Article Text

Abstract
Objective The aim of this study was to evaluate UK trainee experience in endoscopy for acute upper gastrointestinal bleeding (AUGIB).
Methods Data was prospectively collected from all patients presenting to South Yorkshire Hospitals with AUGIB from September 2011 to December 2011 and compared with data from 1996. Concurrently, all gastroenterology trainees registered with the British Society of Gastroenterology were invited to respond to a web-based questionnaire regarding their experience in AUGIB management.
Results 77% (589/766) of the patient cohort underwent endoscopy for AUGIB; 15% (90/589) were performed by trainees. 7.2% (9/125) of the out of hours endoscopy case load was performed by trainees; all were low-risk or medium-risk cases (pre-endoscopy Rockall score ≤4). During the study period, dual therapy was delivered by a trainee on only four occasions. Comparison with the 1996 cohort demonstrated a marked reduction in the number of trainee performed endoscopies (76% vs 15%; p<0.001). Questionnaires were returned by 51% (245/478) of British Society of Gastroenterology trainees. 81% (198/245) thought that <10% of the gastroscopies they had performed involved therapeutic intervention. 23% (57/245) felt they would not be competent in AUGIB endoscopy by completion of specialty training.
Conclusions This study demonstrates the decline over time in trainee experience in AUGIB endoscopy. It also highlights a lack of trainee exposure to more challenging cases, out of hours endoscopy and therapeutic procedures. Furthermore, trainees are concerned that a level of competency may not be attained during specialty training. We advocate reviewing UK endoscopic training provision for AUGIB to ensure that experienced endoscopists are produced to meet future service needs.
- ENDOSCOPY
- GASTROINTESTINAL BLEEDING
Statistics from Altmetric.com
Introduction
Acute upper gastrointestinal bleeding (AUGIB) is a common medical emergency that has a 10% hospital mortality rate.1 The incidence in the UK is around 103 cases per 100 000 adults/year.2 The treatment of this condition has made important progress since the introduction of emergency endoscopy and the development of endoscopic therapy for haemostasis.3 However, despite advances in management, national mortality figures have not significantly improved over the past 50 years.4
Recently, the British Society of Gastroenterology (BSG) has supported the restructuring of AUGIB endoscopy services throughout the UK. This is in response to a nationwide audit in 20075 which highlighted significant deficiencies and inconsistencies in the care of patients presenting with AUGIB. This was most noticeable in the out of hours (OOH) period, where it was found that patients attending hospitals with informal or ‘goodwill’ on-call endoscopy had poorer outcomes.4 ,5 Since then, there has been increasing pressure on UK hospitals to provide a formalised 24/7 consultant-led AUGIB endoscopy service. The 2014 national survey found that this has been achieved in 77% of gastroenterology units across the country;4 a marked improvement since 2007, when only 48% of units provided this service.5
While these results are encouraging, the impact that these changes have had on training in AUGIB management is unclear. Previous studies suggest that gastroenterology trainees, alongside other ‘craft’ specialty trainees, have suffered a reduction in procedural training time since the introduction of working time restrictions such as the New Deal (2003) and the European Working Time Directive (EWTD; 2009).6–8 However, the status of gastroenterology trainee experience in AUGIB management has not recently been objectively evaluated.
Therefore, the primary aim of this study was to examine AUGIB endoscopy practice within the South Yorkshire deanery to identify current trainee experience. We then compared this with a historical cohort from 1996, to illustrate how this has changed over time. The secondary aim was to report on trainee views nationally regarding their experience in AUGIB management, by means of a web-based questionnaire sent to all gastroenterology trainees registered with the BSG.
Methods
South Yorkshire AUGIB data
Definitions
AUGIB was defined as haematemesis, the passage of melaena and/or firm clinical evidence and laboratory support for acute blood loss from the upper gastrointestinal (GI) tract.5 The term ‘trainee’ refers to medical or surgical Specialty Registrar (Year 3+) doctors. ‘Non-trainee’ refers to consultants (medical and surgical), staff grade doctors (ie, those who have completed their Certificate of Completion of Training), general practitioners (GP) and nurse endoscopists who are competent to perform endoscopy independently. Stigmata of recent haemorrhage (SRH) included adherent clot, blood in the GI tract, varices with red spot/weal marking/nipple sign, dark spot in ulcer base, spurting or visible vessel.5 In line with the national audit,5 OOH endoscopy was defined as occurring between 17:00 and 08:00 weekdays and at any time on Saturday or Sunday. All-cause mortality was defined as death occurring up to 30 days post index AUGIB.
Participants
All patients who presented with AUGIB to five out of six hospitals that comprise the South Yorkshire deanery between 1 September 2011 and 31 December 2011 were included in this study. All five sites had a formal 24/7 consultant-led AUGIB endoscopy service. There were 12 gastroenterology trainees across the five sites, of whom none had protected training time on the on-call GI bleeds rota.
Cases were identified by means of International Classification of Diseases-10 code and by searching the endoscopy database at each hospital using specific search terms (‘GI bleed’, ‘upper GI bleed’, ‘gastrointestinal bleed’, ‘gastrointestinal haemorrhage’, ‘GI haemorrhage’, ‘haematemesis’ and ‘melaena’). Subsequently, demographic, clinical, laboratory and management data were reviewed and extracted from case notes. The Rockall score was calculated as previously described.9 Patients were followed up until the end of January 2012, allowing outcomes (rebleeding, mortality and surgery) within 4 weeks of index AUGIB to be assessed.
National BSG trainee survey
All gastroenterology trainees registered with the BSG (n=478) were contacted via email and asked to complete an anonymous web-based questionnaire. Respondents were asked to state their level of training and the total number of gastroscopies they had performed. Trainees were then asked to estimate the percentage (≤5%; 6–10%; 11–15%; 16–20%; >20%) of gastroscopies they had performed on patients with AUGIB, on patients hypotensive at the time of endoscopy and the percentage of therapeutic procedures they had performed. Finally, respondents were asked whether they felt they would be competent in AUGIB endoscopy by completion of specialty training. Potential respondents were contacted only once via email and were not subsequently followed up.
Statistical methods
Data are presented as percentages (numerator/denominator) and as median and IQRs. Statistical analysis was performed using the standard statistical software package SPSS V.18.0 for Windows (LEADTOOLS; LEAD Technologies, Charlotte, North Carolina, USA). Univariate analysis was performed by the χ2 test for frequencies and Kruskal-Wallis test for comparing medians. A p value of <0.05 was considered statistically significant.
Results
South Yorkshire AUGIB data
Patient characteristics
A total of 803 potential cases were identified during the study period. Of these, 37 cases had incomplete or missing data so could not be further evaluated. Therefore, a total of 766 eligible cases comprised the study sample for analysis (median age 65 years (IQR 47–79); 47% (358/766) female patients). Eighty-eight per cent (675/766) of patients presented to hospital with an episode of AUGIB during the study period, the remaining 12% (91/766) were already inpatients. Seventy-seven per cent (589/766) of patients underwent endoscopy, of whom 75% (443/589) underwent the procedure during their inpatient admission.
Of the cohort, 2.2% (17/766) had liver cirrhosis; 23% (176/766) of patients had no comorbidities. Thirty-six per cent (245/766) of patients were taking antiplatelets (aspirin, clopidogrel or dipyridamole) or anticoagulants (warfarin or low molecular weight heparin) at presentation. Sixty-one per cent (428/766) of the cohort were haemodynamically stable (systolic blood pressure ≥100 mm Hg; heart rate <100 bpm), 28% (196/766) had a tachycardia (heart rate ≥100 bpm) and 11% (83/766) were hypotensive (systolic blood pressure <100 mm Hg) at presentation of AUGIB.
Endoscopist training level
Fifteen per cent (90/589) of endoscopies were performed by trainees (table 1). Eighty-one per cent (73/90) were performed by gastroenterology trainees and 5.5% (5/90) by surgical trainees; specialty details were not available for 13% (12/90) of trainee cases. The median pre-endoscopy Rockall scores were similar between trainee performed (3 (IQR 1–4)) and non-trainee performed endoscopy (3 (IQR 2–4); p>0.05). Of those performed by non-trainees, 78% (391/499) of cases were performed by consultants; the rest were performed by either staff grade doctors, GPs or nurse practitioners.
Proportion of endoscopies performed per pre-endoscopy Rockall score by trainees and non-trainees during normal hours and OOH
Timing of AUGIB endoscopy
Trainees performed 7.2% (9/125) of the OOH endoscopy case load (table 1). All OOH trainee performed procedures were on low-risk or medium-risk patients (pre-endoscopy Rockall score ≤4). Conversely, all endoscopy OOH on high-risk patients (pre-endoscopy Rockall score ≥5) was performed by consultants (n=22).
Endoscopic diagnosis and intervention
A cause of bleeding was determined at endoscopy in 72% (421/589) of cases. There were no differences between the frequency of diagnoses found on endoscopy between trainee and non-trainee performed procedures (table 2). SRH was identified at endoscopy in 15% (91/589) of cases (11/90 of trainee and 80/499 non-trainee cases; p>0.05). Eighty-eight per cent (80/91) of cases with SRH had endoscopic intervention, of which 20% (19/91; 4 trainee cases and 15 non-trainee cases) received dual therapy.
Main endoscopic diagnoses
Outcomes from endoscopy
Rebleeding occurred in 1.6% (10/589) of the total cohort (8/499 non-trainee cases and 2/90 trainee cases; p=0.17). 2.2% (2/90) of trainee cases and 0.8% (4/499; p=0.39) of non-trainee cases required surgery following endoscopy. Crude mortality among patients undergoing endoscopy was 7.8% (46/589). Bronchopneumonia was the most common (19%; 9/46) cause of death in those who underwent endoscopy; refractory AUGIB was the cause of death in 4.3% (2/46) of patients. There was no difference between mortality from trainee performed (10%, 9/90) versus non-trainee performed procedures (7.4%, 37/499; p=0.38).
Comparison with a historical South Yorkshire AUGIB cohort
The cohort for comparison comprised 275 patients who presented with an AUGIB to two central Sheffield teaching hospitals between January 1996 and December 1996. All patients were new admissions; 45% (124/275) of the patients were female.
Trainees performed 76% (206/275) of AUGIB endoscopy in 1996, compared with 15% (90/589; p<0.001) in the current 2011 cohort. Timing of endoscopy was available for 182/275 cases from the 1996 cohort. Overall, there was a significantly lower proportion of endoscopy performed OOH in 1996 (12%, 21/182) compared with 2011 (20%, 118/589; p=0.008). However, trainees performed a higher proportion of the OOH case load in 1996 (81%, 17/21) compared with 2011 (7.2%, 9/125; p=0.001). Table 3 shows the comparative outcomes between the current and historical trainee cohorts. It is noteworthy that the registrars from the historical cohort involved in the on-call service had each undertaken more than 1000 upper GI endoscopies.10
Trainee outcomes in the current and historical South Yorkshire acute upper gastrointestinal bleeding (AUGIB) cohorts
National BSG trainee survey
Questionnaires were returned by 51% (245/478) of the BSG trainees (median registrar training years 4, range 1–9 years). The median number of gastroscopies performed by trainees was 500 (IQR 450–1000).
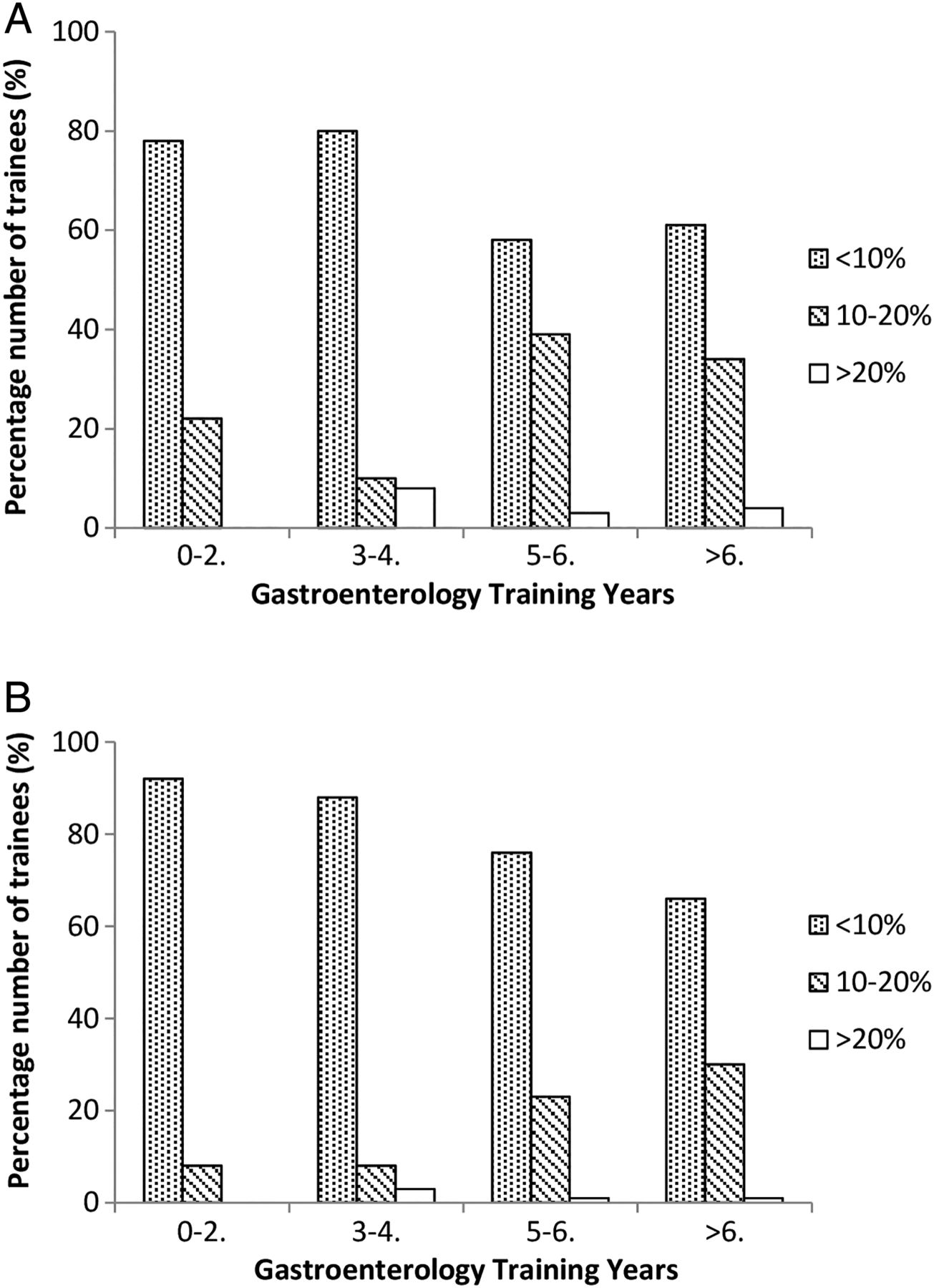
Senior trainees (≥5 years registrar training; n=95) thought that AUGIB cases and therapeutic endoscopy accounted for a greater proportion of their total upper GI endoscopy experience than junior trainees (≤4 years registrar training; n=150) (p=0.001; figure 1). Overall, 81% (198/245) of trainees thought that <10% of the gastroscopies they had performed involved therapeutic intervention. Eighty-six per cent (211/245) of trainees reported that ≤5% of their upper GI endoscopy training was on patients hypotensive at the time of the procedure.
{kind=link}
(Top) Experience of endoscopy for acute upper gastrointestinal bleeding (AUGIB) based on years of specialty training. Spotted bars represent that AUGIB cases accounted for <10% of total upper GI endoscopy experience, striped bars 10–20% and white bars >20%. Seventy-nine per cent (118/150) of junior trainees (0–4 registrar training years) felt that AUGIB cases represented <10% of their total upper GI endoscopy experience compared with 61% (55/90) of senior trainees (≥5 registrar training years; p=0.001). (Bottom) Experience of therapeutic endoscopy based on years of specialty training. Spotted bars represent that therapeutic cases accounted for <10% of total upper GI endoscopy experience, striped bars 10–20% and white bars >20%. Ninety-one per cent (137/150) of junior trainees felt that therapeutic cases represented <10% of their total upper GI endoscopy experience compared with 71% (67/95) of senior trainees (p=<0.0001).
Twenty-three per cent (57/245) of trainees felt that their skills in AUGIB endoscopy would be insufficient by the time of specialty training completion. Fifty-nine per cent (34/57) of those trainees had more than 3 years registrar training experience, indicating that this concern was not limited to the most junior of respondents. Fifty per cent (122/245) of trainees commented that registrars should have protected training time on the GI bleeds rota.
Discussion
This study demonstrates the decline over time in trainee experience in AUGIB endoscopy from 76% to 15%. It also highlights a lack of trainee exposure to more challenging cases, particularly in the OOH period. In a 4-month period over five hospital sites, dual therapy was delivered by a trainee on only four occasions. Furthermore, we report that a proportion of experienced trainees are concerned that a level of competency in AUGIB endoscopy may not be attained during specialty training.
We found that recent trainees performed fewer OOH endoscopies compared with trainees from the historical cohort. The emphasis on implementing a consultant-led service could be responsible for directing attention away from OOH training opportunities in AUGIB. However, it is more likely that current trainees are not afforded protected time on the GI bleeds rota because of time constraints imposed by the EWTD, alongside acute medicine rota pressures. This could have led to the global reduction in trainee exposure to AUGIB endoscopy that we report. Indeed, our unit has previously identified a 19% reduction in the number of trainee performed colonoscopies 6 months after the introduction of the EWTD.6 A number of other studies across a range of the craft specialties have also documented the decline in clinical training since the implementation of the working time restrictions.11–14 Furthermore, the latest BSG Trainees Survey found that 61% of respondents (n=263) felt that general internal medicine (GIM) duties had a negative impact on their gastroenterology training.15 Of note, recent trainees were more likely to be supervised when performing endoscopy than trainees from the historical cohort. This illustrates the potential learning opportunity that the consultant-led service can provide. Trainee rota pressures, however, may mean limited access to this resource.
In the current study, 88% of patients with SRH had endoscopic intervention, in whom only 20% received dual therapy. Trainees only performed dual therapy on four occasions. Previous studies have also reported low rates of dual endoscopic therapy.16 ,17 In the 2007 national audit,5 74% of those with SRH received endoscopic intervention, with 38% receiving dual therapy. It has been suggested that a lack of training may account for the shortfall in dual therapy, as adequate supervision can be difficult to provide in the setting of an unstable patient who requires such intervention.16 In support of this are the current regional trainee data and our findings that the majority of BSG trainees reported minimal experience of therapeutic procedures and endoscopy on hypotensive patients. A previous national survey of UK gastroenterology trainees found that 21% were unsatisfied with their current endoscopy training, mostly due to a lack of therapeutic training lists.18 Furthermore, 29% of respondents from the latest BSG Trainees Survey reported dissatisfaction with the standard of their advanced endoscopy training.11 In addition, a recent study conducted at our tertiary bleed unit19 reported that around 28% of patients with AUGIB with SRH received dual endoscopic therapy. This suggests variable use of dual therapy (albeit marginal) across the South Yorkshire deanery.
Taken together our findings suggest that training provision for AUGIB endoscopy has lagged behind the recent service provision improvements. This has left some trainees concerned that they will not reach a level of competence during their specialty training. These findings pose an important question: with increasing commitments to the GIM rota, how will training requirements for AUGIB (which will be required to provide a workforce for OOH services) be met? Protected time for senior trainees on the GI bleeds rota is a possibility, but is unlikely to be sustainable due to acute medicine rota pressures. Other options may include encouraging trainees to attend AUGIB lists on an ad hoc basis around current clinical commitments, and/or exposure to other therapeutic lists in order to develop transferable endoscopic skills. In either instance, the development of a strategy for trainees is paramount. In the context of the recently published Shape of Training Review,20 which supports the development of a broader specialist training scheme that is delivered through a shorter time frame, gastroenterology trainees may find it even harder to achieve competence in AUGIB endoscopy prior to Certificate of Completion of Training in the future.
There were a number of limitations to the current study. Endoscopy training has been the subject of much attention and change over the last two decades, through the revision of training guidelines and establishment of committees such as the Joint Advisory Group on Gastrointestinal Endoscopy. Inevitably, therefore, there are confounding factors that we have not been able to account for between the current and historical AUGIB data. Only 2.2% of our cohort of patients with AUGIB had liver cirrhosis versus 8.9% in the national audit.5 The former figure likely under-represents the true prevalence, due to the short study period. Finally, the historical AUGIB data is from only two of the six sites that constitute the South Yorkshire deanery, which may affect a direct comparison with the contemporary data (which comprise data from five sites).
During the current study, each gastroenterology trainee performed endoscopy on around five patients presenting with AUGIB. When extrapolated, this amounts to approximately 15/year, or 75 cases per trainee over the 5-year programme. What is clear is the actual and perceived lack of trainee exposure to more challenging cases, OOH endoscopy and therapeutic procedures. The Future Hospital Commission Report21 sets out a vision for future hospital services structured around the needs of patients, 7 days a week. In line with this we, therefore, advocate reviewing UK endoscopic training provision for AUGIB to ensure that experienced endoscopists are produced to meet future service needs. Failure to do so may hinder progress in reducing mortality from this common medical emergency and prevent us from providing the standard of care to which we aspire.
References
Footnotes
Contributors EW collected the data. HAP and MK analysed the data. HAP wrote the article. DSS designed the study, helped analyse data and write the article. All other authors helped collect data and revise the article.
Competing interests None.
Ethics approval This study was registered with the Sheffield Teaching Hospitals Clinical Effectiveness and Audit Department (08/03/2011).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data from this study has been previously presented at the BSG national conference.