Article Text

Abstract
Objective To determine the location and use of small bowel endoscopy services in the UK and to analyse training uptake to assess future demand and shape discussions about training and service delivery.
Design Surveys of British Society of Gastroenterology (BSG) members by web-based and personal contact were conducted to ascertain capsule endoscopy practice and numbers of procedures performed. This was compared with expected numbers of procedures calculated using BSG guidelines, hospital episode statistics and published data of capsule endoscopy in routine practice. Analysis of data from two national training courses provided information about training.
Results 45% of UK gastroenterology services offered in-house capsule endoscopy. 91.3% of survey responders referred patients for capsule endoscopy; 67.7% felt that local availability would increase referrals. Suspected small bowel bleeding and Crohn's disease were considered appropriate indications by the majority. Demand is increasing in spite of restricted use in 21.6% of centres. Only two regions performed more than the minimum estimate of need of 45 procedures per 250 000 population. Eight centres perform regular device-assisted enteroscopy; 14 services are in development. 74% of trainees were interested in training and of those training in image interpretation, 67% are doctors and 28% are nurses.
Conclusions Capsule endoscopy is used by the majority of UK gastroenterologists but appears to be underused. Current demand for device-assisted enteroscopy seems likely to be matched if new services become established. Future demand is likely to increase, however, suggesting the need to formalise training and accreditation for both doctors and nurses.
Statistics from Altmetric.com
Background
Capsule endoscopy has become a first-line small bowel investigative modality in the UK, Europe and the USA1,–,7 with device-assisted enteroscopy enabling biopsy for histology and endoscopic therapy.7 8 This is the first time that gastroenterologists have had direct access to the small bowel without recourse to surgery and arguably the past decade has seen the development of a new subspecialty: the investigation and management of small bowel disease.
In the UK, service development has been driven locally rather than being planned, regulated and monitored, so access to capsule endoscopy is unknown. Small bowel endoscopy tariffs have been introduced relatively recently through payment by results, but the true costs have yet to be established. The Joint Advisory Group on Gastrointestinal Endoscopy provides clear, detailed and structured training programmes and certification processes for most endoscopic procedures,9 but none for small bowel endoscopy.
This working party report was commissioned by the British Society of Gastroenterology (BSG) endoscopy and small bowel and nutrition committees and produced by the UK Capsule Endoscopy Users' Group. It aimed to determine the location of, and demand for, capsule endoscopy services in the UK and assess needs for training in order to predict future demand, shape discussions about training requirements and consider how best to deliver high-quality services.
Methods
BSG members were sent a web-based survey (SurveyMonkey) of small bowel endoscopy practice via email and the BSG e-newsletter. Trainees were invited to complete a training survey.
All UK gastroenterology and/or endoscopy units were contacted to establish if they offered capsule endoscopy or device-assisted enteroscopy services and lead clinicians were asked to provide service details. Gastrointestinal units were asked if, and to where, they referred patients, to ensure that no capsule endoscopy service went unrecognised.
Expected numbers of capsule endoscopies were compared with actual procedures performed in Northern Ireland, Scotland, Wales and in each health authority in England in the year 2009–10. Expected numbers were based on calculations of those requiring capsule endoscopy for the two commonest indications—namely, suspected small bowel bleeding and suspected Crohn's disease, indications recommended by national and international guidelines.2,–,7
Activity data were obtained from the National Health Service (NHS) information centre hospital episode statistics for England 2009–10 and similar activity (per head of population) was assumed for Northern Ireland, Scotland and Wales for the purpose of calculations.10 No code exists for small bowel bleeding, so it was assumed that 5% of gastrointestinal bleeding arose from the small bowel.11 12 The total number of episodes of gastrointestinal bleeding was summated from all relevant codes: ‘iron deficiency anaemia secondary to blood loss (chronic)’ (D50.0), ‘other iron deficiency anaemia’(D50.8), ‘iron deficiency anaemia, unspecified’ (D50.9), ‘iron deficiency’ (E61.1), ‘haematemesis’ (K92.0), ‘melaena’ (K92.1) and gastrointestinal haemorrhage, unspecified (K92.2).
Most episodes coded as Crohn's disease of the small intestine (K50.0) will have been diagnosed using ileocolonoscopy or radiology, which would over-represent the need for capsule endoscopy. Therefore expected demand was calculated from previous studies of indications for capsule endoscopy in routine clinical practice.13,–,17 Population for each strategic health authority in England and in Northern Ireland, Scotland and Wales in mid-2009 was obtained from the Office for National Statistics.18
Reimbursement costs through payment by results were obtained from the NHS Connecting for Health ‘OPCS (Offices of Population and Censuses and Surveys) Classification of Intervention and Procedures’. Information about demand for training was obtained from two national hands-on training courses.
Results
Survey of UK gastroenterologists' practice
Email invitations to complete the survey were received by 701 BSG handbook–listed full members (emails were returned from a further 10% for whom addresses were incorrect). There were 289 survey responders (41%). A total of 91.3% had access to capsule endoscopy referring a median of five patients annually (range 0–70) to in-house services in 54.7%. Of those without local access, 67.7% felt that local availability would increase referrals. Responders considered capsule endoscopy for iron deficiency anaemia (92.0%), suspected overt gastrointestinal bleeding (91.7%), suspected small bowel Crohn's disease (77.2%), assessment of coeliac disease (29.1%) and polyposis syndromes (59.5%).
Capsule endoscopy: use 2002–10
Three hundred and thirty-four sites with gastroenterology units were identified from the BSG database, comprising 187 different hospital trusts with gastroenterology services, of whom 84 (44.9%) offered in-house capsule endoscopy (two of whom had an arrangement with a local private provider to perform NHS procedures).
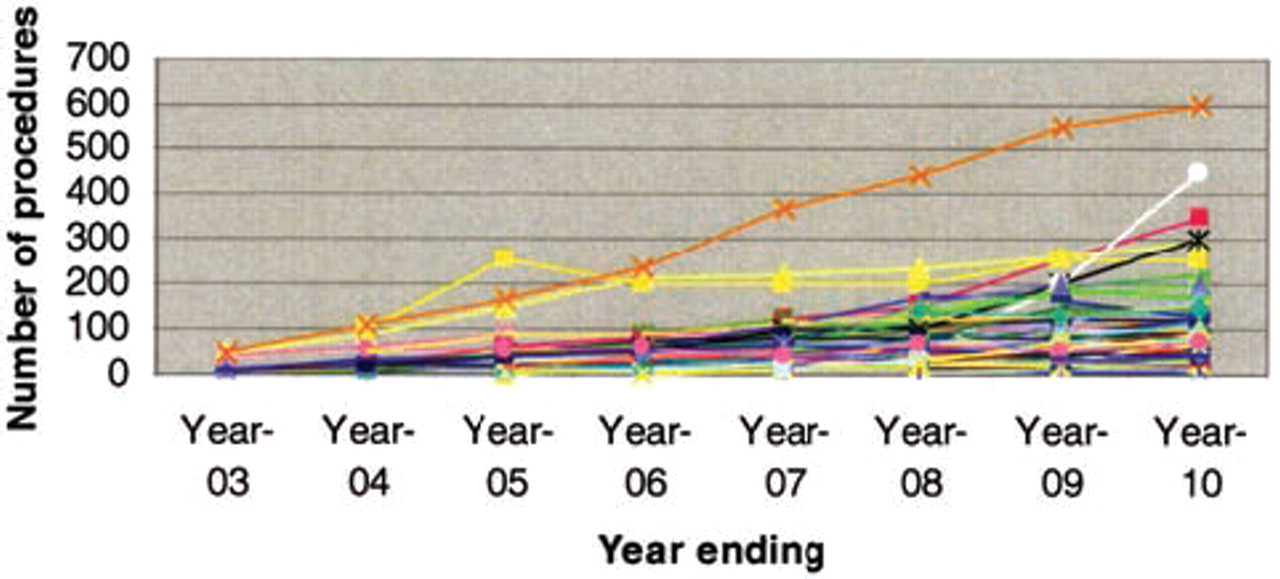
Year-on-year activity data were received from 74 (88.1%), 16 (21.6%) of whom were restricted in their use by the primary care trust or the hospital trust (with a cap on numbers, cost-per-case applications or restricted indications). Numbers of procedures performed in the past year of service (2009–10) were obtained from all 84 users. Services were established from 2002 to 2010 with a peak of 16 new services in 2007–8 (figures 1 and 2). There was a yearly increase in activity from 2002 to 2010 (figure 3) in the 58 units with unrestricted use and a total of 8430 capsule endoscopies performed in the year 2009–10 in the UK.
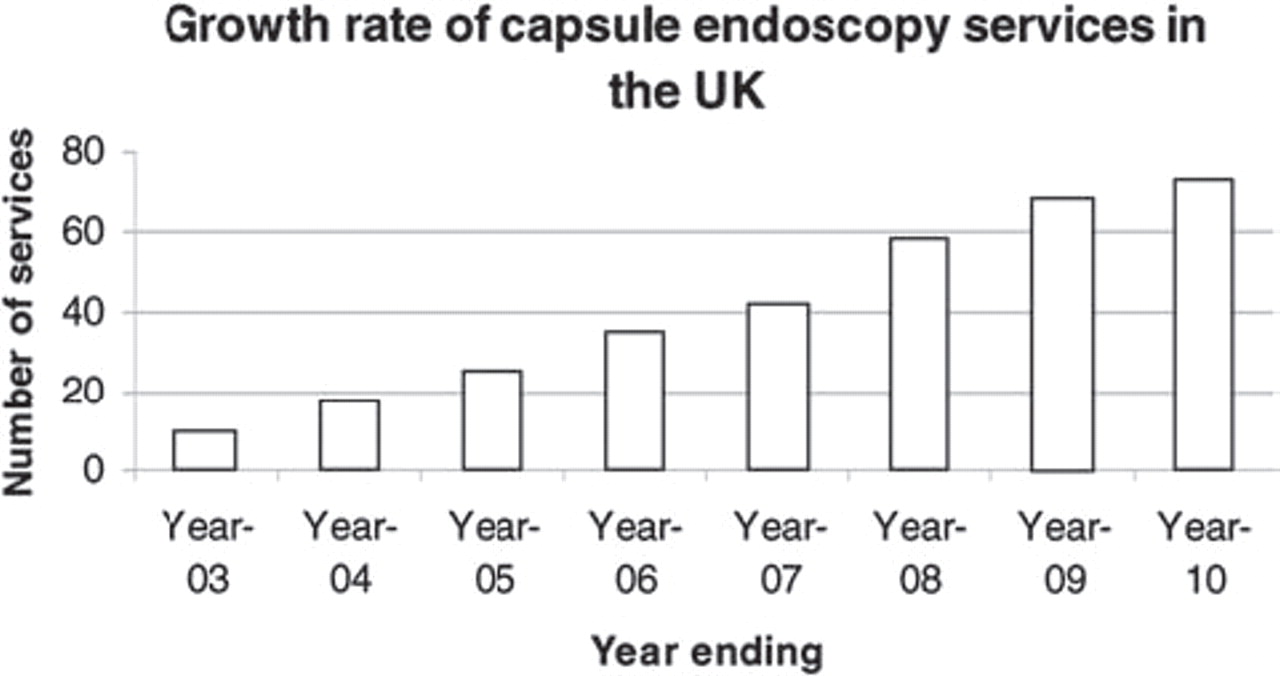
Growth rate of capsule endoscopy services in the UK.

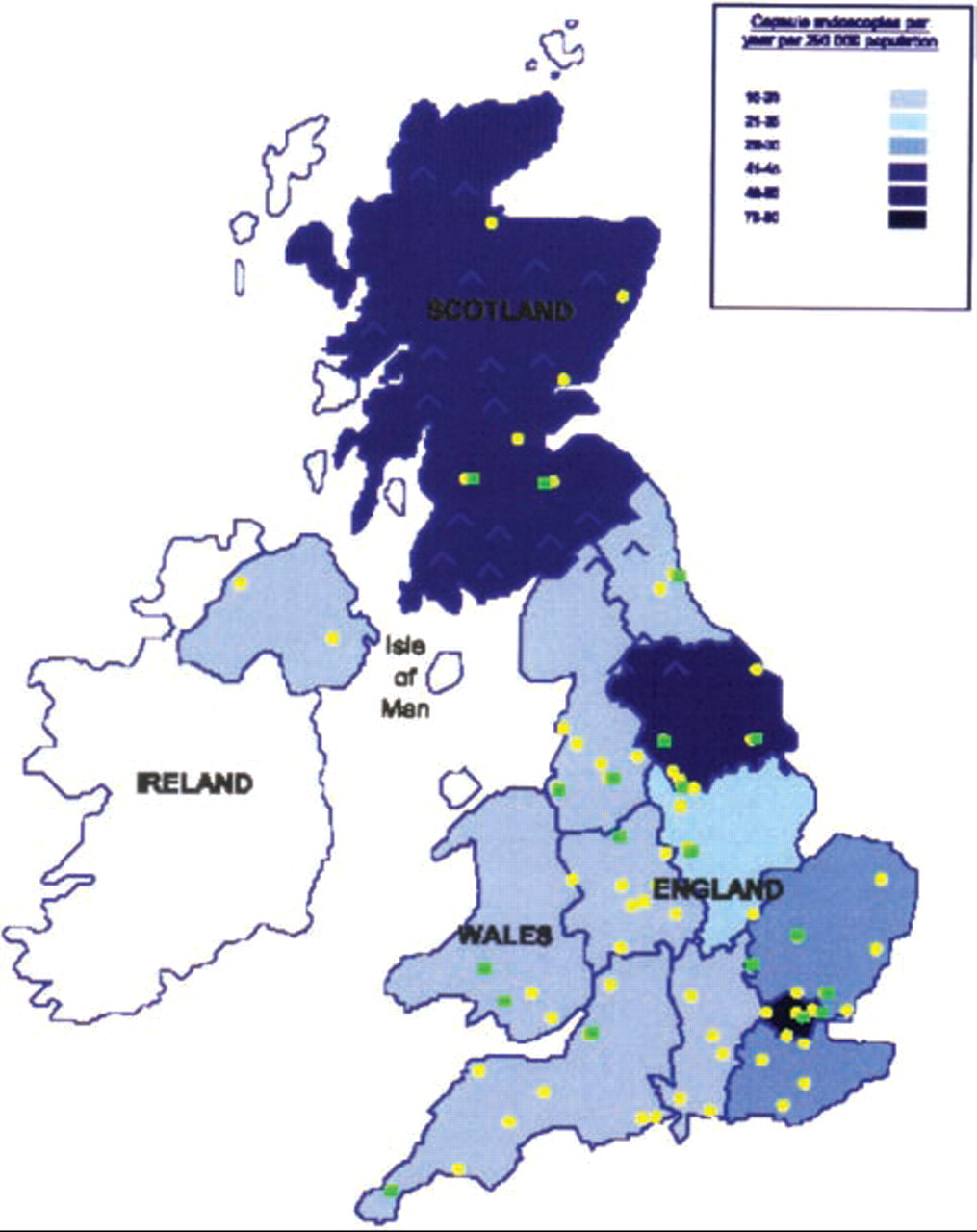
Location of capsule (circle) and device-assisted enteroscopy (square) services in the UK with numbers of capsule endoscopies performed annually per 250 000 population for each region.

{kind=link}
{kind=link}
{kind=link}
Number of capsule endoscopies per centre per year.
Capsule endoscopy: expected use 2002–10
The sum of finished consultant episodes with codes relevant to suspected small bowel bleeding was 158 516. Assuming 5% of patients with gastrointestinal blood loss have no source identified by upper and lower gut endoscopy,2 11 12 small bowel capsule endoscopy would have been indicated for 7926 patients in 2009–10.
Several series reporting the use of capsule endoscopy in routine clinical practice investigate suspected active Crohn's disease to suspected small bowel bleeding in ratios between 1:2.3 and 1:6.0.13,–,17 Assuming the lowest ratio for the purpose of calculating nationwide expected demand would suggest the need for 1321 procedures for suspected Crohn's disease in 2009–10.
Thus, a total of 9247 procedures a year would be expected based on 2009–10 data. Assuming a population in England of 52 million, 45 capsule endoscopies a year would be needed in a trust serving a population of 250 000. The numbers of procedures performed varied over fivefold, fewest in the East Midlands and most in the London health authority (16 and 80 per 250 000 respectively; table 1, figure 2). Only in two regions (London and South Yorkshire and the Humber Health Authorities) were more than 45 procedures per 250 000 population performed.
Capsule endoscopies performed per 250 000 population
Availability of device-assisted enteroscopy
Device-assisted enteroscopy was offered by 22 centres (figure 2): double balloon enteroscopy (12); single balloon enteroscopy (seven) and both double balloon and spiral enteroscopy (three). However only eight of these centres perform weekly procedures, with most in the development stage often with loaned equipment.19
Reimbursement for small bowel endoscopy
Payment by results aims to allow for the huge variability in cost of patient care by assigning procedure and diagnostic codes, of which individual patients may accrue one or many during an episode of care. These are bundled in groups of similar costing care episodes called Healthcare Resource Groups (HRG), each of which attracts set tariffs. Thus a patient having capsule endoscopy (procedure code G802) to investigate anaemia maps to an HRG code of FZ42Z with a tariff of £533 if the patient has no other investigation or significant comorbidity. Device-assisted enteroscopy has been given a procedure code for the first time in OPCS Classification of Interventions and Procedures Version 4.6 (April 2011): ‘balloon-assisted enteroscopy’ (procedure code G803) in the same setting maps to an HRG code of FZ24C equating to £630. By comparison, the HRGs for gastroscopy (procedure code G459) and colonoscopy (code H229) would be FZ03A (£416) and FZ26A (£398), respectively. Including VAT, capsule endoscopes cost between £432 and £526 (Diagmed Healthcare Ltd., Thirsk, UK; SynMed Ltd., Enfield, UK; Olympus Keymed, Southend, UK) and the disposable components for diagnostic double balloon enteroscopy (overtube, balloon kits for endoscope and overtube) are £416.80 (Fujinon GmbH, Willich, Germany).
Training demand
Most capsule endoscopy is performed by nurses trained by doctors or company representatives, but a dedicated ‘Essential capsule endoscopy nursing’ course is run by Diagmed Healthcare. The role of capsule endoscopy in clinical practice and video interpretation requires more in-depth training, provided by the Lumley Castle capsule course, a non-commercial course (supported by Diagmed Healthcare and endorsed by both the BSG and American Society of Gastrointestinal Endoscopy (ASGE)) comprising beginners' and advanced hands-on capsule endoscopy training in interpretation in a 2-day programme.
The nursing course has catered for 90 nurses (94% from the UK) in 10 courses from 2008 to 2010 (Carolyn Davison, personal communication). The Lumley Castle course has seen 387 delegates use 555 places (many attending for both days) in 12 biannual courses from 2005 to 2010 (Carolyn Davison, personal communication). The majority of delegates (67%) have been doctors (46% consultants and 21% trainees), 28% were nurses and 5% from other disciplines (physiologists, technicians, business managers and radiographers).
Of BSG member trainees, 25% completed the training survey, providing 104 responses. All but one trainee (99%) had been involved in the care of a patient who had undergone capsule endoscopy, 83% had worked in a hospital offering a service and 32% had studied a video. Although 74% were interested in training, only 16% had completed a recognised training course.
Discussion
The majority of UK gastroenterologists refer patients for small bowel capsule endoscopy, which has grown rapidly in numbers of services and procedures performed. Forty-five per cent have a service within their hospital trust, others referring to neighbouring centres. Over 90% of gastroenterologists consider suspected small bowel bleeding as an appropriate indication, 77.2% refer for investigation of suspected Crohn's disease and most would consider it to assess polyposis syndromes. There is considerable inter-regional variation in use, the majority significantly underusing capsule endoscopy in comparison with the indications recommended in national and international guidelines.2,–,7 This is partly explained by restrictions imposed on clinicians' use of services, inadequate reimbursement and lack of formal training and accreditation.
From the survey, practice seems to reflect BSG and NICE guidelines.2 3 Anaemia or obscure overt bleeding in patients with negative upper and lower gastrointestinal endoscopy is an appropriate indication for capsule endoscopy (grade B: availability of clinical studies without randomisation). At the time of publication, there were insufficient studies to consider suspected Crohn's disease as an indication beyond a grade C (evidence from expert committee reports or opinions or clinical experience of respected authorities) which might explain the reduced referral rates for this indication, although further favourable data have emerged since.5 20 That only 29.1% would consider coeliac disease as an appropriate indication may reflect the sensitivity of only 80–90% compared with endoscopy and duodenal biopsy and the paucity of published experience of use in complications of coeliac disease.2 5 21 Responders also appeared uncertain of the value of capsule endoscopy in polyposis syndromes. Capsule endoscopy does detect more small Peutz–Jegher's polyps, but MRI is equally sensitive in detecting larger lesions which are more clinically relevant.2 22 Although the most recent European guidelines5 consider capsule endoscopy appropriate in patients with familial adenomatous polyposis who have duodenal polyps (associated with the presence of distal polyps), uncertainty of BSG members as to the value of investigation may reflect the lack of evidence that detecting distal small bowel polyps influences patient outcome.
Using current guidelines as the benchmark, most centres in the UK appear to be underusing capsule endoscopy, an opinion shared by almost 70% of UK gastroenterologists who feel that available local services would increase use. Yet the calculated need for 45 capsule endoscopies per 250 000 population is likely to be a significant underestimate. Data suggesting that only 5% of patients with blood loss have a small bowel cause were published when small bowel investigative techniques had a poor sensitivity,2 11 12 since when capsule endoscopy studies show a high yield of small bowel pathology.13,–,17 The calculated need does not include the use of capsule endoscopy in less common indications (coeliac disease, malabsorption, polyposis syndromes). Furthermore, recent studies confirming better mucosal visualisation of small bowel inflammatory disease than comparators,20 and reflected in a B grade level of recommendation in updated European (2009) guidelines,5 may lead to further demand for use in Crohn's disease. Currently, the BSG guidelines recommend bi-directional conventional endoscopy to investigate anaemia in all but premenopausal women because of a dual pathology rate of between 1% and 10%.12 Demand may increase further if current trials conclude that ‘tri-directional’ endoscopy (including small bowel capsule endoscopy) is warranted to investigate anaemia.
One in five centres in the UK is limited in its use of capsule endoscopy by purchasers or its hospital trusts. This may be partly owing to inadequate reimbursement. Reference costs submitted to payment by results by trusts in 2008–9 were extremely variable and too low resulting in a tariff which barely covers the cost of the capsule. This may change for 2012–13 if the current round of reference costs submitted is more accurate. A similar problem seems to have beset the tariff for balloon-assisted enteroscopy, a highly specialised procedure taking more than twice the time of a colonoscopy, yet attracting a tariff of just over 30% more. A further impediment to the development of services is likely to be the addition of further workload to consultant contracts. Capsule endoscopy reading is time consuming, with an estimated 50 min required to read an average 4 h small bowel examination comprising 28 800 images.23
There are few studies which address training, competencies and accreditation in capsule endoscopy. Endoscopy naïve medical students perform less well than gastroenterology trainees,24 and variability in learning curves is recognised,25 suggesting that at least basic training in lesion recognition is required. To practise independently the ASGE requires completion of a 2-year training fellowship, upper and lower gastrointestinal endoscopy (including enteroscopy) competence, attendance at a hands-on training course and supervised reading of at least 10 videos.26 This is easier to achieve than in conventional endoscopy (which requires training in instrument handling) as image interpretation skills can be taught using de-identified training videos in a time-flexible manner, perhaps even using web-based learning.27 Even if UK training programmes adopt a higher minimum of supervised procedures before independent practice, accreditation in capsule endoscopy should be possible for most UK trainees. Many appear to be interested in learning capsule endoscopy, even allowing for the possibility that the survey responders were a select group.
Training is, however, a different matter from service delivery. Reading and interpretation of 45 videos a year may not add significant pressure to the existing workload, but competencies may be better maintained in centres with a higher throughput. However, if demand increases substantially, it might be possible to follow the lead of conventional endoscopy in which nurse endoscopists have taken a progressively more important role in service delivery.28 Several studies have shown that an experienced endoscopy nurse can identify capsule endoscopy pathology as reliably as a doctor24 29 and may even be trained to report and advise on management.30 Such an approach might allow doctors to focus on other aspects of patient management and training and allow cross cover.
Currently there are eight established device-assisted enteroscopy units in the UK with a further 14 centres beginning to develop services. One centre reports the need for one device-assisted enteroscopy per 17 capsule endoscopies31 such that 496 enteroscopies would be needed for 8430 capsule endoscopies. Assuming that developing services become established, this would equate to 23 procedures per centre per year, suggesting that existing device-assisted enteroscopy services are probably adequate at the present time.
Acknowledgments
The authors acknowledge the significant contributions of consultants and secretaries across the UK, who collated and provided them with the data.
References
Footnotes
-
Competing interests MEM has received support to attend conferences by Given Imaging Ltd. and received honoraria for lectures from Intromedic Ltd.
-
Provenance and peer review Not commissioned; externally peer reviewed.