the goal of establishing the type and breadth of literature available.13 The potential remained to perform a systematic review if the scoping study revealed a large body of relevant literature. Using the framework set out by Arksey and O’Malley,14 the following stages were undertaken: (1) identification of the research question, (2) identification of relevant studies, (3) selection of studies, (4) charting of the data (5) collation, summarising and reporting of results.
The research question was divided into two parts. (1) What is the breadth and type of literature available looking at the perspectives of patients and clinicians on all aspects of PBC and its management? (2) Is there existing data looking specifically at how patients and clinicians view the role of primary care in the management of PBC?
A search of three electronic databases: MEDLINE, CINAHL and EMBASE was carried out. A schematic of the study selection process is shown in figure 1. The following search terms were used: Primary biliary cirrhosis OR primary biliary cholangitis AND quality OR experience OR perception* OR perspective* OR attitude* OR expectation* OR understand* OR view*. Eleven hundred and fifty-one distinct citations were identified by the initial database searches with 24 included in the final analysis. In order to establish whether there were any additional resources available but not captured by the initial electronic database searches, a review of all the reference lists from the 24 texts was undertaken; this yielded one further article. A search of the grey literature using Open Grey (http://www.opengrey.eu) using the search terms ‘primary biliary cirrhosis’ and ‘primary biliary cholangitis’ returned 18 and five citations, respectively. None were relevant to the research question. The key characteristics and emerging research themes of the 25 studies are summarised in table 1.
Summary of research themes in PBC addressing patient and physician perspectives on disease

Study selection process for primary biliary cholangitis.
Choosing a comparable condition
A number of factors were deemed to be of relevance when selecting a comparable condition including the demographics of the patient population, availability of clear stratification parameters and the need for ongoing but minimal input long-term follow-up for low-risk groups. Possible conditions considered included other forms of liver disease, other chronic diseases (including autoimmune and non-autoimmune) and malignancies. Breast cancer satisfied the criteria (see table 2); it is mainly a disease of older females, patients are stratified after primary treatment into those who have achieved remission and those who have not responded, and even where remission has been achieved, there continues to be a need for a form of life-long input for responders that does not necessarily require specialist input.15 A number of other parallels are also evident, including the ongoing psychological morbidity, and symptoms that may persist despite remission being achieved. In addition, issues around how best to follow-up patients who have undergone curative treatment remain a source of debate.16 NICE guidelines on breast cancer from 2002 stated that all patients should be followed up for a minimum of 3 years (although they did not state how frequently patients should be seen) before care could be transferred back to primary care.17 A systematic review of the breast cancer literature in 200718 identified seven randomised controlled trials which compared different forms of follow-up care both in terms of frequency of review and appropriate healthcare professional. Overall, they found no difference in recurrence rates, survival or quality of life. The updated NICE guidelines in 200919 reflect the existing research and recommend patients decide how they would like to be followed up after primary treatment is completed with options including primary care, secondary care or shared care.
Comparison of primary biliary cholangitis and breast cancer
Review of the breast cancer literature
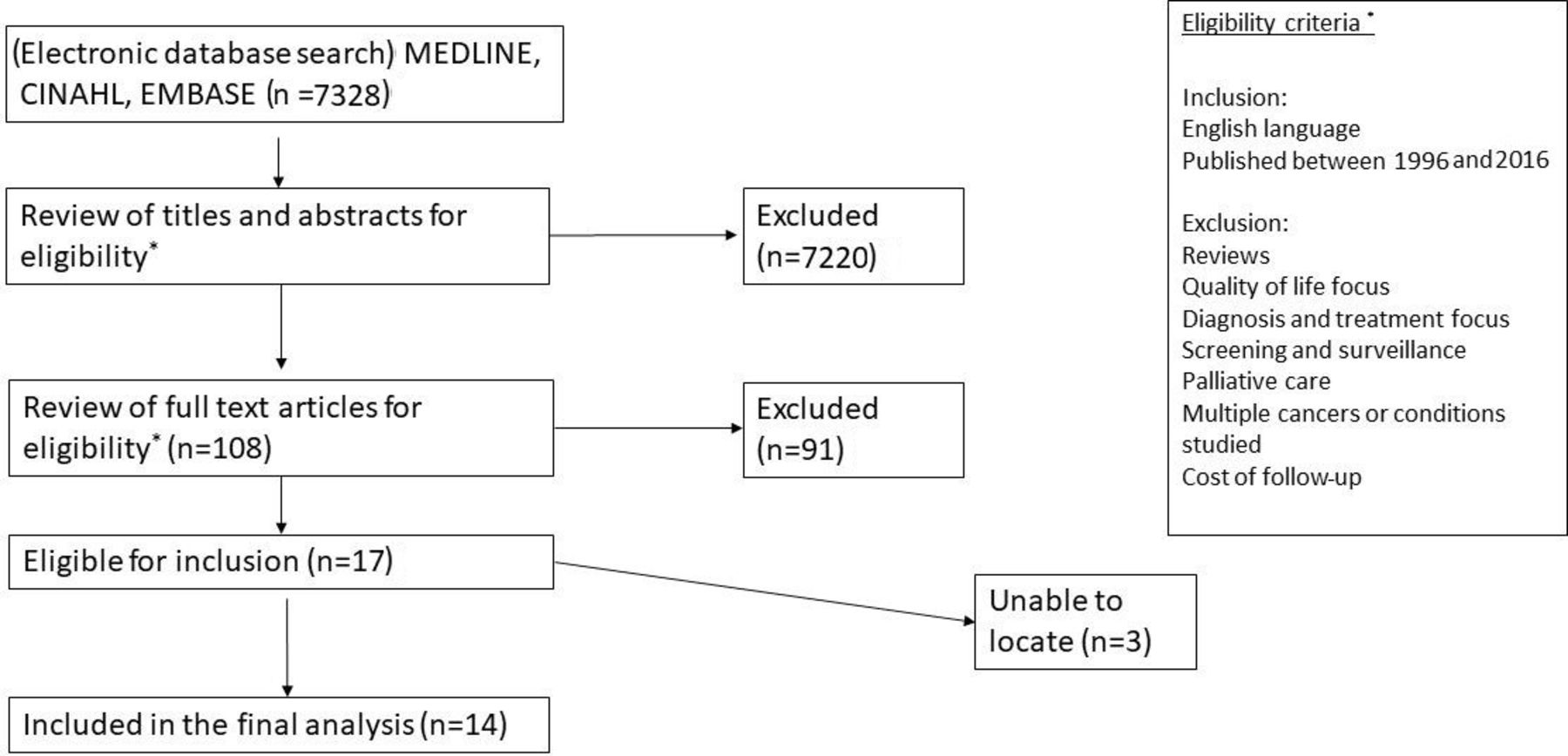
The second scoping exercise again followed the Arksey and O’Malley structure.14 As the topic of long-term follow-up in breast cancer survivorship has been widely studied, the goal of this review was to (1) gain an overview of the commonly occurring themes in this literature and (2) identify barriers to follow-up in primary care which may have potential relevance in PBC. An electronic database search was undertaken using the same three databases. A schematic of the sample selection process is shown in figure 2. The following search terms were used: breast cancer OR breast carcinoma OR breast neoplasm AND perspective* OR opinion* OR view* OR attitude* OR experience* or perception* AND discharge OR ‘follow-up’ OR ‘primary care’ OR ‘secondary care’ OR hospital* OR special* OR general practice*. A date limit was set to cover 1996–2016 in order to capture data relevant to recent changes in breast cancer follow-up strategies between the 2002 and 2009 NICE guidelines and studies undertaken following this change in practice. Review of the reference lists from relevant articles did not identify any further relevant citations within the specified date range. For each study the following data were extracted: authorship, publication date, location, population type, sample size and barriers to primary care follow-up.
{kind=link}
{kind=link}
Study selection process for breast cancer.
Results
PBC literature
Twenty-five studies identified from the PBC literature were included in the final analysis (table 1). Seventeen quantitative studies were identified,20–36 four qualitative,37–40 two mixed methods study,41 42 one literature review43 and one patient narrative.44 Of these studies, 24 focused on the patient perspective only, with one looking at both patient and physician perspectives.31 The majority of the studies focused on symptoms and quality of life. Of those that took a qualitative or mixed approach, one study looked specifically at the impact of fatigue,37 one at the experience of receiving a diagnosis40 and the other at stigma associated with PBC.42 Two studies explored the experience of living with PBC.39 41
While no studies directly addressed issues surrounding follow-up care and the role of primary, secondary and tertiary care, there were a number of emerging themes that are likely to be of relevance when looking at the impact of changes in the structure of care. Montali et al39 identified the theme of ‘delegitimisation’ and how, when patients look well (as is often the case in PBC), the impact of their disease is minimised by familial and social contacts. Discharge from specialist care to the primary care setting may further impact these perceptions both for the patient and their social contacts. The significance of the disease may be perceived as lesser when care is transferred to practitioners who may be seen as being less ‘specialist’ or ‘expert’.40 44 In addition, the stigma experienced by patients may also be influenced by new changes in care structure. A study looking at posts on an internet forum for patients with PBC revealed that a number of posts were related to stigma38 and when directly asked many patients reported that they felt a degree of stigma associated with their disease.42 This stigma seemed to stem not specifically from the diagnosis of PBC itself but with the associations between liver disease and cirrhosis with drugs and alcohol. Of note, this stigma was not just related to the perception of lay people but also to non-specialist HCPs.
Breast cancer literature
From the breast cancer literature, 14 papers were included in the final analysis (table 3). Quantitative methods were used in eight of the studies,45–52 five used qualitative methods53–58 and one mixed methods study58 was identified. Nine studies looked at the views of the patient population,46–48 50 53–57 six included primary care clinicians46 48 49 55 57 58 and five included specialists (comprising surgeons, oncologists and nurses).45 51 52 55 56
Summary of themes identified in breast cancer literature
Barriers to primary care follow-up identified included lack of knowledge among primary care physicians which was a recurrent theme among patients,50 53 54 57 specialists45 51 56 and primary care physicians themselves.49 57 58 Allied to this concern was a fear that recurrence could be missed which was expressed by both primary care and specialist care55 with some primary care clinicians expressly mentioning medicolegal concerns.46 55 There was an association between cases where patients had experienced delays at the time of initial diagnosis and reduced confidence in their primary care practitioners ability to provide adequate follow-up.57 When asked to rate their survival outcomes in different healthcare settings, patients felt that their chance of survival long term was higher if they were followed up by a specialist.47
In terms of practical aspects of care, both patients and doctors felt that primary care clinicians are already overworked,46 49 53 that communication between primary care and specialists was poor54 55 and this may impact on care. Specialists highlighted that they would lose long-term outcome data if they did not follow-up patients themselves.45 They also described the relationship that forms with patients over time which was echoed by patients who described forming a bond with their specialists and feelings of abandonment when discharged.54 55 The specialists reported the positive reinforcement they received from following up patients in remission rather than just seeing patients with complications and more advanced/untreatable disease.55
Discussion
This scoping exercise identified the paucity of available literature exploring patient and HCP perspectives on the follow-up and management of PBC and a lack of any data around the role of primary care in the long-term management of patients with low-risk PBC. However, studies reporting stakeholder perspectives on changes to the delivery of breast cancer follow-up care have shown that not all patients or practitioners are comfortable with management being located substantially in the primary care setting. A series of themes emerged which have relevance to proposed care pathway changes including the knowledge base and workload of primary care, communication between care settings and the importance of the doctor–patient relationship. Within the data available specifically for PBC, the impact of delegitimisation and stigmatisation felt by PBC patients is likely to be of relevance when developing new strategies for follow-up care.
This scoping review has identified a gap in the literature around patient and HCP perspectives on management in primary care and the need for further study in this area to look specifically at the potential concerns of users of this pathway and whether or not the themes identified in this scoping review are relevant, if there are additional barriers or facilitators not identified here and, if so, how they can be overcome.
As is common with the use of a scoping review rather than a systematic review, there was a focus on identifying the breadth of literature available rather than looking at the available studies in depth and the quality of the studies identified was not assessed. However, the identification that there is little relevant literature in this field meant that this was less important. We aimed to conduct a comprehensive search of the literature, using a multiple database strategy. However, it is possible that some relevant articles were missed. The lack of identification of additional relevant studies from reference lists of the chosen papers would support the belief that the search identified the relevant data in the field. Finally, it is not possible to know whether, and to what extent, any of the conditions considered by the authors for the second stage of the scoping study (including other forms of autoimmune disease, other forms of chronic liver disease and breast cancer) truly act as comparators to PBC. While breast cancer was chosen as a comparator condition due to its similarities to PBC in terms of demographics of the patient population, this decision makes the assumption about the overall importance of patient demographics in determining its healthcare related behaviours. In addition, there are likely to be fundamental differences in comparing a malignant and non-malignant condition that will impact on how patients and clinicians view their future care needs. Finally, PBC as a rare disease is likely to pose different challenges to breast cancer which is now relatively common.
Conclusion
The recent guidelines from both the UK and European Societies propose a shift towards individualised care for patients with PBC. While individualised care is not explicitly defined, one potential consequence that is discussed in the British Guidelines is the discharge of patients deemed ‘low risk’ from hospital care to follow-up in primary care. The feasibility of this strategy is unclear and as such, the purpose of this scoping review was to identify the breadth and depth of the data already available about patient and clinician perspectives on management in primary care in order to identify facilitators and barriers to implementing this in practice. This review however highlighted that there is in fact a lack of data and that in order to be able to definitively answer the question of feasibility within PBC, further study may be required.
In developing a stratified approach to the care of the patient with PBC it will be essential to frame changes in care around high quality research. Underpinning this are opportunities to change practice by first of all an emphasis on education. This should address specific education for patients with PBC, and for primary care physicians, a broader education effort on the management of chronic liver diseases. With such an approach there would then be a greater opportunity to perhaps implement further change though targeted education, and use of smart technology/Apps to aid individualise risk assessment and changes to care pathways. Any approaches to change would require sensitive implementation adapted to local resources: for example, where large group practices and primary networks exist in primary care, opportunities to use a few embedded primary care liver champions may be effective, whereas in rural areas, IT/nurse supported change to care for GPs may be better.
Across the various models of healthcare delivery, it will be essential to evaluate feasibility of stratified care for patients with PBC in many different settings and healthcare models. Solutions for urban areas may, for example, be distinct to those for rural environments, and obstacles to implementation may include economic and personnel issues. Nevertheless, there exists the opportunity to be innovative in-service design and then to evaluate the impact of any service change.
We believe the similarities between the patient, disease and management characteristics of postsurgery breast cancer and low-risk PBC patients to be such that it is reasonable to anticipate comparable barriers will emerge to the implementation of the new management guidelines for PBC. Dedicated research involving patients and clinicians is still required to confirm that barriers to change exist, to identify what these barriers are and to plan strategies for intervention in this group of patients and clinicians. This information will be relevant not only to the possible future implementation of stratified care models in the PBC population but will also be applicable to other rare chronic diseases including, but not exclusive to, liver disease.
Acknowledgments
This paper presents independent research supported by the NIHR Birmingham Biomedical Research Centre at the University Hospitals Birmingham NHS Foundation Trust and the University of Birmingham. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
References
Footnotes
Contributors MC contributed to the conception and design of this scoping review, the acquisition and analysis of the data, and drafted and revised the paper for final submission. GH, SG and JP contributed to conception and design and revised the draft paper for final submission. MC acts as the guarantor for this submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests MC and GH are collaborating investigators for UK-PBC, a MC stratified medicine platform. SG and JP declare no competing interests.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No additional data are available.