Article Text

Abstract
Background and aims Endoscopy performance is dependent on the technical ability and experience of the operator. There is anxiety among surgical trainees that certification to perform independent endoscopy to agreed national standards by the date of award of certificate of completion of training is not achievable. The aim of this study was to evaluate the delivery of endoscopy training to UK-based general surgery trainees.
Materials and methods An electronic survey of general surgery trainees holding a national training number or in a locum appointment to training post between July and September 2010 was undertaken.
Results Two hundred and thirty-three trainees responded from all UK training regions. Stated subspeciality interests included coloproctology (47%), oesophagogastric/bariatric (22%) and hepatobiliary/pancreatic (10%) general surgery. 92% of trainees were training or planned to train in endoscopy, 62% of whom had registered with the Joint Advisory Group (JAG). Thirteen trainees had JAG certification in diagnostic upper GI endoscopy and eight in colonoscopy. There were high rates of dissatisfaction with endoscopy training nationally. Two thirds of trainees had no scheduled training lists. Conflicting elective/emergency commitments, competition and absence of training lists were the most common reasons for a failure to access endoscopy training.
Conclusions Higher surgical trainees are failing to achieve national standards for endoscopy practice. There is an urgent need to address the deficiencies in endoscopy training to ensure a competent cohort of surgical endoscopists.
- Endoscopy
- Surgical Training
Statistics from Altmetric.com
Introduction
The Joint Advisory Group on gastrointestinal endoscopy (JAG) was established in 1994 under the auspices of the Academy of Medical Royal Colleges to set standards for individual endoscopists and training in endoscopy and to provide quality assurance for endoscopy units and training courses.
The JAG working group sets standards for training and assessment in upper and lower gastrointestinal (GI) endoscopy, endoscopic retrograde cholangiopancreatography (ERCP) and endoscopic ultrasound (EUS), and currently awards certification of competence to individuals to undertake independent gastroscopy, flexible sigmoidoscopy and colonoscopy.
Recent guidance from the Association of Upper GI Surgeons and the Association of Coloproctology1 has emphasised the need to improve standards of endoscopy training in GI surgery, to ensure that there is parity in the provision of endoscopy training regardless of background discipline and that greater emphasis is placed on endoscopy training within the surgical curriculum.
Previous work by the author2 indentified that deficiencies are present in the delivery of endoscopy training. In light of these findings the JAG commissioned this review to evaluate the delivery of endoscopy training nationally among UK based general surgery trainees.
Materials and methods
An electronic survey (Survey Monkey(R) (Palo Alto, California, USA)) was designed to evaluate standards in endoscopy training: trainee demographics; engagement with the JAG (registration and certification rates and the use of regular summative assessment of endoscopy training); quality of endoscopy training and trainee satisfaction. In the absence of a direct measure of quality of training, parameters that the JAG uses to certify trainees and assess the quality of training delivered at individual units were recorded. These include use of simulation, course attendance, number of index procedures performed and the frequency of training and non-training lists.
Trainees holding a national training number or in a locum appointment to training post were contacted via their subspeciality organisation (the Association of Upper GI Surgeons and the Association of Coloproctology) and via programme directors. The JAG provided £500 as an incentive to take part in the survey. To be eligible for the award responders were asked to provide their name and email address after completing the survey. Only one response was allowed per applicant, with multiple entries leading to invalidation of that response and withdrawal from the draw. Responses were collected between July and September 2010. The recipient was selected at random once the survey had closed.
Results
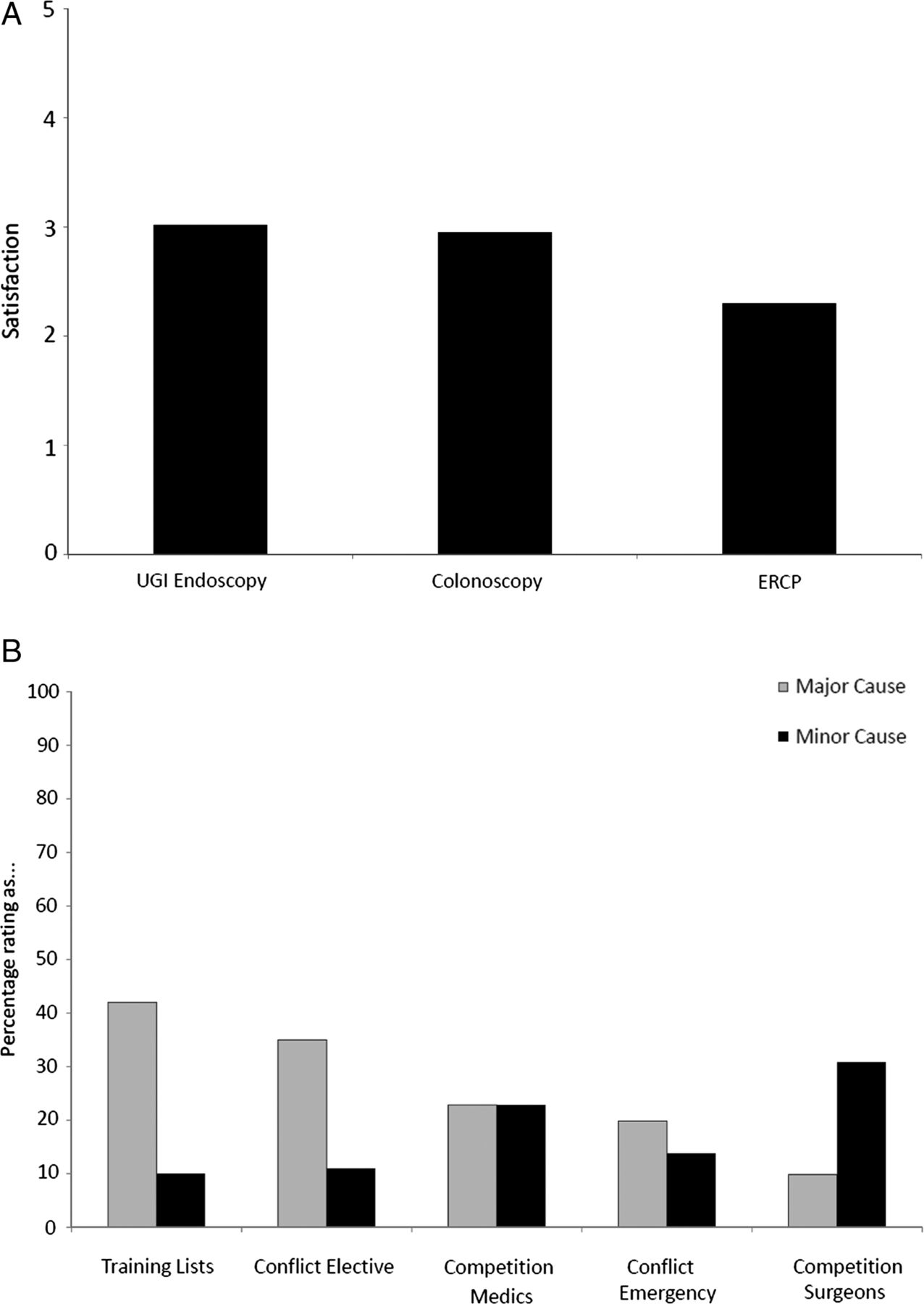
There were 233 responses (female:male 1 : 2.3). All deaneries were represented (median 10, range 4–39). All trainees were ≥ST3 Speciality training level (ST)3 and over 56% had completed at least 3 years of higher surgical training. Subspecialty interests included coloproctology (47%, n=108), oesophagogastric (OG) surgery (22%, n=50) and hepatobiliary/pancreatic (HPB) surgery (10%, n=23) (figure 1A). Ninety-two per cent of trainees expressed an intention to train in GI endoscopy (upper GI endoscopy (88%) and colonoscopy (72%)) (figure 1B).

Summarises the basic demographic data for this study. Subspecialty interests (A) and endoscopy preference (B).
Quality of endoscopy training
Sixty-one per cent of trainees wishing to train in endoscopy had used an endoscopy simulator prior to commencing endoscopy training. Eighty-nine per cent of trainees wishing to train in endoscopy had attended a JAG approved basic endoscopy training course (41% basic skills course in upper GI endoscopy and/or flexible sigmoidoscopy, 34% basic skills in colonoscopy, with the remainder having attended simulator-based courses). Seven per cent of trainees had attended an advanced course (intermediate/advanced colonoscopy, basic skills in therapeutic upper GI endoscopy or basic skills in ERCP). Two trainees had attended a ‘Training the Trainers’ course.
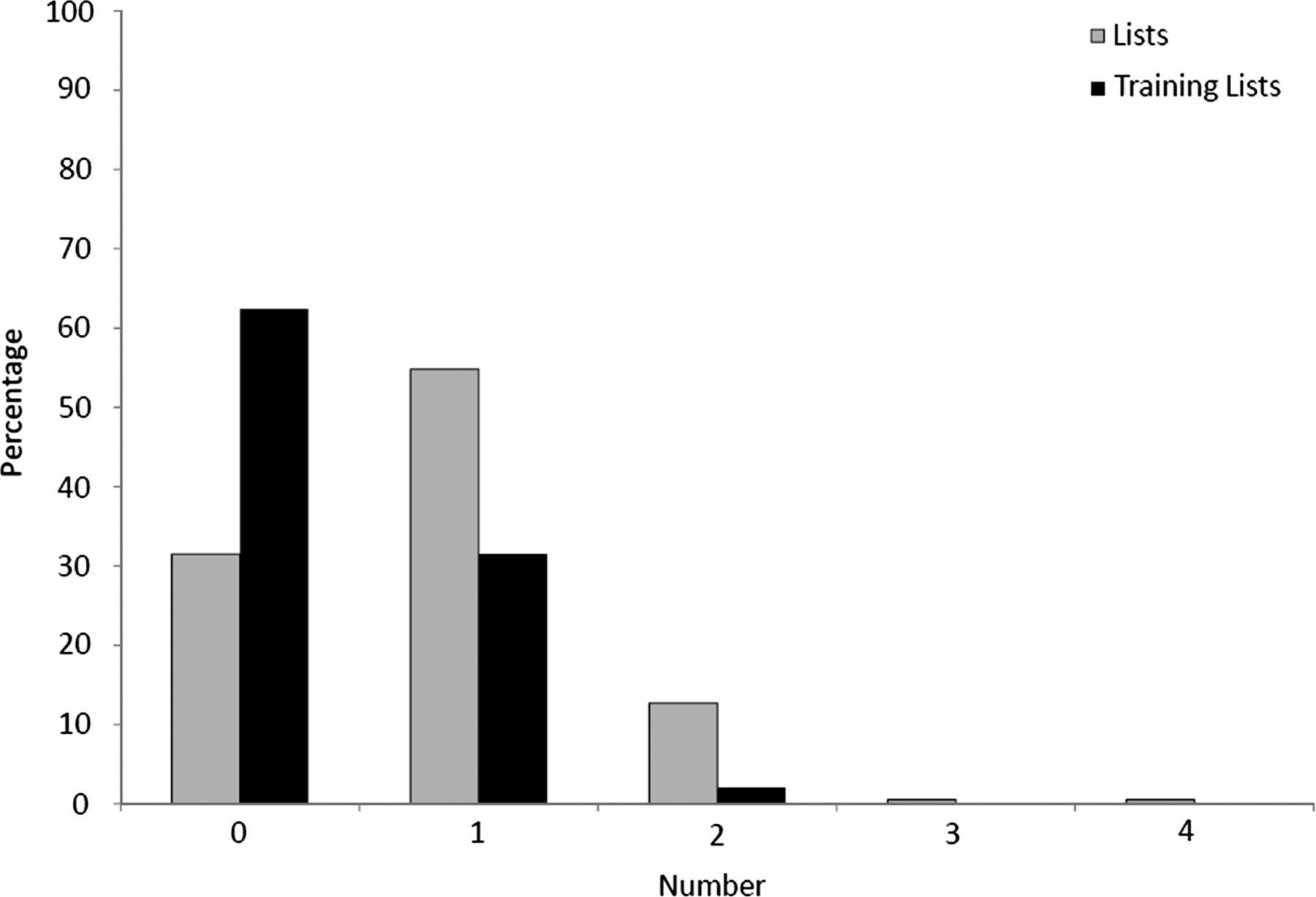
Regarding endoscopy lists, 51% of trainees attended one list per week and 13% attended two or more lists per week. Thirty-six per cent of trainees wishing to train in GI endoscopy attended no regular endoscopy sessions. Thirty-one per cent of trainees had one dedicated training list per week (a reduced volume list to enable additional time for training) with 2% trainees having two training lists per week (figure 2). These training lists occurred 33% of the time. Comparing junior (<year 3) and senior (≥year 4) trainees, senior trainees were more likely to have regular endoscopy lists, but were no more likely to have access to training lists.

Presents the number of endoscopy lists and endoscopy training lists accessed by trainees.
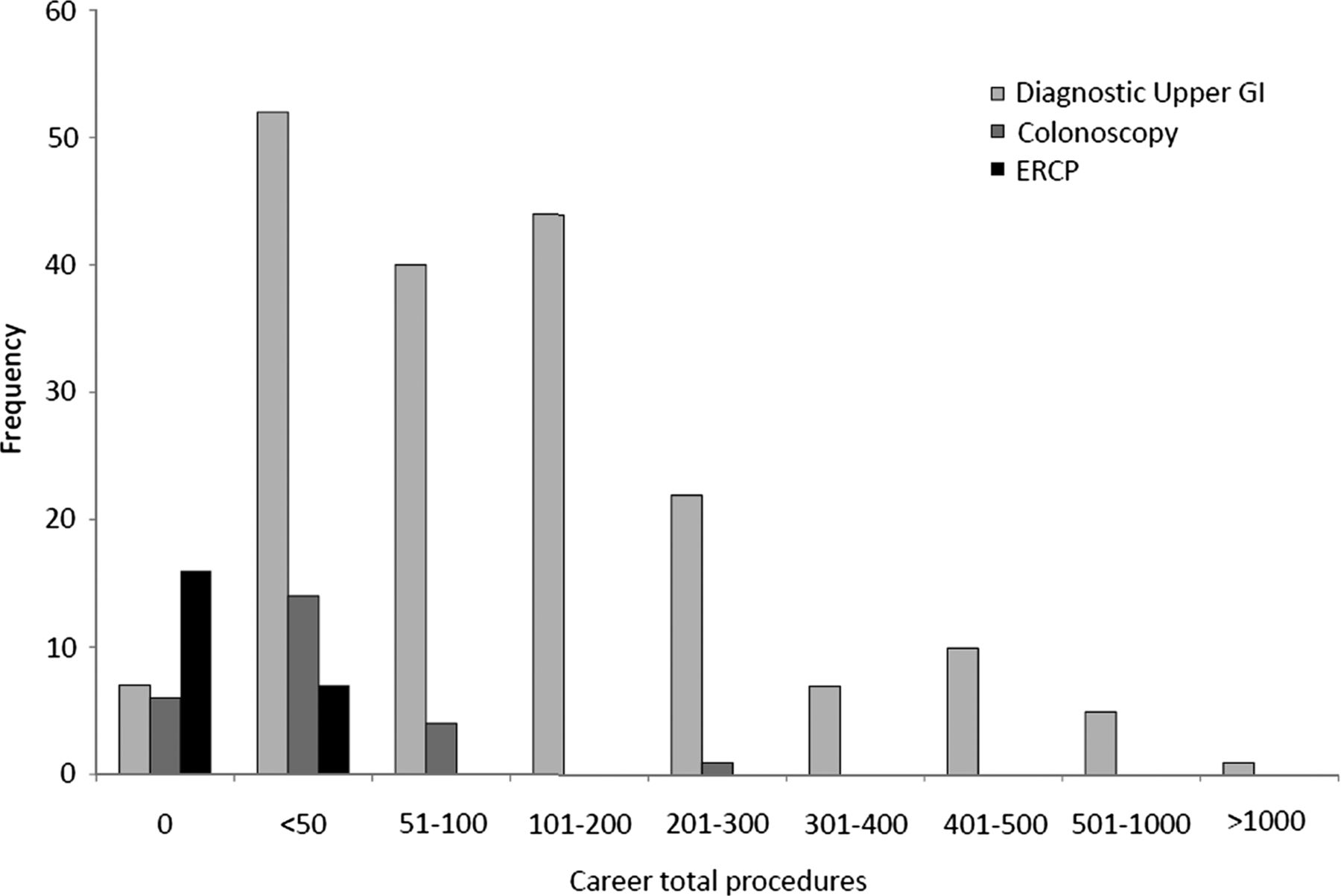
Concerning trainee volume (figure 3), 28% of trainees training in upper GI endoscopy had performed >200 diagnostic or therapeutic Upper GI endoscopies. Twenty per cent of trainees training in lower GI endoscopy had performed >200 flexible sigmoidoscopies and 22% had performed >200 colonoscopies. Twelve upper GI trainees had performed up to 50 ERCP procedures with none having performed >50. Six upper GI trainees had performed up to 50 EUS procedures with one trainee reporting experience with >500 EUS procedures. Of the 25 trainees who declared a non-GI interest, 17 and 15 stated that they intended to practice diagnostic upper GI endoscopy or lower GI endoscopy respectively, and 7 had registered their intention with the JAG. Of these two had performed >200 diagnostic upper GI endoscopies. None had performed >200 lower GI endoscopies.

Presents the lifetime endoscopy experience of the surgical trainees in diagnostic upper GI endoscopy colonoscopy and endoscopic retrograde cholangiopancreatography.
Engagement with the JAG
Ninety-four per cent of trainees were aware of the JAG, and of those wishing to train in GI endoscopy 62% had registered with the JAG. Twenty-one per cent of trainees undertook regular summative assessment of endoscopy training. JAG certification in diagnostic upper GI endoscopy had been achieved by 13 trainees (with subspecialty interests OG/HPB=5, coloproctology=5, general surgery=2 and breast=1). Certification in colonoscopy had been achieved by eight trainees (coloproctology=7, OG/HPB=1).
Trainee satisfaction with endoscopy training
Ten per cent of trainees <years 3, and 5% of trainees ≥years 4 were very satisfied with their training in diagnostic upper GI endoscopy, as compared with 30% and 24% who were very dissatisfied respectively (figure 4A). Ten per cent and 13% of junior and senior trainees were very satisfied with their training in lower GI endoscopy, compared with 31% and 18% very dissatisfied. Figure 4B presents reasons for trainees failing to access endoscopy training. Absence of allocated endoscopy training lists and conflicting elective surgical commitments were considered the most important factors for failing to access endoscopy training.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Presents the levels of satisfaction in endoscopy training expressed by the general surgery trainees by endoscopic technique (A) and reasons for failure to access endoscopic training (B).
Discussion
This study set out to review standards of GI endoscopy training among UK-based general surgery trainees. It demonstrates that there are deficiencies in the delivery and quality of endoscopy training and that these deficiencies may limit the ability of trainees to achieve competency in endoscopy prior to completion of training.
The imperative to comply with the European Working Time Directive and the ‘New Deal’ has reduced the time available for trainees to access endoscopy training. Additional demands on local endoscopy services and the participation of many proficient and motivated endoscopists in the National Bowel Cancer Screening Project may further compound the problem. In the future the roll-out of flexible sigmoidoscopy screening (‘Flexi-scope’)3 will generate additional service demands, while absorbing available training opportunities as a cohort of additional screening practitioners are trained.
It appears that trainees in medical gastroenterology, do not experience the same limitations in training; a recent national survey of 359 gastroenterology trainees indicated that over 70% have two or more timetabled endoscopy sessions per week, with nearly 60% having already completed the required summative assessment of competence in colonoscopy.4 In our review only 13% of trainees had this level of access to endoscopy training, and less than one third had dedicated training lists. As a result, the absolute numbers of procedures performed by surgical trainees are much lower than reported by medical gastroenterology trainees, and the proportion of surgeons who have completed summative assessments in colonoscopy and diagnostic upper GI endoscopy is much smaller. This situation is also reflected in data from the USA, where gastroenterology fellows have been shown to perform significantly more endoscopic procedures than surgical residents.4
In a 2004 cross-sectional study of colonoscopy practice in the UK, Bowles et al5 noted that only 12% of surgical consultants and 0% of surgical trainees had received supervised training for their first 100 colonoscopies. While this situation appears to have improved, our survey highlights that many surgical trainees are still left to perform procedures unsupervised, with 30% of junior trainees reporting that their trainers are never present for the entire list. Current surgical trainees have increased their participation in formal training courses, with 34% having attended a basic colonoscopy training course, as compared with 16% of those in Bowles’ historical cohort.
There was a failure of general surgery trainees to register and certify with JAG. Small numbers of trainees had achieved JAG certification for upper GI or lower GI endoscopy despite a larger proportion of trainees with experience of >200 upper or lower GI endoscopies. In addition only a small number of trainees undertook regular formative assessment, an essential component of the certification process.
Between 2002 and 2007, UK medical gastroenterology trainees noted marked improvements in the quality of their colonoscopy training, with 87% of 26 trainees reporting in 2007 that their training had been adequate or better than adequate, compared with 25% in 2002.6 In contrast 65% of surgical trainees in the current study were unsatisfied or very unsatisfied with their endoscopy training to date. Aside from an absence of allocated training lists, conflicting elective work commitments, and to a lesser extent competition from medical trainees were perceived to be the main barriers.
There are limitations to this study. Although a representative snapshot of endoscopy training among trainees in general surgery has been obtained, only one fifth of all higher trainees have responded.7 Since undertaking this review the JAG have made three key changes to how training and certification are assessed. They have switched from volume- based and competency- based to largely competency-based assessment. The certification process has been streamlined by the introduction of the JAG Endoscopy Training programme which provides an e-portfolio to record and validate summative assessments, courses and certification. In the future this will also synchronise with the Intercollegiate Surgical Curriculum Project to avoid duplicating the training record. The JAG has introduced the Endoscopy Global Rating Scale to evaluate the delivery of all aspects of the endoscopy service including training. The Association of Upper GI Surgeons and the Association of Coloproctology will review the impact of these changes on delivery of endoscopy training to UK-based general surgery trainees.
In order to address the deficiencies in the delivery of endoscopy training to UK-based general surgery trainees without reduction in the threshold of competence that is expected, the levels of engagement with the JAG must be improved and greater emphasis must be placed on the provision of endoscopy training to surgeons.
To improve trainee engagement, JAG has worked with subspecialty organisations to publicise its role in endoscopy training and certification. This must be an ongoing process. It is essential that all trainees with a GI interest wishing to train in endoscopy are required by their programme directors to register with JAG at the earliest possible stage, and to maintain an accurate, contemporaneous record of their endoscopy experience using the JAG e-portfolio. Trainees must be proactive in ensuring that they undergo regular formal appraisal of their endoscopy skills, and to clearly identify to their trainers and local training leads their individual training needs, and opportunities to gain the necessary experience at each stage of their training.
To improve the delivery of endoscopy training to surgical trainees, training in endoscopy must be balanced with other training domains for trainees with an interest in GI surgery either within timetabled weekly slots or within separate training modules. Trainees require frequent, consistent and protected sessions in which to develop their endoscopy skills to the standard required. Integration of endoscopic training into the surgical curriculum in this way is successful in increasing case volume.8 Endoscopy training should be carefully evaluated at the trainee's Annual Review of Competence Progression and the provision of endoscopy training to surgical, medical and nurse trainees should be formally evaluated by the JAG assessors at the time of unit accreditation by JAG.
Improved delivery of endoscopy training to surgeons also requires suitably trained, motivated trainers and enough list capacity at departmental level to allow protected time for training. While the ability to maintain a consistent trainer/trainee relationship in the traditional surgical model may facilitate early skills acquisition, it may be more advantageous to disregard traditional specialty boundaries and instead train with individuals from a range of professional backgrounds in order to experience a wider range of patients and pathologies. In addition, opportunities for simulation-based learning should be made available, as this has been shown to improve colonoscopy completion rates and completion times at the early stages of acquiring competency.9 Simulators have also been demonstrated to be effective aids to the acquisition of therapeutic endoscopic skills such as polypectomy and obtaining control of upper gastrointestinal bleeding.10
Attendance at a JAG approved basic skills course is a mandatory requirement for certification, however, a more intensive and longer duration focused training programme has been shown to produce an improvement in performance which is sustained at a median of 9 months follow-up.11 At a local level training lists should be provided with fewer cases to mitigate the extra time required with a trainee present. This may lead to conflicts with service delivery targets, but training should be seen as an investment and supported by local and national stakeholders. Furthermore, we believe that opportunities for endoscopy training should be provided for GI surgery trainees throughout higher surgical training, irrespective of the subspecialty of the post occupied by the trainee at the time. Trainees with a declared vascular or breast subspecialty interest could in return be released from timetabled endoscopy sessions to undertake directed activity of their own. Trainers from all backgrounds should be encouraged to attend endoscopy-specific ‘Training the Trainers’ courses, and senior trainees may also benefit from attending local endoscopy users groups and endoscopy department steering groups meetings, as engagement at a local level with the non-surgical endoscopy community should open further training opportunities.
Conclusion
Higher surgical trainees in the UK are failing to achieve national standards for independent endoscopy practice. To maintain a surgical presence in the endoscopy department urgent remedial action is required. Endoscopy training needs to be more consistent and flexible within a weekly timetable or in a modular structure and requires the support of stakeholders. Trainers need to be supported in their acquisition of training skills and greater emphasis needs to be placed on competency documentation rather than procedure volume as a benchmark.
What is new in this paper
-
This paper identifies deficiencies in the delivery of endoscopy training to UK-based general surgery trainees and outlines strategies to address these shortfalls.
Footnotes
JSH and NFSW contributed equally.
-
Contributors JSH and NFSW are joint first authors, conducted the study and wrote the paper. JNL and JRB are the senior authors and supervised the project. All authors contributed to the drafting process and have seen and approved the final version.
-
Funding JSH is funded by an NIHR Clinical Lecturer Award. The study was supported by the Joint Advisory Group on GI Endoscopy. This work was presented in part at the Association of Surgeons of Great Britain and Ireland, Bournemouth May 2011.
-
Competing interests JSH is the AUGISt President; NFSW is the Dukes’ Club representative on the JAG committee; JNL is the Head of School for the East Midlands (North) Deanery; JRB is former Chair of the JAG.
-
Provenance and peer review Not commissioned; externally peer reviewed.