Article Text

Abstract
Endoscopic surveillance remains the core management of non-dysplastic Barrett's oesophagus, although questions regarding its efficacy in reducing mortality from oesophageal adenocarcinoma have yet to be definitively answered, and randomised trial data are awaited. One of the main goals of current research is to achieve risk stratification, identifying those at high risk of progression. The recent British Society of Gastroenterology (BSG) guidelines on surveillance have taken a step in this direction with interval stratification on clinicopathological grounds. The majority of Barrett's oesophagus remains undiagnosed, and this has led to investigation of methods of screening for Barrett's oesophagus, ideally non-endoscopic methods capable of reliably identifying dysplasia.
Chemoprevention to prevent progression is currently under investigation, and may become a key component of future treatment.
The availability of effective endotherapy means that accurate identification of dysplasia is more important than ever. There is now evidence to support intervention with radiofrequency ablation (RFA) for low-grade dysplasia (LGD), but recent data have emphasised the need for consensus pathology for LGD. Ablative treatment has become well established for high-grade dysplasia, and should be employed for flat lesions where there is no visible abnormality. Of the ablative modalities, RFA has the strongest evidence base. Endoscopic resection should be performed for all visible lesions, and is now the treatment of choice for T1a tumours.
Targeting those with high-risk disease will, hopefully, lead to efficacious and cost-effective surveillance, and the trend towards earlier intervention to halt progression gives cause for optimism that this will ultimately result in fewer deaths from oesophageal adenocarcinoma.
- BARRETT'S OESOPHAGUS
- BARRETT'S METAPLASIA
- ENDOSCOPY
- SCREENING
- CHEMOPREVENTION
Statistics from Altmetric.com
Introduction
Barrett's oesophagus has been recognised as a precursor lesion for oesophageal adenocarcinoma (OAC) for over 50 years,1 ,2 and the metaplasia-dysplasia-adenocarcinoma sequence is now well characterised.3 Endoscopic surveillance is now widely practised, and endoscopic therapy has become a central part of the management of dysplasia in Barrett's oesophagus. Nonetheless, there are many areas which remain the subject of debate in the management of Barrett's oesophagus. Current controversies include the efficacy and cost-effectiveness of surveillance programmes, how to risk-stratify to identify those most likely to progress, the role of chemoprevention, whether ablative therapy is indicated for those with low-grade dysplasia (LGD), and optimal management for dysplastic Barrett's oesophagus given an ever-growing array of endotherapeutic options. This review will focus on current management strategies for Barrett's oesophagus and Barrett's oesophagaus-associated neoplasia.
Management of non-dysplastic Barrett's oesophagus
Surveillance
The increased risk of OAC for patients with Barrett's oesophagus is well recognised, and this has led to the introduction of endoscopic surveillance programmes in many countries to achieve early detection of dysplastic or malignant change, and to enable curative intervention. Historically, early detection of cancer before lymphatic spread remains the primary aim of surveillance, but with increasing endoscopic options for early disease, the accurate identification of dysplasia is now critical.
Choosing an appropriate interval for surveillance endoscopy must balance this goal against the costs and acceptability of frequent endoscopy, along with the low annual cancer risk for patients with Barrett's oesophagus, which is below 0.5% for those in surveillance, and evidence from population studies suggest it may be closer to 0.12%–0.16%, overall.4–6
Evidence that endoscopic surveillance for Barrett's oesophagus reduces mortality from OAC continues to be debated. There is evidence for improved outcomes, or earlier stage at diagnosis with surveillance,7–14 however, randomised trial data are lacking. Recent population-wide studies in Northern Ireland15 and The Netherlands16 have shown improved outcomes from OAC, with participation in surveillance programmes, with this result persisting after adjustment for lead-time and length-time bias. However, other retrospective studies have failed to demonstrate any benefit from surveillance programmes.17 ,18
Surveillance programmes are expensive, and with uncertain efficacy, the cost-effectiveness of such programmes has been questioned.19–21 A large, randomised, controlled trial (RCT) is underway in the UK (Barrett's Oesophagus Surveillance Study) to assess the efficacy and cost-effectiveness of surveillance.
Given these concerns, risk stratification is a key goal of current research to identify those at highest risk of progression, rather than a ‘one size fits all’ policy that includes those at very low risk of malignancy. The recently updated British Society of Gastroenterology (BSG) guidelines have made several changes in line with this approach. For those with Barrett's oesophagus segment <3 cm, surveillance is now only advocated for those with intestinal metaplasia, and the recommended interval has been extended to 3–5 years.22 Surveillance every 2–3 years is reserved for those with Barrett's oesophagus segments with a length of 3 cm or greater. The current guidelines on endoscopic surveillance are summarised in figure 1.
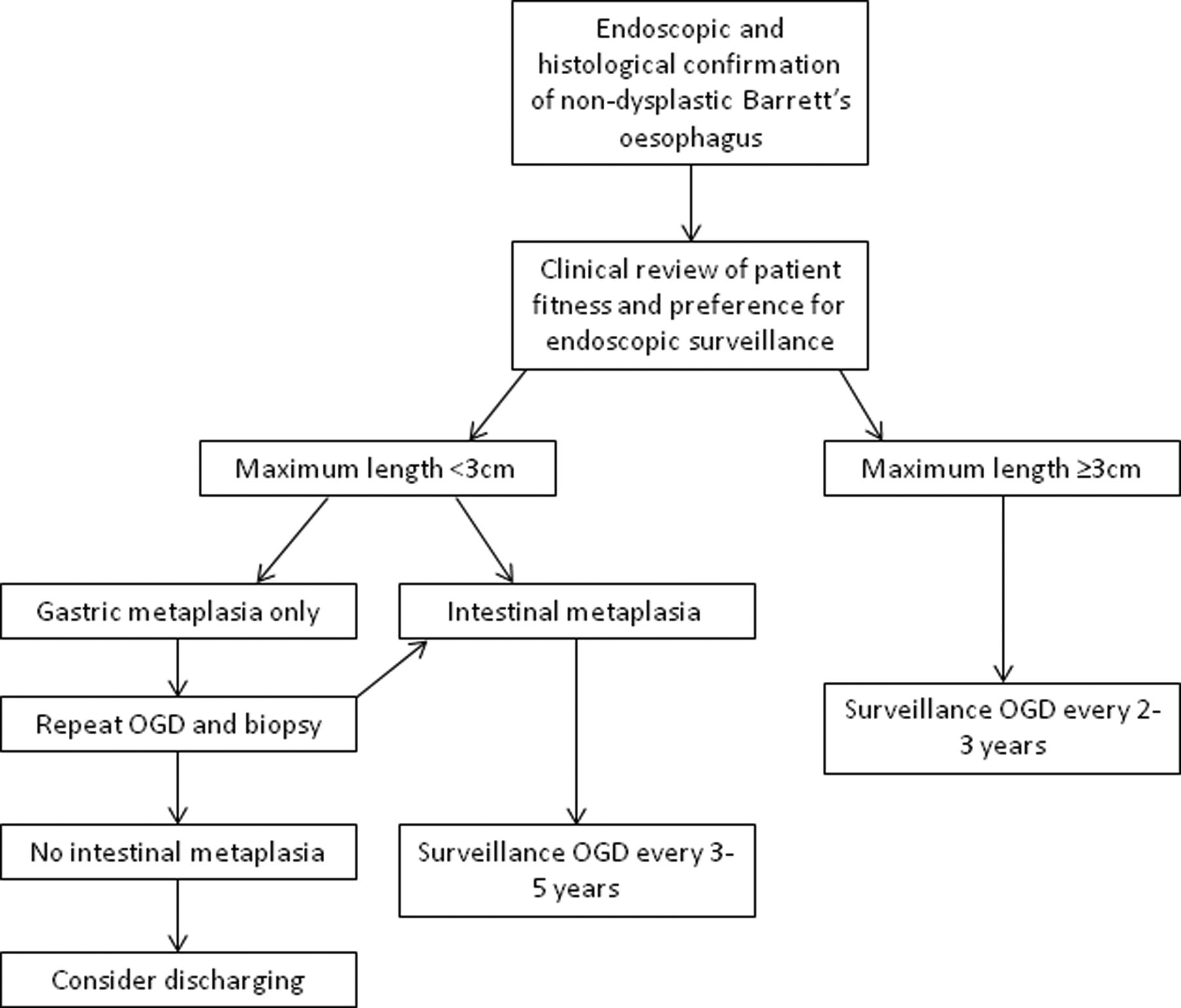
Guidelines for endoscopic surveillance of Barrett's oesophagus. Adapted from Fitzgerald et al,22 with permission. Note: the interval for repeat oesophagogastroduodenoscopy and biopsy after a finding of gastric metaplasia only, depends on the confidence of the endoscopic and histological findings and the number of biopsies taken. OGD, oesophagogastroduodenoscopy.
Further risk stratification through biomarkers has been a key aim of much recent research. The genetic changes that occur in progression from Barrett's oesophagus to invasive adenocarcinoma have been shown to be protean and complex.23–25 A large, genome-wide study of patients with disease across the spectrum from Barrett's oesophagus, dysplasia and adenocarcinoma, identified p53 and SMAD4 as the strongest markers of high-risk disease.23 As a biomarker, p53 has shown promise, and BSG guidelines advise consideration of its use as an immunostain to identify dysplasia.22 A preliminary study identified 86% of patients with dysplasia using a non-endoscopic cell collection device.23 The same genome-wide study showed that SMAD4 was highly specific, occurring only in adenocarcinoma, but since it was found in only 13% of cases it would be a low-sensitivity biomarker.23
Screening
Even highly effective surveillance can only have a limited outcome on overall survival from OAC, as only a small proportion of patients who develop adenocarcinoma have a previous diagnosis of Barrett's oesophagus. In a large, population-based study in Northern Ireland, only 7.3% of cases with OAC occurred in patients known to have Barrett's oesophagus.26 Although this may be influenced by successful surveillance programmes, this results largely from the high proportion of patients with undiagnosed Barrett's oesophagus: previous studies have estimated that up to 2% of the population have Barrett's oesophagus, with 80% undiagnosed.27–29
This has led some to consider screening for Barrett's oesophagus: several groups have examined the possibility of screening patients with chronic symptoms of gastro-oesophageal reflux disease (GORD). The prevalence of Barrett's oesophagus in patients with chronic GORD is 5%–15%.30 A meta-analysis by Taylor and Rubenstein31 found that while there was a strongly increased risk of long-segment Barrett's oesophagus with GORD symptoms (OR, 4.92, 95% CI 2.01 to 12.0), there was no association between short-segment Barrett's oesophagus and GORD (OR 1.15, 95% CI 0.76 to 1.73).
However, these symptoms are common among the general population, with around 20% having symptoms up to once a week,30 and around 6% of the population over the age of 45 years experiencing chronic symptoms.32 To screen all these individuals with endoscopy would require huge resources: estimates from the USA suggest that 6.6 million individuals would require endoscopy, with 1 OAC detected for every 1320 procedures.19 ,20 It must also be noted that 40% of patients with OAC (and 71% of patients with junctional adenocarcinoma of the cardia) do not report any GORD symptoms.33
Consequently, endoscopic screening in an unselected population with GORD is not currently recommended either in the USA or the UK.22 ,34 ,35 However, in the presence of multiple risk factors (chronic GORD plus 3 of the following: male, aged over 50 years, Caucasian, obese), the BSG guidelines advise consideration of screening, with a lower threshold for those with a first-degree relative with Barrett's oesophagus, or OAC.22
An alternative approach to screening is to use less invasive techniques to reduce the cost and/or morbidity. Studies assessing capsule endoscopy to identify Barrett's oesophagus have shown a relatively low sensitivity at 60%–78%.36–38 Others have used ultrathin transnasal endoscopes in patients with GORD or known Barrett's oesophagus, and demonstrated results very similar to conventional endoscopy.39 ,40
A further possibility currently being trialled is a swallowed cytology collection device (Cytosponge).41 The device is contained within a small capsule which is attached to a length of string: patients swallow the capsule, the gelatine capsule then dissolves in the acidic gastric secretions to reveal the collection device (analogous to a cytology brush), which is then withdrawn through the oesophagus using the string, collecting cells as it passes.
Accurate biomarkers of Barrett's oesophagus are required due to the mixed cell population collected by the device, with a previous study suggesting the most promising molecular marker using immunohistochemistry is Trefoil Factor 3 (TFF3).42 Furthermore, the acceptability of the device has been demonstrated in a primary care setting.41
The Barrett's oEsophagus Screening Trial (BEST2, ISRCTN 12730505)43 is a case-controlled study which aims to identify the sensitivity and specificity of the Cytosponge, and whether biomarkers can be used to risk-stratify patients when compared with the grade of dysplasia found at endoscopy and biopsy. Other outcomes include the safety profile of the device, along with the feasibility of high-throughput processing if the device were to be used for population-based screening.
To date, none of these technologies have entered routine clinical practice, but further trial results are awaited, and the prospect of screening could radically alter surveillance for Barrett's oesophagus and, potentially, lead on to a significant reduction in deaths from OAC.
Chemoprevention
There is increasing evidence for the use of certain drugs as chemoprevention for patients with Barrett's oesophagus. A number of cohort studies have shown a significantly reduced risk of progression to high-grade dysplasia (HGD) or OAC for patients taking proton pump inhibitors (PPI) versus no therapy, or on histamine-2 receptor antagonists (H2RA).44 ,45 However, data from RCTs are still awaited, and the BSG guidelines advise that ‘there is not yet sufficient evidence to advocate acid suppression drugs as chemopreventive agents’.22
Evidence for a protective effect from non-steroidal anti-inflammatory drugs (NSAID) comes from large meta-analyses of patients taking aspirin as primary or secondary prevention for cardiovascular disease.46–48 In the largest of these, incorporating data from 23 535 patients, those followed-up for 10–20 years after starting aspirin, and having taken aspirin daily for 5 years or more, had a significant reduction in risk of OAC, HR 0.36 (95% CI 0.18 to 0.71).46
Once again, there are no data from randomised trials, and given the risks of NSAIDs, such as gastrointestinal bleeding and cerebral haemorrhage, this will be crucial in informing management decisions for patients with Barrett's oesophagus.49
Aspirin and Esomeprazole for Chemoprevention in Barrett's metaplasia is a large, multicentre RCT (NCT00357682) which aims to address the lack of randomised data, and evaluate the risks and benefits of both PPIs and NSAIDs as chemoprevention in Barrett's oesophagus.50 The trial has four arms, with patients randomised to low-dose or high-dose PPI (esomeprazole)± aspirin.
There is some evidence from observational studies for a protective effect from statins against oesophageal cancer. A recent meta-analysis reviewed the effects of statins in a patient with Barrett's oesophagus,51 including 11 observational studies with a total of 1999 patients, and found an OR for progressing to OAC was 0.57 (95%CI 0.43 to 0.75) for those on a statin.
While the absence of randomised data limits current recommendations for chemoprevention, this paradigm may become a key component in the management of Barrett's oesophagus in future.
Management of Barrett's oesophagus-associated neoplasia
Endoscopic treatments aim to remove or destroy areas of neoplasia in the oesophagus, either through resection or ablation, and promote regrowth of the normal squamous lining. The goal of ablative techniques is to achieve complete eradication of dysplasia, along with complete eradication of intestinal metaplasia.52 These minimally invasive treatments can offer treatment without recourse to radical surgery and, thus, can be considered in patients with earlier-stage disease, and those for whom major surgery would be a very high risk.
The BSG guidelines advise the following algorithm (see figure 2) for management of dysplastic Barrett's oesophagus, and this is discussed further below.
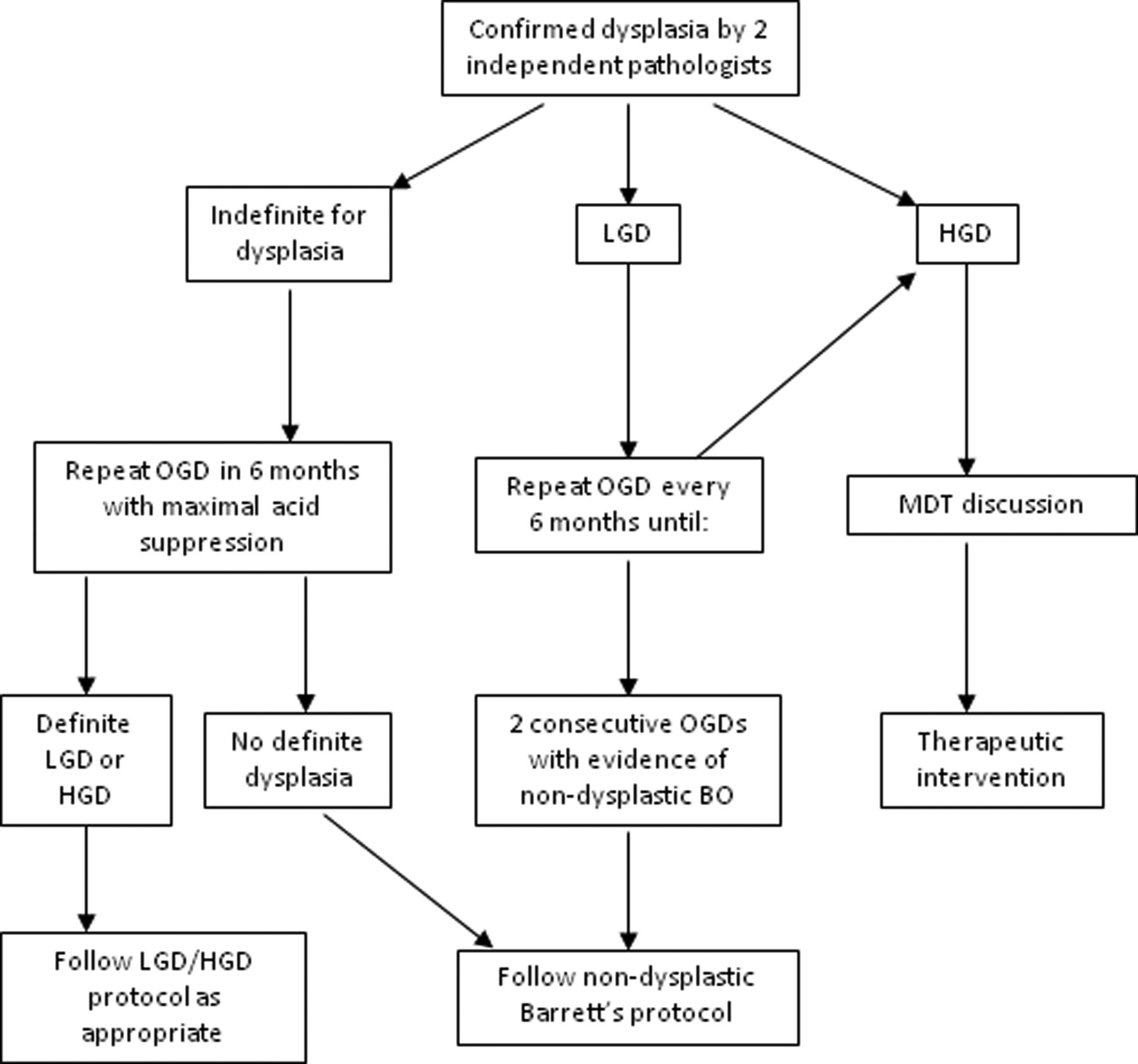
Algorithm for management of dysplastic Barrett's oesophagus. Adapted from Fitzgerald et al,22 with permission. LGD, low-grade dysplasia; HGD, high-grade dysplasia; OGD, oesophagogastroduodenoscopy; MDT, multidisciplinary team.
Low-grade dysplasia
In the 2014 BSG guidelines, as shown in figure 3, patients found to have LGD are advised to have 6-monthly oesophagogastroduodenoscopy (OGD) surveillance until biopsy confirms regression to non-dysplastic Barrett's oesophagus on successive OGDs, or progression to HGD occurs.22 However, a recent RCT from European centres reported a highly significant reduction in progression for patients with LGD treated with radiofrequency ablation (RFA).53 The rate of progression to HGD or cancer over a 3-year follow-up was 1.5% in the ablation group versus 26.5% in the untreated group (p<0.001), with progression to cancer 1.5% vs 8.8%, respectively (p=0.03).

{kind=link}
{kind=link}
{kind=link}
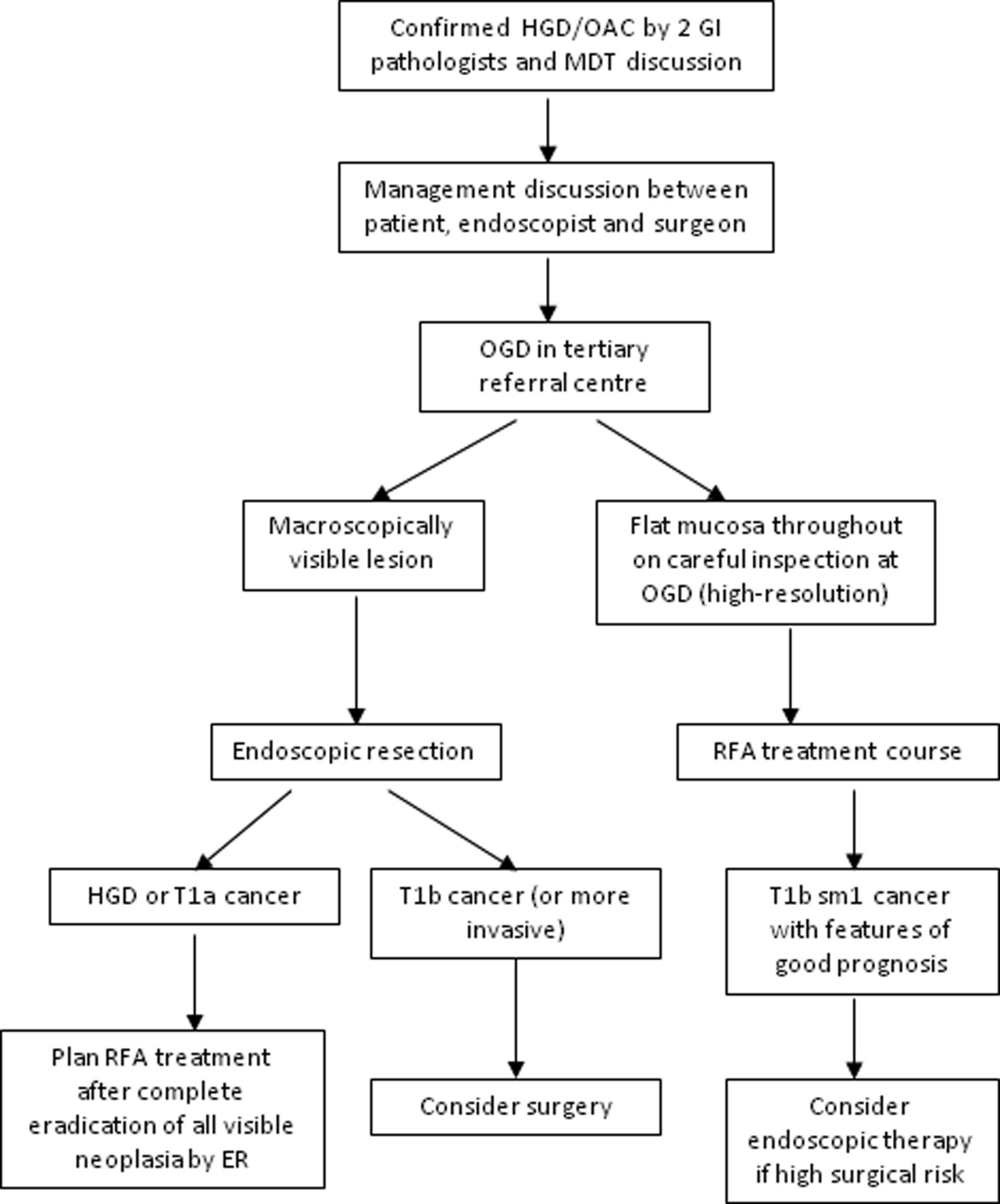
Algorithm for managing HGD and early oesophageal adenocarcinoma. Adapted from Fitzgerald et al,22 with permission. HGD, high-grade dysplasia; OAC, early oesophageal adenocarcinoma; MDT, multidisciplinary team; OGD, oesophagogastroduodenoscopy; RFA, radiofrequency ablation.
It must be noted that the rate of progression in the control arm in this trial (26.5% over 3 years) was much higher than might be expected from the natural history of LGD reported in other studies, with a recent meta-analysis calculating a risk of progression to HGD or cancer of around 1% per year.54 The use of an expert pathology panel for consensus diagnosis, with a very robust classification as LGD, is likely to have influenced the composition of the group seen in the study by Phoa et al53 Of 511 patients with an initial diagnosis of LGD screened for entry to the trial, only 247 were confirmed to have LGD after review by the expert panel, and 140 went on to be randomised.53
In light of these findings, it seems likely that historical overdiagnosis of LGD has led to an underestimation of the true risk of progression with LGD.54 This suggests the need for consensus reporting of all Barrett's dysplasia specimens, and the question of whether to offer intervention in the absence of consensus is difficult.
The recently published National Institute for Health and Care Excellence guidelines now support the use of RFA for the ablation of LGD.55
High-grade dysplasia
The diagnosis of HGD has serious implications for patients. They have a high risk of progression to adenocarcinoma, and also a significant risk that a small focus of cancer may already be present, but not yet detected.56 For this reason, historically, the treatment of HGD was radical oesophagectomy for those considered fit for surgery. The advent of endotherapy led to great debate over whether these treatments could offer oncologically sound treatment. Although there have not been any randomised trials directly comparing surgery with endotherapies, the growing body of evidence for endotherapies over the past 20 years or so has resolved this debate, and endoscopic resection (ER) is now considered the treatment of choice for patients with macroscopically visible HGD or T1a adenocarcinoma.22 The management of HGD and early oesophageal cancer is shown in the algorithm in figure 3.
For visible lesions, ER is preferred over ablative therapy alone because it provides the most accurate staging information. Depth of invasion can be accurately assessed: data from stepwise ER of entire Barrett's oesophagus segments have confirmed that the most advanced disease is located in visible lesions.57 A meta-analysis of studies in which patients have undergone oesophagectomy for HGD found the risk of invasive OAC to be 11% in those with visible lesions, compared to 3% in those with no visible lesion.56
There are now numerous ablative techniques for HGD: each of these techniques has its strengths and weaknesses, and some key features are presented in table 1 below. RCT data are available for some of these modalities, and includes direct comparison of certain techniques. Currently, there is a large-scale trial (Barrett's Radiofrequency Intervention for Dysplasia by Endoscopy, NCT017337) underway aiming to compare outcomes between RFA and argon plasma coagulation.58 This pilot study has just been closed to recruitment, and initial data will be available soon. On the basis of currently available RCT data, and taking account of the side effect profiles of each treatment, RFA is recommended as the first-line therapy for HGD outside the context of RCTs.22
Comparison of ablative techniques for HGD
The first major RCT of RFA randomised 127 patients on a 2:1 allocation to RFA or a sham procedure.59 Complete eradication of HGD was seen in 81.0% of treated patients versus 19.0% of controls (p<0.001). In a later report on extended follow-up of this group, 96% of those achieving eradication of HGD remained free of HGD at 3-year follow-up.60 Risk of any disease progression was reduced in the ablation group (3.6% vs 16.3%, p=0.03), as was the risk of cancer (1.2% vs 9.3%, p=0.045).
A meta-analysis of RFA for Barrett's oesophagus calculated pooled estimates for complete eradication of dysplasia of 91% (87%–95%, 95% CI), and complete eradication of intestinal metaplasia 78% (70%–86%, 95% CI).61 The commonest complication was stricture, which occurred in 5% of patients treated with RFA.
Intramucosal adenocarcinoma
The low risk of nodal metastasis with T1a cancer (0%–10%)62–69 has resulted in very good tumour-free and overall survival with ER for T1a cancers in high-volume centres. One recent large series reported tumour-free survival of 93.8% at mean follow-up of 56.6 months.70 ER for T1b tumours is associated with poorer outcomes, with 5-year tumour-free and overall survival at 60% and 58%, respectively, likely due to increased depth and higher risk of nodal involvement (up to 46%).62–69 For upper third tumours of the submucosa (T1bsm1) the risk of lymph node metastasis is relatively low (around 10%), and some series report good outcomes treating T1bsm1 tumours endoscopically.63 ,68 ,70 Decision making may be further influenced by pathological indicators of good prognosis, such as clear resection margins, and absence of vascular and lymphatic invasion.71 The use of ER for T1bsm1 cancer remains debated, however, and the current BSG guidance advises surgery for patients who are fit enough, but that ER should be offered with curative intent in patients who are high-risk surgical candidates (see figure 3).22
While ER is effective at removing Barrett's oesophagus-associated intramucosal lesions, these patients have a high rate of metachronous lesions after ER alone, affecting around 15%–20%.70 ,72 The risk of developing further lesions can be reduced significantly with ablative therapy to the remaining Barrett's oesophagus segment.57 ,72 Current guidance advises removal of all visible lesions with ER, followed by ablative therapy (currently, RFA is the preferred method) to all residual areas of Barrett's oesophagus.22
Conclusions
The recent update to BSG guidelines represents a move towards a more stratified approach to surveillance of Barrett's oesophagus. This trend is likely to continue with ongoing efforts to identify those at high risk of progression through appropriate genetic or cellular biomarkers.
Advances in endoscopic therapy have revolutionised the treatment of dysplastic Barrett's oesophagus, and this indication now extends to those with confirmed LGD, although the challenges of achieving consensus histology remain a pressing issue.
Ongoing trials of chemoprevention and screening may lead to new approaches to Barrett's oesophagus. The possibility of an efficacious, non-endoscopic test offers hope of a cost-effective means of achieving this, and large-scale randomised trial data are eagerly awaited to evaluate agents, such as aspirin and PPIs, as chemoprevention in Barrett's oesophagus.
Thus, it seems likely that the future will bring a continued increase in intervention for those with early disease through chemoprevention and endotherapy, more targeted surveillance, and a reduction in patients requiring radical surgery or presenting with disseminated disease.
References
Footnotes
-
Contributors All the authors contributed to preparation of the manuscript.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.