Article Text

Abstract
Background Severe sepsis is likely to account for around 37 000 deaths annually in the UK. Five years after the international Surviving Sepsis Campaign (SSC) care bundles were published, care standards in the management of patients with severe sepsis are achieved in fewer than one in seven patients.
Methods This was a prospective observational cohort study across a 500-bed acute general hospital, to assess the delivery and impact of two interventions: the SSC resuscitation bundle and a new intervention designed to facilitate delivery, the sepsis six. Process measures included compliance with the bundle and the sepsis six; the outcome measure was mortality at hospital discharge.
Results Data from 567 patients were suitable for analysis. Compliance with the bundle increased from baseline. 84.6% of those receiving the sepsis six (n=220) achieved the resuscitation bundle compared with only 5.8% of others. Delivery of the interventions had an association with reduced mortality: for the sepsis six (n=220), 20.0% compared with 44.1% (p<0.001); for the resuscitation bundle (n=204), 5.9% compared with 51% (p<0.001). Those receiving the sepsis six were much more likely to receive the full bundle. Those seen by the sepsis team had improved compliance with bundles and reduced mortality.
Conclusions This study supports the SSC resuscitation bundle, and is suggestive of an association with reduced mortality although does not demonstrate causation. It demonstrates that simplified pathways, such as the sepsis six, and education programmes such as survive sepsis can contribute to improving the rate of delivery of these life-saving interventions.
- Emergency departments
- infection
- intensive care
- nursing
- wounds
Statistics from Altmetric.com
In the UK, severe sepsis is estimated to kill 37 000 patients1 annually, and consume 50% of critical care resources.2
Guidelines3 (revised in 20084) were created to drive change. The resuscitation bundle (box 1) was developed for the first 6 h following the onset of severe sepsis. This remains the internationally recognised standard of care. It comprises early goal-directed therapy (EGDT), which requires specialist skills to deliver, and more basic aspects that do not. EGDT has been associated with a 34.4% relative risk reduction for mortality.5
The Surviving Sepsis Campaign severe sepsis resuscitation bundle
Measure serum lactate within first 6 h after presentation.
Obtain blood cultures before antibiotic administration.
From the time of presentation, give broad-spectrum antibiotics within 1 h.
Source of infection to be identified and controlled within 6 h.
In the event of hypotension and/or lactate >4 mmol/l (36 mg/dl):
Deliver an immediate minimum of 20 ml/kg crystalloid (or colloid equivalent).
Give vasopressors for hypotension not responding to initial fluid resuscitation to maintain mean arterial pressure ≥65 mm Hg.
In the event of persistent arterial hypotension despite volume resuscitation (septic shock) and/or initial lactate >4 mmol/l (36 mg/dl):
Achieve central venous pressure of ≥8 mm Hg within 6 h.
Achieve central venous oxygen saturation ≥70% within 6 h.
The Surviving Sepsis Campaign (SSC) has reported observational data on 15 022 patients.6 Improved compliance with the resuscitation bundle (‘the bundle’) was associated with a 19% relative risk reduction for mortality. Despite this, the bundle is poorly performed in the UK, having been achieved for only 14% of 1232 patients in 18 reporting centres (UK SSC, 2009, unpublished data).
In recognition of poor compliance, we developed an operational solution reflective of NHS practice to improve delivery of the bundle. The ‘sepsis six’,7 8 (box 2) is designed to facilitate early intervention with three diagnostic and three therapeutic steps to be delivered by staff within 1 h. The tasks were identified from those poorly performed in our initial gap analysis.9 The accompanying education programme, survive sepsis,10 reinforces that failure of a patient to respond to the sepsis six (persistent evidence of hypoperfusion) mandates immediate referral to critical care to complete the remaining elements of the resuscitation bundle (ie, EGDT).
The sepsis six
The sepsis six to be delivered within 1 h
Deliver high-flow oxygen.
Take blood cultures.
Administer empiric intravenous antibiotics.
Measure serum lactate and send full blood count.
Start intravenous fluid resuscitation.
Commence accurate urine output measurement.
The sepsis six, endorsed by SSC, has been embraced by the UK College of Emergency Medicine11 and the Welsh Saving 1000 Lives Campaign,12 and is in use in over 30 units in England and Wales.
A prospective observational study cannot determine cause and effect. This study, across a 500-bed acute general hospital, was designed to define our severely septic patient population, to evaluate whether the sepsis six, supported by a sepsis team, could be reliably delivered, and whether it facilitated delivery of the resuscitation bundle. Recognising limitations, we also set out to report whether compliance with the sepsis six and the full bundle were associated with improved survival.
Methods
Patient selection and identification
All patients (≥16 years) with severe sepsis defined by the American College of Chest Physicians (ACCP)/Society of Critical Care Medicine (SCCM) consensus definitions13 were included. Patients with a limitation of treatment decision made within 6 h of the onset of severe sepsis were excluded.
For a patient to have complied with the sepsis six and resuscitation bundle, they had to receive all elements of care within 1 h and 6 h, respectively. Time zero was taken as the point at which severe sepsis was first present rather than first identified to reduce confounding factors in evaluating any association with mortality. Time zero was identified from triage time for patients in the emergency department. In critical care, time zero could be identified prospectively through continuous observations. Outside these areas, the sepsis team identified time zero retrospectively, by checking back through patients' charts and our pathology database.
Staff were trained to use a standard screening tool based on ACCP/SCCM definitions whenever infection was suspected, when the observations scoring system modified early warning scores (MEWS) triggered, or if they were concerned about a patient. As a redundancy, an electronic flag on the pathology information system prompted the sepsis team to evaluate patients with a white cell count of greater than 14×109/l. This level was set following pilot work to allow a manageable caseload. Identification of severe sepsis mandated completion of the sepsis six and referral to the sepsis team.
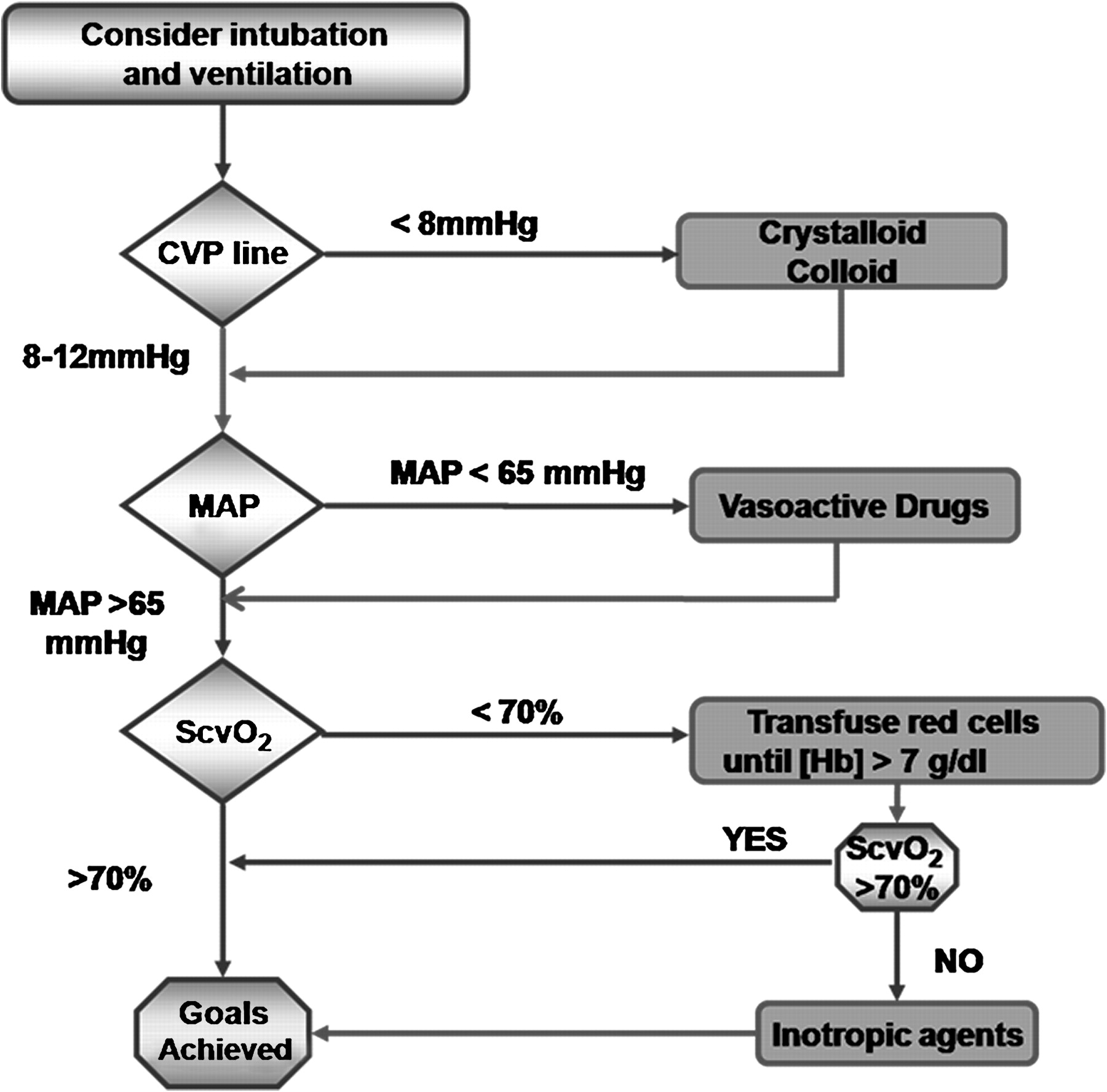
Hypoperfusion was defined by ACCP/SCCM definitions. In the absence of hypoperfusion, the sepsis six alone would complete the bundle. In hypoperfused patients, the sepsis six mandated an immediate fluid challenge of 20 ml/kg (or colloid equivalent). If this reversed hypoperfusion, the resuscitation bundle was complete. If not, early goal-directed therapy (EGDT, figure 1) was required. This was led by the critical care or sepsis team depending on the time of day.
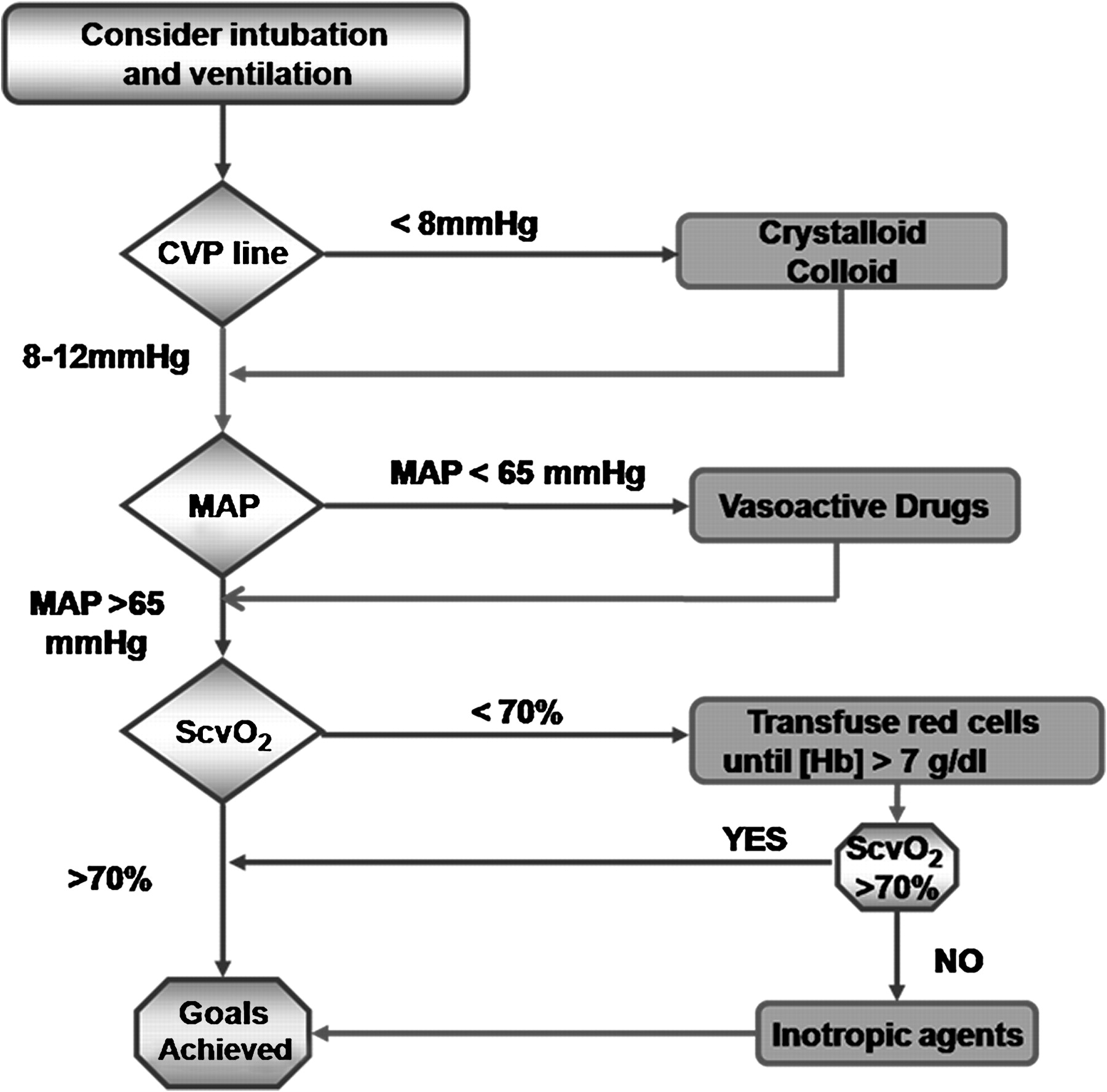
Schematic for the delivery of early goal-directed therapy. Adapted from Rivers et al.5 CVP, central venous pressure; MAP, mean arterial pressure; ScvO2, central venous oxygen saturation.
A standard pro forma was used to collect data on patients referred directly to the sepsis team, or identified out of hours and referred by dedicated voicemail.
MEWS and numbers of organ dysfunctions were recorded at time zero.
The sepsis team
The sepsis team comprised two sepsis nurses (critical care outreach sisters) sharing one whole-time post. Funding was obtained from the National Institute for Healthcare Research (NIHR-RfPB grant PB-PG-0706-10167).
Training
This study was supported by the trust board and patient safety team. We obtained buy-in from all stakeholder directorates. A focused programme of education was implemented. Over 800 staff underwent survive sepsis training10 on recognition of sepsis and the use of the sepsis six, including evaluation of knowledge using a participant voting system (KeePad, UK). All junior doctors were briefed, and presentations were made quarterly at grand grounds.
Data analysis
Data were entered into an Excel spreadsheet on a password-enabled computer. Hospital identifiers were included until discharge. A senior audit clerk blinded to outcome entered data. Any ambiguous fields were clarified with the investigating team. The team, blinded to compliance, would enter discharge status.
Patients were grouped into cohorts listed in table 1 according to their compliance with the sepsis six and resuscitation bundle, and whether or not they required EGDT in delivering the bundle. Some patients were able to achieve the full resuscitation bundle without having achieved the sepsis six, as the resuscitation bundle allows 6 h for measurement of serum lactate and fluid challenges, whereas the sepsis six allows only 1 h.
Cohort description
Data were analysed by an independent statistician using Minitab 15 using the Pearson χ2 test for categorical data and the Kruskal–Wallis test for non-parametric numerical data.
Results
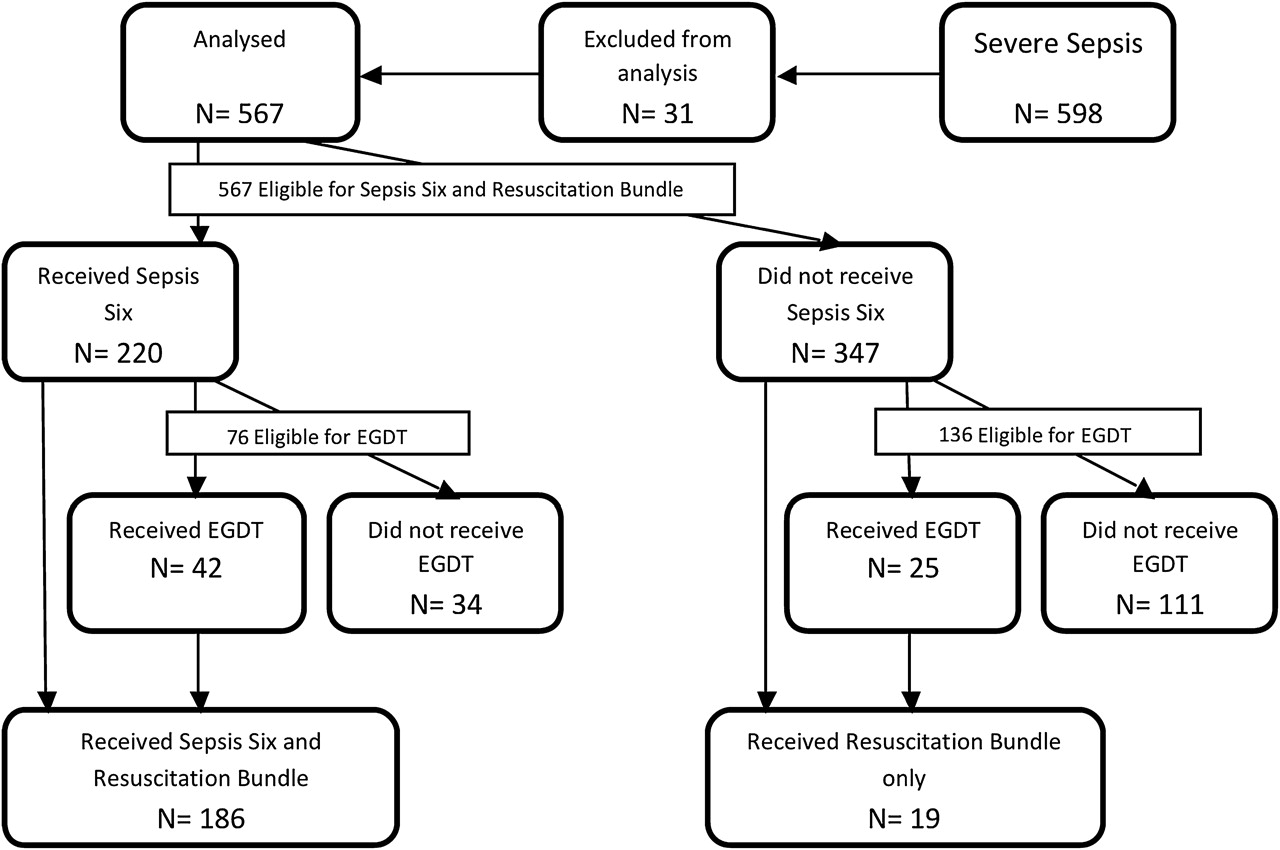
Data were prospectively collected for 598 patients from November 2007 to October 2008. Thirty-one episodes were excluded due to incomplete datasets (n=23) and second episodes of sepsis in the same patient (n=8, first episode analysed). Analysis was undertaken for 567 patients. Cohort ‘EGDT only’ included only two patients, so was excluded from some analyses. Figure 2 shows flow through the study. Overall mortality was 34.7%.

Patient flow through the study care pathway. EGDT, early goal-directed therapy.
Patient characteristics
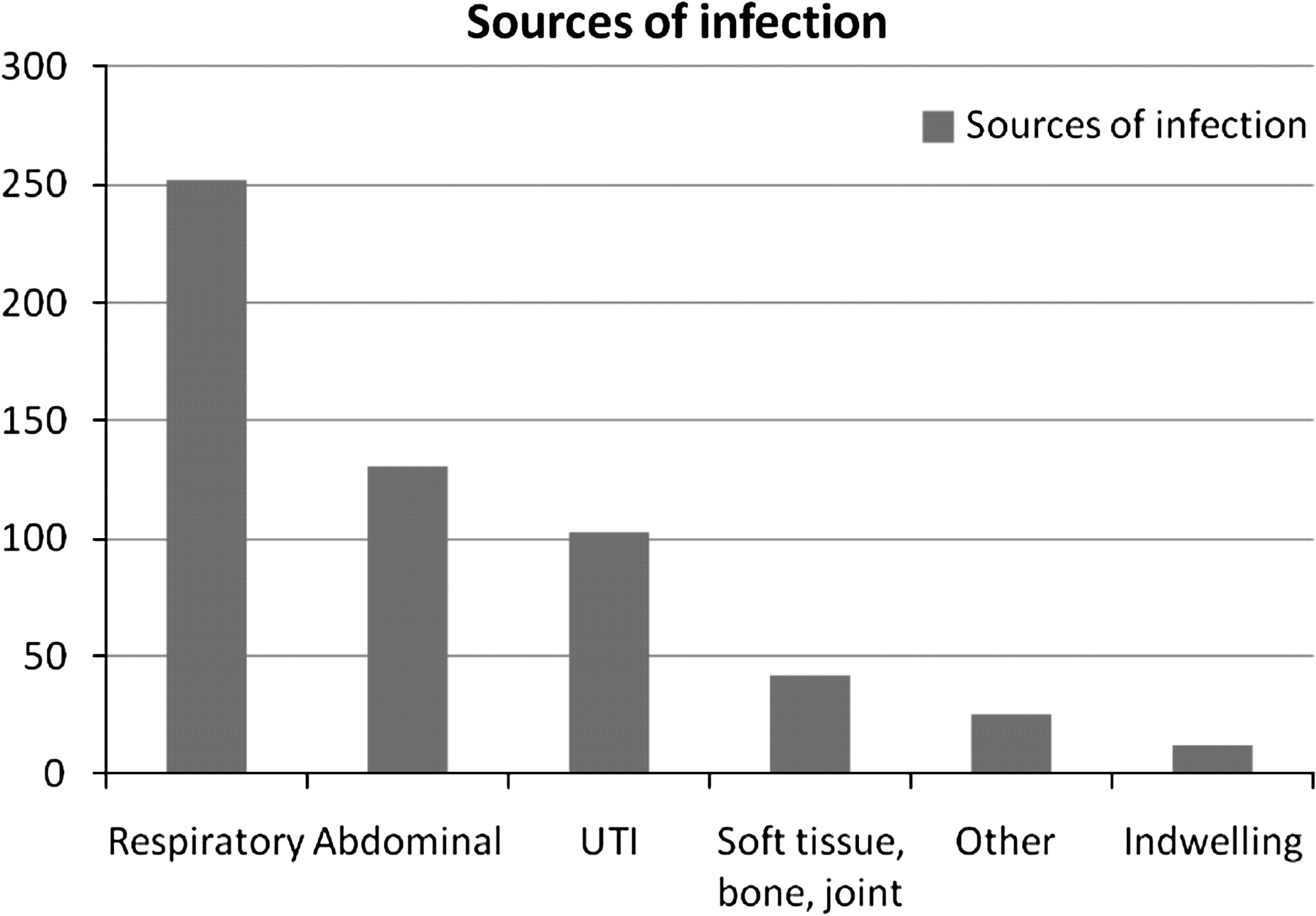
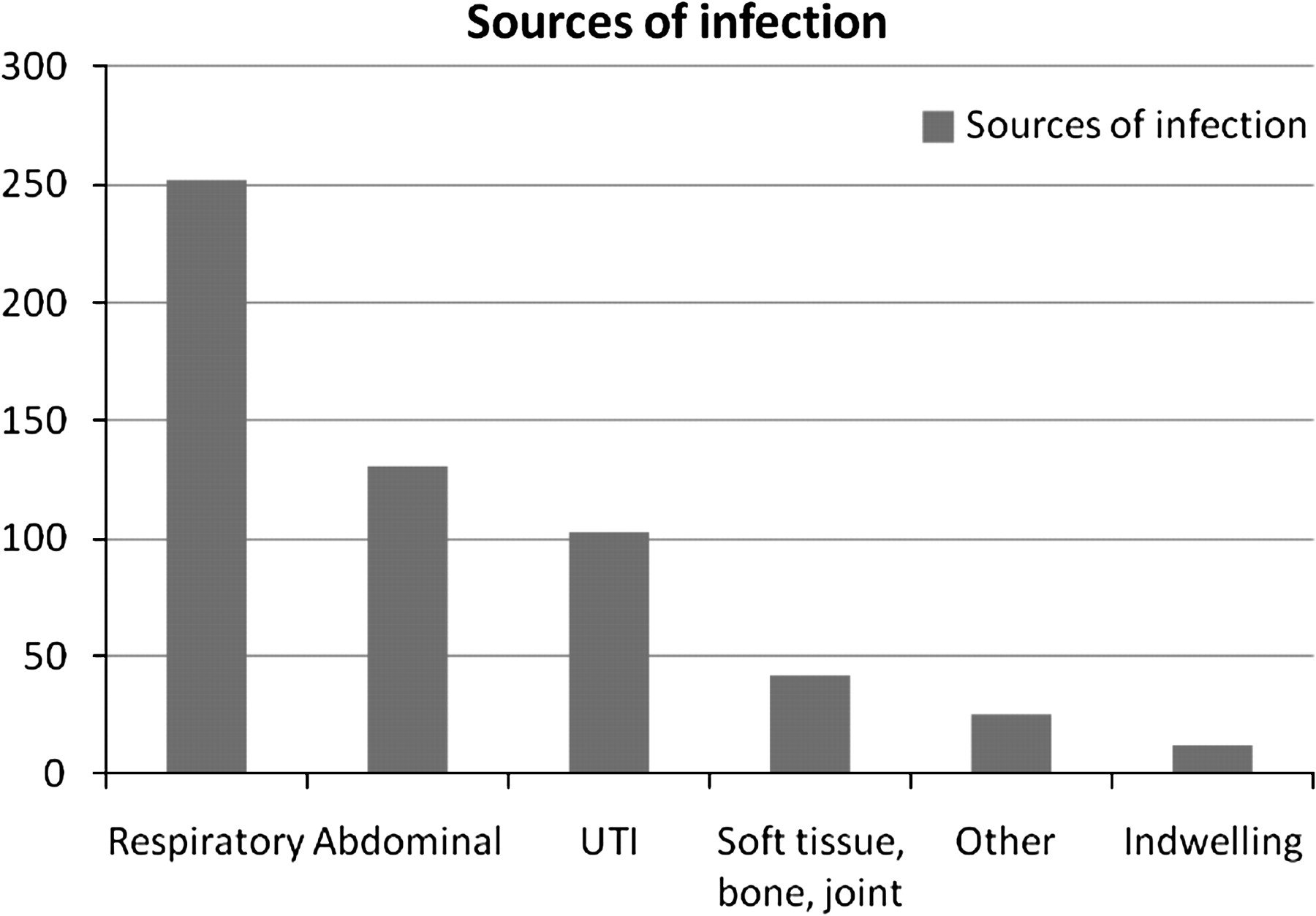
Figure 3 demonstrates sources of infection. If multiple sources were suspected, the more common was reported. There were no significant differences in outcome according to the source of infection (mortality range 23.8–41.7%, p=0.236).
{kind=link}
{kind=link}
{kind=link}
Sources of infection. UTI, urinary tract infection.
Three hundred and sixty-eight patients (64.0%) were referred to the sepsis team by other staff, 207 (36.0%) were identified by a high white blood cell count.
Table 2 shows population characteristics. Average age was 68.5 years (range 18–101), with survivors younger than non-survivors (at discharge, 70 vs 77 years, p<0.001). Patients had median MEWS at time zero of 6.0 (range 0–15), with 467 (81.2%) meeting the trigger threshold of 4. Median scores in survivors and non-survivors were similar (p=0.333).
Population characteristics
Cohort characteristics are given in table 3. Cohorts were similar for the source of infection. Older patients were less likely to receive EGDT (p<0.001). Patients with higher MEWS scores and more organ dysfunctions were more likely to receive interventions (p<0.001, p=0.017). One hundred and eighty-six (32.4%) patients were admitted to critical care, with a mean stay of 15.4 days (range 1–829).
Characteristics of cohorts
Both hypoperfusion (present in 74.6% of patients) and ‘cryptic shock’14 (present in 38.1% of normotensive patients) were associated with poor outcome (table 2).
Three hundred and three of 423 hypoperfused patients received fluid challenges (71.7%), which reversed the hypoperfusion in 65.0% of cases. The remainder (septic shock, n=197) qualified for EGDT. Shock was associated with poor outcome (mortality 64.5% vs 17.1%).
Delivery of interventions
The sepsis nurses treated a representative sample (34.0% shocked) of 144 patients. These patients were more likely to receive the resuscitation bundle (72.9% vs 23.4%, p<0.001) and less likely to die (mortality 25.5% vs 38.4%, p<0.001).
Two hundred and twenty patients received the sepsis six, which appeared to facilitate delivery of the resuscitation bundle operationally, with 186 (84.6%) achieving the bundle compared with only 20 (5.8%) of the remaining 347 patients (p<0.001).
Outcome varied between cohorts (p<0.001, table 3). The lowest hospital mortality (4.8%) was seen in shocked patients receiving all care: group ‘shock: all bundles’. Of 34 patients in group ‘shock: sep 6 only’, who were shocked but failed to receive EGDT, none survived.
Some 5.9% of patients receiving the resuscitation bundle (table 4) died, compared with 51.0% of those not receiving it (p<0.001).
Outcomes for ‘raw’ cohorts
Patients receiving the sepsis six (n=220) were less likely to die, with mortality 20.0% in those receiving the sepsis six and 44.1% in those not receiving it (p<0.001). In the absence of shock, the sepsis six remained associated with survival with 94.4% of 144 patients surviving compared with 74.9% of 211 patients not receiving it (p<0.001). Admission to critical care was also associated with improved outcome (mortality 30.1% compared with 37.2%).
Table 5 lists individual elements of the sepsis six, the delivery of each of which was associated with higher survival. For a glossary of terms see table 6.
Individual sepsis six interventions and outcomes
Glossary of terms
Discussion
The SSC resuscitation bundle remains a challenge to deliver.15 Challenges in early identification are one of the most significant barriers to implementation.16 17
This study combined a prospective observational cohort study with the introduction of the sepsis six toolkit and education programme, following a baseline retrospective audit showing compliance of 19%. It is unique in the UK applying a whole-hospital approach to defining delivery of the resuscitation bundle: in fact, almost half of patients developed severe sepsis for the first time on the wards, where treatment is often greatly delayed through lack of recognition. Our previous study9 had attempted to measure whole-hospital compliance, but was unresourced and captured far fewer patients.
The SSC6 showed resuscitation bundle compliance to be 31.3% after 2 years and mortality to have reduced during the study period. During our study, independent data from the Intensive Care National Research and Audit Centre showed reducing hospital mortality for our severely septic patients from 38% (95% CI 21% to 57%) to 20% (11% to 40%).
The number of patients identified in 12 months is higher than expected compared with European observational studies.18 19 A recent study in Southampton estimated similar numbers of patients to those seen here.20 Earlier work in the USA suggested a rate of three cases per 1000 population per annum, a level also more in keeping with our findings.21 Our sepsis nurses are likely to have increased detection rates for sepsis. The SSC showed differences in outcome according to the source of sepsis, a distinction not seen in this study, although our smaller numbers may not have been sufficiently sensitive.
The electronic trigger for white cell counts (>14×109/l) identified severe sepsis in 207 patients of 2500 screened—this approach is more sensitive than specific. However, this did identify over a third of patients, and was a useful redundancy, in that these 207 patients had either not triggered MEWS or had triggered but not been screened for sepsis.
Contrary to expectation, no association was observed between increasing numbers of organ dysfunctions and poor outcome. The most likely explanation is that the study was too small to identify a difference—fewer than 10% had three or more organ failures. However, the higher median numbers of organ dysfunctions seen in intervention cohorts suggest that those with greater numbers of dysfunctions were identified earlier and treated more aggressively. There did appear to be a trend towards increasing mortality in the progression from single to two organ failures.
Our patients were sick, with high median MEWS (a score of more than 5 predicts critical care admission22), 1.63 (mean) organ dysfunctions, and hypoperfusion in 74.6%; 34.6% were admitted to critical care. Although patients receiving the sepsis six and resuscitation bundle were younger, they tended to be more unwell. This would tend to offset the possibility that relative youth may have accounted for improved outcome in the intervention groups, but to what extent is not clear. Organisations would be wise to consider improving sepsis identification and management to direct resources towards their sickest patients. Only just over 80% of our patients had MEWS reaching the trigger threshold at time zero—MEWS is not sufficiently sensitive to be used alone to identify severe sepsis.
Track-and-trigger systems such as MEWS incorporate blood pressure, although most use systolic only. In this study, shocked patients were over three times more likely to die. Measurement of lactate has been suggested as a triage tool,23 24 and the high prevalence of cryptic shock (38.1%) in this population would support this practice. Early fluid challenges reversed hypoperfusion in two-thirds of eligible patients. Given that hypoperfusion is associated with poor outcome, this reinforces the need to prioritise rapid ‘basic’ intervention over EGDT.
The sepsis six operationally facilitated delivery of the resuscitation bundle, with patients receiving the sepsis six 14.6 times more likely to receive it. The sepsis nurses achieved treatment guidelines more reliably than non-specialist colleagues, and their patients were more likely to survive.
Other centres have evaluated EGDT according to Rivers' protocol.5 Some have noted improved outcomes,25–27 although all studies claiming to validate EGDT have been observational ‘before and after’ trials. The SSC showed apparent lack of efficacy of central venous pressure and ScvO2 targets, two of the requirements of Rivers' EGDT protocol. Opponents to EGDT cite the unreliability of CVP and ScvO2 in the assessment of ventricular filling pressures and oxygen delivery, and a high control group mortality (46.5%) in Rivers' patients—drawn from a public hospital in deprived inner-city Detroit. Groups from the USA and The Netherlands have found a low incidence of low ScvO2 in their own populations, and found their mortality in the absence of EGDT to be lower than that of Rivers' intervention group.28 29
We did not attempt to study components of EGDT. Rivers' protocol is being evaluated in multicentre studies including the ARISE study30 and the ProMISe study in the UK. The PROCESS study in the USA31 is examining it against controls and a third arm allowing greater flexibility in circulatory assessment.
In our study, patients receiving either or both of the sepsis six and resuscitation bundle were less likely to die. The resuscitation bundle, with its invasive aspects of EGDT appeared to be particularly associated with improved outcome.
We achieved compliance with the sepsis six and resuscitation bundle of 38.6 and 35.8%, respectively, with 32.6% receiving both. Our background data showed compliance with the resuscitation bundle of 19% in the emergency department, showing a relative improvement of over 80%. The SSC showed organisations achieving 31.3% compliance during the last quarter of their contribution—our study lasted only 1 year and showed higher rates even when rates were averaged over the entire period. For our emergency department patients, compliance was much higher at 62.8% (73.6% compliance with the sepsis six). This unplanned analysis, showing a 230% relative improvement, may more accurately reflect the potential impact of a dedicated, hospital-wide programme.
We found that the delivery of each sepsis six element was associated with significant outcome improvements (table 5). The SSC6 found similar relationships for antibiotic administration (OR 0.86) and taking blood cultures (OR 0.76), but not for lactate (OR 0.97) and did not report on fluid challenges. Measuring lactate will not improve outcome unless a response is made. It is conceivable that the measurement within the context of the sepsis six empowers relatively junior staff to seek senior advice more rapidly.
This observational study has significant limitations due to the inability to control adequately for confounding factors. We are unable to draw any ‘cause and effect’ conclusions, although groups receiving treatments did appear to have better outcomes. With any observational study involving care bundles, it is impossible to distinguish whether delivery of the bundles simply reflects a globally higher standard of care for compliant patients or whether the bundles themselves impact on outcome. We can say with certainty that delivery of care improved during this study, and that patients receiving the sepsis six were far more likely to receive the resuscitation bundle. It is clear that reliable delivery of the bundle, defined as 80% of patients receiving the standard of care, is a long way off.32 Greater investment, awareness and refinement of process are needed to embed gold-standard sepsis care.
Although cohorts were similar for the source of infection and organ dysfunctions, the younger patients (possibly more likely to survive) were more likely to receive EGDT. However, the elderly were just as likely to receive the other bundles, and the differences in outcome with age was not marked enough to account for the mortality reduction seen with EGDT. In addition, patients receiving all interventions were sicker, which would tend to support observed outcome differences being genuine. We attempted to minimise observer bias by blinding the individual collecting mortality data to process measures, and by using a trained independent clerk to input data. Despite limitations, the numbers of patients recruited has allowed us to draw some relevant conclusions.
Conclusions
This study supports implementation of the SSC resuscitation bundle, which appears to be associated with reduced mortality. It demonstrates that the sepsis six and education programmes such as survive sepsis can contribute to improving delivery of these interventions. In our organisation, patients receiving the sepsis six fared better, although we are unable to claim that this was directly due to the sepsis six. In patients with shock, the sepsis six only appeared to be of benefit if non-responders also received EGDT. EGDT is currently being re-evaluated in three multicentre trials, the results of which will further inform practice.
We recommend that organisations consider the implementation of dedicated programmes to improve recognition and management of sepsis in all areas. Consideration should be given to the implementation of the sepsis six as the initial treatment of septic patients. Sepsis nurses, education programmes and redundancies such as white cell count triggers are valuable.
References
Footnotes
Linked articles 101808.
See Commentary, p 459
Funding This study was entirely funded by the National Institute for Healthcare Research Research for Patient Benefit programme (NIHR-RfPB grant PB-PG-0706-10167). The funding body approved the study design only.
Competing interests RD was chair of the UK Surviving Sepsis Campaign at the time of the study. He has received honoraria and consultancy fees, and been reimbursed by Eli Lilly and Co, the manufacturer of the critical care drug xigris, for attending a number of conferences. The education programme, survive sepsis, received unrestricted educational grants in 2007 from Eli Lilly and from Astra Zeneca, manufacturers of the antibiotic meropenem, Edwards Lifesciences, manufacturer of the vigileo/flotrac cardiac output monitoring system and Vygon UK, manufacturers of central venous catheters. Neither RD nor survive sepsis have received funds during the past 24 months. TN received a single honorarium from Eli Lilly and Co in 2007 for a presentation at a European meeting. GM and CG have no competing interests.
Ethics approval Discussion with our Local Research and Ethics Committee and with the National Institute for Healthcare Research (NIHR) concluded that the study fell outside the need for ethical approval, and that since the study aimed to deliver an accepted gold standard of care, informed consent was unnecessary.
Provenance and peer review Not commissioned; externally peer reviewed.