Article Text

Abstract
Mood disturbances such as anxiety and depression are common in patients with inflammatory bowel disease (IBD), and impact negatively on their quality of life and disease course. An integrated multidisciplinary IBD team, which includes access to psychology and psychiatry opinion, makes possible the prompt recognition and management of psychological disturbance in patients with IBD. Based on our experience and existing literature, including systematic reviews of the effectiveness of available treatment modalities, a stepwise approach to the maintenance and restoration of psychological well-being is recommended, evolving upwards from lifestyle advice, through behavioural therapies to pharmacotherapy.
- inflammatory bowel disease
- psychological stress
Statistics from Altmetric.com
What is already known on this subject
Mental disorders such as anxiety and depression are very common in patients with inflammatory bowel disease (IBD), but IBD clinicians often lack confidence in their management.
Psychological membership of the IBD multidisciplinary team (MDT) is mandated by the UK IBD Standards but many services do not yet meet this target.
Of the available psychological therapies, cognitive behavioural treatment has the strongest evidence base for efficacy in IBD.
What this study adds
This guide provides a stepwise approach to psychological care in patients with IBD which all members of the MDT can use.
An overview of the management options for optimising mental well-being in IBD is given, ranging from lifestyle measures to a combination of psychological therapy and antidepressants.
How might it impact on clinical practice in the foreseeable future
Patients with anxiety or depression, depending on its severity, can be offered psychological therapy and/or started on an antidepressant by the IBD clinician alongside referral to psychiatry, if appropriate.
This practical guide will help all members of the IBD MDT provide holistic care and improve psychological wellbeing in patients with IBD.
Introduction
Psychological stress and mood disorders are common in inflammatory bowel disease (IBD).1 2 In recent surveys, people with IBD have reported that they want more attention paid to their emotional needs.3–5 In busy gastroenterology clinics, however, psychological needs may be overlooked, and the negative impact of stress or low mood on the quality of life (QOL) and course of patients’ IBD underestimated. Furthermore, the gastroenterology care team may lack the necessary training and confidence to assess and treat patients suffering from psychological distress, anxiety and depression (definitions in table 1).
Plain English explanations of psychological disorders and psychological therapies
After a brief overview of the prevalence of mood disorders in patients with IBD, we shall outline what is known of the mechanisms underlying the bidirectional relationship between mood disturbances and IBD. We shall then describe how the IBD team can offer holistic care—from the time of diagnosis and across the lifespan, maximising the chance of prompt recognition and treatment of mood disorders when they arise. We shall conclude by offering practical suggestions about how to provide a stepped care approach to prevention and management of mood disturbances in patients with IBD. As we shall mention later, there is limited trial data on the effectiveness of some of the available therapeutic modalities in the specific context of IBD. Our recommendations are therefore based additionally on evidence of how best to treat comorbid mental disorders in other long-term conditions, and on our clinical experience.
Prevalence of, and risk factors for mood disorders in IBD
Mood disorders are more common in people with IBD than in the general population. In two large recent meta-analyses including over 30 000 and 1 50 000 patients, respectively, the prevalence of symptoms of anxiety in IBD was 32%–35%, and of depression 22%–25%,1 2 with figures for established anxiety and depression being 20% and 15%, respectively. Differences in the provision of psychiatric support at local community level make it hard to quantify with precision the impact of these disorders on IBD outpatient and emergency services in the UK. However, reports from Australia, the USA and the UK suggest that an integrated psychiatric service for patients with IBD, offered along the lines we advocate below, may reduce this impact and its related costs.6–8
At increased risk of mood disturbance are women, elderly patients9 and those with Crohn’s disease, a severe disease course, active disease or comorbidities. This risk is influenced by illness perceptions, coping strategies, past experiences and social support.10 11 Emotions such as distress, grief, guilt and denial are common and should be routinely anticipated.9 12 Functional gastrointestinal symptoms and fatigue in quiescent IBD and in the absence of anaemia or nutritional deficiencies, are much more common than in the general population and are associated with psychological morbidity.13–15 Their presence should thus alert healthcare professionals (HCPs) to possible mood disturbance.
A recent systematic review with meta-analysis suggested that, contrary to widespread belief, mood disorders are less common in children and adolescents than in adults.16 It should be noted, however, that young people suffering from psychiatric morbidity may present differently from adults: for example, use of psychotropic drugs, non-adherence to IBD medications,17 eating disorders and failure to attend follow-up clinic appointments commonly reflect mood disorders in adolescents.
In active IBD, gut symptoms are often associated with food intake, leading to restrictive eating behaviour. Disordered eating behaviour is more prevalent in patients with IBD than in the general population and persistent abnormal food intake, especially in the absence of active disease, should alert the clinician to a possible eating disorder.18 19
Recent reports from all over the world indicate that the COVID-19 pandemic has increased psychological stress and symptoms of anxiety and depression in patients with IBD, particularly in younger people and in those with pre-existing mood disturbances.20 During the pandemic, it has been difficult to provide prompt access for patients to hospital IBD services, especially face to face, and it is important for their well-being to maintain availability of IBD nursing and psychological support as far as possible, and to provide them with information about the interactions between COVID-19, IBD and its treatment.21–23
Bidirectional links between mood disorders and IBD
The links between mood disorders and IBD are bidirectional.24 Thus, while IBD can pose a potent threat to psychological well-being, antecedent depression and anxiety may predispose to the development of IBD, particularly Crohn’s disease.25 Furthermore, several studies have indicated that incident psychological disorders can trigger relapse, worsen disease course and impair response to treatment in IBD.24 26–28 Conversely, improvement of psychological well-being on induction of remission29 and a beneficial effect of antidepressant use on IBD disease course use30 have also been documented. Whether psychological disorders should be regarded as an extra-intestinal manifestation of IBD, for example, mechanistically linked via the gut-brain axis to mucosal inflammation and the gut microbiome,31 is beyond the scope of this paper.
The practical implications of the bidirectional links between the gut and brain in IBD are fourfold. First, treating psychological disorders in patients with IBD may improve their mood and QOL, and the natural history of their IBD.32 Second, recognition that patients with IBD are at risk of psychological disturbance at particular times in their disease course should focus the care provider on enquiring for symptoms indicative of mood disorder at such psychological ‘pressure points’. Third, given the clear relationship between mood disturbances and active IBD, in order to optimise psychological well-being, every effort should be made to maintain patients in clinical remission. Lastly, and more speculatively, it is possible that further understanding of the links between the brain and gut may in the future open new approaches to the management of both IBD and its associated mood disturbances.
Management
The need for change in IBD service provision
Patient numbers in IBD clinics are rising and many services can offer only limited time for consultations. Most gastroenterologically trained HCPs have had little or no training in how to recognise or manage psychological aspects of IBD33 as they evolve during the course of their illness.
Integrated biopsychosocial model of IBD care
There is consensus that integrated care offers an ideal framework to meet patients’ biopsychosocial needs.3 33 In the UK at least, we are far from reaching this ideal: a recent survey organised by Crohn’s and Colitis UK showed that only 2% of IBD services have sufficient support from psychologists to meet the UK National IBD Standards.5 HCPs with special expertise in the diagnosis and treatment of psychological disorders may include psychiatrists, psychologists, counsellors, psychiatric nurses, social workers and others.33 Including such HCPs in the multidisciplinary team (MDT) enables the prompt provision of personalised psychological therapies and is welcomed by patients.5 34 It also leads to the diffusion of their specialist skills towards other members of the team. Lastly, since patients with IBD with a co-existing mental health diagnosis incur significantly greater overall IBD healthcare costs than those without,6 provision of an integrated IBD MDT may reduce rather than increase net costs, for example, by reducing attendances of patients with IBD to emergency departments.3 6
Stepped care for the recognition and management of psychological disorders in IBD
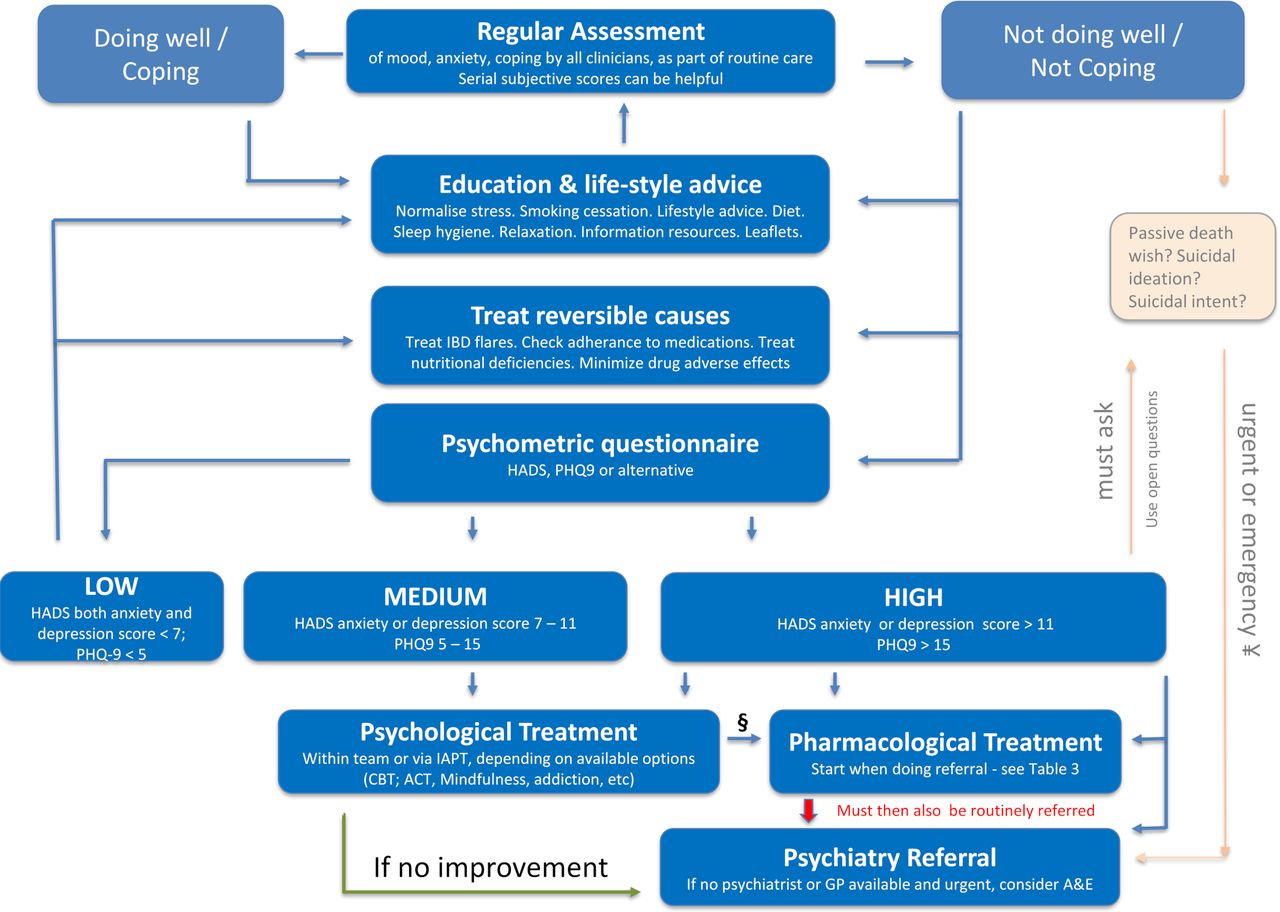
Living with IBD brings physical symptoms and uncertainty over a lifetime. Self-management with discussion between patients and HCPs to agree treatments, increases patients’ sense of control and, for most people, will reduce psychological burden. In busy IBD clinics, psychological distress is easily overlooked35 but it is everyone’s job within the MDT to assess patients regularly for mood disorders. There are several guiding principles for managing this task, which can be followed in a stepwise approach (figure 1).
Regular assessment of mood normalises the concept of stress (see below) and promotes engagement while reducing perceived stigma and reluctance to discuss ‘emotional stuff’. Ask open questions (“how are you doing generally?”) then more specific ones (“describe your mood lately; how are your stress levels?”) that alert the team that a person feels overwhelmed.
{kind=link}
This figure serves as a guide for the steps than can be taken in the psychological care of IBD patients by all members of the MDT. HADS or other psychometric scores can be used in adult patients (over 18) to alert clinicians that patients need help, but scores alone are not diagnostic of mood disorders and the decision to treat always depends on physician judgement and patient preference. § Some patients with mild to moderate depression may benefit from pharmacological together with psychological treatment; the decision will depend on symptom load. ¥ Patients with a passive death wish could be referred for routine or urgent psychiatric evaluation. For patients with current suicidal ideas or active suicidal intent an emergency (same day) referral must be made. ACT, acceptance and commitment therapy; A&E, accident and emergency department; CBT, cognitive behavioural therapy; GP, general practitioner; HADS, hospital anxiety and depression scale; IAPT, improving access to psychological therapies; IBD, inflammatory bowel disease; PHQ-9, patient health questionnaire 9.
Identify also the patient’s narrative about their IBD: age of first symptoms, time taken to IBD diagnosis, disruption to a person’s identity, relationships, education/employment, treatment failures and current concerns (about intimacy, fertility, surgery, cancer). A shared family narrative where relatives had negative IBD experiences (‘the doctors missed this; bad surgery’) may inform the patient’s current overview.
Measurements of patients’ subjective anxiety are useful. Ask them to score this out of 10; 0 is none, and 10 is the most anxiety possible, and record these in a series of anxiety scores: score at time of first diagnosis, perisurgery, times of severe IBD or a family crisis, etc, as this can provide comparative information about how someone is currently managing.
Measure subjective mood too. Most of us on most days carry a subjective mood of 8/10 (0 is the worst possible; 10 is the happiest day of our life). Ask the difficult closed question: “your mood now is 3/10, do you ever wish you could go to sleep and not wake up?” A yes answer indicates a passive death wish, and alerts the clinician that a patient feels overwhelmed or depressed. “Is this fleeting or constant, and did you think you might act on these thoughts?” For patients with a passive death wish that has led to suicidal ideation, referral for psychiatric evaluation should be considered. If they are already engaged in mental health services, direct them back to this care. Psychiatric referral becomes urgent in patients with current suicidal ideas or active suicidal intent. If prompt assessment by the mental health team or GP is unavailable, consider referring to accident and emergency department. Know also your local mental health crisis phonelines, and provide these plus national helplines (table 2).
Mental health support available in the UK
Education and lifestyle advice benefit everyone. Normalise psychological reactions: stress and distress are common with all unpredictable, painful long-term conditions—and IBD disrupts key social activities (eating with others, visits to bathroom, dating). There is some evidence for the benefits of smoking cessation, gentle exercise 3–5 times a week and sleep-hygiene including avoidance of stimulants, in general populations36 and patients with irritable bowel syndrome.37 Patients’ perspectives are key: if they perceive high stress and/or judge their social supports to be poor, respond with achievable lifestyle changes and problem solving. Apps such as MyIBDCare38 and MyIBDCoach39 can be used to nudge patients to make positive changes.
Functional GI symptoms are common in IBD, occurring in a quarter of patients in deep remission and associated with psychological comorbidity.13 A diet low in fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAPs) may provide relief of these gut symptoms in quiescent IBD and improve food-related QOL.40
In our experience, early discussion of these lifestyle and other social interventions helps many patients cope with their current stress and facilitates later discussion of antidepressants if low mood and anxiety fail to improve.
Treat reversible causes of psychological distress: active IBD is associated with increased psychological distress1 2 and should be assessed and treated where possible.29 Anaemia in patients with IBD is often associated with both depression and fatigue, and its treatment can improve QOL in general and psychological state and fatigue.41 42 Systemic steroids can adversely affect mood43 and should be avoided/withdrawn where possible. However, do not limit thinking to the two ‘boxes’ of IBD severity and mental disorders: many other factors drive poorer QOL. These include poor diet, addictions and social stressors such as poverty, insecure housing and relationship breakdown.
Psychometric questionnaires are useful for identifying the presence and severity of adverse mood symptoms and low mood should trigger their use. The result obtained can direct referral for psychological and/or psychiatric assessment.35 A range of validated options is available: we favour the Hospital Anxiety and Depression Scale (HADS),44 because it is quick and easy to complete, is widely used and does not include somatic symptoms which could reflect IBD activity rather than mental state. CORE1045 is a good tool for its brevity. Across primary care and psychological services, the Patient Health Questionnaire 9 (PHQ-9)46 and Generalized Anxiety Disorder 747 are widely used. These psychometric scores have been validated in adults and cannot be used in children (under 18 years of age).
Psychometric questionnaires alone are not diagnostic and cannot be a substitute for a conversation as they do not necessarily reflect an individual’s personal context or understanding of their situation. Some patients will score well on a measure but feel they cannot cope, while others who score badly may feel they are managing well and do not want specialist support.
Psychometric scores
HADS scores can be used to alert clinicians that a patient needs intervention. A decision to treat always depends on physician judgement and patient preference, hence the below HADS cut-offs are used to serve as a guide to the symptom burden and risk level of these patients. In addition, individual services may have differing capacity and referral criteria.
Low
For patients with low psychometric score (HADS score <7 on both the anxiety and depression scales; PHQ score <5), no specific psychological treatment is recommended and they should be encouraged to follow the lifestyle interventions described (figure 1).
Medium
When mood or anxiety symptoms are persistently impinging on functioning, referral for more specific psychological treatment should be considered. This corresponds to medium psychometric scores: HADS score 7–11 on either the anxiety or depression scale; PHQ-9 score 5–14.
High
For patients with severe anxiety or depression, corresponding with a HADS score >11 on either scale, or PHQ-9 score >15, we recommend referral for psychological treatment and that clinicians consider, based on their clinical impression, an antidepressant. This can be started by the IBD doctor or IBD nurse prescriber, and should be accompanied by referral to a psychiatrist.
Psychological treatments
There is limited good quality research into the effects of psychological interventions on mood, QOL and disease course specifically in patients with IBD, and conclusions drawn are generally mixed. Additionally, an intervention shown to be effective when given to populations of patients with IBD may not be beneficial in a given individual in which a range of different factors may be contributing to their psychological distress.12 48 Conversely, despite lack of evidence from trials, particular psychological interventions might be of benefit in an individual patient with IBD.49 Notwithstanding this practical limitation of the therapeutic application of trial data, the following psychological treatments can be offered to patients with IBD.
Cognitive behavioural therapy (CBT) has a strong evidence base in the general population.50 51 In IBD, the best available evidence for psychological therapies on psychological well-being is for CBT, which has been shown to improve QOL, at least briefly. In systematic review and meta-analyses, however, CBT has no clear effect on anxiety or stress in patients with IBD.52–54 The studies demonstrating benefit were done in patients with quiescent disease and there is very limited data with mixed results in patients with active disease.53 54
Mindfulness-based therapies have a modest effect in IBD on QOL, stress and depression but have no effect on anxiety.54 55 CBT can be combined with mindfulness and in one recent randomised controlled trial (RCT) was shown to reduce psychological symptoms and fatigue in patients with mild-to-moderate Crohn’s disease.56
Hypnotherapy has given mixed results in IBD, with improved QOL in one and non-significant improvement in another study.54
Acceptance and commitment therapy (ACT) is a newer treatment57 58 that thus far has a limited evidence base, but is showing promise for use in long-term conditions.59 In one RCT of patients with quiescent and active IBD, it was shown to reduce stress, perceived stress and depression, but not anxiety.60
Notwithstanding the results of some individually reported studies, none of these psychological interventions has been shown to improve IBD disease activity or course in systematic reviews.54
Accessing psychological therapies
The decision for referral for psychological treatment should consider motivation for change and ability to engage with the proposed psychological intervention. Few interventions will lift the mood of someone in a toxic relationship or of a heavy drinking, isolated patient.
Psychological therapy can be provided from within the team, if the IBD MDT includes a psychologist or psychotherapist. If this is not available, in England, everyone aged 18 years and registered with a GP can access NHS psychological therapies using improving access to psychological services (IAPT) (table 2), via GP or self-referral. IAPT services offer a range of talking therapies including CBT. A minority of patients will not improve with these CBT interventions and will be referred on by IAPT to specialist mental health services.
Antidepressants
There is a reluctance among physicians to prescribe antidepressants, probably as a result of their lack of experience in this area, but they are very effective in treating anxiety and depression.61 While evidence for the efficacy of antidepressants in improving mood in patients with IBD62 is less clear, this is in part because there have been only a small number of studies, including limited patient numbers. Some benefits have been identified and include improving QOL, managing associated functional GI symptoms, improving sleep, reducing chronic pain and (with some antidepressants) potentially favourable immunoregulatory effects.62 Despite the limitations of existing data relating to the use of antidepressants in people with IBD, there is good evidence that they are effective in other chronic illnesses.63
Our practice is to encourage gastroenterologists to start antidepressants for patients with a HADS score >11 on either the anxiety or depression axis, and in parallel with psychiatric referral. Regular review by psychiatry of response to antidepressants, identifies non-responders and risk of suicidal behaviours. A practical guide for prescribing antidepressants is given in table 3.
Guide to prescribing first-line antidepressants
For the general population, CBT is recommended as treatment for mild-to-moderate depression; however, for long-term conditions including IBD, the National Institute for Health and Care Excellence recommend that CBT combined with antidepressants works better than either alone.63 Meta-analysis of treatment of depression in patients with IBD also shows that combined therapy showed greater benefit than either alone.64
Discussion
Two major challenges hinder the optimisation of the management of patients with IBD and psychological comorbidity. The first is to ensure that the IBD team in every centre includes in-built psychological and psychiatric support, in line with recommendations in the UK National IBD Standards. This is to share in the care of patients with IBD when appropriate, and, as mentioned earlier, to make possible regular in-house training of non-specialists in how to manage comorbid mood disorders. Those seeking to persuade hospital managers of the need to expand their IBD team in this way can remind them that this is a cost-reducing move.6 7
The second, less immediately tractable problem is to rectify the paucity of currently available high-quality data, as mentioned above, to guide treatment decisions. Indeed, for this reason, some of the present recommendations should be regarded as expert advice based on clinical experience rather than following directly from published evidence. Reasons for the inadequacy of current trial data have been reviewed elsewhere,49 and in part reflect the ‘one-size-fits-all’ principle necessary for RCTs. Thus, even if the substantial difficulties associated with the design of trials to assess the efficacy of psychological and pharmacological therapies can be overcome, there will remain the need to tailor therapy to the individual patient, for example, to the stage of their adjustment to their IBD.48
Psychological comorbidity has a major negative impact on the lives of people with IBD. In this paper, we have set out a stepwise approach, based on our own practice, to identify and manage psychological stress and mood disorders in patients with IBD. This approach should be adopted by every member of the IBD team, with the aim of providing holistic and individualised care throughout the course of the IBD of the patients attending their clinics. Not everyone who works in the team will feel confident about how to proceed when faced with a distressed patient in a time-limited clinic, and we hope that the advice and the algorithm provided here (figure 1) will help guide their response.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Footnotes
Contributors All authors were responsible for design of study, data collection and critical revisions to the manuscript. KBK, PB, PM, DSR: data analysis and authorship. DSR and PB original idea.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- UpFront