Article Text

Abstract
Introduction The measurement of the quality of colonoscopy has been in the vanguard of quality improvement. The Joint Advisory Group on Gastrointestinal endoscopy (JAG) has issued guidance for practitioners to achieve caecal intubation rates (CIR) of ≥90% and to undertake ≥100 colonoscopies per annum. The British Society of Gastroenterology National Colonoscopy Audit published in 2012–2013 demonstrated a combined CIR of 92.3%. In 2012, we published data from 16 064 colonoscopies showing a combined CIR of 90.57%—both meeting JAG's standard. Analysis of our audit looked at the relationship of volume and outcome. CIR of operators performing ≥100 procedures per annum was 91.76%; those performing <100 was 87.77%. The 2-year data we collected involved 120+ operators. This provided an opportunity to study the correlation between volume and CIR in detail.
Methods We analysed 129 operator records who had undertaken 20–399 procedures per annum (total 12 594). Each operator's volume was plotted against CIR as individuals and groups of operators undertaking a similar annual volume. 9859 procedures (78.3%) were performed by operators undertaking 20–199 procedures per annum (120 operators); this subgroup was further analysed.
Results When plotting individuals and groups of individuals who have undertaken a similar annual volume against CIR, the trend-lines cross a 90% CIR at a volume of 120–125 procedures. The subgroup analysis showed the trend-line crossing at 110–120 procedures.
Conclusions This detailed analysis of 12 594 colonoscopies over 2 years suggests that JAG should advise operators to undertake ≥120 procedures per annum to support the quality standard for CIR of ≥90%.
- COLONOSCOPY
Statistics from Altmetric.com
Introduction
The measurement of quality of colonoscopy has been in the vanguard of quality improvement, with two large UK based audits describing key performance standards.1 ,2 The Joint Advisory Group on Gastrointestinal endoscopy (JAG), an inter-collegiate body responsible for standards, quality and training, has issued guidance for caecal intubation rates (CIR) of 90% or higher on an intention-to-colonoscope basis.3 They also advise that practitioners should undertake at least 100 colonoscopies per annum. The published audits have compared the data collected with these standards.
In February 2011, the British Society of Gastroenterology undertook a prospective National Colonoscopy Audit to assess quality standards, which included metrics such as CIR, sedation practice, comfort scores, perforation rate and adenoma detection rate. It looked at over 20 085 procedures across the UK over a 2-week period. The study published in 2012–2013 demonstrated an overall CIR of 92.3% meeting JAG's standard.1
In May 2012, we published data from 16 064 colonoscopies—a multi-centre retrospective audit of practice from a 2-year period, 2008–2009, showing a total CIR of 90.57%, also meeting JAG's standard.2
Analysis of this audit looked at the relationship of volume and outcome. We compared combined CIR of operators meeting JAG's guidance of performing 100 or more procedures per annum (91.76%) against those performing fewer than 100 procedures per annum (CIR 87.77%). The gap in performance against this key standard was not surprising as the relationship of volume to quality and outcomes is well established, and has been used in England as the basis to reorganise vascular services and other complex specialities over the past few years.4
The detailed data we have collected from a 2-year period involved over 120 operators. This provided an opportunity to study the correlation between volume of practice and CIR. We were therefore able to test JAG's standards and guide operators appropriately on volumes of colonoscopies an operator should aim to undertake per annum in order to ensure quality standards are maintained.
Methods
Prospectively recorded data from all colonoscopies undertaken (symptomatic, surveillance and bowel cancer screening programme (BCSP) procedures) were retrospectively collected from six hospitals in three regions (North Northamptonshire, Leicestershire and Coventry/Warwickshire).
Data were collected by use of audit tools for Unisoft software (Unisoft Medical Systems, 7 London Road, Enfield. Middlesex EN2 6BN UK) and Fujinon Adam software (Fujinon (Europe) GmbH, Halskestraße 4, 47877 Willich, Germany).
The audit took place from 1 January 2008 to 31 December 2009. Data have been collated and analysed using Microsoft Excel software.
There were 120 operators who undertook between 1 and 1257 colonoscopies over the 2-year period (total number 16 064 procedures). When looking at 2008 and 2009 as separate 12-month periods and combining these records, there are 191 operator records who undertook between 1 and 730 colonoscopies per 12-month period.
Operators who have undertaken less than 20 procedures or 400+ procedures per annum were excluded—these groups are outliers as the correlation between volume and practice at the extreme ends of the scale are not meaningful to the majority of operators currently practising. One operator was excluded as of the 200 procedures undertaken in the 2 years, 138 were recorded as ‘complete’ (without accurate description of the landmark reached). Finally, 67 procedures were excluded as they were recorded under generic logins and represent many operators undertaking procedures on training courses or before they are assigned their own logins on starting new posts.
The remaining 129 operator records have undertaken between 20 and 399 procedures per annum (total 12 594 procedures). Consultants (all practising independently) comprise 66 of the 129 records. Each operator's volume per annum was plotted against CIR. This was plotted as individual operators (figure 1) and groups of operators undertaking a similar volume per annum (20–49, 50–99, 100–149, 150–199, 200–249, 250–299, 300–349, 350–399—groups of 50, figure 2).
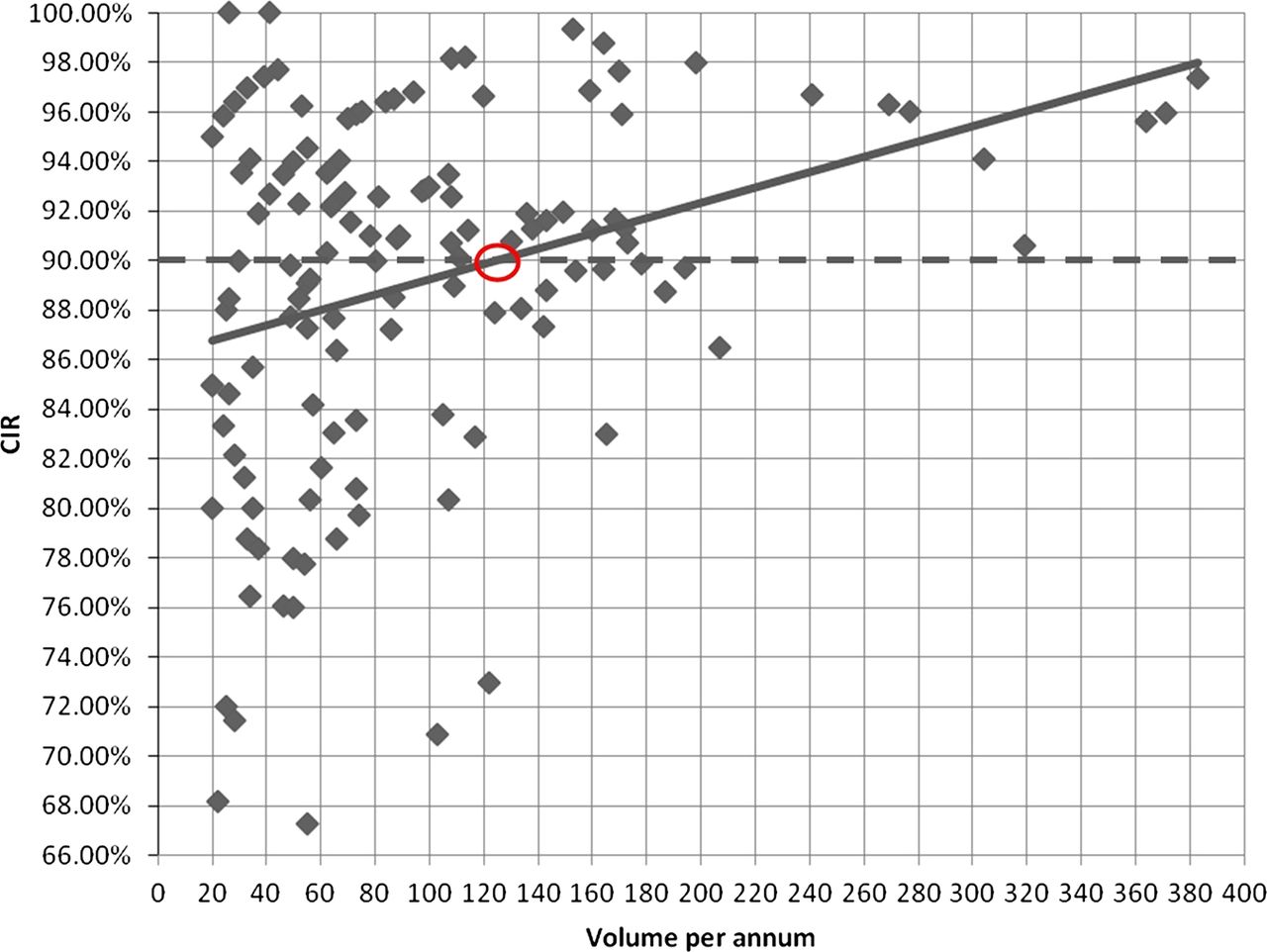
Scatter chart of individuals’ volume against caecal intubation rate (CIR).
Scatter chart of individuals’ volume (grouped in 50s) against caecal intubation rate (CIR).
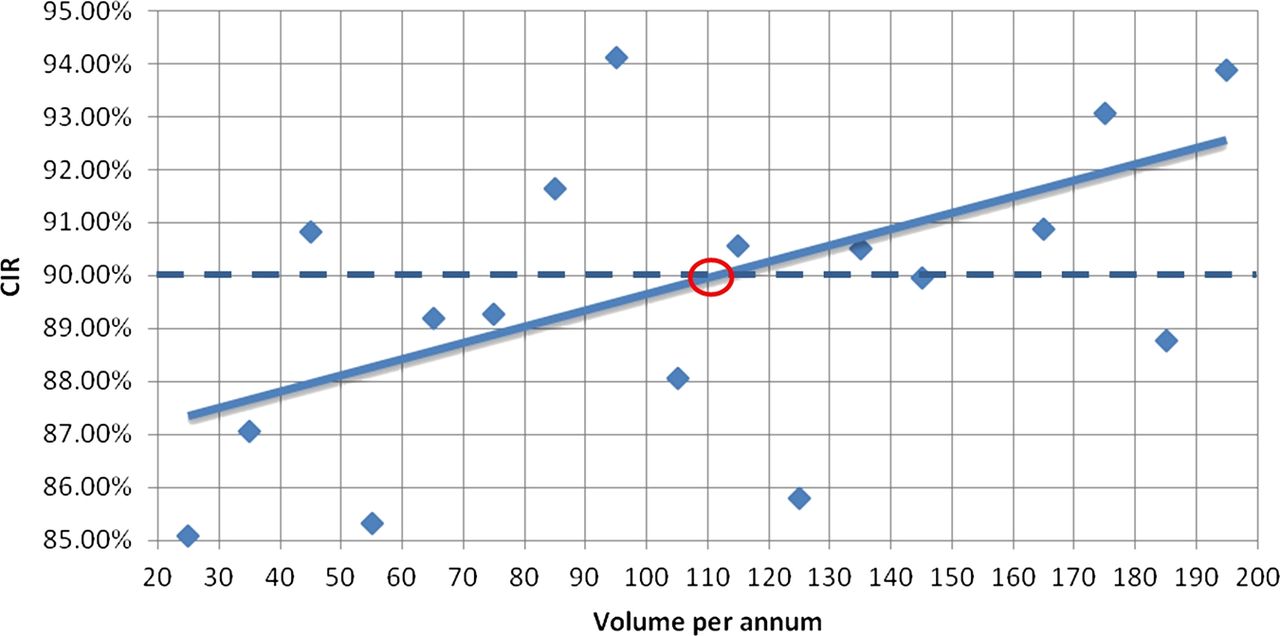
Finally, of the 12 594 procedures analysed, 9859 (78.3%) were performed by operators undertaking between 20 and 199 procedures per annum (120 operators out of 129). This subgroup was further analysed with operators being grouped with those undertaking a similar volume per annum—groups of 20 (figure 3) and groups of 10 (figure 4).

Scatter chart of individuals’ volume (grouped in 20s) against caecal intubation rate (CIR).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Scatter chart of individuals’ volume (grouped in 10s) against caecal intubation rate (CIR).
Results
Individuals’ volume per annum was plotted against CIR. The trend-line crosses 90% CIR standard at approximately 125 procedures (figure 1).
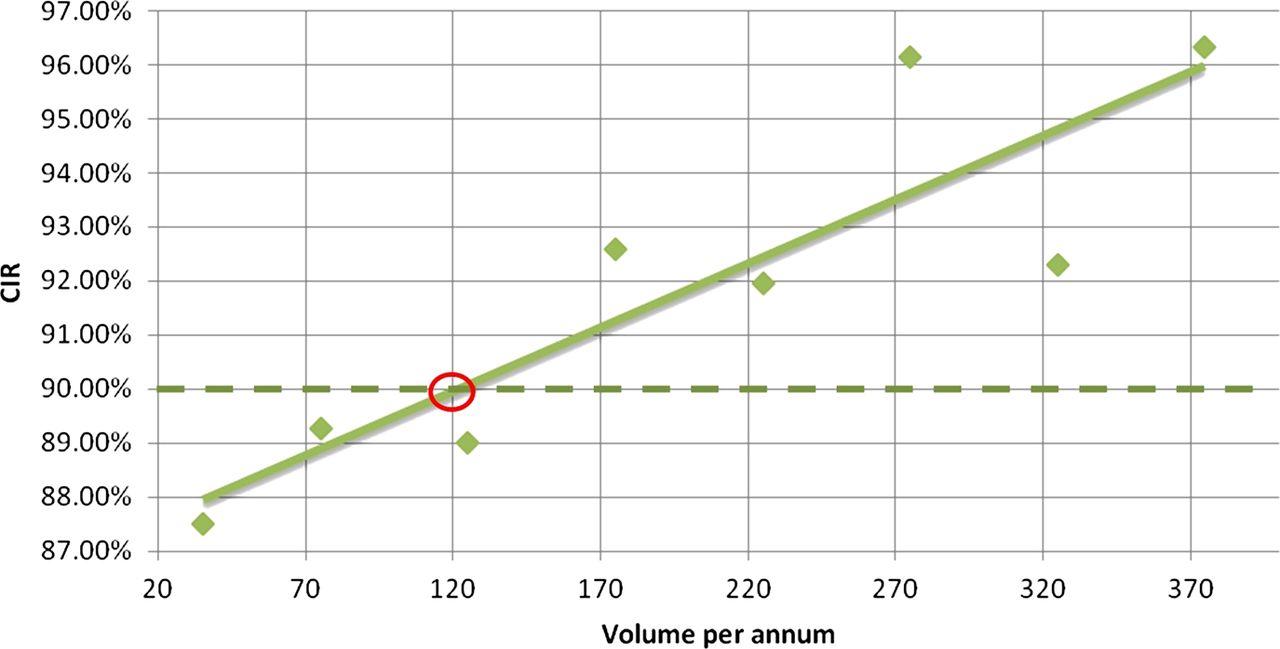
If operators are grouped with those undertaking a similar volume per annum (20–49, 50–99, 100–149, 150–199, 200–249, 250–299, 300–349, 350–399, groups of 50—table 1), when plotting these groups against combined CIR, trend-line crosses 90% CIR standard at approximately 120 procedures (figure 2).
Data represented in figure 2
If operators are grouped with those undertaking a similar volume per annum (groups of 20—table 2), when plotting these groups against combined CIR, trend-line crosses 90% CIR standard at approximately 115 procedures (figure 3).
Data represented in figure 3
If operators are grouped with those undertaking a similar volume per annum (groups of 10—table 3), when plotting these groups against combined CIR, trend-line crosses 90% CIR standard at approximately 110 procedures (figure 4).
Data represented in figure 4
Table 4 shows the totals of the data in tables 1⇑–3.
Totals
Discussion
When plotting individuals’ volume per annum against their CIR and when plotting groups of individuals who have undertaken a similar volume per annum (groups of 50), the trend-line on both charts (figures 1 and 2) crosses a 90% CIR at a volume of 120–125 procedures. The subanalysis focuses on individuals undertaking between 20 and 199 procedures per annum. Individuals were grouped with others undertaking a similar volume per annum (groups of 20 and groups of 10). Plotting these data against CIR, the trend-line on both charts (figures 3 and 4) crosses a 90% CIR at a volume of 110–120 procedures per annum.
While there will be variance in the quality of colonoscopy provided by individuals, the relationship with larger volume per annum and improved quality is intuitive—‘practice makes perfect’. This detailed analysis of such a large number of colonoscopies (12 594 in 2 years) suggests that JAG should advise operators to undertake a minimum of 120 procedures per annum to assist in attaining a minimum CIR standard of 90%.
Is this a feasible target? We believe strongly that it is. Most full time operators will be endoscoping at least 40 weeks per calendar year (allowances for annual leave, study leave and on-call commitments). A total of 120 colonoscopies for an operator endoscoping 40 weeks per annum is equivalent to three colonoscopies per week. An operator doing one list per week should be able to do three colonoscopies on that list, and those undertaking two or more lists per week should be able to achieve this with ease.
We believe strongly that a minimum standard of 120 colonoscopies per annum will have a positive effect on service and training. We would suggest that units flex capacity in order to achieve this. Lists should be profiled to operators’ capabilities concentrating more colonoscopies in fewer operators to preserve the volume and associated improved outcomes. Consolidating the number of operators performing more colonoscopies with improved outcomes will potentially translate into an enhanced training experience and skills translation.
Of real concern are operators carrying out less than 100 procedures per year; they did not meet the desired CIR quality standard, and performed 4793 colonoscopies.2 We would suggest that this reflects a wider experience in the English health service and needs to be addressed. It would be of great value and insight to triangulate this performance against a range of quality standards for colonoscopy.
In conclusion, this analysis of 12 594 colonoscopies over 2 years, namely, 129 operators doing between 20 and 399 colonoscopies per annum, suggests that to attain a minimum CIR of 90% operators should undertake at least 120 colonoscopies per annum. For most operators, this is equivalent to three colonoscopies per week—which is possible if one list per week is undertaken. For those undertaking two or more lists then this is achievable with ease. Endoscopy units need to reflect on this and consolidate operators to preserve volume and the associated improved outcomes. This will benefit patients, service and training.
We recommend a minimum volume of 120 colonoscopies be performed per year in order to meet current quality standards, and this should be reflected in JAG guidance.
What is already known on this topic
-
The Joint Advisory Group on Gastrointestinal endoscopy (JAG) advises that colonoscopists should undertake at least 100 procedures per annum.
-
The relationship of volume to quality and outcomes is well established in vascular surgery and other complex medical specialties.
-
Practitioners who undertake <100 colonoscopies per annum have statistically significant lower caecal intubation rates when compared with those who undertake ≥100 per annum.
What this study adds
-
This study analyses the correlation between volume and outcome, plotting individual and group volume per annum against caecal intubation rates.
-
Trend-lines on these plotted charts suggest that operators should undertake 120 colonoscopies per annum to achieve a caecal intubation rate of 90% or more.
-
This study is one of the most detailed published in looking at the correlation of volume of colonoscopies per annum to caecal intubation rates.
How might it impact on clinical practice in the foreseeable future
-
We suggest that JAG should revise guidance in light of this evidence and advise operators to undertake 120 colonoscopies per annum. This is an achievable standard; 120 colonoscopies for an operator endoscoping 40 weeks per year is equivalent to three colonoscopies per week.
http://www.icmje.org/coi_disclosure.pdf
http://resources.bmj.com/bmj/authors/checklists-forms/licence-for-publication)
Footnotes
-
Contributors AMV: collected and analysed the data and co-wrote the manuscript. AD reviewed the manuscript. APC reviewed the data and co-wrote the manuscript.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.